


Mental Fatigue Is Associated with Subjective Cognitive Decline among Older Adults
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Participants and Procedure
2.2. Measure
2.3. Data Analyses
3. Results
3.1. Sample Characteristics
3.2. SCD Mean Score Differences between Age and Gender Groups
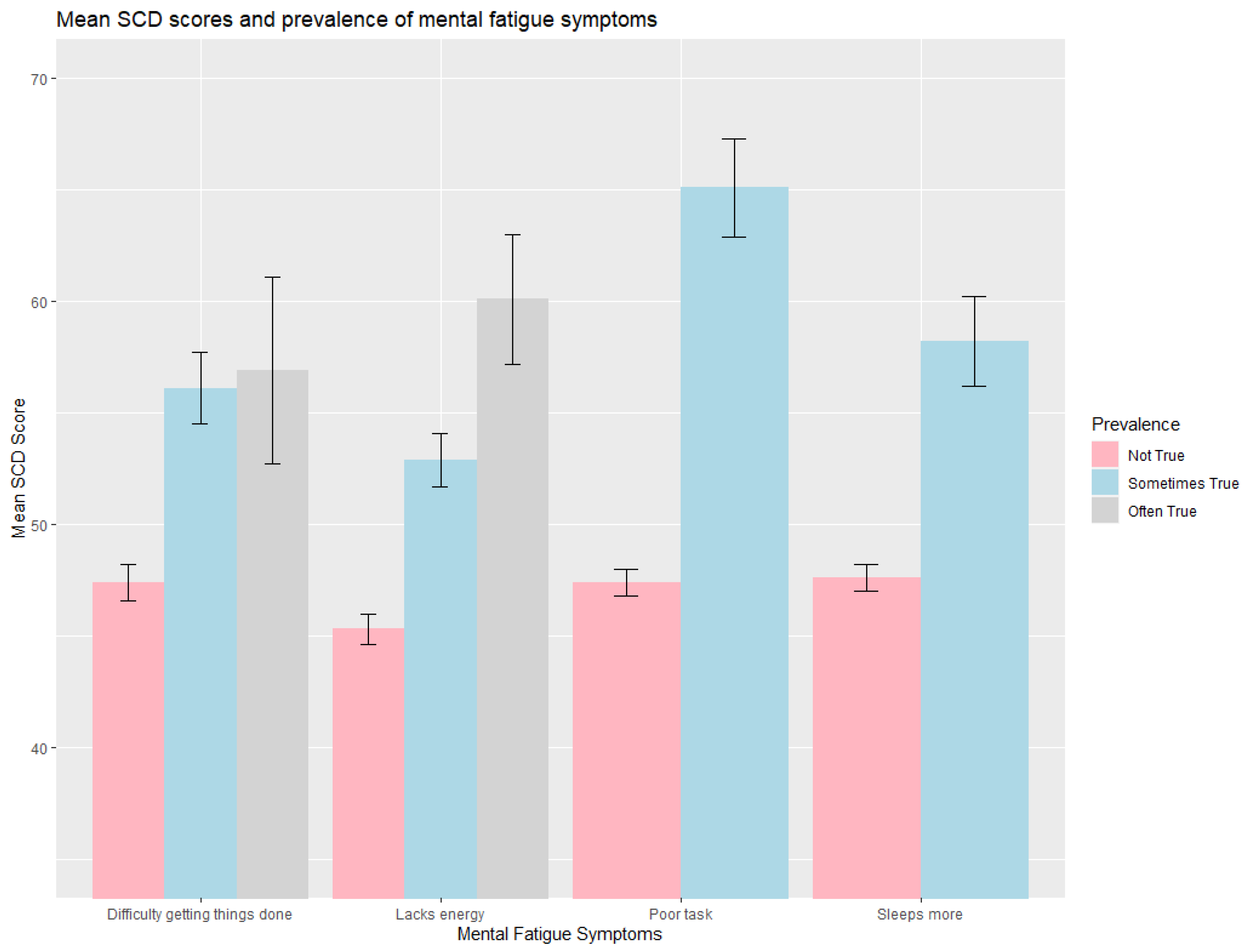
3.3. SCD Score and Prevalence of Mental Fatigue Symptoms
3.4. Factors Associated with SCD among Old Adults
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Variables | N | Mean (SD) | p | |
|---|---|---|---|---|
| Difficulty getting things done | Not True | 480 | 47.4 (8.18) | <0.001 *** |
| Sometimes True | 156 | 56.1 (10.4) | ||
| Often True | 45 | 56.9 (13.8) | ||
| Poor task | Not True | 581 | 47.4 (7.19) | <0.001 *** |
| Sometimes True | 100 | 65.1 (11.1) | ||
| Sleeps more | Not True | 529 | 47.6 (7.52) | <0.001 *** |
| Sometimes True | 152 | 58.2 (13.00) | ||
| Lacks energy | Not True | 332 | 45.3 (6.52) | <0.001 *** |
| Sometimes True | 274 | 52.9 (9.76) | ||
| Often True | 75 | 60.1 (12.50) |
References
- Vaupel, J.W. Biodemography of human ageing. Nature 2010, 464, 536–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations. Department of Economic and Social Affairs. Population Division. World Population Ageing.. 2019. Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Report.pdf (accessed on 9 December 2022).
- Textor, C. Aging Population in China—Statistics & Facts. Available online: https://www.statista.com/topics/6000/aging-population-in-china/#topicOverview (accessed on 9 December 2022).
- Ageing and Health—China. Available online: https://www.who.int/china/health-topics/ageing (accessed on 9 December 2022).
- Jia, L.; Du, Y.; Chu, L.; Zhang, Z.; Li, F.; Lyu, D.; Li, Y.; Li, Y.; Zhu, M.; Jiao, H.; et al. Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: A cross-sectional study. Lancet 2020, 5, E661–E671. [Google Scholar] [CrossRef] [PubMed]
- Murman, D.L. The Impact of Age on Cognition. Semin. Hear. 2015, 36, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Cognitive Impairment: A Call for Action, Now! Available online: https://www.cdc.gov/aging/pdf/cognitive_impairment/cogimp_poilicy_final.pdf (accessed on 30 January 2023).
- Subjective Cognitive Decline—A Public Health Issue. Available online: https://www.cdc.gov/aging/data/subjective-cognitive-decline-brief.html (accessed on 9 December 2022).
- Alzheimer’s Association. 2018 Alzheimer’s disease facts and figures. Alzheimer’s Dement. 2018, 14, 367–429. [Google Scholar] [CrossRef]
- Jessen, F.; Amariglio, R.E.; Boxtel, M.V.; Breteler, M.; Ceccaldi, M.; Chételat, G.; Dubois, B.; Dufouil, C.; Ellis, K.A.; Flier, W.M.v.d.; et al. A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheimer’s Dement. 2014, 10, 844–852. [Google Scholar] [CrossRef] [Green Version]
- Slot, R.E.R.; Sikkes, S.A.M.; Berkhof, J.; Brodaty, H.; Buckley, R.; Cavedo, E.; Dardiotis, E.; Guillo-Benarous, F.; Hampel, H.; Kochan, N.A.; et al. Subjective cognitive decline and rates of incident Alzheimer’s disease and non–Alzheimer’s disease dementia. Alzheimer’s Dement. 2018, 15, 465–476. [Google Scholar] [CrossRef]
- Sperling, R.A.; Aisen, P.S.; Beckett, L.A.; Bennett, D.A.; Craft, S.; Fagan, A.M.; Iwatsubo, T.; Jack, C.R., Jr.; Kaye, J.; Montine, T.J.; et al. Toward defining the preclinical stages of Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 280–292. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Blázquez, M.A.; Ávila-Villanueva, M.; Maestú, F.; Medina, M. Specific Features of Subjective Cognitive Decline Predict Faster Conversion to Mild Cognitive Impairment. J. Alzheimer’s Dis. 2016, 52, 271–281. [Google Scholar] [CrossRef]
- Yan, X.; Lin, S.; Li, J.; Cheng, H.; Liu, X.; Pei, L. Vital Surveillances: Trends in the Prevalence of Cognitive Impairment Among Older Adults Aged 65 to 105 Years—China, 2002–2018. China CDC Wkly. 2022, 4, 945–949. [Google Scholar] [CrossRef]
- Ouchi, Y.; Rakugi, H.; Arai, H.; Akishita, M.; Ito, H.; Toba, K.; Kai, I. Redefining the elderly as aged 75 years and older: Proposal from the Joint Committee of Japan Gerontological Society and the Japan Geriatrics Society. Geriatr. Gerontol. Int. 2017, 17, 1045–1047. [Google Scholar] [CrossRef] [Green Version]
- Alterovitz, S.S.R.; Mendelsohn, G.A. Relationship goals of middle-aged, young-old, and old-old internet daters: An analysis of online personal ads. J. Aging Stud. 2013, 27, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.B.; Oh, J.H.; Park, J.H.; Choi, S.P.; Wee, J.H. Differences in youngest-old, middle-old, and oldest-old patients who visit the emergency department. Clin. Exp. Emerg. Med. 2018, 5, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Forman, D.E.; Berman, A.D.; McCabe, C.H.; Baim, D.S.; Wei, J.Y. PTCA in the elderly: The “young-old” versus the “old-old”. J. Am. Geriatr. Soc. 1992, 40, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Röhr, S.; Pabst, A.; Riedel-Heller, S.G.; Jessen, F.; Turana, Y.; Handajani, Y.S.; Brayne, C.; Matthews, F.E.; Stephan, B.C.M.; Lipton, R.B.; et al. Estimating prevalence of subjective cognitive decline in and across international cohort studies of aging: A COSMIC study. Alzheimer’s Res. Ther. 2020, 12, 167. [Google Scholar] [CrossRef] [PubMed]
- Yuan, L.; Zhang, X.; Guo, N.; Li, Z.; Lv, D.; Wang, H.; Jin, J.; Wen, X.; Zhao, S.; Xu, T.; et al. Prevalence of cognitive impairment in Chinese older inpatients and its relationship with 1-year adverse health outcomes: A multi-center cohort study. BMC Geriatr. 2021, 21, 595. [Google Scholar] [CrossRef]
- Rabin, L.A.; Smart, C.M.; Crane, P.K.; Amariglio, R.E.; Berman, L.M.; Boada, M.; Buckley, R.F.; Chételat, G.; Dubois, B.; Ellis, K.A.; et al. Subjective Cognitive Decline in Older Adults: An Overview of Self-Report Measures Used Across 19 International Research Studies. J. Alzheimer’s Dis. 2015, 48, S63–S86. [Google Scholar] [CrossRef] [Green Version]
- Song, M.; Lee, S.H.; Kim, S.Y.; Kang, Y. Measurement of Subjective Cognitive Decline (SCD) Using Korean-Everyday Cognition (K-ECog) as a Screening Tool: A Feasibility Study. Dement. Neurocogn. Disord. 2021, 20, 80–88. [Google Scholar] [CrossRef]
- Díaz-García, J.; González-Ponce, I.; Ponce-Bordón, J.C.; López-Gajardo, M.Á.; Ramírez-Bravo, V.; Rubio-Morales, A.; García-Calvo, T. Mental Load and Fatigue Assessment Instruments: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 419. [Google Scholar] [CrossRef]
- Lin, F.; Roiland, R.; Heffner, K.; Johnson, M.; Chen, D.; Mapstone, M. Evaluation of objective and perceived mental fatigability in older adults with vascular risk. J. Psychosom. Res. 2014, 76, 458–464. [Google Scholar] [CrossRef] [Green Version]
- Cohen, R.W.; Meinhardt, A.J.; Gmelin, T.; Qiao, Y.S.; Moored, K.D.; Katz, R.D.; Renner, S.W.; Glynn, N.W. Prevalence and severity of perceived mental fatigability in older adults: The Long Life Family Study. J. Am. Geriatr. Soc. 2021, 69, 1401. [Google Scholar] [CrossRef]
- Boksem, M.A.S.; Meijman, T.F.; Lorist, M.M. Mental fatigue, motivation and action monitoring. Biol. Psychol. 2006, 72, 123–132. [Google Scholar] [CrossRef]
- Marcora, S.M.; Staiano, W.; Manning, V. Mental fatigue impairs physical performance in humans. J. Appl. Physiol. 2009, 106, 857–864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Achenbach, T.M.; Newhouse, P.A.; Rescorla, L.A. Manual for the ASEBA Older Adult Forms & Profiles; University of Vermont, Research Center for Children, Youth, & Families: Burlington, VT, USA, 2004. [Google Scholar]
- Lin, L.-H.; Wang, S.-B.; Xu, W.-Q.; Hu, Q.; Zhang, P.; Ke, Y.-F.; Huang, J.-H.; Ding, K.-R.; Li, X.-L.; Hou, C.-L.; et al. Subjective cognitive decline symptoms and its association with socio-demographic characteristics and common chronic diseases in the southern Chinese older adults. BMC Public Health 2022, 22, 127. [Google Scholar] [CrossRef] [PubMed]
- Nelson, A.; Gavelin, H.M.; Boraxbekk, C.-J.; Eskilsson, T.; Josefsson, M.; Järvholm, L.S.; Neely, A.S. Subjective cognitive complaints in patients with stress-related exhaustion disorder: A cross sectional study. BMC Psychol. 2021, 9, 84. [Google Scholar] [CrossRef] [PubMed]
- Kuba, K.; Weißflog, G.; Götze, H.; García-Torres, F.; Mehnert, A.; Esser, P. The relationship between acceptance, fatigue, and subjective cognitive impairment in hematologic cancer survivors. Int. J. Clin. Health Psychol. 2019, 19, 2. [Google Scholar] [CrossRef]
- Podlesek, A.; Komidar, L.; Kavcic, V. The Relationship Between Perceived Stress and Subjective Cognitive Decline During the COVID-19 Epidemic. Front. Psychol. 2021, 12, 647971. [Google Scholar] [CrossRef]
- Si, T.; Xing, G.; Han, Y. Subjective Cognitive Decline and Related Cognitive Deficits. Front. Neurol. 2020, 11, 247. [Google Scholar] [CrossRef]
- Liu, J.; Lee, C.M.; An, Y.; Sun, Q.; Mei, H.; Shi, S.; Ivanova, M.; Rao, H. Application of the Older Adult Self-Report and Older Adult Behavior Checklist to Chinese Older Adults: Syndrome Structure and Inter-Informant Agreement. J. Gerontol. Nurs. 2022, 48, 26–32. [Google Scholar] [CrossRef]
- Ivanova, M.Y.; Achenbach, T.M.; Rescorla, L.A.; Turner, L.V.; Dumas, J.A.; Almeida, V.; Anafarta-Sendag, M.; Bite, I.; Boomsma, D.I.; Caldas, J.C.; et al. The generalizability of Older Adult Self-Report (OASR)syndromes of psychopathology across 20 societies. Int. J. Geriatr. Psychiatry 2020, 35, 525–536. [Google Scholar] [CrossRef]
- Schliep, K.C.; Barbeau, W.A.; Lynch, K.E.; Sorweid, M.K.; Varner, M.W.; Foster, N.L.; Qeadan, F. Overall and sex-specific risk factors for subjective cognitive decline: Findings from the 2015–2018 Behavioral Risk Factor Surveillance System Survey. Biol. Sex Differ. 2022, 13, 16. [Google Scholar] [CrossRef]
- Wang, L.; Tian, T. Gender Differences in Elderly With Subjective Cognitive Decline. Front. Aging Neurosci. 2018, 10, 166. [Google Scholar] [CrossRef] [PubMed]
- Levine, D.A.; Gross, A.L.; Briceño, E.M.; Tilton, N.; Giordani, B.J.; Sussman, J.B.; Hayward, R.A.; Burke, J.F.; Hingtgen, S.; Elkind, M.S.V.; et al. Sex Differences in Cognitive Decline Among US Adults. JAMA Netw. Open 2021, 4, e210169. [Google Scholar] [CrossRef] [PubMed]
- Deng, Q.; Liu, W. Inequalities in cognitive impairment among older adults in China and the associated social determinants: A decomposition approach. Int. J. Equity Health 2021, 20, 82. [Google Scholar] [CrossRef] [PubMed]
- Hara, Y.; Waters, E.M.; McEwen, B.S.; Morrison, J.H. Estrogen Effects on Cognitive and Synaptic Health Over the Lifecourse. Physiol. Rev. 2015, 95, 785–807. [Google Scholar] [CrossRef] [Green Version]
- Reuben, R.; Karkaby, L.; McNamee, C.; Einstein, G.; Phillips, N.A. Menopause and cognitive complaints: Are ovarian hormones linked withsubjective cognitive decline? Climacteric 2021, 24, 321–332. [Google Scholar] [CrossRef]
- Chen, S.; Wang, Y.; She, R. Prevalence and gender disparity of those who screen positive for depression in China by the classification of the employer and industry: A cross-sectional, population-based study. BMC Psychiatry 2023, 23, 62. [Google Scholar] [CrossRef]
- Zhou, L.; Ma, X.; Wang, W. Relationship between Cognitive Performance and Depressive Symptoms in Chinese Older Adults: The China Health and Retirement Longitudinal Study (CHARLS). J. Affect. Disord. 2021, 281, 454–458. [Google Scholar] [CrossRef]
- Lv, Q.; Li, X.; Zhang, Y.; Lu, D.; Lu, J.; Xie, Q.; Li, H.; Wu, Y.; Wang, C.; Yi, Z. Sex Differences in cognitive impairment and clinical correlates in Chinese patients with subthreshold depression. Biol. Sex Differ. 2022. in review. [Google Scholar] [CrossRef]
- Danielewicz, A.L.; Wagner, K.J.P.; d’Orsi, E.; Boing, A.F. Is Cognitive Decline in the Elderly Associated with Contextual Income? Results of a Population-Based Study in Southern Brazil. Cad. Saúde Pública 2016, 32, e00112715. [Google Scholar] [CrossRef] [Green Version]
- Hazzouri, A.Z.A.; Haan, M.N.; Osypuk, T.; Abdou, C.; Hinton, L.; Aiello, A.E. Neighborhood Socioeconomic Context and Cognitive Decline Among Older Mexican Americans: Results From the Sacramento Area Latino Study on Aging. Am. J. Epidemiol. 2011, 174, 423–432. [Google Scholar] [CrossRef] [Green Version]
- Livingston, P.G.; Huntley, J.; Sommerlad, A.; Ames, P.D.; Ballard, P.C.; Banerjee, P.S.; Brayne, P.C.; Burns, P.A.; Cohen-Mansfield, P.J.; Cooper, P.C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef] [PubMed]
- Carbone, E.; Piras, F.; Pellegrini, F.F.; Caffarra, P.; Borella, E. Individual differences among older adults with mild and moderate dementia in social and emotional loneliness and their associations with cognitive and psychological functioning. BMC Geriatr. 2022, 22, 859. [Google Scholar] [CrossRef] [PubMed]
- Gierveld, J.D.J. A review of loneliness: Concept and definitions, determinants and consequences. Rev. Clin. Gerontol. 1998, 8, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Nerobkova, N.; Park, Y.S.; Shin, J.; Park, E.-C. Marital transition and cognitive function among older adults: The korean Longitudinal Study of Aging (2006–2020). BMC Geriatr. 2022, 22, 1003. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Zhang, Y.; Burgard, S.A.; Needham, B.L. Marital status and cognitive impairment in the United States: Evidence from the National Health and Aging Trends Study. Ann. Epidemiol. 2019, 38, 28–34.e22. [Google Scholar] [CrossRef]
- Feng, L.; Ng, X.-T.; Yap, P.; Li, J.; Lee, T.-S.; Håkansson, K.; Kua, E.-H.; Ng, T.-P. Marital Status and Cognitive Impairment among Community-Dwelling Chinese Older Adults: The Role of Gender and Social Engagement. Dement. Geriatr. Cogn. Disord. Extra 2014, 4, 375–384. [Google Scholar] [CrossRef]
- Erickson, K.I.; Hillman, C.; Stillman, C.M.; Ballard, R.M.; Bloodgood, B.; Conroy, D.E.; Macko, R.; Marquez, D.X.; Petruzzello, S.J.; Powell, K.E. Physical activity, cognition, and brain outcomes: A review of the 2018 physical activity guidelines. Med. Sci. Sport. Exerc. 2019, 51, 1242. [Google Scholar] [CrossRef]
- Tanaka, M.; Ishii, A.; Watanabe, Y. Neural effect of mental fatigue on physical fatigue: A magnetoencephalography study. Brain Res. 2014, 1542, 49–55. [Google Scholar] [CrossRef]
- Suh, S.W.; Han, J.W.; Lee, J.R.; Byun, S.; Kwon, S.J.; Oh, S.H.; Lee, K.H.; Han, G.; Hong, J.W.; Kwak, K.P.; et al. Sleep and cognitive decline: A prospective nondemented elderly cohort study. Ann. Neurol. 2018, 83, 472–482. [Google Scholar] [CrossRef]

| Variables | Young-Old (N = 508) | Old-Old (N = 173) | Males (N = 306) | Females (N = 375) | Total (N = 681) |
|---|---|---|---|---|---|
| Age | 66.13 (4.37) | 80.17 (4.11) | 70.69 (7.65) | 68.89 (7.25) | 69.7 (7.48) |
| Young-Old | -- | -- | 212 (69.28%) | 296 (78.93%) | 508 (74.60%) |
| Old-old | -- | -- | 84 (27.45%) | 79 (21.07%) | 173 (25.40%) |
| Gender | |||||
| Males | 212 (41.73%) | 94 (54.34%) | -- | -- | 306 (44.93%) |
| Females | 296 (58.27%) | 79 (45.66%) | -- | -- | 375 (55.07%) |
| Education Level | |||||
| High-Edu | 182 (35.83%) | 74 (42.77%) | 127 (41.50%) | 129 (34.40%) | 256 (37.59%) |
| Low-Edu | 326 (64.17%) | 99 (57.23%) | 179 (58.50%) | 246 (65.60%) | 425 (62.41%) |
| Income Level | |||||
| High-income | 251 (49.41%) | 95 (54.91%) | 179 (58.50%) | 167 (44.53%) | 356 (52.28%) |
| Low-income | 257 (50.59%) | 78 (45.09%) | 127 (41.50%) | 208 (55.47%) | 335 (49.19%) |
| Marital/Living Status | |||||
| Live w. Spouse/Partner | 393 (77.36%) | 93 (53.76%) | 244 (79.74%) | 242 (64.53%) | 486 (71.37%) |
| Other | 115 (22.64%) | 80 (46.24%) | 62 (20.26%) | 133 (35.47%) | 196 (28.78%) |
| All | Young-Old | Old-Old | |||||
|---|---|---|---|---|---|---|---|
| Group | n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | F(p) 2 |
| All | 681 | 50.00 (10.05) | 508 | 49.49 (9.96) | 173 | 51.48 (10.21) | 7.044 (0.008) ** |
| Males | 306 | 48.69 (8.83) | 212 | 48.25 (8.25) | 94 | 49.68 (9.98) | 1.728 (0.190) |
| Females | 375 | 51.06 (10.85) | 296 | 50.38 (10.95) | 79 | 53.62 (10.13) | 5.802 (0.016) * |
| F (p) 1 | 9.759 (0.002) ** | 5.881 (0.015) * | 6.583 (0.011) * |
| Total | Males | Females | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | β (SE) | 95% CI | p | β (SE) | 95% CI | p | β (SE) | 95% CI | p |
| Gender | 1.63 (0.533) | (0.583, 2.677) | 0.002 ** | -- | -- | -- | -- | -- | -- |
| Age | 0.07 (0.036) | (−0.005, 0.135) | 0.071 | 0.06 (0.048) | (−0.034, 0.153) | 0.209 | 0.05 (0.053) | (−0.051, 0.157) | 0.317 |
| Education | −0.15 (0.175) | (−0.488, 0.197) | 0.404 | −0.31 (0.238) | (−0.782, 0.156) | 0.190 | −0.02 (0.250) | (−0.510, 0.474) | 0.943 |
| Income | −0.52 (0.543) | (−1.588, 0.544) | 0.337 | −0.98 (0.753) | (−2.465, 0.499) | 0.193 | −0.26 (0.764) | (−1.762, 1.241) | 0.733 |
| Marital/living status | −0.78 (0.600) | (−1.955, 0.400) | 0.195 | 1.11 (0.912) | (−0.684, 2.907) | 0.224 | −1.61 (0.804) | (−3.188, −0.027) | 0.046 * |
| Difficulty getting things done | 2.74 (0.449) | (1.861, 3.623) | 0.000 *** | 2.39 (0.628) | (1.150, 3.620) | 0.000 *** | 2.98 (0.626) | (1.753, 4.214) | 0.000 *** |
| Poor task | 12.00 (0.817) | (10.392, 13.601) | 0.000 *** | 11.44 (1.105) | (9.268, 13.618) | 0.000 *** | 12.12 (1.217) | (9.731, 14.517) | 0.000 *** |
| Sleeps more | 3.79 (0.678) | (2.459, 5.121) | 0.000 *** | 1.45 (0.903) | (−0.330, 3.224) | 0.110 | 5.51 (1.026) | (3.496, 7.530) | 0.000 *** |
| Lacks energy | 4.49 (0.406) | (3.689, 5.283) | 0.000 *** | 4.26 (0.580) | (3.117, 5.398) | 0.000 *** | 4.512 (0.559) | (3.413, 5.610) | 0.000 *** |
| Young-Old Adult | Old-Old Adult | |||||
|---|---|---|---|---|---|---|
| Variables | β (SE) | 95% CI | p | β (SE) | 95% CI | p |
| Gender | 1.46 (0.557) | (0.369, 2.556) | 0.009 ** | 2.52 (1.478) | (−0.406, 5.438) | 0.091 |
| Age | 0.09 (0.059) | (−0.024, 0.208) | 0.120 | 0.16 (0.177) | (−0.193, 0.509) | 0.375 |
| Education | −0.15 (0.182) | (−0.505, 0.211) | 0.421 | −0.38 (0.480) | (−1.329, 0.567) | 0.428 |
| Income | −1.17 (0.564) | (−2.275, −0.058) | 0.039 * | 1.95 (1.483) | (−0.985, 4.877) | 0.192 |
| Living status | −0.86 (0.663) | (−2.164, 0.440) | 0.194 | −0.35 (1.470) | (−3.258, 2.551) | 0.810 |
| Difficulty getting things done | 3.05 (0.484) | (2.100, 4.000) | 0.000 *** | 1.68 (1.133) | (−0.563, 3.916) | 0.141 |
| Poor task | 12.26 (0.916) | (10.457, 14.055) | 0.000 *** | 11.31 (1.889) | (7.573, 15.040) | 0.000 *** |
| Sleeps more | 3.61 (0.736) | (2.169, 5.059) | 0.000 *** | 3.87 (1.656) | (0.599, 7.145) | 0.021 * |
| Lacks energy | 4.90 (0.441) | (4.036, 5.767) | 0.000 *** | 3.49 (1.001) | (1.512, 5.467) | 0.000 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Q.; Sun, M.A.; Sun, Q.; Mei, H.; Rao, H.; Liu, J. Mental Fatigue Is Associated with Subjective Cognitive Decline among Older Adults. Brain Sci. 2023, 13, 376. https://doi.org/10.3390/brainsci13030376
Zhang Q, Sun MA, Sun Q, Mei H, Rao H, Liu J. Mental Fatigue Is Associated with Subjective Cognitive Decline among Older Adults. Brain Sciences. 2023; 13(3):376. https://doi.org/10.3390/brainsci13030376
Chicago/Turabian StyleZhang, Qianqian, McKenna Angela Sun, Qiuzi Sun, Hua Mei, Hengyi Rao, and Jianghong Liu. 2023. "Mental Fatigue Is Associated with Subjective Cognitive Decline among Older Adults" Brain Sciences 13, no. 3: 376. https://doi.org/10.3390/brainsci13030376