
Influence of Executive Function Training on BMI, Food Choice, and Cognition in Children with Obesity: Results from the TOuCH Study
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
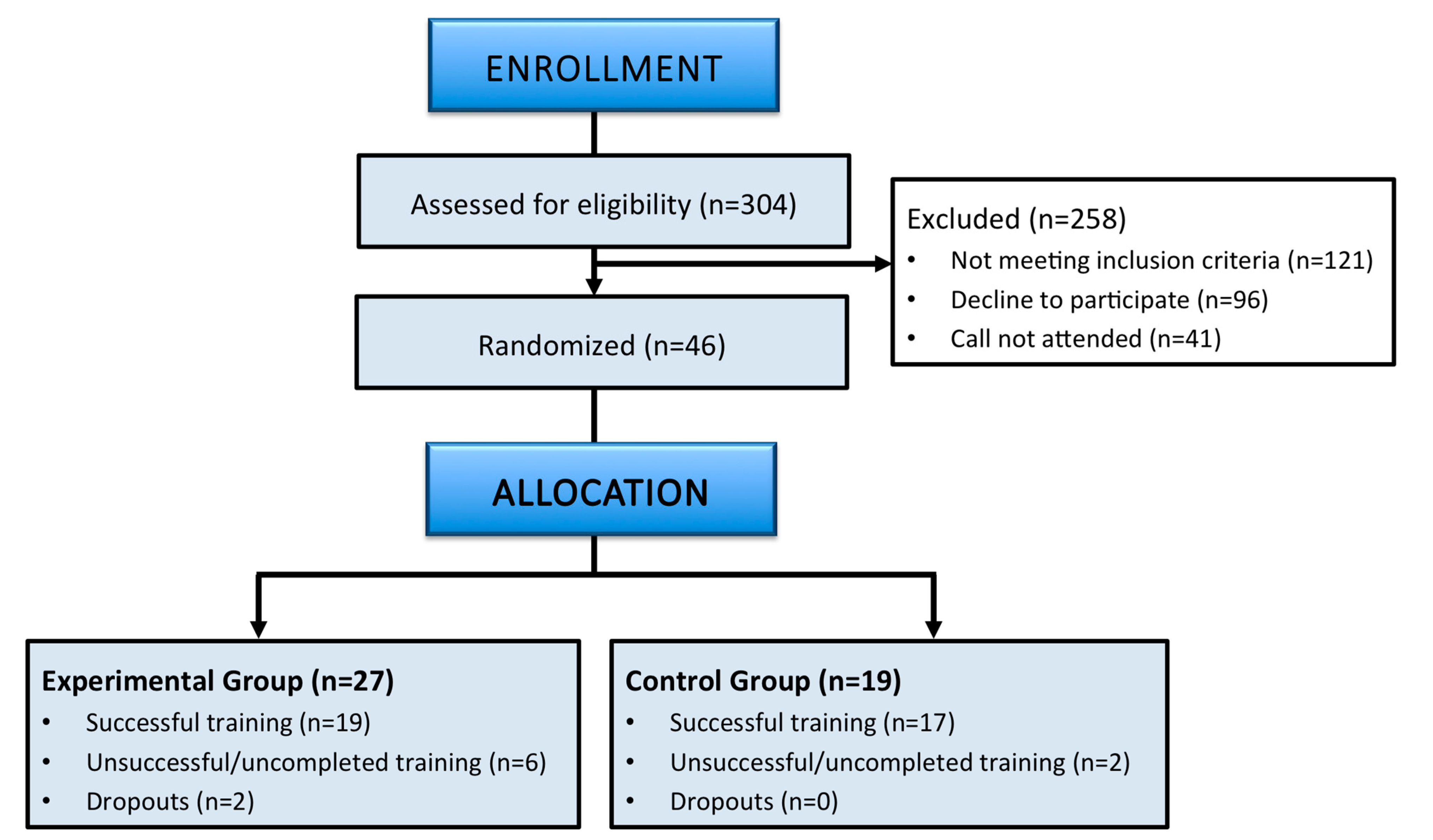
2.1. Study Design
2.2. Participants
Sample Size
2.3. Intervention
2.3.1. Cognitive Training
2.3.2. Psychoeducation and Food Register
2.3.3. Activity and Sleep Pattern Feedback
2.4. Outcomes
2.4.1. Pediatric Assessment
2.4.2. Neuropsychological Assessment
2.4.3. Rating Scales (Quality of Life, Emotional, and Behavioral Measures)
2.4.4. Food Choice
2.4.5. Physical Activity and Sleep Pattern
2.5. Statistical Analysis
3. Results
3.1. Effects of EF Training on Primary Outcomes
3.1.1. Cognition, Anthropometric Measures, and Food Choice
3.1.2. Evolution of Food Choice across Six-Week Training
3.2. Effects of EF Training on Secondary Outcomes: Post Hoc Analyses
3.2.1. Cognitive Subdomains
3.2.2. Rating Scales
3.2.3. Evolution of Healthy Habits (Physical Activity and Sleep Patterns)
3.3. Additional Analysis of Treatment Adherence
4. Discussion
4.1. Strengths and Limitations
4.2. Conclusions and Future Research
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Child Overweight and Obesity; World Health Organization: Geneva, Switzerland, 2023; Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 1 February 2023).
- Griffiths, L.J.; Parsons, T.J.; Hill, A.J. Self-esteem and quality of life in obese children and adolescents: A systematic review. Int. J. Pediatr. Obes. 2010, 5, 282–304. [Google Scholar] [CrossRef] [PubMed]
- Morrison, K.M.; Shin, S.; Tarnopolsky, M.; Taylor, V. Association of depression & health related quality of life with body composition in children and youth with obesity. J. Affect. Disord. 2015, 172, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Halfon, N.; Larson, K.; Slusser, W. Associations between Obesity and Comorbid Mental Health, Developmental, and Physical Health Conditions in a Nationally Representative Sample of US Children Aged 10 to 17. Acad. Pediatr. 2013, 13, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.R. Psychosocial Aspects of Obesity. NASN Sch. Nurse 2016, 31, 23–27. [Google Scholar] [CrossRef]
- Turk, M.W.; Yang, K.; Hravnak, M.; Sereika, S.M.; Ewing, L.J.; Burke, L.E. Randomized Clinical Trials of Weight Loss Maintenance: A review. J. Cardiovasc. Nurs. 2009, 24, 58–80. [Google Scholar] [CrossRef] [Green Version]
- Stice, E.; Burger, K.S.; Yokum, S. Reward Region Responsivity Predicts Future Weight Gain and Moderating Effects of the TaqIA Allele. J. Neurosci. 2015, 35, 10316–10324. [Google Scholar] [CrossRef] [Green Version]
- Townshend, T.; Lake, A. Obesogenic environments: Current evidence of the built and food environments. Perspect. Public Health 2017, 137, 38–44. [Google Scholar] [CrossRef] [Green Version]
- Higgs, S. Cognitive processing of food rewards. Appetite 2016, 104, 10–17. [Google Scholar] [CrossRef] [Green Version]
- Cortese, S.; Comencini, E.; Vincenzi, B.; Speranza, M.; Angriman, M. Attention-deficit/hyperactivity disorder and impairment in executive functions: A barrier to weight loss in individuals with obesity? BMC Psychiatry 2013, 13, 286. [Google Scholar] [CrossRef] [Green Version]
- Liang, J.; Matheson, B.E.; Kaye, W.H.; Boutelle, K.N. Neurocognitive correlates of obesity and obesity-related behaviors in children and adolescents. Int. J. Obes. 2014, 38, 494–506. [Google Scholar] [CrossRef] [Green Version]
- Berg, L.V.D.; Pieterse, K.; Malik, J.; Luman, M.; Van Dijk, K.W.; Oosterlaan, J.; Waal, H.A.D.-V.D. Association between impulsivity, reward responsiveness and body mass index in children. Int. J. Obes. 2011, 35, 1301–1307. [Google Scholar] [CrossRef] [Green Version]
- Stok, F.M.; de Vet, E.; Wardle, J.; Chu, M.T.; De Wit, J.; De Ridder, D.T.D. Navigating the obesogenic environment: How psychological sensitivity to the food environment and self-regulatory competence are associated with adolescent unhealthy snacking. Eat. Behav. 2015, 17, 19–22. [Google Scholar] [CrossRef] [PubMed]
- De Cock, N.; Van Lippevelde, W.; Vervoort, L.; Vangeel, J.; Maes, L.; Eggermont, S.; Braet, C.; Lachat, C.; Huybregts, L.; Goossens, L.; et al. Sensitivity to reward is associated with snack and sugar-sweetened beverage consumption in adolescents. Eur. J. Nutr. 2016, 55, 1623–1632. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Nicolo, M.; Yi, L.; Dunton, G.; Mason, T. Interactions among Reward Sensitivity and Fast-Food Access on Healthy Eating Index Scores in Adolescents: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 5744. [Google Scholar] [CrossRef] [PubMed]
- De Decker, A.; Verbeken, S.; Sioen, I.; Van Lippevelde, W.; Braet, C.; Eiben, G.; Pala, V.; Reish, L.A.; De Henauw, S. Palatable food consumption in children: Interplay between (food) reward motivation and the home food environment. Eur. J. Pediatr. 2017, 176, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Rollins, B.Y.; Loken, E.; Savage, J.S.; Birch, L.L. Maternal controlling feeding practices and girls’ inhibitory control interact to predict changes in BMI and eating in the absence of hunger from 5 to 7 y. Am. J. Clin. Nutr. 2014, 99, 249–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinert, K.R.S.; Po’E, E.K.; Barkin, S.L. The Relationship between Executive Function and Obesity in Children and Adolescents: A Systematic Literature Review. J. Obes. 2013, 2013, 820956. [Google Scholar] [CrossRef] [Green Version]
- Hayes, J.F.; Eichen, D.M.; Barch, D.M.; Wilfley, D.E. Executive function in childhood obesity: Promising intervention strategies to optimize treatment outcomes. Appetite 2018, 124, 10–23. [Google Scholar] [CrossRef]
- Luis-Ruiz, S.; Caldú, X.; Sánchez-Castañeda, C.; Pueyo, R.; Garolera, M.; Jurado, M. Is cognitive training an effective tool for improving cognitive function and real-life behaviour in healthy children and adolescents? A systematic review. Neurosci. Biobehav. Rev. 2020, 116, 268–282. [Google Scholar] [CrossRef]
- Simons, D.J.; Boot, W.R.; Charness, N.; Gathercole, S.E.; Chabris, C.F.; Hambrick, D.Z.; Stine-Morrow, E.A.L. Do “Brain-Training” Programs Work? Psychol. Sci. Public Interest 2016, 17, 103–186. [Google Scholar] [CrossRef]
- Verbeken, S.; Braet, C.; Goossens, L.; van der Oord, S. Executive function training with game elements for obese children: A novel treatment to enhance self-regulatory abilities for weight-control. Behav. Res. Ther. 2013, 51, 290–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verbeken, S.; Braet, C.; Naets, T.; Houben, K.; Boendermaker, W. Computer training of attention and inhibition for youngsters with obesity: A pilot study. Appetite 2018, 123, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Favieri, F.; Forte, G.; Casagrande, M. The Executive Functions in Overweight and Obesity: A Systematic Review of Neuropsychological Cross-Sectional and Longitudinal Studies. Front. Psychol. 2019, 10, 2126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varni, J.W.; Limbers, C.A.; Burwinkle, T.M. Impaired health-related quality of life in children and adolescents with chronic conditions: A comparative analysis of 10 disease clusters and 33 disease categories/severities utilizing the PedsQLTM 4.0 Generic Core Scales. Health Qual. Life Outcomes 2007, 5, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, T.E.; Landgraf, J.M. Improvements in Executive Function Correlate with Enhanced Performance and Functioning and Health-Related Quality of Life: Evidence from 2 Large, Double-Blind, Randomized, Placebo-Controlled Trials in ADHD. Postgrad. Med. 2010, 122, 42–51. [Google Scholar] [CrossRef]
- Davis, J.C.; Marra, C.A.; Najafzadeh, M.; Liu-Ambrose, T. The independent contribution of executive functions to health related quality of life in older women. BMC Geriatr. 2010, 10, 16. [Google Scholar] [CrossRef] [Green Version]
- Diamond, A. Executive Functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [Green Version]
- Tavares, J.V.T.; Clark, L.; Cannon, D.M.; Erickson, K.; Drevets, W.C.; Sahakian, B.J. Distinct Profiles of Neurocognitive Function in Unmedicated Unipolar Depression and Bipolar II Depression. Biol. Psychiatry 2007, 62, 917–924. [Google Scholar] [CrossRef]
- Sanchez-Castañeda, C.; Luis-Ruiz, S.; Ramon-Krauel, M.; Lerin, C.; Sanchez, C.; Miró, N.; Martínez, S.; Garolera, M.; Jurado, M.A. Executive Function Training in Childhood Obesity: Food Choice, Quality of Life, and Brain Connectivity (TOuCH): A Randomized Control Trial Protocol. Front. Pediatr. 2021, 9, 551869. [Google Scholar] [CrossRef]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [Green Version]
- Schulz, K.F.; Altman, U.G.; Moher, D.; CONSORT Group. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 340, c332. [Google Scholar] [CrossRef]
- Aksayli, N.D.; Sala, G.; Gobet, F. The cognitive and academic benefits of Cogmed: A meta-analysis. Educ. Res. Rev. 2019, 27, 229–243. [Google Scholar] [CrossRef]
- Siberski, J.; Shatil, E.; Siberski, C.; Eckroth-Bucher, M.; French, A.; Horton, S.; Loefflad, R.F.; Rouse, P. Computer-Based Cognitive Training for Individuals with Intellectual and Developmental Disabilities: Pilot study. Am. J. Alzheimer’s Dis. Other Dement. 2014, 30, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Verghese, J.; Mahoney, J.; Ambrose, A.F.; Wang, C.; Holtzer, R. Effect of Cognitive Remediation on Gait in Sedentary Seniors. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2010, 65, 1338–1343. [Google Scholar] [CrossRef] [Green Version]
- Serra Majem, L.; Ribas Barba, L.; Ngo de la Cruz, J.; Ortega Anta, R.M.; Pérez Rodrigo, C.; Aranceta Bartrina, J. Alimentación, jóvenes y dieta mediterránea en España. In Desarrollo del KIDMED, Índice de Calidad de la Dieta Mediterránea en la Infancia y la Adolescencia, Alimentación Infantil y Juvenil; Serra Majem, L., Aranceta Bartrina, J., Eds.; Masson: Paris, France; Barcelona, Spain, 2004; pp. 51–59. [Google Scholar]
- Wechsler, D. Wechsler Intelligence Scale for Children, 5th ed.; Spanish Version; Pearson: San Antonio, TX, USA; Madrid, Spain, 2015. [Google Scholar]
- Wechsler, D.; Naglieri, J.A. Weschler No Verbal, Spanish Version; Pearson: San Antonio, TX, USA; Madrid, Spain, 2011. [Google Scholar]
- Llorente, A.M.; Williams, J.; Satz, P.; D’Elia, L.F. Children’s Color Trails Test; PAR, Psychological Assessment Resources Inc.: Lutz, FL, USA, 2003. [Google Scholar]
- Sedó, M.A. Five Digit Test, Spanish Version; TEA Ediciones SA: Madrid, Spain, 2007. [Google Scholar]
- Conners, C.K. Continuous Performance Test (CPT3); MHS Multi-Health Systems Inc.: Toronto, ON, Canada, 2014. [Google Scholar]
- Gelonch, O.; Garolera, M.; Valls, J.; Rosselló, L.; Pifarré, J. Executive function in fibromyalgia: Comparing subjective and objective measures. Compr. Psychiatry 2016, 66, 113–122. [Google Scholar] [CrossRef] [Green Version]
- Mueller, S.T.; Piper, B.J. The Psychology Experiment Building Language (PEBL) and PEBL Test Battery. J. Neurosci. Methods 2014, 222, 250–259. [Google Scholar] [CrossRef] [Green Version]
- Shallice, T. Specific impairments of planning. Philos. Trans. R. Soc. Lond. B Biol. Sci. 1982, 298, 199–209. [Google Scholar] [CrossRef]
- Gioia, G.A.; Isquith, P.K.; Guy, S.C.; Kenworthy, L. BRIEF 2, Spanish Version; TEA Ediciones SA: Madrid, Spain, 2015. [Google Scholar]
- Varni, J.W.; Seid, M.; Rode, C.A. The PedsQL™: Measurement Model for the Pediatric Quality of Life Inventory. Med. Care 1999, 37, 126–139. [Google Scholar] [CrossRef]
- Harter, S.; Broc, M.A. Perfil de Autoconcepto, Autoestima, y Apoyo Social Para Adolescentes; COSPA: Madrid, Spain, 2000. [Google Scholar]
- Achenbach, T.M. Child Behaviour Checklist, Spanish Version. 2001. Available online: www.aseba.org (accessed on 10 January 2021).
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle Nyström, C.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef]
- Mooses, K.; Oja, M.; Reisberg, S.; Vilo, J.; Kull, M. Validating Fitbit Zip for monitoring physical activity of children in school: A cross-sectional study. BMC Public Health 2018, 18, 858. [Google Scholar] [CrossRef] [Green Version]
- Diamond, A.; Ling, D.S. Conclusions about interventions, programs, and approaches for improving executive functions that appear justified and those that, despite much hype, do not. Dev. Cogn. Neurosci. 2016, 18, 34–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Shields, G.S.; Wu, Q.; Liu, Y.; Chen, H.; Guo, C. Cognitive training on eating behaviour and weight loss: A meta-analysis and systematic review. Obes. Rev. 2019, 20, 1628–1641. [Google Scholar] [CrossRef] [PubMed]
- Siddique, N.; Dhakan, P.; Rano, I.; Merrick, K. A Review of the Relationship between Novelty, Intrinsic Motivation and Rein-forcement Learning. Paladyn. J. Behav. Robot. 2017, 8, 58–69. [Google Scholar] [CrossRef] [Green Version]
- Melby-Lervåg, M.; Redick, T.S.; Hulme, C. Working Memory Training Does Not Improve Performance on Measures of Intelligence or Other Measures of “Far Transfer” evidence from a meta-analytic review. Perspect. Psychol. Sci. 2016, 11, 512–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunning, D.L.; Holmes, J.; Gathercole, S. Does working memory training lead to generalized improvements in children with low working memory? A randomized controlled trial. Dev. Sci. 2013, 16, 915–925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epreiss, M.; Eshatil, E.; Ecermakova, R.; Ecimermannova, D.; Ram, I. Personalized Cognitive Training in Unipolar and Bipolar Disorder: A Study of Cognitive Functioning. Front. Hum. Neurosci. 2013, 7, 108. [Google Scholar] [CrossRef] [Green Version]
- Broadbent, D.E.; Cooper, P.F.; FitzGerald, P.; Parkes, K.R. The Cognitive Failures Questionnaire (CFQ) and its correlates. Br. J. Clin. Psychol. 1982, 21, 1–16. [Google Scholar] [CrossRef]
- Moritz, S.; Ferahli, S.; Naber, D. Memory and attention performance in psychiatric patients: Lack of correspondence between clinician-rated and patient-rated functioning with neuropsychological test results. Neuropsychol. Soc. 2004, 10, 623–633. [Google Scholar] [CrossRef]
- National Center for Health Statistics. Clinical Growth Charts. 2017. Available online: https://www.cdc.gov/growthcharts/clinical_charts.htm (accessed on 3 January 2021).
- De Voogd, E.; Wiers, R.; Prins, P.; de Jong, P.; Boendermaker, W.; Zwitser, R.; Salemink, E. Online attentional bias modification training targeting anxiety and depression in unselected adolescents: Short- and long-term effects of a randomized controlled trial. Behav. Res. Ther. 2016, 87, 11–22. [Google Scholar] [CrossRef] [Green Version]
- Hitchcock, C.; Westwell, M.S. A cluster-randomised, controlled trial of the impact of Cogmed Working Memory Training on both academic performance and regulation of social, emotional and behavioural challenges. J. Child Psychol. Psychiatry 2017, 58, 140–150. [Google Scholar] [CrossRef]
- Roberts, G.; Quach, J.; Spencer-Smith, M.; Anderson, P.J.; Gathercole, S.; Gold, L.; Sia, K.-L.; Mensah, F.; Rickards, F.; Ainley, J.; et al. Academic Outcomes 2 Years after Working Memory Training for Children with Low Working Memory. JAMA Pediatr. 2016, 170, e154568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diao, H.; Wang, H.; Yang, L.; Li, T. The impacts of multiple obesity-related interventions on quality of life in children and adolescents: A randomized controlled trial. Health Qual. Life Outcomes 2020, 18, 213. [Google Scholar] [CrossRef] [PubMed]
- Melby-Lervåg, M.; Hulme, C. Is working memory training effective? A meta-analytic review. Dev. Psychol. 2013, 49, 270–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ball, G.D.C.; Sebastianski, M.; Wijesundera, J.; Keto-Lambert, D.; Ho, J.; Zenlea, I.; Perez, A.; Nobles, J.; Skelton, J.A. Strategies to reduce attrition in managing paediatric obesity: A systematic review. Pediatr. Obes. 2020, 16, e12733. [Google Scholar] [CrossRef]
- Dhaliwal, J.; Nosworthy, N.M.; Holt, N.; Zwaigenbaum, L.; Avis, J.L.; Rasquinha, A.; Ball, G.D. Attrition and the Management of Pediatric Obesity: An Integrative Review. Child. Obes. 2014, 10, 461–473. [Google Scholar] [CrossRef] [Green Version]
- Skelton, J.A.; Beech, B.M. Attrition in paediatric weight management: A review of the literature and new directions. Obes. Rev. 2011, 12, e273–e281. [Google Scholar] [CrossRef]
- Chacko, A.; Feirsen, N.; Bedard, A.-C.; Marks, D.; Uderman, J.Z.; Chimiklis, A. Cogmed Working Memory Training for Youth with ADHD: A Closer Examination of Efficacy Utilizing Evidence-Based Criteria. J. Clin. Child Adolesc. Psychol. 2013, 42, 769–783. [Google Scholar] [CrossRef] [Green Version]
- Althubaiti, A. Information bias in health research: Definition, pitfalls, and adjustment methods. J. Multidiscip. Healthc. 2016, 9, 211–217. [Google Scholar] [CrossRef] [Green Version]
- Ross, E.; Ray, C.; Stoor, C. Measuring children’s health behaviours, comparing answers from 10–11 years old children and their parents. In Proceedings of the 7th International Conference on Diet and Activity Methods (4–7 June 2009); National Cancer Institute: Washington, DC, USA, 2009; pp. 305–306. [Google Scholar]


{kind=link}
| Experimental Group | Control Group | Group Comparison | ||||||
|---|---|---|---|---|---|---|---|---|
| N | Mean | SD | N | Mean | SD | T/U | Sig. | |
| Age (years) | 19 | 10.32 | 1.108 | 17 | 10.65 | 0.93 | 130.500 | 0.302 |
| BMI (percentile) | 19 | 98.63 | 0.83 | 17 | 98.52 | 0.76 | −0.437 | 0.665 |
| Physical activity (hours) | 19 | 2.72 | 1.81 | 17 | 3.21 | 4.38 | 147.500 | 0.652 |
| Visual IQ (scalar score) | 19 | 10.68 | 2.31 | 17 | 10.35 | 2.15 | 135.500 | 0.403 |
| Verbal IQ (scalar score) | 19 | 11.42 | 2.80 | 17 | 10.76 | 2.25 | −0.770 | 0.447 |
| Motivation for treatment | 19 | 6.31 | 0.749 | 16 | 6.63 | 0.719 | 114.000 | 0.217 |
| N | N | X2 | Sig. | |||||
| Sex (F:M) | 5:14 | 8:9 | 1.673 | 0.196 | ||||
| Handedness (R:L) | 18:1 | 15:2 | - | 0.593 † | ||||
| Economic income (I:II:III:IV:V) | 6:7:1:2:1 | 3:3:4:4:0 | 5.485 | 0.219 †† | ||||
| Hospital (CST: SJD) | 14:5 | 12:5 | .043 | 0.836 | ||||
| Main Effects | Group-by-Time Interaction | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (a) Pre-Post Primary Outcomes | n | Pre-Test | Post-Test | Group | Time | |||||||
| Mean | (SD) | Mean (SD) | F (df); p | ηp2 | F (df); p | ηp2 | F (df); p | ηp2 | ||||
| Cognition (z score) | EG | 19 | 0.054 (0.430) | 0.107 (0.457) | F(1,34) = 1.50; 0.229 | 0.042 | F(1,34) = 0.004; 0.949 | 0.000 | F(1,34) = 1.22; 0.277 | 0.035 | ||
| CG | 17 | −0.061 (0.444) | −0.121 (0.453) | |||||||||
| BMI | EG | 19 | 29.29 (3.18) | 28.75 (2.99) | F(1,34) = 0.19; 0.662 | 0.006 | F(1,34) = 8.81; 0.005 | 0.206 | F(1,34) = 0.72; 0.402 | 0.021 | ||
| CG | 17 | 29.70 (4.22) | 29.40 (4.11) | |||||||||
| WC | EG | 19 | 91.94 (9.18) | 89.60 (7.87) | F(1,33) = 0.22; 0.640 | 0.007 | F(1,33) = 8.22; 0.007 | 0.199 | F(1,33) = 2.60; 0.116 | 0.073 | ||
| CG | 16 | 92.53 (9.57) | 91.44 (9.66) | |||||||||
| Kidmed | EG | 16 | 7.11 (1.88) | 6.13 (1.86) | F(1,29) = 0.00; 0.964 | 0.000 | F(1,29) = 1.19; 0.284 | 0.040 | F(1,29) = 2.21; 0.148 | 0.071 | ||
| CG | 15 | 6.71 (2.02) | 6.60 (2.19) | |||||||||
| (b) Six-Week Training Primary Outcomes† | Fixed Effects | Random Effects | Model Fit | |||||||||
| Est/Beta | SE | t | p | Param. | Covariance | SE | Sig. | AIC/BIC | ||||
| Kidmed Modified †† | Intercept | 4.559 | 0.598 | 3.328 to 5.792 | 7.620 | 0.000 | Residual | 1.804 | 0.258 | 0.000 | 592.548/ | |
| Group | −0.899 | 0.989 | −2.923 to 1.131 | −0.908 | 0.372 | Intercept + Time | 604.590 | |||||
| Time | −0.926 | 0.427 | −1.806 to −0.045 | −2.166 | 0.040 | [subject] UN (1,1) | 4.690 | 1.831 | 0.010 | |||
| Group x time | 0.387 | 0.715 | −1.079 to 1.853 | 0.541 | 0.593 | UN (2,1) | −2.335 | 1.228 | 0.057 | |||
| UN (2,2) | 1.391 | 0.954 | 0.145 | |||||||||
| Main Effects | Group by Time Interaction | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | Pre-Test | Post-Test | Group | Time | ||||||
| Mean (SD) | Mean (SD) | F (df); p | ηp2 | F (df); p | ηp2 | F (df); p | ηp2 | |||
| Cognitive Domains | ||||||||||
| Attention and Speed | ||||||||||
| WISC-V Digit Span | EG | 19 | 5.63 (1.38) | 5.63 (0.90) | F(1,34) = 0.61; 0.439 | 0.018 | F(1,34) = 0.51; 0.480 | 0.015 | F(1,34) = 0.51; 0.480 | 0.015 |
| Forward | CG | 17 | 5.29 (0.77) | 5.53 (0.62) | ||||||
| WNV Spatial Span | EG | 19 | 5.74 (1.15) | 6.47 (1.02) | F(1,34) = 0.87; 0.357 | 0.025 | F(1,34) = 6.76; 0.014 | 0.166 | F(1,34) = 0.84; 0.366 | 0.024 |
| Forward | CG | 17 | 5.65 (1.22) | 6.00 (1.00) | ||||||
| CCTT Part I Time | EG | 19 | 25.89 (11.16) | 22.37 (8.93) | F(1,34) = 0.08; 0.781 | 0.002 | F(1,34) = 4.12; 0.050 | 0.108 | F(1,34) = 0.29; 0.597 | 0.008 |
| CG | 17 | 24.29 (9.98) | 22.24 (10.45) | |||||||
| FDT Reading Time | EG | 19 | 25.79 (4.21) | 24.42 (4.06) | F(1,34) = 0.34; 0.562 | 0.010 | F(1,34) = 6.76; 0.014 | 0.166 | F(1,34) = 0.54; 0.467 | 0.016 |
| CG | 17 | 26.29 (4.40) | 25.53 (4.58) | |||||||
| FDT Counting Time | EG | 19 | 33.05 (5.67) | 30.68 (5.00) | F(1,34) = 0.92; 0.343 | 0.026 | F(1,34) = 17.85; 0.000 * | 0.344 | F(1,34) = 0.25; 0.622 | 0.007 |
| CG | 17 | 35.06 (6.12) | 32.06 (5.63) | |||||||
| CPT Detectability | EG | 19 | 55.00 (9.32) | 53.79 (8.69) | F(1,34) = 0.39; 0.535 | 0.011 | F(1,34) = 1.98; 0.168 | 0.055 | F(1,34) = 0.01; 0.915 | 0.000 |
| CG | 17 | 56.94 (9.22) | 55.53 (9.72) | |||||||
| CPT Omissions | EG | 19 | 49.32 (6.79) | 51.00 (7.89) | F(1,34) = 3.75; 0.061 | 0.099 | F(1,34) = 1.45; 0.231 | 0.042 | F(1,34) = 0.04; 0.853 | 0.001 |
| CG | 17 | 54.47 (9.25) | 56.76 (14.03) | |||||||
| CPT Reaction Time | EG | 19 | 47.42 (6.44) | 49.68 (8.37) | F(1,34) = 1.15; 0.291 | 0.033 | F(1,34) = 12.03; 0.001 * | 0.261 | F(1,34) = 2.03; 0.164 | 0.056 |
| CG | 17 | 48.76 (7.09) | 54.18 (12.37) | |||||||
| Working Memory | ||||||||||
| WISC-V Digit Span | EG | 19 | 4.42 (0.84) | 4.74 (0.81) | F(1,34) = 2.97; 0.094 | 0.080 | F(1,34) = 0.69; 0.412 | 0.020 | F(1,34) = 0.69; 0.412 | 0.020 |
| Backward | CG | 17 | 4.18 (1.02) | 4.18 (0.95) | ||||||
| WNV Spatial Span | EG | 19 | 5.21 (0.71) | 6.16 (1.07) | F(1,34) = 1.72; 0.199 | 0.048 | F(1,34) = 6.73; 0.014 | 0.165 | F(1,34) = 5.25; 0.028 | 0.134 |
| Backward | CG | 17 | 5.29 (1.21) | 5.35 (0.99) | ||||||
| N-Back (1-back) | EG | 19 | 5.08 (1.00) | 4.84 (1.28) | F(1,34) = 0.10; 0.758 | 0.003 | F(1,34) = 0.11; 0.741 | 0.003 | F(1,34) = 0.98; 0.328 | 0.028 |
| CG | 17 | 5.00 (1.16) | 5.12 (0.84) | |||||||
| N-Back (2-back) | EG | 19 | 4.26 (1.33) | 4.29 (1.84) | F(1,34) = 0.39; 0.538 | 0.011 | F(1,34) = 5.06; 0.031 | 0.129 | F(1,34) = 4.55; 0.041 | 0.118 |
| CG | 17 | 4.06 (1.58) | 5.03 (0.79) | |||||||
| N-Back (3-back) | EG | 19 | 3.08 (0.93) | 3.13 (1.36) | F(1,34) = 0.02; 0.894 | 0.001 | F(1,34) = 0.15; 0.703 | 0.004 | F(1,34) = 0.02; 0.884 | 0.001 |
| CG | 17 | 3.09 (1.08) | 3.21 (1.15) | |||||||
| Cognitive Flexibility | ||||||||||
| CCTT Part II Time | EG | 19 | 49.16 (14.24) | 41.68 (11.02) | F(1,34) = 0.14; 0.715 | 0.004 | F(1,34) = 10.23; 0.003 * | 0.231 | F(1,34) = 0.26; 0.612 | 0.008 |
| CG | 17 | 49.35 (11.94) | 43.94 (8.31) | |||||||
| FDT Shifting Time | EG | 19 | 62.89 (12.77) | 54.63 (12.33) | F(1,34) = 0.00; 0.955 | 0.000 | F(1,34) = 61.02; 0.000 * | 0.642 | F(1,34) = 0.18; 0.667 | 0.006 |
| CG | 17 | 63.59 (10.60) | 54.35 (9.31) | |||||||
| Inhibitory Control | ||||||||||
| FDT Choosing Time | EG | 19 | 56.42 (11.99) | 49.79 (9.03) | F(1,34) = 0.06; 0.809 | 0.002 | F(1,34) = 39.74; 0.000 * | 0.539 | F(1,34) = 0.17; 0.685 | 0.005 |
| CG | 17 | 56.76 (7.60) | 50.94 (9.20) | |||||||
| GNG Correct | EG | 19 | 214.58 (20.88) | 226.68 (16.95) | F(1,32) = 1.25; 0.272 | 0.038 | F(1,32) = 6.65; 0.015 | 0.172 | F(1,32) = 0.16; 0.686 | 0.005 |
| Responses | CG | 15 | 210.00 (30.74) | 216.06 (19.09) | ||||||
| GNG | EG | 19 | 32.89 (19.42) | 24.26 (13.89) | F(1,32) = 0.051; 0.823 | 0.002 | F(1,32) = 15.56; 0.000 * | 0.327 | F(1,32) = 0.02; 0.895 | 0.001 |
| Commissions | CG | 15 | 33.25 (13.62) | 27.75 (15.84) | ||||||
| Planning | ||||||||||
| ToL Total Move | EG | 19 | 38.26 (15.19) | 31.11 (15.59) | F(1,34) = 0.01; 0.947 | 0.000 | F(1,34) = 2.14; 0.152 | 0.059 | F(1,34) = 0.17; 0.681 | 0.005 |
| CG | 17 | 36.41 (24.21) | 32.41 (7.47) | |||||||
| ToL Total Time | EG | 19 | 304.16 (117.94) | 227.21 (106.61) | F(1,34) = 0.01; 0.912 | 0.000 | F(1,34) = 7.98; 0.008 | 0.190 | F(1,34) = 0.06; 0.806 | 0.002 |
| CG | 18 | 302.18 (207.86) | 237.65 (86.45) | |||||||
| Main Effects Group Time | Group-by-Time Interaction | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (a) Rating Scales (Raw Score) | n | Pre-Test | Post-Test | F (df); p | ηp2 | F (df); p | ηp2 | F (df); p | ηp2 | |||
| BRIEF-2 | 19 | 52.74 (13.59) | 49.79 (14.37) | F(1,34) = 0.05; 0.820 | 0.002 | F(1,34) = 9.94; 0.003 * | 0.226 | F(1,34) = 0.53; 0.474 | 0.015 | |||
| Cognitive | 17 | 52.65 (13.65) | 47.94 (10.58) | |||||||||
| 19 | 25.68 (5.86) | 24.11 (5.20) | F(1,34) = 0.04; 0.840 | 0.001 | F(1,34) = 5.26; 0.028 | 0.134 | F(1,34) = 0.31; 0.582 | 0.009 | ||||
| Emotional | 17 | 26.53 (6.29) | 23.94 (5.49) | |||||||||
| 19 | 19.16 (5.98) | 17.32 (5.46) | F(1,34) = 0.01; 0.907 | 0.000 | F(1,34) = 5.46; 0.026 | 0.138 | F(1,34) = 0.17; 0.686 | 0.005 | ||||
| Behavioral | 17 | 18.71 (3.97) | 17.41 (3.95) | |||||||||
| PedsQl | 19 | 76.72 (11.94) | 81.64 (11.19) | F(1,34) = 0.00; 0.953 | 0.000 | F(1,34) = 4.80; 0.035 | 0.124 | F(1,34) = 0.33; 0.570 | 0.010 | |||
| Child’s Total Score | 17 | 77.94 (12.78) | 80.81 (10.49) | |||||||||
| 19 | 73.92 (11.46) | 79.29 (13.18) | F(1,34) = 0.56; 0.461 | 0.016 | F(1,32) = 2.05; 0.162 | 0.057 | F(1,34) = 0.86; 0.361 | 0.025 | ||||
| Parents’ Total Score | 17 | 72.72 (16.35) | 73.87 (18.48) | |||||||||
| SPPC | 18 | 20.50 (3.70) | 21.74 (2.40) | F(1,30) = 0.72; 0.402 | 0.023 | F(1,31) = 10.80; 0.003 * | 0.258 | F(1,31) = 1.15; 0.292 | 0.036 | |||
| Self-Esteem | 15 | 18.93 (4.98) | 21.82 (2.38) | |||||||||
| 18 | 21.25 (2.71) | 21.64 (2.92) | F(1,30) = 0.17; 0.680 | 0.006 | F(1,30) = 4.18; 0.050 | 0.122 | F(1,30) = 0.00; 0.948 | 0.000 | ||||
| Social Support | 14 | 20.91 (2.70) | 21.16 (1.98) | |||||||||
| CBCL | 19 | 7.53 (4.11) | 6.00 (4.64) | F(1,34) = 4.09; 0.051 | 0.107 | F(1,34) = 5.65; 0.023 | 0.142 | F(1,34) = 0.08; 0.778 | 0.002 | |||
| Internalizing Symptoms | 17 | 11.30 (5.73) | 9.35 (7.89) | |||||||||
| 19 | 7.53 (6.25) | 6.31 (6.40) | F(1,34) = 0.11; 0.748 | 0.003 | F(1,34) = 4.74; 0.037 | 0.122 | F(1,34) = 0.02; 0.904 | 0.000 | ||||
| Externalizing Symptoms | 17 | 8.18 (4.45) | 6.82 (4.98) | |||||||||
| (b) Six-Week Training Secondary Outcomes† | Fixed Effects | Random Effects | Model Fit | |||||||||
| Est/Beta | SE | 95% CI | t | p | Param. | Covariance | SE | Sig. | AIC/BIC | |||
| Daily Steps Sleep Time (min.) | Intercept | 13,414.78 | 800.83 | 11,777.28 to 15,052.27 | 16.75 | 0.000 | Residual Intercept + Time (subject) UN (1,1) UN (2,1) UN (2,2) Residual Intercept + Time (subject) UN (1,1) UN (2,1) UN (2,2) | 4,433,933.35 | 581,326.30 | 0.000 | 3378.48/ | |
| Group | −1357.17 | 1207.205 | −3821.22 to 1106.88 | 0.112 | 0.270 | 3391.25 | ||||||
| Time | −230.94 | 50.32 | −1357.39 to 895.50 | −4.20 | 0.678 | 7,852,777.77 | 3,225,415.08 | 0.015 | ||||
| Group x time | 9.04 | 847.63 | −1723.23 to 1741.32 | 0.011 | 0.992 | 1,263,820.19 | 1,682,233.75 | 0.452 | ||||
| 1,193,283.55 | 1,579,116.74 | 0.450 | ||||||||||
| Intercept | 494.91 | 8.73 | 477.122 to 512.69 | 56.66 | 0.000 | 792.493 | 105.84 | 0.000 | 1700.26/ | |||
| Group | −1.68 | 13.18 | −28.525 to 25.16 | −0.13 | 0.899 | 1712.83 | ||||||
| Time | −18.151 | 7.416 | −33.242 to -3.06 | −2.45 | 0.020 | 656.081 | 369.28 | 0.076 | ||||
| Group x time | −0.67 | 11.09 | −23.242 to 21.92 | −0.06 | 0.95 | −165.994 | 270.63 | 0.540 | ||||
| 3 | 167.384 | 259.45 | 0.519 | |||||||||
| Completers | Non-Completers | Group Comparison | ||||
|---|---|---|---|---|---|---|
| Accomplishment | N | % | N | % | ||
| EG | 19 | 70.37% | 8 | 29.63% | 0.160 † | |
| CG | 17 | 89.17% | 2 | 10.53% | ||
| Individual Characteristics at Baseline | ||||||
| N | Mean (SD) | N | (SD) | X/T/U | p | |
| Sex (M: F) | 23:13 | - | 4:6 | - | 1.842 | 0.175 |
| Age (years) | 36 | 10.47 (1.03) | 10 | 11.00 (0.816) | 125.500 | 0.128 |
| BMI (percentile) | 36 | 98.58 (0.789) | 10 | 98.32 (0.853) | 0.89 | 0.380 |
| WC (cm) | 35 | 92.21 (9.23) | 10 | 92.55 (14.01) | −0.09 | 0.928 |
| Kidmed (raw score) | 35 | 6.91 (1.93) | 10 | 6.50 (1.96) | 146.000 | 0.420 |
| Physical activity (hours) | 36 | 2.95 (3.24) | 8 | 0.38 (1.06) | 52.000 | 0.004 |
| Daily screen time(hours) | 36 | 2.14 (1.15) | 8 | 2.39 (1.31) | 120.500 | 0.469 |
| Visual IQ (scalar score) | 36 | 10.53 (2.21) | 10 | 8.30 (1.83) | 2.92 | 0.006 |
| Verbal IQ (scalar score) | 36 | 11.11 (2.54) | 10 | 10.30 (2.87) | 0.868 | 0.389 |
| Motivation for treatment | 35 | 6.48 (0.741) | 8 | 5.75 (1.035) | 82.500 | 0.048 |
| Economic income | 31 | 2.35 (1.19) | 8 | 3.25 (1.58) | 81.000 | 0.124 |
| WISC-V | ||||||
| Digit span forward | 36 | 5.47 (1.13) | 10 | 5.40 (0.84) | 171.500 | 0.799 |
| Digit span backward | 36 | 4.31 (0.92) | 10 | 4.10 (0.74) | 160.500 | 0.581 |
| WNV | ||||||
| Spatial span forward | 36 | 5.69 (1.17) | 10 | 5.50 (1.08) | 162.000 | 0.619 |
| Spatial span backward | 36 | 5.25 (0.97) | 10 | 5.00 (1.70) | 170.500 | 0.791 |
| ToL | ||||||
| Total move | 36 | 37.39 (19.68) | 10 | 33.60 (15.78) | 179.000 | 0.979 |
| Total time | 36 | 303.22 (164.03) | 10 | 328.20 (113.25) | 130.500 | 0.187 |
| CCTT | ||||||
| Part I-seconds | 36 | 25.14 (10.50) | 10 | 30.80 (17.07) | 145.500 | 0.358 |
| Part II-seconds | 36 | 49.25 (13.02) | 10 | 55.20 (14.43) | 137.000 | 0.252 |
| FDT | ||||||
| Reading | 36 | 26.03 (4.24) | 10 | 26.40 (4.86) | −0.238 | 0.813 |
| Counting | 36 | 34.00 (5.89) | 10 | 36.50 (8.07) | −1.093 | 0.280 |
| Choosing | 36 | 56.58 (10.02) | 10 | 57.70 (8.51) | 162.500 | 0.641 |
| Shifting | 63.22 (11.64) | 10 | 68.90 (15.92) | 142.000 | 0.311 | |
| CPT (T-score) | ||||||
| Detectability | 36 | 55.92 (9.19) | 10 | 57.50 (5.74) | 176.500 | 0.926 |
| Omissions | 36 | 51.75 (8.34) | 10 | 50.60 (6.52) | 177.000 | 0.936 |
| Hit reaction time | 36 | 48.06 (6.69) | 10 | 50.80 (9.09) | −1.059 | 0.205 |
| N-back Correct responses | ||||||
| 1-back | 36 | 5.01 (1.06) | 10 | 4.60 (1.47) | 148.500 | 0.388 |
| 2-back | 36 | 4.17 (1.43) | 10 | 3.70 (1.36) | 143.500 | 0.327 |
| 3-back | 36 | 3.08 (0.99) | 10 | 3.10 (1.05) | −0.047 | 0.963 |
| Go–No Go | ||||||
| Correct responses | 35 | 212.49 (25.56) | 10 | 214.00 (20.07) | 172.500 | 0.946 |
| Commissions | 35 | 33.06 (16.78) | 10 | 34.10 (14.07) | 167.000 | 0.827 |
| BRIEF-2 | ||||||
| Cognitive | 36 | 52.69 (13.42) | 10 | 51.40 (13.22) | 0.271 | 0.788 |
| Emotional | 36 | 26.08 (5.99) | 10 | 25.20 (5.53) | 0.419 | 0.677 |
| Behavioral | 36 | 18.94 (5.07) | 10 | 17.70 (4.86) | 154.000 | 0.487 |
| PedsQl | ||||||
| Child’s total score | 36 | 77.29 (12.18) | 10 | 68.95 (12.10) | 113.500 | 0.076 |
| Parents’ total score | 36 | 73.36 (13.79) | 10 | 70.21 (15.50) | 0.622 | 0.537 |
| SPPC | ||||||
| Global self-esteem | 33 | 19.79 (4.33) | 10 | 17.60 (5.27) | 117.000 | 0.164 |
| Social support | 33 | 21.10 (2.66) | 10 | 19.09 (3.34) | 101.500 | 0.083 |
| CBCL | ||||||
| Internalizing symptoms | 36 | 9.30 (5.23) | 10 | 10.80 (6.91) | 163.000 | 0.650 |
| Externalizing symptoms | 36 | 7.83 (5.41) | 10 | 6.70 (4.55) | 0.605 | 0.548 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luis-Ruiz, S.; Sánchez-Castañeda, C.; Garolera, M.; Miserachs-González, S.; Ramon-Krauel, M.; Lerin, C.; Sanchez, C.; Miró, N.; Martínez, S.; Jurado, M.A. Influence of Executive Function Training on BMI, Food Choice, and Cognition in Children with Obesity: Results from the TOuCH Study. Brain Sci. 2023, 13, 346. https://doi.org/10.3390/brainsci13020346
Luis-Ruiz S, Sánchez-Castañeda C, Garolera M, Miserachs-González S, Ramon-Krauel M, Lerin C, Sanchez C, Miró N, Martínez S, Jurado MA. Influence of Executive Function Training on BMI, Food Choice, and Cognition in Children with Obesity: Results from the TOuCH Study. Brain Sciences. 2023; 13(2):346. https://doi.org/10.3390/brainsci13020346
Chicago/Turabian StyleLuis-Ruiz, Sandra, Cristina Sánchez-Castañeda, Maite Garolera, Sara Miserachs-González, Marta Ramon-Krauel, Carles Lerin, Consuelo Sanchez, Núria Miró, Sònia Martínez, and Maria Angeles Jurado. 2023. "Influence of Executive Function Training on BMI, Food Choice, and Cognition in Children with Obesity: Results from the TOuCH Study" Brain Sciences 13, no. 2: 346. https://doi.org/10.3390/brainsci13020346