

Associations between Autonomic Function and Cognitive Performance among Patients with Cerebral Small Vessel Disease
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject Recruitment
2.2. HRV Assessments
2.3. Clinical and Cognitive Function Assessment
2.4. Brain MRI Acquisition and Assessment
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics of Patients
3.2. Univariate Comparisons of HRV According to Different Cognitive Function
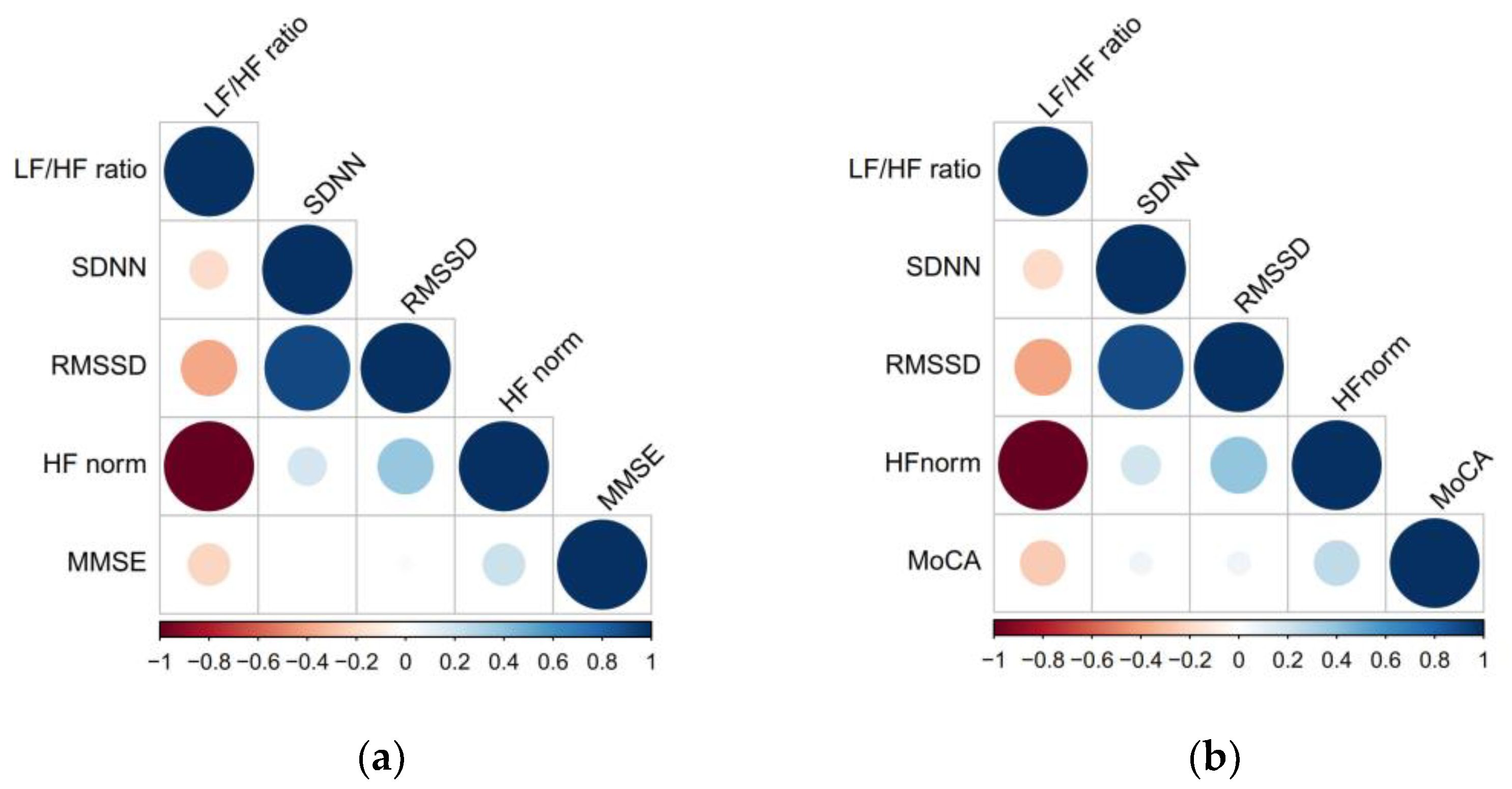
3.3. Spearman Correlation between HRV and Global Cognitive Performance
3.4. Association between HRV Parameters and Global Cognitive Function
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Nichols, E.; Szoeke, C.E.I.; Vollset, S.E.; Abbasi, N.; Abd-Allah, F.; Abdela, J.; Aichour, M.T.E.; Akinyemi, R.O.; Alahdab, F.; Asgedom, S.W.; et al. Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 88–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prince, M.; Bryce, R.; Albanese, E.; Wimo, A.; Ribeiro, W.; Ferri, C.P. The global prevalence of dementia: A systematic review and metaanalysis. Alzheimers Dement. 2013, 9, 63–75.e62. [Google Scholar] [CrossRef] [PubMed]
- Jia, J.; Wei, C.; Chen, S.; Li, F.; Tang, Y.; Qin, W.; Zhao, L.; Jin, H.; Xu, H.; Wang, F.; et al. The cost of Alzheimer’s disease in China and re-estimation of costs worldwide. Alzheimers Dement. 2018, 14, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.A.; Chang, C.-H.; Simonton, S.; Bynum, J.P.W. Trends in US Medicare Decedents’ Diagnosis of Dementia From 2004 to 2017. JAMA Health Forum 2022, 3, e220346. [Google Scholar] [CrossRef]
- Wardlaw, J.M.; Smith, E.E.; Biessels, G.J.; Cordonnier, C.; Fazekas, F.; Frayne, R.; Lindley, R.I.; O’Brien, J.T.; Barkhof, F.; Benavente, O.R.; et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. 2013, 12, 822–838. [Google Scholar] [CrossRef] [Green Version]
- Ter Telgte, A.; van Leijsen, E.M.C.; Wiegertjes, K.; Klijn, C.J.M.; Tuladhar, A.M.; de Leeuw, F.E. Cerebral small vessel disease: From a focal to a global perspective. Nat. Rev. Neurol. 2018, 14, 387–398. [Google Scholar] [CrossRef]
- Consortium, M. METACOHORTS for the study of vascular disease and its contribution to cognitive decline and neurodegeneration: An initiative of the Joint Programme for Neurodegenerative Disease Research. Alzheimers Dement. 2016, 12, 1235–1249. [Google Scholar] [CrossRef] [Green Version]
- Cannistraro, R.J.; Badi, M.; Eidelman, B.H.; Dickson, D.W.; Middlebrooks, E.H.; Meschia, J.F. CNS small vessel disease: A clinical review. Neurology 2019, 92, 1146–1156. [Google Scholar] [CrossRef]
- Han, F.; Zhai, F.F.; Wang, Q.; Zhou, L.X.; Ni, J.; Yao, M.; Li, M.L.; Zhang, S.Y.; Cui, L.Y.; Jin, Z.Y.; et al. Prevalence and Risk Factors of Cerebral Small Vessel Disease in a Chinese Population-Based Sample. J. Stroke 2018, 20, 239–246. [Google Scholar] [CrossRef]
- Draghici, A.E.; Taylor, J.A. The physiological basis and measurement of heart rate variability in humans. J. Physiol. Anthropol. 2016, 35, 22. [Google Scholar] [CrossRef] [Green Version]
- Task Force of ESC. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef] [Green Version]
- Singh, J.P.; Larson, M.G.; Tsuji, H.; Evans, J.C.; O’Donnell, C.J.; Levy, D. Reduced heart rate variability and new-onset hypertension: Insights into pathogenesis of hypertension: The Framingham Heart Study. Hypertension 1998, 32, 293–297. [Google Scholar] [CrossRef] [Green Version]
- Carnethon, M.R.; Golden, S.H.; Folsom, A.R.; Haskell, W.; Liao, D. Prospective investigation of autonomic nervous system function and the development of type 2 diabetes: The Atherosclerosis Risk In Communities study, 1987–1998. Circulation 2003, 107, 2190–2195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sajadieh, A.; Nielsen, O.W.; Rasmussen, V.; Hein, H.O.; Abedini, S.; Hansen, J.F. Increased heart rate and reduced heart-rate variability are associated with subclinical inflammation in middle-aged and elderly subjects with no apparent heart disease. Eur. Heart J. 2004, 25, 363–370. [Google Scholar] [CrossRef] [Green Version]
- Forte, G.; Favieri, F.; Casagrande, M. Heart Rate Variability and Cognitive Function: A Systematic Review. Front. Neurosci. 2019, 13, 710. [Google Scholar] [CrossRef] [Green Version]
- Schaich, C.L.; Malaver, D.; Chen, H.; Shaltout, H.A.; Zeki Al Hazzouri, A.; Herrington, D.M.; Hughes, T.M. Association of Heart Rate Variability With Cognitive Performance: The Multi-Ethnic Study of Atherosclerosis. J. Am. Heart Assoc. 2020, 9, e013827. [Google Scholar] [CrossRef]
- Kim, D.H.; Lipsitz, L.A.; Ferrucci, L.; Varadhan, R.; Guralnik, J.M.; Carlson, M.C.; Fleisher, L.A.; Fried, L.P.; Chaves, P.H. Association between reduced heart rate variability and cognitive impairment in older disabled women in the community: Women’s Health and Aging Study I. J. Am. Geriatr. Soc. 2006, 54, 1751–1757. [Google Scholar] [CrossRef] [Green Version]
- Dalise, A.M.; Prestano, R.; Fasano, R.; Gambardella, A.; Barbieri, M.; Rizzo, M.R. Autonomic Nervous System and Cognitive Impairment in Older Patients: Evidence From Long-Term Heart Rate Variability in Real-Life Setting. Front. Aging Neurosci. 2020, 12, 40. [Google Scholar] [CrossRef]
- Thayer, J.F.; Yamamoto, S.S.; Brosschot, J.F. The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. Int. J. Cardiol. 2010, 141, 122–131. [Google Scholar] [CrossRef]
- Thayer, J.F.; Ahs, F.; Fredrikson, M.; Sollers, J.J.; Wager, T.D. A meta-analysis of heart rate variability and neuroimaging studies: Implications for heart rate variability as a marker of stress and health. Neurosci. Biobehav. Rev. 2012, 36, 747–756. [Google Scholar] [CrossRef]
- Jennings, J.R.; Allen, B.; Gianaros, P.J.; Thayer, J.F.; Manuck, S.B. Focusing neurovisceral integration: Cognition, heart rate variability, and cerebral blood flow. Psychophysiology 2015, 52, 214–224. [Google Scholar] [CrossRef] [Green Version]
- Chinese Stroke Association; Chinese Society of Cerebral Small Vessel Diseases. Expert consensus on the design of clinical trials of drugs for the treatment of cerebral small vessel diseases. Chin. J. Stroke 2021, 16, 288–297. [Google Scholar] [CrossRef]
- Pantoni, L. Cerebral small vessel disease: From pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol. 2010, 9, 689–701. [Google Scholar] [CrossRef] [PubMed]
- Yamauchi, H.; Fukuda, H.; Oyanagi, C. Significance of white matter high intensity lesions as a predictor of stroke from arteriolosclerosis. J. Neurol. Neurosurg. Psychiatry 2002, 72, 576–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duan, J.; Lv, Y.B.; Gao, X.; Zhou, J.H.; Kraus, V.B.; Zeng, Y.; Su, H.; Shi, X.M. Association of cognitive impairment and elderly mortality: Differences between two cohorts ascertained 6-years apart in China. BMC Geriatr. 2020, 20, 29. [Google Scholar] [CrossRef] [Green Version]
- Cui, G.H.; Yao, Y.H.; Xu, R.F.; Tang, H.D.; Jiang, G.X.; Wang, Y.; Wang, G.; Chen, S.D.; Cheng, Q. Cognitive impairment using education-based cutoff points for CMMSE scores in elderly Chinese people of agricultural and rural Shanghai China. Acta Neurol. Scand. 2011, 124, 361–367. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Frewen, J.; Finucane, C.; Savva, G.M.; Boyle, G.; Coen, R.F.; Kenny, R.A. Cognitive function is associated with impaired heart rate variability in ageing adults: The Irish longitudinal study on ageing wave one results. Clin. Auton. Res. 2013, 23, 313–323. [Google Scholar] [CrossRef]
- Hammerle, P.; Aeschbacher, S.; Springer, A.; Eken, C.; Coslovsky, M.; Dutilh, G.; Moschovitis, G.; Rodondi, N.; Chocano, P.; Conen, D.; et al. Cardiac autonomic function and cognitive performance in patients with atrial fibrillation. Clin. Res. Cardiol. 2021, 111, 60–69. [Google Scholar] [CrossRef]
- Britton, A.; Singh-Manoux, A.; Hnatkova, K.; Malik, M.; Marmot, M.G.; Shipley, M. The association between heart rate variability and cognitive impairment in middle-aged men and women. The Whitehall II cohort study. Neuroepidemiology 2008, 31, 115–121. [Google Scholar] [CrossRef]
- Zeki Al Hazzouri, A.; Elfassy, T.; Carnethon, M.R.; Lloyd-Jones, D.M.; Yaffe, K. Heart Rate Variability and Cognitive Function In Middle-Age Adults: The Coronary Artery Risk Development in Young Adults. Am. J. Hypertens. 2017, 31, 27–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nonogaki, Z.; Umegaki, H.; Makino, T.; Suzuki, Y.; Kuzuya, M. Relationship between cardiac autonomic function and cognitive function in Alzheimer’s disease. Geriatr. Gerontol. Int. 2017, 17, 92–98. [Google Scholar] [CrossRef]
- Auroprajna, P.; Naik, B.M.; Sahoo, J.P.; Keerthi, G.S.; Pavanya, M.; Pal, G.K. Association of Sympathovagal Imbalance With Cognitive Impairment in Type 2 Diabetes in Adults. Can. J. Diabetes 2018, 42, 44–50. [Google Scholar] [CrossRef] [Green Version]
- Morandi, G.N.; Lin, S.H.; Lin, C.W.; Yeh, T.L.; Chu, C.L.; Lee, I.H.; Chi, M.H.; Chen, K.C.; Chen, P.S.; Yang, Y.K. Heart Rate Variability is Associated with Memory in Females. Appl. Psychophysiol. Biofeedback 2019, 44, 117–122. [Google Scholar] [CrossRef]
- van Buchem, M.A.; Biessels, G.J.; Brunner la Rocca, H.P.; de Craen, A.J.; van der Flier, W.M.; Ikram, M.A.; Kappelle, L.J.; Koudstaal, P.J.; Mooijaart, S.P.; Niessen, W.; et al. The heart-brain connection: A multidisciplinary approach targeting a missing link in the pathophysiology of vascular cognitive impairment. J. Alzheimers Dis. 2014, 42 (Suppl. S4), S443–S451. [Google Scholar] [CrossRef]
- Sloan, R.P.; DeMeersman, R.E.; Shapiro, P.A.; Bagiella, E.; Chernikhova, D.; Kuhl, J.P.; Zion, A.S.; Paik, M.; Myers, M.M. Blood pressure variability responses to tilt are buffered by cardiac autonomic control. Am. J. Physiol. 1997, 273, H1427–H1431. [Google Scholar] [CrossRef]
- Sloan, R.P.; Demeersman, R.E.; Shapiro, P.A.; Bagiella, E.; Kuhl, J.P.; Zion, A.S.; Paik, M.; Myers, M.M. Cardiac autonomic control is inversely related to blood pressure variability responses to psychological challenge. Am. J. Physiol. 1997, 272, H2227–H2232. [Google Scholar] [CrossRef]
- Gomez-Angelats, E.; de La Sierra, A.; Sierra, C.; Parati, G.; Mancia, G.; Coca, A. Blood pressure variability and silent cerebral damage in essential hypertension. Am. J. Hypertens. 2004, 17, 696–700. [Google Scholar] [CrossRef] [Green Version]
- Kukla, C.; Sander, D.; Schwarze, J.; Wittich, I.; Klingelhöfer, J. Changes of circadian blood pressure patterns are associated with the occurence of lucunar infarction. Arch. Neurol. 1998, 55, 683–688. [Google Scholar] [CrossRef] [Green Version]
- Whitmer, R.A.; Sidney, S.; Selby, J.; Johnston, S.C.; Yaffe, K. Midlife cardiovascular risk factors and risk of dementia in late life. Neurology 2005, 64, 277–281. [Google Scholar] [CrossRef]
- Yaffe, K.; Vittinghoff, E.; Pletcher, M.J.; Hoang, T.D.; Launer, L.J.; Whitmer, R.; Coker, L.H.; Sidney, S. Early adult to midlife cardiovascular risk factors and cognitive function. Circulation 2014, 129, 1560–1567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muller, M.; Grobbee, D.E.; Aleman, A.; Bots, M.; van der Schouw, Y.T. Cardiovascular disease and cognitive performance in middle-aged and elderly men. Atherosclerosis 2007, 190, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Femminella, G.D.; Rengo, G.; Komici, K.; Iacotucci, P.; Petraglia, L.; Pagano, G.; de Lucia, C.; Canonico, V.; Bonaduce, D.; Leosco, D.; et al. Autonomic dysfunction in Alzheimer’s disease: Tools for assessment and review of the literature. J. Alzheimers Dis. 2014, 42, 369–377. [Google Scholar] [CrossRef]
- Verberne, A.J.; Owens, N.C. Cortical modulation of the cardiovascular system. Prog. Neurobiol. 1998, 54, 149–168. [Google Scholar] [CrossRef]
- Kirchhoff, B.A.; Wagner, A.D.; Maril, A.; Stern, C.E. Prefrontal-temporal circuitry for episodic encoding and subsequent memory. J. Neurosci. 2000, 20, 6173–6180. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| All CSVD (n = 117) | |
|---|---|
| Age, mean (SD) | 59.53 (11.79) |
| Women, n (%) | 46 (39.32) |
| BMI, mean (SD) | 25.32 (3.29) |
| Education, n (%) | |
| College degree or above | 30 (25.64) |
| Middle school | 69 (58.97) |
| Elementary school or below | 18 (15.38) |
| Risk factors, n (%) | |
| Hypertension | 95 (81.20) |
| Diabetes mellitus | 48 (41.03) |
| Dyslipidemia | 105 (89.74) |
| Current smoking | 37 (31.62) |
| Drinking | 29 (24.79) |
| Medical history, n (%) | |
| Stroke | 52 (44.44) |
| Coronary heart disease | 17 (14.53) |
| MMSE, median (Q1, Q3) | 26.00 (22.00, 27.00) |
| MoCA, median (Q1, Q3) | 21.00 (17.00, 25.00) |
| All CSVD (n = 117) | Normal Cognitive Function Defined by MMSE (n = 76) | Impaired Cognitive Function Defined by MMSE (n = 41) | p Value | Normal Cognitive Function Defined by MoCA (n = 18) | Impaired Cognitive Function Defined by MoCA (n = 98) | p Value | |
|---|---|---|---|---|---|---|---|
| Time domain | |||||||
| SDNN (ms) | 17.98 (12.31, 23.52) | 17.79 (12.71, 23.11) | 17.98 (11.27, 26.35) | 0.882 | 20.10 (15.44, 25.59) | 17.27 (12.05, 23.52) | 0.250 |
| RMSSD (ms) | 19.37 (12.25, 28.20) | 19.23 (12.86, 27.94) | 19.85 (10.73, 28.77) | 0.656 | 22.97 (17.03, 28.20) | 18.96 (11.25, 28.37) | 0.234 |
| Frequency domain | |||||||
| HF norm (n.u.) | 50.13 (39.46, 64.99) | 57.23 (42.68, 67.46) | 42.95 (29.05, 52.59) | <0.001 | 56.31 (45.39, 68.75) | 48.22 (39.35, 64.08) | 0.225 |
| LF/HF ratio | 0.99 (0.54, 1.53) | 0.75 (0.48, 1.34) | 1.33 (0.90, 2.44) | <0.001 | 0.78 (0.45, 1.20) | 1.07 (0.56, 1.54) | 0.225 |
| MMSE Scores | MoCA Scores | |||||||
|---|---|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | Unadjusted | Adjusted | |||||
| β (95% CI) | p Value | β (95% CI) | p Value | β (95% CI) | p Value | β (95% CI) | p Value | |
| Time domain | ||||||||
| SDNN (ms) | −0.520 (−1.925, 0.884) | 0.465 | −0.610 (−1.832, 0.613) | 0.325 | −0.167 (−1.833, 1.498) | 0.843 | −0.534 (−1.918, 0.850) | 0.446 |
| RMSSD (ms) | −0.106 (−1.301, 1.090) | 0.861 | −0.061 (−1.109, 0.986) | 0.908 | 0.110 (−1.304, 1.524) | 0.878 | 0.049 (−1.132, 1.231) | 0.934 |
| Frequency domain | ||||||||
| HF norm (n.u.) | 0.057 (0.010, 0.104) | 0.018 | 0.051 (0.012, 0.090) | 0.011 | 0.069 (0.014, 0.124) | 0.014 | 0.061 (0.017, 0.105) | 0.007 |
| LF/HF ratio | −0.576 (−1.058, −0.093) | 0.020 | −0.492 (−0.893, −0.092) | 0.017 | −0.738 (−1.302, −0.174) | 0.011 | −0.691 (−1.134, −0.248) | 0.003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, G.; Collet, J.-P.; Zhao, M.; Lu, Y.; Wang, Y. Associations between Autonomic Function and Cognitive Performance among Patients with Cerebral Small Vessel Disease. Brain Sci. 2023, 13, 344. https://doi.org/10.3390/brainsci13020344
Hu G, Collet J-P, Zhao M, Lu Y, Wang Y. Associations between Autonomic Function and Cognitive Performance among Patients with Cerebral Small Vessel Disease. Brain Sciences. 2023; 13(2):344. https://doi.org/10.3390/brainsci13020344
Chicago/Turabian StyleHu, Guoliang, Jean-Paul Collet, Mengxi Zhao, Yao Lu, and Yilong Wang. 2023. "Associations between Autonomic Function and Cognitive Performance among Patients with Cerebral Small Vessel Disease" Brain Sciences 13, no. 2: 344. https://doi.org/10.3390/brainsci13020344