

Current Opinions about the Use of Duloxetine: Results from a Survey Aimed at Psychiatrists
 , , , , , ,
, , , , , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gutiérrez-Rojas, L.; Porras-Segovia, A.; Dunne, H.; Andrade-González, N.; Cervilla, J.A. Prevalence and Correlates of Major Depressive Disorder: A Systematic Review. Braz. J. Psychiatry 2020, 42, 657. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, M.J. Depression Is the Leading Cause of Disability around the World. JAMA 2017, 317, 1517. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Ortega, M.A.; Alvarez-Mon, M.A.; García-Montero, C.; Fraile-Martinez, O.; Guijarro, L.G.; Lahera, G.; Monserrat, J.; Valls, P.; Mora, F.; Rodríguez-Jiménez, R.; et al. Gut Microbiota Metabolites in Major Depressive Disorder-Deep Insights into Their Pathophysiological Role and Potential Translational Applications. Metabolites 2022, 12, 50. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Mon, M.A.; Ortega, M.A.; García-Montero, C.; Fraile-Martinez, O.; Monserrat, J.; Lahera, G.; Mora, F.; Rodriguez-Quiroga, A.; Fernandez-Rojo, S.; Quintero, J.; et al. Exploring the Role of Nutraceuticals in Major Depressive Disorder (MDD): Rationale, State of the Art and Future Prospects. Pharmaceuticals 2021, 14, 821. [Google Scholar] [CrossRef] [PubMed]
- Ortega, M.A.; Fraile-Martínez, Ó.; García-Montero, C.; Alvarez-Mon, M.A.; Lahera, G.; Monserrat, J.; Llavero-Valero, M.; Mora, F.; Rodríguez-Jiménez, R.; Fernandez-Rojo, S.; et al. Nutrition, Epigenetics, and Major Depressive Disorder: Understanding the Connection. Front. Nutr. 2022, 9, 979. [Google Scholar] [CrossRef]
- Jesulola, E.; Micalos, P.; Baguley, I.J. Understanding the Pathophysiology of Depression: From Monoamines to the Neurogenesis Hypothesis Model—Are We there yet? Behav. Brain Res. 2018, 341, 79–90. [Google Scholar] [CrossRef]
- Bakunina, N.; Pariante, C.M.; Zunszain, P.A. Immune Mechanisms Linked to Depression via Oxidative Stress and Neuroprogression. Immunology 2015, 144, 365. [Google Scholar] [CrossRef] [Green Version]
- Greenberg, P.E.; Fournier, A.A.; Sisitsky, T.; Simes, M.; Berman, R.; Koenigsberg, S.H.; Kessler, R.C. The Economic Burden of Adults with Major Depressive Disorder in the United States (2010 and 2018). Pharmacoeconomics 2021, 39, 653–665. [Google Scholar] [CrossRef]
- Vieta, E.; Alonso, J.; Pérez-Sola, V.; Roca, M.; Hernando, T.; Sicras-Mainar, A.; Sicras-Navarro, A.; Herrera, B.; Gabilondo, A. Epidemiology and Costs of Depressive Disorder in Spain: The EPICO Study. Eur. Neuropsychopharmacol. 2021, 50, 93–103. [Google Scholar] [CrossRef]
- Gautam, S.; Jain, A.; Gautam, M.; Vahia, V.N.; Grover, S. Clinical Practice Guidelines for the Management of Depression. Indian J. Psychiatry 2017, 59, S34. [Google Scholar] [CrossRef]
- Cipriani, A.; Furukawa, T.A.; Salanti, G.; Chaimani, A.; Atkinson, L.Z.; Ogawa, Y.; Leucht, S.; Ruhe, H.G.; Turner, E.H.; Higgins, J.P.T.; et al. Comparative Efficacy and Acceptability of 21 Antidepressant Drugs for the Acute Treatment of Adults with Major Depressive Disorder: A Systematic Review and Network Meta-Analysis. Lancet 2018, 391, 1357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhaliwal, J.S.; Spurling, B.C.; Molla, M. Duloxetine. Essence Analg. Analg. 2022, 353–356. [Google Scholar] [CrossRef]
- Stahl, S.M.; Grady, M.M.; Moret, C.; Briley, M. SNRIs: Their Pharmacology, Clinical Efficacy, and Tolerability in Comparison with Other Classes of Antidepressants. CNS Spectr. 2005, 10, 732–747. [Google Scholar] [CrossRef] [PubMed]
- Sansone, R.A.; Sansone, L.A. Serotonin Norepinephrine Reuptake Inhibitors: A Pharmacological Comparison. Innov. Clin. Neurosci. 2014, 11, 37. [Google Scholar] [PubMed]
- Yuan, Z.; Chen, Z.; Xue, M.; Zhang, J.; Leng, L. Application of Antidepressants in Depression: A Systematic Review and Meta-Analysis. J. Clin. Neurosci. 2020, 80, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Isacsson, G.; Redfors, I.; Wasserman, D.; Bergman, U. Choice of Antidepressants: Questionnaire Survey of Psychiatrists and General Practitioners in Two Areas of Sweden. BMJ 1994, 309, 1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerman, M.; McGlinchey, J.B. Why don’t Psychiatrists Use Scales to Measure Outcome when Treating Depressed Patients? J. Clin. Psychiatry 2008, 69, 1916–1919. [Google Scholar] [CrossRef]
- Liu, F.; Demosthenes, P. Real-World Data: A Brief Review of the Methods, Applications, Challenges and Opportunities. BMC Med. Res. Methodol. 2022, 22, 287. [Google Scholar] [CrossRef]
- Bozzatello, P.; Giordano, B.; Montemagni, C.; Rocca, P.; Bellino, S. Real-World Functioning in Psychiatric Outpatients: Predictive Factors. J. Clin. Med. 2022, 11, 4400. [Google Scholar] [CrossRef]
- de Anta, L.; Alvarez-Mon, M.A.; Ortega, M.A.; Salazar, C.; Donat-Vargas, C.; Santoma-Vilaclara, J.; Martin-Martinez, M.; Lahera, G.; Gutierrez-Rojas, L.; Rodriguez-Jimenez, R.; et al. Areas of Interest and Social Consideration of Antidepressants on English Tweets: A Natural Language Processing Classification Study. J. Pers. Med. 2022, 12, 155. [Google Scholar] [CrossRef]
- de las Cuevas, C.; Gutiérrez-Rojas, L.; Alvarez-Mon, M.A.; Andreu-Bernabeu, Á.; Capitán, L.; Gómez, J.C.; Grande, I.; Hidalgo-Mazzei, D.; Mateos, R.; Moreno-Gea, P.; et al. Evaluating the Effect of a Telepsychiatry Educational Program on the Awareness, Knowledge, Attitude, and Skills of Telepsychiatry among Spanish Psychiatrists during COVID-19 Pandemic. Telemed. J. E. Health. 2023, 29, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.; Saadabadi, A. Venlafaxine. xPharm Compr. Pharmacol. Ref. 2022, 1–5. [Google Scholar] [CrossRef]
- Hillhouse, T.M.; Porter, J.H. A Brief History of the Development of Antidepressant Drugs: From Monoamines to Glutamate. Exp. Clin. Psychopharmacol. 2015, 23, 1. [Google Scholar] [CrossRef]
- Li, J.; Lu, C.; Gao, Z.; Feng, Y.; Luo, H.; Lu, T.; Sun, X.; Hu, J.; Luo, Y. SNRIs Achieve Faster Antidepressant Effects than SSRIs by Elevating the Concentrations of Dopamine in the Forebrain. Neuropharmacology 2020, 177, 108237. [Google Scholar] [CrossRef] [PubMed]
- MacHado, M.; Einarson, T.R. Comparison of SSRIs and SNRIs in Major Depressive Disorder: A Meta-Analysis of Head-to-Head Randomized Clinical Trials. J. Clin. Pharm. Ther. 2010, 35, 177–188. [Google Scholar] [CrossRef]
- Thase, M. Are SNRIs more Effective than SSRIs? A Review of the Current State of the Controversy—PubMed. Psychopharmacol. Bull. 2008, 41, 58–85. [Google Scholar] [PubMed]
- Cipriani, A.; La Ferla, T.; Furukawa, T.A.; Signoretti, A.; Nakagawa, A.; Churchill, R.; McGuire, H.; Barbui, C. Sertraline versus Other Antidepressive Agents for Depression. Cochrane Database Syst. Rev. 2009. [Google Scholar] [CrossRef] [Green Version]
- Marasine, N.R.; Sankhi, S.; Lamichhane, R.; Marasini, N.R.; Dangi, N.B. Use of Antidepressants among Patients Diagnosed with Depression: A Scoping Review. Biomed Res. Int. 2021, 2021, 1–8. [Google Scholar] [CrossRef]
- Mowla, A.; Dastgheib, S.A.; Razeghian Jahromi, L. Comparing the Effects of Sertraline with Duloxetine for Depression Severity and Symptoms: A Double-Blind, Randomized Controlled Trial. Clin. Drug Investig. 2016, 36, 539–543. [Google Scholar] [CrossRef]
- Sir, A.; D’Souza, R.F.; Uguz, S.; George, T.; Vahip, S.; Hopwood, M.; Martin, A.J.; Lam, W.; Burt, T. Randomized Trial of Sertraline versus Venlafaxine XR in Major Depression: Efficacy and Discontinuation Symptoms. J. Clin. Psychiatry 2005, 66, 1312–1320. [Google Scholar] [CrossRef]
- Frampton, J.E.; Plosker, G.L. Duloxetine: A Review of Its Use in the Treatment of Major Depressive Disorder. CNS Drugs 2007, 21, 581–609. [Google Scholar] [CrossRef]
- Rodrigues-Amorim, D.; Olivares, J.M.; Spuch, C.; Rivera-Baltanás, T. A Systematic Review of Efficacy, Safety, and Tolerability of Duloxetine. Front. Psychiatry 2020, 11, 554899. [Google Scholar] [CrossRef] [PubMed]
- Bitter, I.; Filipovits, D.; Czobor, P. Adverse Reactions to Duloxetine in Depression. Expert Opin. Drug Saf. 2011, 10, 839–850. [Google Scholar] [CrossRef]
- Wernicke, J.F.; Gahimer, J.; Yalcin, I.; Wulster-Radcliffe, M.; Viktrup, L. Safety and Adverse Event Profile of Duloxetine. Expert Opin. Drug Saf. 2005, 4, 987–993. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, A.; Koesters, M.; Furukawa, T.A.; Nosè, M.; Purgato, M.; Omori, I.M.; Trespidi, C.; Barbui, C. Duloxetine versus Other Anti-Depressive Agents for Depression. Cochrane Database Syst. Rev. 2012, 10, CD006533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serafini, G.; Pompili, M.; Del Casale, A.; Mancini, M.; Innamorati, M.; Lester, D.; Girardi, P.; Tatarelli, R. Duloxetine versus Venlafaxine in the Treatment of Unipolar and Bipolar Depression—PubMed. Clin Ter. 2010, 161, 321–327. [Google Scholar]
- Wang, J.; Liu, X.; Mullins, C.D. Treatment Adherence and Persistence with Duloxetine, Venlafaxine XR, and Escitalopram among Patients with Major Depressive Disorder and Chronic Pain-Related Diseases. Curr. Med. Res. Opin. 2011, 27, 1303–1313. [Google Scholar] [CrossRef]
- Schueler, Y.B.; Koesters, M.; Wieseler, B.; Grouven, U.; Kromp, M.; Kerekes, M.F.; Kreis, J.; Kaiser, T.; Becker, T.; Weinmann, S. A Systematic Review of Duloxetine and Venlafaxine in Major Depression, including Unpublished Data. Acta Psychiatr. Scand. 2011, 123, 247–265. [Google Scholar] [CrossRef]
- Ye, W.; Zhao, Y.; Robinson, R.L.; Swindle, R.W. Treatment Patterns Associated with Duloxetine and Venlafaxine Use for Major Depressive Disorder. BMC Psychiatry 2011, 11, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Lavindran, L.N.; Eisfeld, B.S.; Kennedy, S.H. Combining Mirtazapine and Duloxetine in Treatment-Resistant Depression Improves Outcomes and Sexual Function. J. Clin. Psychopharmacol. 2008, 28, 107–108. [Google Scholar] [CrossRef]
- Engel, D.; Zomkowski, A.D.E.; Lieberknecht, V.; Rodrigues, A.L.; Gabilan, N.H. Chronic Administration of Duloxetine and Mirtazapine Downregulates Proapoptotic Proteins and Upregulates Neurotrophin Gene Expression in the Hippocampus and Cerebral Cortex of Mice. J. Psychiatr. Res. 2013, 47, 802–808. [Google Scholar] [CrossRef] [PubMed]
- Dunlop, B.W.; Davis, P.G. Combination Treatment with Benzodiazepines and SSRIs for Comorbid Anxiety and Depression: A Review. Prim. Care Companion J. Clin. Psychiatry 2008, 10, 222. [Google Scholar] [CrossRef] [PubMed]
- Cuomo, A.; Ballerini, A.; Bruni, A.C.; Decina, P.; Di Sciascio, G.; Fiorentini, A.; Scaglione, F.; Vampini, C.; Fagiolini, A. Clinical Guidance for the Use of Trazodone in Major Depressive Disorder and Concomitant Conditions: Pharmacology and Clinical Practice. Riv. Psichiatr. 2019, 54, 137–149. [Google Scholar] [CrossRef]
- Menchetti, M.; Ferrari Gozzi, B.; Saracino, M.A.; Mercolini, L.; Petio, C.; Raggi, M.A. Non-Fatal Overdose of Duloxetine in Combination with Other Antidepressants and Benzodiazepines. World J. Biol. Psychiatry 2009, 10, 385–389. [Google Scholar] [CrossRef]
- Liu, J.; Li, R.; Zhang, T.; Xue, R.; Li, T.; Li, Z.; Zhuang, X.; Wang, Q.; Chen, Y.A.; Dong, J.; et al. High-Content Imaging of Human Hepatic Spheroids for Researching the Mechanism of Duloxetine-Induced Hepatotoxicity. Cell Death Dis. 2022, 13, 669. [Google Scholar] [CrossRef] [PubMed]
- Kornstein, S.G.; Wohlreich, M.M.; Mallinckrodt, C.H.; Watkin, J.G.; Stewart, D.E. Duloxetine Efficacy for Major Depressive Disorder in Male vs. Female Patients: Data from 7 Randomized, Double-Blind, Placebo-Controlled Trials. J. Clin. Psychiatry 2006, 67, 761–770. [Google Scholar] [CrossRef]
- Stewart, D.E.; Wohlreich, M.M.; Mallinckrodt, C.H.; Watkin, J.G.; Kornstein, S.G. Duloxetine in the Treatment of Major Depressive Disorder: Comparisons of Safety and Tolerability in Male and Female Patients. J. Affect. Disord. 2006, 94, 183–189. [Google Scholar] [CrossRef]
- Hensley, P.L.; Nurnberg, H.G. SSRI Sexual Dysfunction: A Female Perspective. J. Sex Marital Ther. 2002, 28, 143–153. [Google Scholar] [CrossRef]
- Wise, T.N.; Perahia, D.G.S.; Pangallo, B.A.; Losin, W.G.; Wiltse, C.G. Effects of the Antidepressant Duloxetine on Body Weight: Analyses of 10 Clinical Studies. Prim. Care Companion J. Clin. Psychiatry 2006, 8, 269–278. [Google Scholar] [CrossRef]
- Bet, P.M.; Hugtenburg, J.G.; Penninx, B.W.J.H.; Hoogendijk, W.J.G. Side Effects of Antidepressants during Long-Term Use in a Naturalistic Setting. Eur. Neuropsychopharmacol. 2013, 23, 1443–1451. [Google Scholar] [CrossRef] [Green Version]
- Hagovska, M.; Svihra, J. Evaluation of Duloxetine and Innovative Pelvic Floor Muscle Training in Women with Stress Urinary Incontinence (DULOXING): Study Protocol Clinical Trial (SPIRIT Compliant). Medicine 2020, 99, e18834. [Google Scholar] [CrossRef] [PubMed]
- Kotecha, P.; Sahai, A.; Malde, S. Use of Duloxetine for Postprostatectomy Stress Urinary Incontinence: A Systematic Review. Eur. Urol. Focus 2021, 7, 618–628. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.J.; Lu, Y.; Detke, M.J.; Hudson, J.; Iyengar, S.; Demitrack, M.A. Effects of Duloxetine on Painful Physical Symptoms Associated with Depression. Psychosomatics 2004, 45, 17–28. [Google Scholar] [CrossRef]
- Bailey, K.P. Physical Symptoms Comorbid with Depression and the New Antidepressant Duloxetine. J. Psychosoc. Nurs. Ment. Health Serv. 2003, 41, 13–18. [Google Scholar] [CrossRef]
- Ling, H.Q.; Chen, Z.H.; He, L.; Feng, F.; Weng, C.G.; Cheng, S.J.; Rong, L.M.; Xie, P.G. Comparative Efficacy and Safety of 11 Drugs as Therapies for Adults with Neuropathic Pain after Spinal Cord Injury: A Bayesian Network Analysis Based on 20 Randomized Controlled Trials. Front. Neurol. 2022, 13, 818522. [Google Scholar] [CrossRef]
- Gül, Ş.K.; Tepetam, H.; Gül, H.L. Duloxetine and Pregabalin in Neuropathic Pain of Lung Cancer Patients. Brain Behav. 2020, 10, e01527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, I.; Ahmad, W.; Islam, M.; Jan, B.; Haq, E.U.; Mahmood, J.; Iqbal, N.; Shah, M.; Shah, I.; Ahmad, W.; et al. A Prospective Observational Study Comparing the Efficacy and Safety of Duloxetine and Pregabalin in Diabetic Peripheral Neuropathic Pain. Cureus J. Med. Sci. 2022, 14, e28683. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Questions Included in the Survey. | Answers |
|---|---|
| Among the following antidepressants, which do you think has generated the most indexed publications in the last five years? Order, please, from the first (the one that has generated the most posts) to the fourth (the one that has generated the fewest posts) |
|
| What is the mechanism of action of Duloxetine? (Single answer) |
|
| In your opinion, does Duloxetine have specific advantages over other antidepressants? (Single answer) |
|
| In what clinical situations does Duloxetine have advantages over other antidepressants? (Multiple answer) |
|
| How would you rate the tolerance of Duloxetine? (Single answer) |
|
| Can you please cite the commercial names of duloxetine that you remember? Please write down your answer. | |
| In a patient diagnosed with major depression, what would be the maximum dose of duloxetine that you would use? (Single answer) |
|
| In relation to subjective well-being, which antidepressant do you think patients prefer? (Single answer) |
|
| Do you usually associate Duloxetine with any other psychoactive drug? (Single answer) |
|
| With what type of psychotropic drugs do you most frequently associate Duloxetine? Please write down your answer. | |
| For which of the following diseases is Duloxetine approved? (Possible multiple answers) |
|
| In a 63-year-old patient with diabetes mellitus and metabolic disorders who is referred for the first time to psychiatry for presenting a major depressive episode, what antidepressant would you start the treatment with? (Single answer) |
|
| In which of the following clinical situations would you use duloxetine? (Possible multiple answer of the codes, 1,2,3 and 4) |
|
| Which of the following antidepressants do you think is most indicated in a patient who is referred to psychiatry for presenting anxious-depressive symptoms in the context of poorly controlled Fibromyalgia? (Single answer) |
|
| Which of the following antidepressants do you think is most indicated in a patient who is referred to psychiatry for presenting anxious-depressive symptoms in the context of a tension-type headache of months of evolution that has not improved with amitriptyline? (Single answer) |
|
| In your opinion, in which of the following clinical situations would Duloxetine be less indicated? (Single answer) |
|
| Which of the following antidepressants do you think is most indicated in a 20-year-old male patient who is being followed up with Psychiatry for Attention Deficit Hyperactivity Disorder who suffers a depressive episode? (Single answer) |
|
| In what symptoms do you think Duloxetine is more effective than Venlafaxine? Please write down your answer. | |
| In what symptoms do you think Venlafaxine is more effective than duloxetine? Please write down your answer. | |
| In your opinion, which SNRIs (Serotonin and norepinephrine reuptake inhibitors) is better tolerated? (Single answer) |
|
| Result from the Survey | Scientific Literature | References |
|---|---|---|
| Duloxetine has advantages over other antidepressants, especially for patients with MDD and somatic manifestations (mainly pain). | Duloxetine has proven to be effective in the short- and long-term treatment of MDD, particularly for treating the core emotional symptoms as well as the painful physical symptoms related to depression. | [32,54,55] |
| The maximum dose of duloxetine for patients with MDD is 120 mg per day, with favorable responses in 97% of patients. | Duloxetine is safe, effective, and well-tolerated at doses comprised between 60 and 120 mg/day, even in elderly patients or in those with concomitant illnesses. | [33,34] |
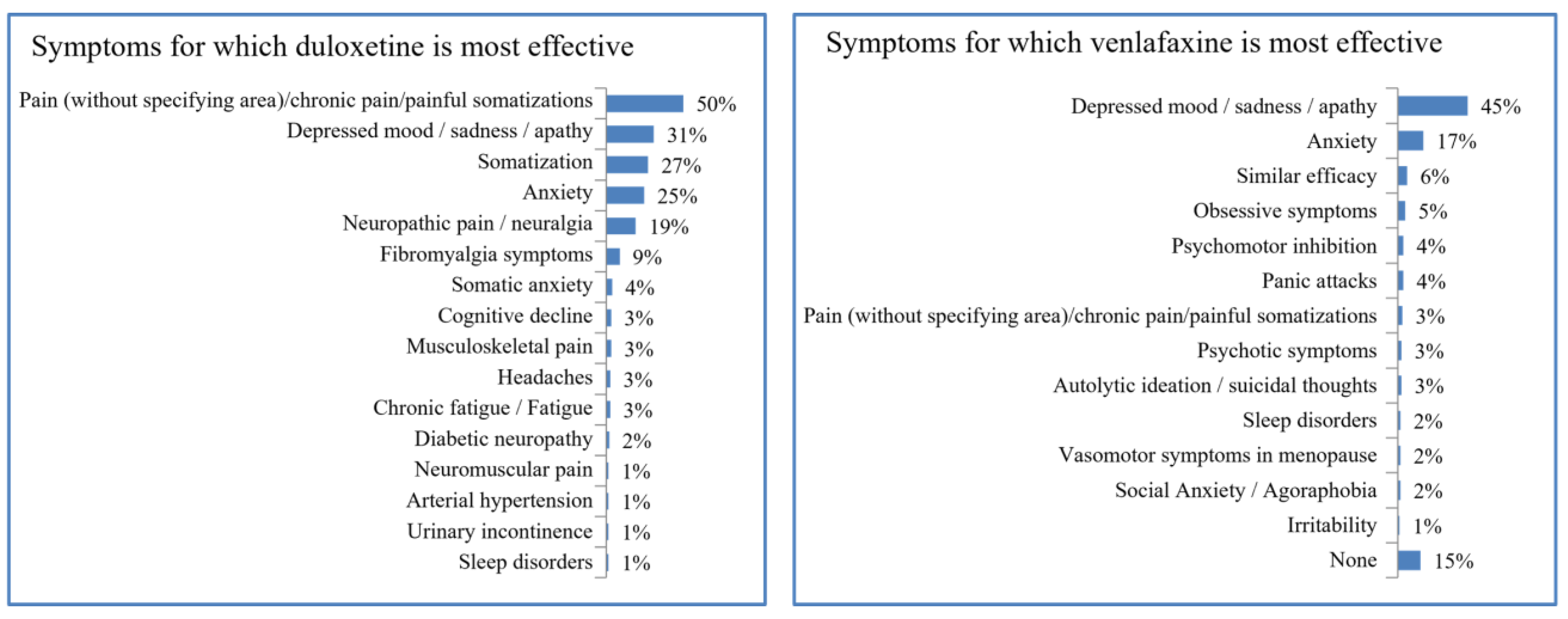
| Compared to venlafaxine, duloxetine exerts greater efficacy against pain and somatization. However, venlafaxine is somewhat more effective against sadness or apathy. | Both venlafaxine and duloxetine are two of the most effective drugs for the clinical management of MDD. | [16] |
| Duloxetine seems to be more effective in reducing anxiety and suicidal ideation in depressed patients and in pain alleviation. In general, patients receiving duloxetine tend to have a more complex and costly antecedent clinical presentation whereas venlafaxine could be a valid alternative in patients who do not tolerate or respond to SSRIs. | [37,38,39,40] | |
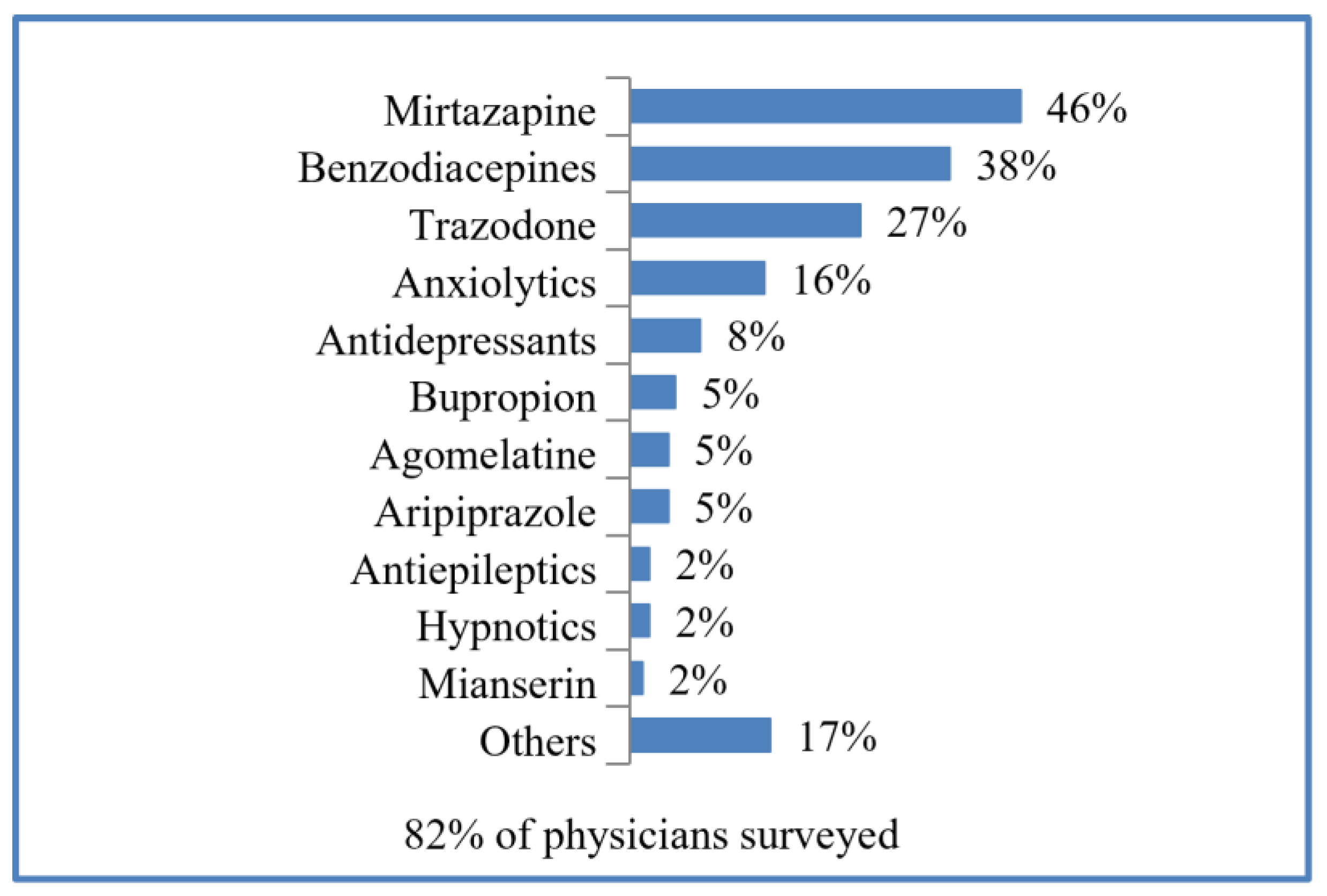
| 8 out of 10 clinicians prescribed duloxetine in combination with other agents, mainly mirtazapine, followed by benzodiazepines and trazodone. | Duloxetine is used with mirtazapine in patients with treatment-resistant depression, and some preclinical model studies endorse their synergic benefits to alleviate depression symptoms. The combination of SNRIs with benzodiazepines seem to improve treatment outcomes in patients with comorbid anxiety and depression, whereas trazodone may be effective in depressed patients with comorbid insomnia, anxiety, or psychomotor agitation. However, some authors are aware of the possible warnings related to combining duloxetine with other antidepressants in terms of possible toxicity and adverse effects. | [41,42,43,44,45] |
| Duloxetine is more frequently prescribed in women. | Duloxetine is more commonly prescribed to women, although the efficacy of duloxetine does not vary among male and female populations. Duloxetine is related to more severe sexual dysfunction in women when compared to men, and it is also related to less weight gain when compared to other antidepressants, a common adverse effect associated with the female gender. | [47,48,49,50,51] |
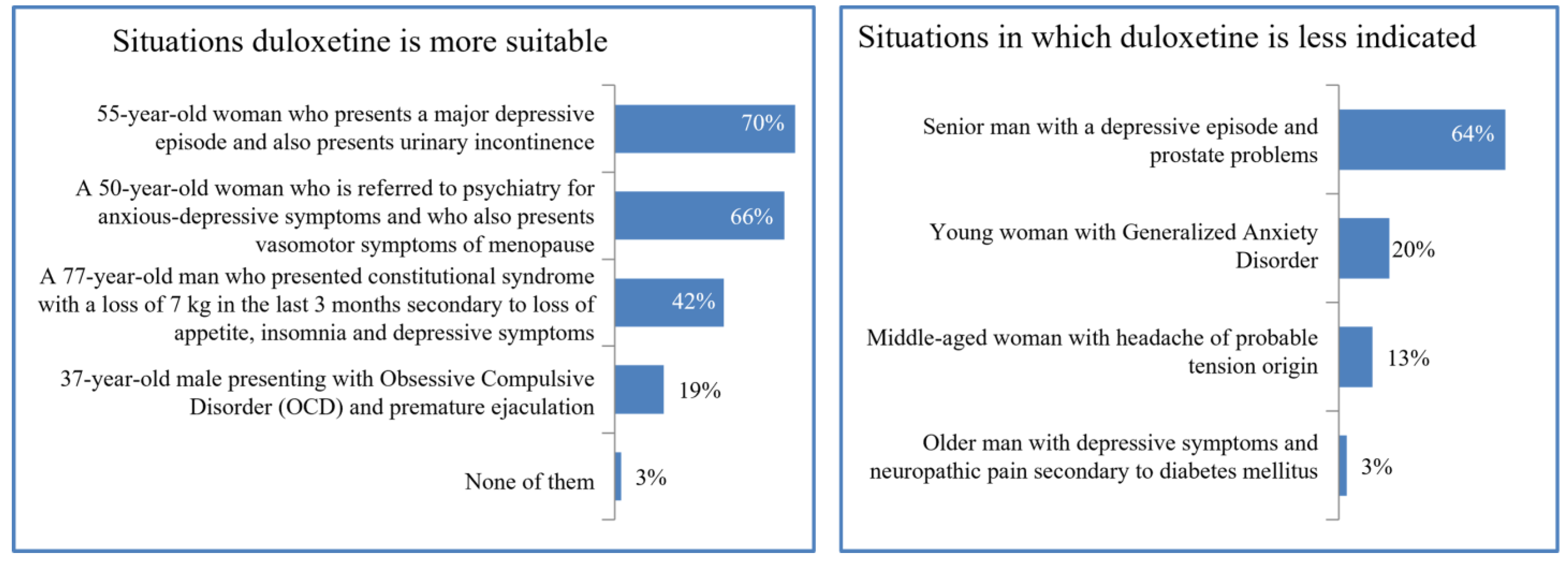
| 7 out of 10 clinicians would recommend duloxetine in female patients with depressive episodes in menopause and urinary incontinence, although almost 65% reject it for elderly males with depressive episodes and prostate problems. | Duloxetine shows favorable effects in women with stress urinary incontinence, whereas in men with urinary incontinence and depressive symptoms after a prostatectomy the mean adverse event rates are relatively high. | [52,53] |
| Duloxetine can be recommended for alleviating musculoskeletal or unspecified pain, but not in elderly patients with depressive symptoms and neuropathic diabetic pain. | Neuropathic pain relief by duloxetine has also been reported in other comorbidities beyond MDD, with slight benefits in comparison to the use of other therapeutic alternatives, although its safety profile in neuropathic diabetic pain is limited when compared to other therapeutic alternatives. | [56,57,58] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alvarez-Mon, M.A.; García-Montero, C.; Fraile-Martinez, O.; Quintero, J.; Fernandez-Rojo, S.; Mora, F.; Gutiérrez-Rojas, L.; Molina-Ruiz, R.M.; Lahera, G.; Álvarez-Mon, M.; et al. Current Opinions about the Use of Duloxetine: Results from a Survey Aimed at Psychiatrists. Brain Sci. 2023, 13, 333. https://doi.org/10.3390/brainsci13020333
Alvarez-Mon MA, García-Montero C, Fraile-Martinez O, Quintero J, Fernandez-Rojo S, Mora F, Gutiérrez-Rojas L, Molina-Ruiz RM, Lahera G, Álvarez-Mon M, et al. Current Opinions about the Use of Duloxetine: Results from a Survey Aimed at Psychiatrists. Brain Sciences. 2023; 13(2):333. https://doi.org/10.3390/brainsci13020333
Chicago/Turabian StyleAlvarez-Mon, M. A., Cielo García-Montero, Oscar Fraile-Martinez, Javier Quintero, Sonia Fernandez-Rojo, Fernando Mora, Luis Gutiérrez-Rojas, Rosa M. Molina-Ruiz, Guillermo Lahera, Melchor Álvarez-Mon, and et al. 2023. "Current Opinions about the Use of Duloxetine: Results from a Survey Aimed at Psychiatrists" Brain Sciences 13, no. 2: 333. https://doi.org/10.3390/brainsci13020333