
Dynamic Amyloid and Metabolic Signatures of Delayed Recall Performance within the Clinical Spectrum of Alzheimer’s Disease
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Classification Criteria
2.3. Memory Tests
2.4. Imaging Acquisition and Processing
2.5. Statistical Analysis
3. Results
3.1. Demographic and Neuropsychological Data
3.2. Association between RAVLT30 and LM30
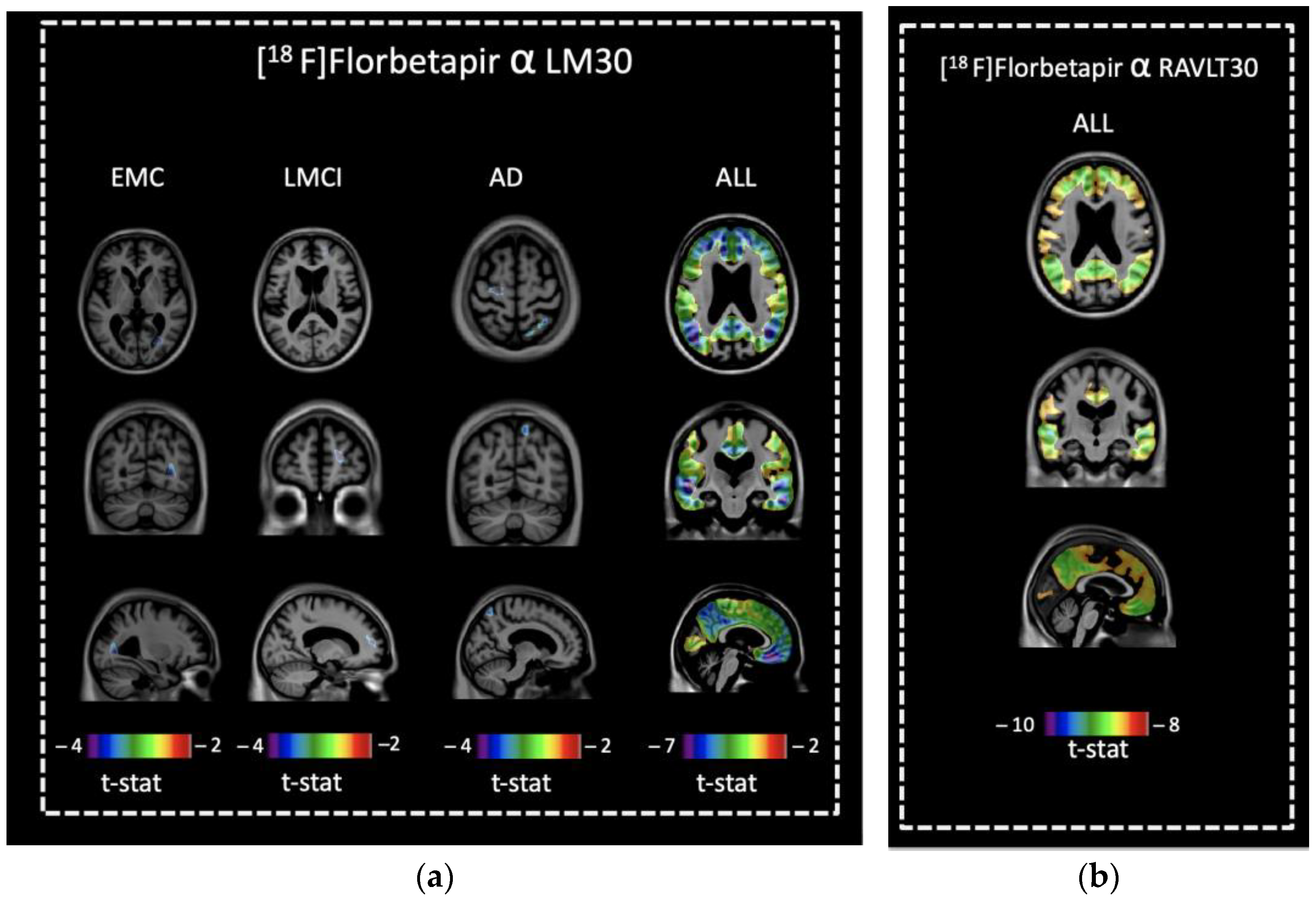
3.3. Voxel-Based Comparisons of [18F]florbetapir Retention and Memory Scores
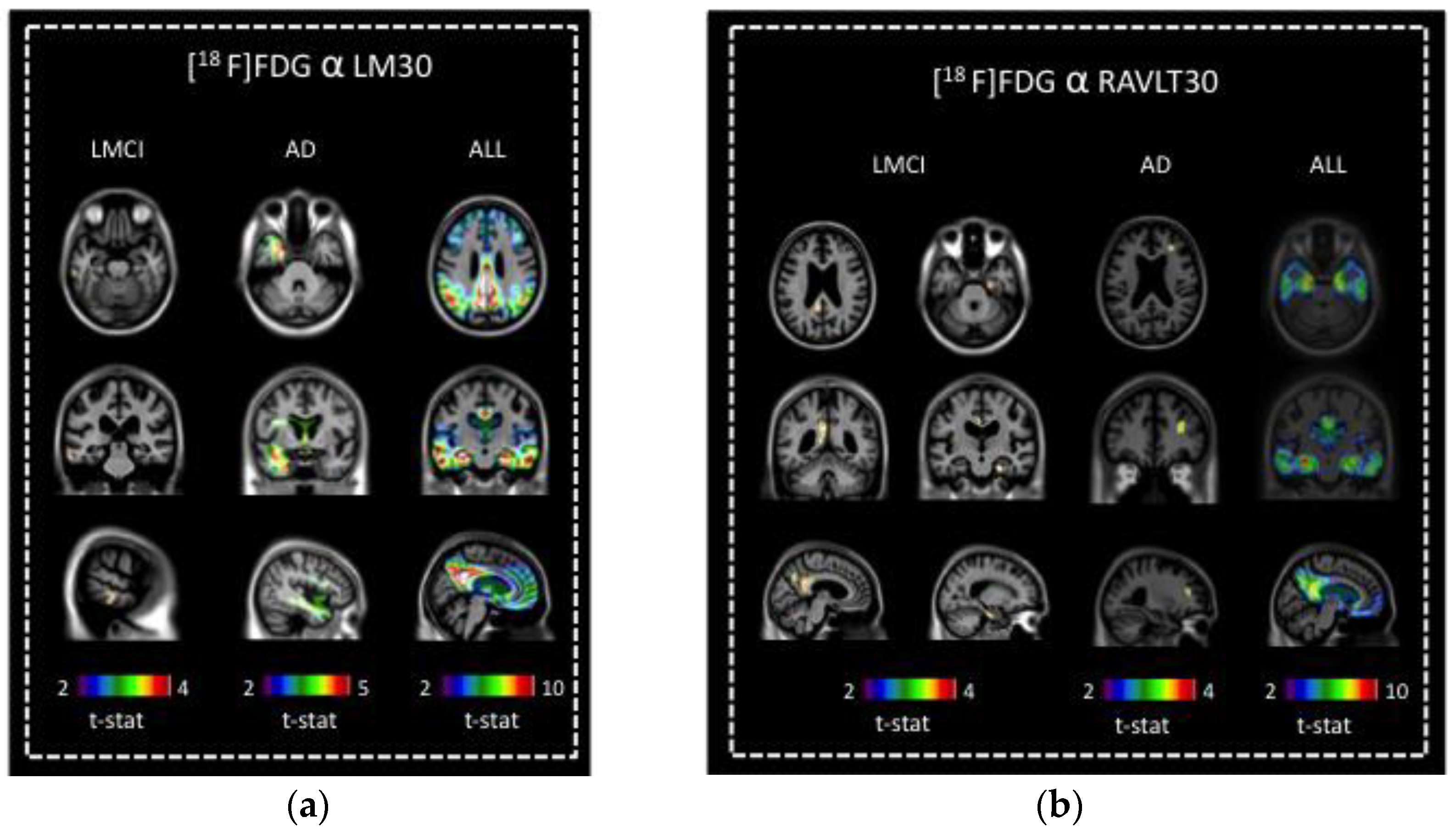
3.4. Voxel-Based Comparisons of [18F]FDG Uptake and Memory Scores
4. Discussion
4.1. Associations of Amyloid Deposition with Delayed Recall
4.2. Decreased Regional Cerebral Metabolism and Memory
4.3. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alzheimer’s Disease Facts and Figures; Alzheimer’s Association: Chicago, IL, USA, 2022.
- World Health Organization—Dementia Fact Sheet; World Health Organization: Geneva, Switzerland, 2022.
- Hardy, J.; Allsop, D. Amyloid Deposition as the Central Event in the Aetiology of Alzheimer’s Disease. Trends Pharmacol. Sci. 1991, 12, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Hardy, J.A.; Higgins, G.A. Alzheimer’s Disease: The Amyloid Cascade Hypothesis. Science 1992, 256, 184–185. [Google Scholar] [CrossRef] [PubMed]
- Hyman, B.T. Amyloid-Dependent and Amyloid-Independent Stages of Alzheimer Disease. Arch. Neurol. 2011, 68, 1062–1064. [Google Scholar] [CrossRef] [PubMed]
- Jack, C.R.; Knopman, D.S.; Jagust, W.J.; Petersen, R.C.; Weiner, M.W.; Aisen, P.S.; Shaw, L.M.; Vemuri, P.; Wiste, H.J.; Weigand, S.D.; et al. Tracking Pathophysiological Processes in Alzheimer’s Disease: An Updated Hypothetical Model of Dynamic Biomarkers. Lancet Neurol. 2013, 12, 207–216. [Google Scholar] [CrossRef] [Green Version]
- Greene, J.D.; Baddeley, A.D.; Hodges, J.R. Analysis of the Episodic Memory Deficit in Early Alzheimer’s Disease: Evidence from the Doors and People Test. Neuropsychologia 1996, 34, 537–551. [Google Scholar] [CrossRef]
- Gainotti, G.; Marra, C.; Villa, G.; Parlato, V.; Chiarotti, F. Sensitivity and Specificity of Some Neuropsychological Markers of Alzheimer Dementia. Alzheimer Dis. Assoc. Disord. 1998, 12, 152–162. [Google Scholar] [CrossRef]
- Dubois, B.; Feldman, H.H.; Jacova, C.; Dekosky, S.T.; Barberger-Gateau, P.; Cummings, J.; Delacourte, A.; Galasko, D.; Gauthier, S.; Jicha, G.; et al. Research Criteria for the Diagnosis of Alzheimer’s Disease: Revising the NINCDS-ADRDA Criteria. Lancet Neurol. 2007, 6, 734–746. [Google Scholar] [CrossRef] [PubMed]
- Stopford, C.L.; Thompson, J.C.; Neary, D.; Richardson, A.M.T.; Snowden, J.S. Working Memory, Attention, and Executive Function in Alzheimer’s Disease and Frontotemporal Dementia. Cortex 2012, 48, 429–446. [Google Scholar] [CrossRef]
- Ong, K.T.; Villemagne, V.L.; Bahar-Fuchs, A.; Lamb, F.; Langdon, N.; Catafau, A.M.; Stephens, A.W.; Seibyl, J.; Dinkelborg, L.M.; Reininger, C.B.; et al. Aβ Imaging with 18F-Florbetaben in Prodromal Alzheimer’s Disease: A Prospective Outcome Study. J. Neurol. Neurosurg. Psychiatry 2015, 86, 431–436. [Google Scholar] [CrossRef]
- Wagner, M.; Wolf, S.; Reischies, F.M.; Daerr, M.; Wolfsgruber, S.; Jessen, F.; Popp, J.; Maier, W.; Hüll, M.; Frölich, L.; et al. Biomarker Validation of a Cued Recall Memory Deficit in Prodromal Alzheimer Disease. Neurology 2012, 78, 379–386. [Google Scholar] [CrossRef]
- Brugnolo, A.; Morbelli, S.; Arnaldi, D.; De Carli, F.; Accardo, J.; Bossert, I.; Dessi, B.; Famà, F.; Ferrara, M.; Girtler, N.; et al. Metabolic Correlates of Rey Auditory Verbal Learning Test in Elderly Subjects with Memory Complaints. J. Alzheimer’s Dis. 2014, 39, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Ray, A. L’examen Clinique En Psychologie; Presse Universitaires de France: Paris, France, 1964. [Google Scholar]
- Ray, A. L’examen Psychologique Dans Les Cas d’encephopathie Traumatique. Arch. De Psychol. 1941, 28, 21. [Google Scholar]
- Schmidt, M. Rey Auditory Verbal Learning Test: A Handbook; Western Psychological Services: Los Angeles, CA, USA, 1996. [Google Scholar]
- Wechsler, D. A Standardized Memory Scale for Clinical Use. J. Psychol. 1945, 19, 87–95. [Google Scholar] [CrossRef]
- Abikoff, H.; Alvir, J.; Hong, G.; Sukoff, R.; Orazio, J.; Solomon, S.; Saravay, S. Logical Memory Subtest of the Wechsler Memory Scale: Age and Education Norms and Alternate-Form Reliability of Two Scoring Systems. J. Clin. Exp. Neuropsychol. 1987, 9, 435–448. [Google Scholar] [CrossRef]
- Desgranges, B.; Baron, J.-C.; Lalevée, C.; Giffard, B.; Viader, F.; de La Sayette, V.; Eustache, F. The Neural Substrates of Episodic Memory Impairment in Alzheimer’s Disease as Revealed by FDG-PET: Relationship to Degree of Deterioration. Brain 2002, 125, 1116–1124. [Google Scholar] [CrossRef]
- Mormino, E.C.; Kluth, J.T.; Madison, C.M.; Rabinovici, G.D.; Baker, S.L.; Miller, B.L.; Koeppe, R.A.; Mathis, C.A.; Weiner, M.W.; Jagust, W.J.; et al. Episodic Memory Loss Is Related to Hippocampal-Mediated Beta-Amyloid Deposition in Elderly Subjects. Brain 2009, 132, 1310–1323. [Google Scholar] [CrossRef]
- Perani, D.; Bressi, S.; Cappa, S.F.; Vallar, G.; Alberoni, M.; Grassi, F.; Caltagirone, C.; Cipolotti, L.; Franceschi, M.; Lenzi, G.L. Evidence of Multiple Memory Systems in the Human Brain. A [18F]FDG PET Metabolic Study. Brain 1993, 116, 903–919. [Google Scholar] [CrossRef]
- Slansky, I.; Herholz, K.; Pietrzyk, U.; Kessler, J.; Grond, M.; Mielke, R.; Heiss, W.D. Cognitive Impairment in Alzheimer’s Disease Correlates with Ventricular Width and Atrophy-Corrected Cortical Glucose Metabolism. Neuroradiology 1995, 37, 270–277. [Google Scholar] [CrossRef]
- Desgranges, B.; Baron, J.C.; de la Sayette, V.; Petit-Taboué, M.C.; Benali, K.; Landeau, B.; Lechevalier, B.; Eustache, F. The Neural Substrates of Memory Systems Impairment in Alzheimer’s Disease. A PET Study of Resting Brain Glucose Utilization. Brain 1998, 121, 611–631. [Google Scholar] [CrossRef] [Green Version]
- Eustache, F.; Desgranges, B.; Giffard, B.; de la Sayette, V.; Baron, J.C. Entorhinal Cortex Disruption Causes Memory Deficit in Early Alzheimer’s Disease as Shown by PET. Neuroreport 2001, 12, 683–685. [Google Scholar] [CrossRef]
- Teipel, S.J.; Willoch, F.; Ishii, K.; Bürger, K.; Drzezga, A.; Engel, R.; Bartenstein, P.; Möller, H.-J.; Schwaiger, M.; Hampel, H. Resting State Glucose Utilization and the CERAD Cognitive Battery in Patients with Alzheimer’s Disease. Neurobiol. Aging 2006, 27, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Edison, P.; Archer, H.A.; Hinz, R.; Hammers, A.; Pavese, N.; Tai, Y.F.; Hotton, G.; Cutler, D.; Fox, N.; Kennedy, A.; et al. Amyloid, Hypometabolism, and Cognition in Alzheimer Disease: An [11C]PIB and [18F]FDG PET Study. Neurology 2007, 68, 501–508. [Google Scholar] [CrossRef]
- Förster, S.; Yousefi, B.H.; Wester, H.-J.; Klupp, E.; Rominger, A.; Förstl, H.; Kurz, A.; Grimmer, T.; Drzezga, A. Quantitative Longitudinal Interrelationships between Brain Metabolism and Amyloid Deposition during a 2-Year Follow-up in Patients with Early Alzheimer’s Disease. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 1927–1936. [Google Scholar] [CrossRef] [PubMed]
- Chetelat, G.; Desgranges, B.; de la Sayette, V.; Viader, F.; Berkouk, K.; Landeau, B.; Lalevée, C.; Le Doze, F.; Dupuy, B.; Hannequin, D.; et al. Dissociating Atrophy and Hypometabolism Impact on Episodic Memory in Mild Cognitive Impairment. Brain 2003, 126, 1955–1967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, L.; Rowley, J.; Mohades, S.; Leuzy, A.; Dauar, M.T.; Shin, M.; Fonov, V.; Jia, J.; Gauthier, S.; Rosa-Neto, P.; et al. Dissociation between Brain Amyloid Deposition and Metabolism in Early Mild Cognitive Impairment. PLoS ONE 2012, 7, e47905. [Google Scholar] [CrossRef]
- Collins, D.L.; Neelin, P.; Peters, T.M.; Evans, A.C. Automatic 3D Intersubject Registration of MR Volumetric Data in Standardized Talairach Space. J. Comput. Assist. Tomogr. 1994, 18, 192–205. [Google Scholar] [CrossRef]
- Petersen, R.C.; Smith, G.E.; Ivnik, R.J.; Kokmen, E.; Tangalos, E.G. Memory Function in Very Early Alzheimer’s Disease. Neurology 1994, 44, 867–872. [Google Scholar] [CrossRef]
- Nellessen, N.; Rottschy, C.; Eickhoff, S.B.; Ketteler, S.T.; Kuhn, H.; Shah, N.J.; Schulz, J.B.; Reske, M.; Reetz, K. Specific and Disease Stage-Dependent Episodic Memory-Related Brain Activation Patterns in Alzheimer’s Disease: A Coordinate-Based Meta-Analysis. Brain Struct. Funct. 2015, 220, 1555–1571. [Google Scholar] [CrossRef] [PubMed]
- Doi, T.; Shimada, H.; Makizako, H.; Yoshida, D.; Shimokata, H.; Ito, K.; Washimi, Y.; Endo, H.; Suzuki, T. Characteristics of Cognitive Function in Early and Late Stages of Amnestic Mild Cognitive Impairment. Geriatr. Gerontol. Int. 2013, 13, 83–89. [Google Scholar] [CrossRef]
- Jessen, F.; Wolfsgruber, S.; Wiese, B.; Bickel, H.; Mösch, E.; Kaduszkiewicz, H.; Pentzek, M.; Riedel-Heller, S.G.; Luck, T.; Fuchs, A.; et al. AD Dementia Risk in Late MCI, in Early MCI, and in Subjective Memory Impairment. Alzheimer’s Dement. 2014, 10, 76–83. [Google Scholar] [CrossRef]
- Aisen, P.S.; Petersen, R.C.; Donohue, M.C.; Gamst, A.; Raman, R.; Thomas, R.G.; Walter, S.; Trojanowski, J.Q.; Shaw, L.M.; Beckett, L.A.; et al. Clinical Core of the Alzheimer’s Disease Neuroimaging Initiative: Progress and Plans. Alzheimer’s Dement. 2010, 6, 239–246. [Google Scholar] [CrossRef]
- Tierney, M.C.; Fisher, R.H.; Lewis, A.J.; Zorzitto, M.L.; Snow, W.G.; Reid, D.W.; Nieuwstraten, P. The NINCDS-ADRDA Work Group Criteria for the Clinical Diagnosis of Probable Alzheimer’s Disease: A Clinicopathologic Study of 57 Cases. Neurology 1988, 38, 359–364. [Google Scholar] [CrossRef]
- Collins, D.L.; Zijdenbos, A.P.; Baaré, W.F.C.; Evans, A.C. ANIMAL+INSECT: Improved Cortical Structure Segmentation. In Information Processing in Medical Imaging; Lecture Notes in Computer Science; Kuba, A., Šáamal, M., Todd-Pokropek, A., Eds.; Springer: Berlin/Heidelberg, Germany, 1999; Volume 1613, pp. 210–223. [Google Scholar] [CrossRef]
- Rosenberg, P.B.; Wong, D.F.; Edell, S.L.; Ross, J.S.; Joshi, A.D.; Brašić, J.R.; Zhou, Y.; Raymont, V.; Kumar, A.; Ravert, H.T.; et al. Cognition and Amyloid Load in Alzheimer Disease Imaged with Florbetapir F 18(AV-45) Positron Emission Tomography. Am. J. Geriatr. Psychiatry 2013, 21, 272–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grimmer, T.; Henriksen, G.; Wester, H.-J.; Förstl, H.; Klunk, W.E.; Mathis, C.A.; Kurz, A.; Drzezga, A. Clinical Severity of Alzheimer’s Disease Is Associated with PIB Uptake in PET. Neurobiol. Aging 2009, 30, 1902–1909. [Google Scholar] [CrossRef] [PubMed]
- Worsley, K.J.; Taylor, J.E.; Tomaiuolo, F.; Lerch, J. Unified Univariate and Multivariate Random Field Theory. Neuroimage 2004, 23 (Suppl. 1), S189–S195. [Google Scholar] [CrossRef] [PubMed]
- Woost, T.B.; Dukart, J.; Frisch, S.; Barthel, H.; Sabri, O.; Mueller, K.; Schroeter, M.L. Neural Correlates of the DemTect in Alzheimer’s Disease and Frontotemporal Lobar Degeneration—A Combined MRI & FDG-PET Study. Neuroimage Clin. 2013, 2, 746–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butters, N.; Wolfe, J.; Martone, M.; Granholm, E.; Cermak, L.S. Memory Disorders Associated with Huntington’s Disease: Verbal Recall, Verbal Recognition and Procedural Memory. Neuropsychologia 1985, 23, 729–743. [Google Scholar] [CrossRef] [PubMed]
- Bigler, E.D.; Rosa, L.; Schultz, F.; Hall, S.; Harris, J. Rey-Auditory Verbal Learning and Rey-Osterrieth Complex Figure Design Performance in Alzheimer’s Disease and Closed Head Injury. J. Clin. Psychol. 1989, 45, 277–280. [Google Scholar] [CrossRef]
- Moore, P.M.; Baker, G.A. Validation of the Wechsler Memory Scale-Revised in a Sample of People with Intractable Temporal Lobe Epilepsy. Epilepsia 1996, 37, 1215–1220. [Google Scholar] [CrossRef]
- Schoenberg, M.R.; Dawson, K.A.; Duff, K.; Patton, D.; Scott, J.G.; Adams, R.L. Test Performance and Classification Statistics for the Rey Auditory Verbal Learning Test in Selected Clinical Samples. Arch. Clin. Neuropsychol. 2006, 21, 693–703. [Google Scholar] [CrossRef]
- Longoni, G.; Rocca, M.A.; Pagani, E.; Riccitelli, G.C.; Colombo, B.; Rodegher, M.; Falini, A.; Comi, G.; Filippi, M. Deficits in Memory and Visuospatial Learning Correlate with Regional Hippocampal Atrophy in MS. Brain Struct. Funct. 2015, 220, 435–444. [Google Scholar] [CrossRef] [PubMed]
- Price, L.; Said, K.; Haaland, K.Y. Age-Associated Memory Impairment of Logical Memory and Visual Reproduction. J. Clin. Exp. Neuropsychol. 2004, 26, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Shallice, T.; Fletcher, P.; Frith, C.D.; Grasby, P.; Frackowiak, R.S.; Dolan, R.J. Brain Regions Associated with Acquisition and Retrieval of Verbal Episodic Memory. Nature 1994, 368, 633–635. [Google Scholar] [CrossRef] [Green Version]
- Engler, H.; Forsberg, A.; Almkvist, O.; Blomquist, G.; Larsson, E.; Savitcheva, I.; Wall, A.; Ringheim, A.; Långström, B.; Nordberg, A. Two-Year Follow-up of Amyloid Deposition in Patients with Alzheimer’s Disease. Brain 2006, 129, 2856–2866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishi, H.; Sawamoto, N.; Namiki, C.; Yoshida, H.; Dinh, H.D.T.; Ishizu, K.; Hashikawa, K.; Fukuyama, H. Correlation between Cognitive Deficits and Glucose Hypometabolism in Mild Cognitive Impairment. J. Neuroimaging 2010, 20, 29–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habeck, C.; Risacher, S.; Lee, G.J.; Glymour, M.M.; Mormino, E.; Mukherjee, S.; Kim, S.; Nho, K.; DeCarli, C.; Saykin, A.J.; et al. Relationship between Baseline Brain Metabolism Measured Using [18F]FDG PET and Memory and Executive Function in Prodromal and Early Alzheimer’s Disease. Brain Imaging Behav. 2012, 6, 568–583. [Google Scholar] [CrossRef] [Green Version]
- Frisch, S.; Dukart, J.; Vogt, B.; Horstmann, A.; Becker, G.; Villringer, A.; Barthel, H.; Sabri, O.; Müller, K.; Schroeter, M.L. Dissociating Memory Networks in Early Alzheimer’s Disease and Frontotemporal Lobar Degeneration—A Combined Study of Hypometabolism and Atrophy. PLoS ONE 2013, 8, e55251. [Google Scholar] [CrossRef] [Green Version]
- Schönknecht, O.D.P.; Hunt, A.; Toro, P.; Guenther, T.; Henze, M.; Haberkorn, U.; Schröder, J. Bihemispheric Cerebral FDG PET Correlates of Cognitive Dysfunction as Assessed by the CERAD in Alzheimer’s Disease. Clin. EEG Neurosci. 2011, 42, 71–76. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| CN (n = 169) | EMCI (n = 134) | LMCI (n = 65) | AD (n = 84) | p-Value | |
|---|---|---|---|---|---|
| Sex (M/F) | 86/83 | 72/62 | 39/26 | 50/34 | 0.463 |
| Age (years) | 77.6 ± 6.5 | 73.6 ± 8.2 a | 77.6 ± 7.6 b | 76.8 ± 7.3 d | <0.001 |
| Education (years) | 16.5 ± 2.7 | 15.7 ± 2.7 | 16.2 ± 2.7 | 16.3 ± 2.6 | 0.068 |
| MMSE | 29.0 ± 1.3 | 28.4 ± 1.6 | 27.5 ± 2.1 a | 21.4 ± 4.5 abc | <0.001 |
| Logical memory 30 min delay recall | 14.5 ± 3.6 | 11.8 ± 3.7 a | 4.1 ± 2.8 ab | 1.7 ± 2.8 abc | <0.001 |
| Rey Auditory Verbal Learning Test 30 min delay recall | 8.1 ± 4.1 | 5.6 ± 4.5 a | 2.7 ± 3.3 ab | 0.7 ± 2.3 abc | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tedeschi Dauar, M.; Pascoal, T.A.; Therriault, J.; Rowley, J.; Mohaddes, S.; Shin, M.; Zimmer, E.R.; Eskildsen, S.F.; Fonov, V.S.; Gauthier, S.; et al. Dynamic Amyloid and Metabolic Signatures of Delayed Recall Performance within the Clinical Spectrum of Alzheimer’s Disease. Brain Sci. 2023, 13, 232. https://doi.org/10.3390/brainsci13020232
Tedeschi Dauar M, Pascoal TA, Therriault J, Rowley J, Mohaddes S, Shin M, Zimmer ER, Eskildsen SF, Fonov VS, Gauthier S, et al. Dynamic Amyloid and Metabolic Signatures of Delayed Recall Performance within the Clinical Spectrum of Alzheimer’s Disease. Brain Sciences. 2023; 13(2):232. https://doi.org/10.3390/brainsci13020232
Chicago/Turabian StyleTedeschi Dauar, Marina, Tharick Ali Pascoal, Joseph Therriault, Jared Rowley, Sara Mohaddes, Monica Shin, Eduardo R. Zimmer, Simon Fristed Eskildsen, Vladimir S. Fonov, Serge Gauthier, and et al. 2023. "Dynamic Amyloid and Metabolic Signatures of Delayed Recall Performance within the Clinical Spectrum of Alzheimer’s Disease" Brain Sciences 13, no. 2: 232. https://doi.org/10.3390/brainsci13020232