
Balance Training with Weight Shift-Triggered Electrical Stimulation for Stroke Patients: A Randomized Controlled Trial
Abstract
:1. Introduction
2. Materials and Methods
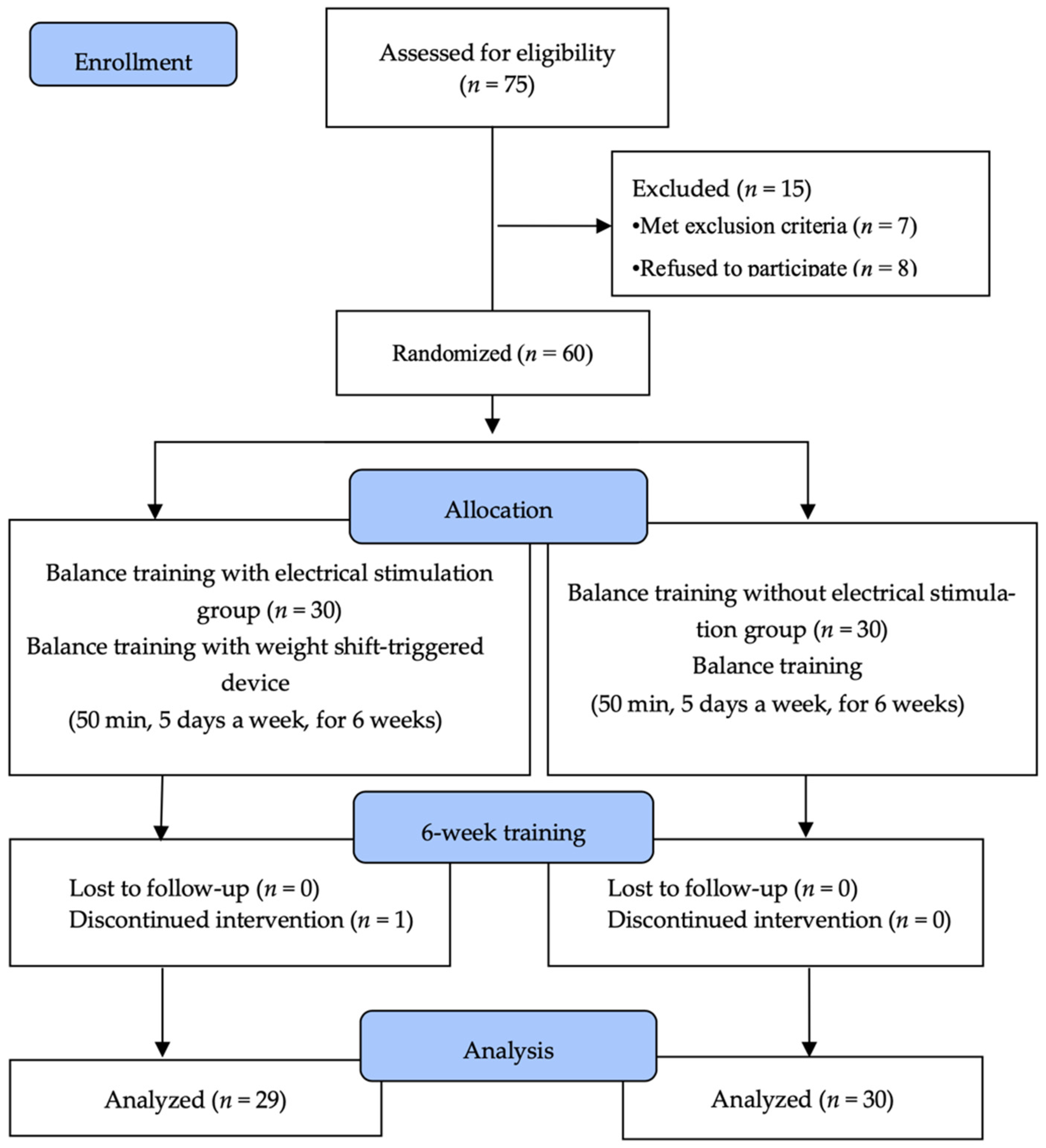
2.1. Subjects
2.2. Experimental Procedure
2.3. Experimental Method
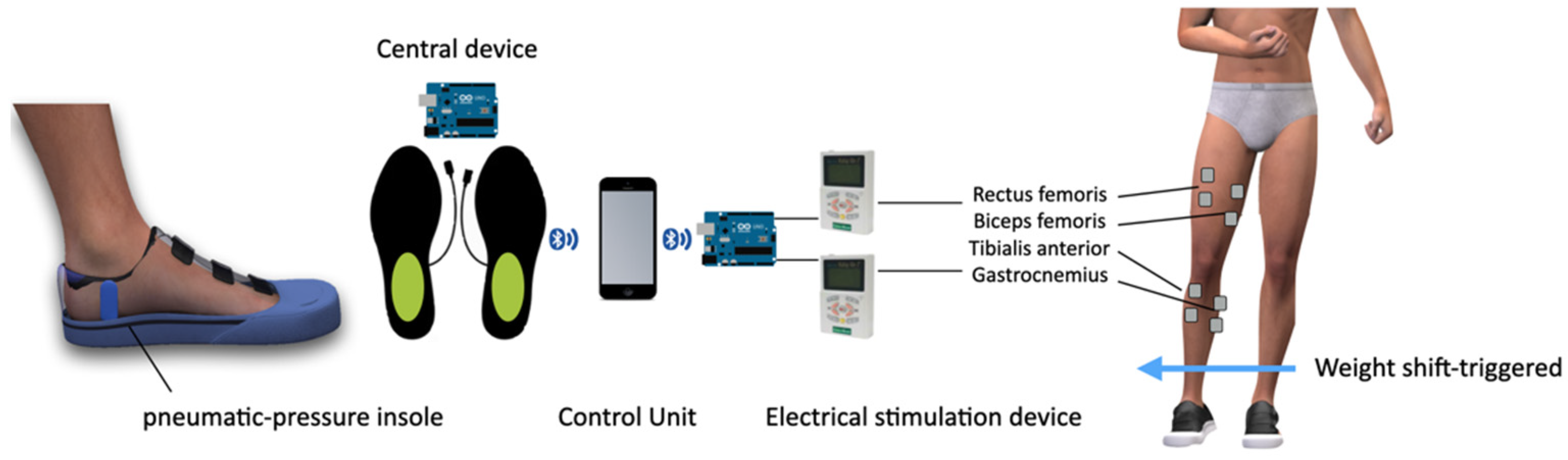
2.3.1. Weight Shift-Triggered Electrical Stimulation Device
2.3.2. Balance Training Program
2.4. Outcome Measurements
2.4.1. Static Balance Ability
2.4.2. Dynamic Balance Ability
2.4.3. Lower-Extremity Motor Function
2.4.4. Activities of Daily Living (ADL)
2.5. Data Analysis
3. Results
3.1. General Characteristics of the Subjects
3.2. Changes in Static Balance Ability
3.3. Changes in Dynamic Balance Ability
3.4. Changes in Lower-Extremity Motor Function and ADL
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Jonsson, E.; Henriksson, M.; Hirschfeld, H. Age-related differences in postural adjustments in connection with different tasks involving weight transfer while standing. Gait Posture 2007, 26, 508–515. [Google Scholar] [CrossRef] [PubMed]
- Adegoke, B.O.; Olaniyi, O.; Akosile, C.O. Weight bearing asymmetry and functional ambulation performance in stroke survivors. Glob. J. Health Sci. 2012, 4, 87–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laufer, Y.; Dickstein, R.; Resnik, S.; Marcovitz, E. Weight-bearing shifts of hemiparetic and healthy adults upon stepping on stairs of various heights. Clin. Rehabil. 2000, 14, 125–129. [Google Scholar] [CrossRef]
- Dickstein, R.; Nissan, M.; Pillar, T.; Scheer, D. Foot-ground pressure pattern of standing hemiplegic patients. Major characteristics and patterns of improvement. Phys. Ther. 1984, 64, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Mizrahi, J.; Solzi, P.; Ring, H.; Nisell, R. Postural stability in stroke patients: Vectorial expression of asymmetry, sway activity and relative sequence of reactive forces. Med. Biol. Eng. Comput. 1989, 27, 181–190. [Google Scholar] [CrossRef]
- Eng, J.J.; Chu, K.S. Reliability and comparison of weight-bearing ability during standing tasks for individuals with chronic stroke. Arch. Phys. Med. Rehabil. 2002, 83, 1138–1144. [Google Scholar] [CrossRef] [Green Version]
- Umemura, G.S.; Makhoul, M.P.; Torriani-Pasin, C.; Forner-Cordero, A. Circadian parameter as a possible indicator of gait performance and daily activity levels in chronic stroke survivors. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2022, 2022, 4370–4373. [Google Scholar] [PubMed]
- Aries, A.M.; Downing, P.; Sim, J.; Hunter, S.M. Effectiveness of somatosensory stimulation for the lower limb and foot to improve balance and gait after stroke: A systematic review. Brain Sci. 2022, 12, 1102. [Google Scholar] [CrossRef]
- Knutson, J.S.; Fu, M.J.; Sheffler, L.R.; Chae, J. Neuromuscular electrical stimulation for motor restoration in hemiplegia. Phys. Med. Rehabil. Clin. N. Am. 2015, 26, 729–745. [Google Scholar] [CrossRef] [Green Version]
- Hong, Z.; Sui, M.; Zhuang, Z.; Liu, H.; Zheng, X.; Cai, C.; Jin, D. Effectiveness of neuromuscular electrical stimulation on lower limbs of patients with hemiplegia after chronic stroke: A systematic review. Arch. Phys. Med. Rehabil. 2018, 99, 1011–1022. [Google Scholar] [CrossRef] [PubMed]
- Riaz, M.T.; AlSanad, A.A.; Ahmad, S.; Akbar, M.A.; AlSuwaidan, L.; Al, A.H.A.; AlSagri, H.S. A wireless controlled intelligent healthcare system for diplegia patients. Math. Biosci. Eng. 2022, 19, 456–472. [Google Scholar] [CrossRef] [PubMed]
- Luque-Moreno, C.; Oliva-Pascual-Vaca, A.; Kiper, P.; Rodriguez-Blanco, C.; Agostini, M.; Turolla, A. Virtual reality to assess and treat lower extremity disorders in post-stroke patients. Methods Inf. Med. 2016, 55, 89–92. [Google Scholar] [PubMed]
- Liu, X.; Zhao, C.; Zheng, B.; Guo, Q.; Duan, X.; Wulamu, A.; Zhang, D. Wearable devices for gait analysis in intelligent healthcare. Front. Comput. Sci. 2021, 3, 661676. [Google Scholar] [CrossRef]
- Bowman, T.; Gervasoni, E.; Arienti, C.; Lazzarini, S.G.; Negrini, S.; Crea, S.; Cattaneo, D.; Carrozza, M.C. Wearable devices for biofeedback rehabilitation: A systematic review and meta-analysis to design application rules and estimate the effectiveness on balance and gait outcomes in neurological diseases. Sensors 2021, 21, 3444. [Google Scholar] [CrossRef] [PubMed]
- De Nunzio, A.; Zucchella, C.; Spicciato, F.; Tortola, P.; Vecchione, C.; Pierelli, F.; Bartolo, M. Biofeedback rehabilitation of posture and weightbearing distribution in stroke: A center of foot pressure analysis. Funct. Neurol. 2014, 29, 127–134. [Google Scholar]
- Stanton, R.; Ada, L.; Dean, C.M.; Preston, E. Biofeedback improves activities of the lower limb after stroke: A systematic review. J. Physiother. 2011, 57, 145–155. [Google Scholar] [CrossRef] [Green Version]
- Delgado-Gonzalo, R.; Hubbard, J.; Renevey, P.; Lemkaddem, A.; Vellinga, Q.; Ashby, D.; Willardson, J.; Bertschi, M. Real-time gait analysis with accelerometer-based smart shoes. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Republic of Korea, 11–15 July 2017. [Google Scholar]
- Kim, S.H.; Huizenga, D.E.; Handzic, I.; Ditwiler, R.E.; Lazinski, M.; Ramakrishnan, T.; Bozeman, A.; Rose, D.Z.; Reed, K.B. Relearning functional and symmetric walking after stroke using a wearable device: A feasibility study. J. Neuroeng. Rehabil. 2019, 16, 106. [Google Scholar] [CrossRef] [Green Version]
- Saghaei, M. Random allocation software for parallel group randomized trials. BMC Med. Res. Methodol. 2004, 4, 26. [Google Scholar] [CrossRef] [Green Version]
- Clark, B.C.; Manini, T.M.; Ordway, N.R.; Ploutz-Snyder, L.L. Leg muscle activity during walking with assistive devices at varying levels of weight bearing. Arch. Phys. Med. Rehabil. 2004, 85, 1555–1560. [Google Scholar] [CrossRef]
- Flaxman, T.E.; Speirs, A.D.; Benoit, D.L. Joint stabilisers or moment actuators: The role of knee joint muscles while weight-bearing. J. Biomech. 2012, 45, 2570–2576. [Google Scholar] [CrossRef] [PubMed]
- Madhavan, S.; Shields, R.K. Weight-bearing exercise accuracy influences muscle activation strategies of the knee. J. Neurol. Phys. Ther. 2007, 31, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.; Lee, K.; Kim, M.; Song, C. Audiovisual biofeedback-based trunk stabilization training using a pressure biofeedback system in stroke patients: A randomized, single-blinded study. Stroke Res. Treat. 2017, 2017, 6190593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maciaszek, J. Effects of posturographic platform biofeedback training on the static and dynamic balance of older stroke patients. J. Stroke Cerebrovasc. Dis. 2018, 27, 1969–1974. [Google Scholar] [CrossRef]
- Maciaszek, J.; Borawska, S.; Wojcikiewicz, J. Influence of posturographic platform biofeedback training on the dynamic balance of adult stroke patients. J. Stroke Cerebrovasc. Dis. 2014, 23, 1269–1274. [Google Scholar] [CrossRef]
- Era, P.; Sainio, P.; Koskinen, S.; Haavisto, P.; Vaara, M.; Aromaa, A. Postural balance in a random sample of 7979 subjects aged 30 years and over. Gerontology 2006, 52, 204–213. [Google Scholar] [CrossRef]
- Ng, S.S.; Hui-Chan, C.W. The timed up & go test: Its reliability and association with lower-limb impairments and locomotor capacities in people with chronic stroke. Arch. Phys. Med. Rehabil. 2005, 86, 1641–1647. [Google Scholar]
- Katz-Leurer, M.; Fisher, I.; Neeb, M.; Schwartz, I.; Carmeli, E. Reliability and validity of the modified functional reach test at the sub-acute stage post-stroke. Disabil. Rehabil. 2009, 31, 243–248. [Google Scholar] [CrossRef]
- Downs, S.; Marquez, J.; Chiarelli, P. The berg balance scale has high intra- and inter-rater reliability but absolute reliability varies across the scale: A systematic review. J. Physiother. 2013, 59, 93–99. [Google Scholar] [CrossRef] [Green Version]
- Duncan, P.W.; Propst, M.; Nelson, S.G. Reliability of the fugl-meyer assessment of sensorimotor recovery following cerebrovascular accident. Phys. Ther. 1983, 63, 1606–1610. [Google Scholar] [CrossRef]
- Ohura, T.; Hase, K.; Nakajima, Y.; Nakayama, T. Validity and reliability of a performance evaluation tool based on the modified barthel index for stroke patients. BMC Med. Res. Methodol. 2017, 17, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Vliet, P.M.; Wulf, G. Extrinsic feedback for motor learning after stroke: What is the evidence? Disabil. Rehabil. 2006, 28, 831–840. [Google Scholar] [CrossRef]
- Chastan, N.; Westby, G.W.; du Montcel, S.T.; Do, M.C.; Chong, R.K.; Agid, Y.; Welter, M.L. Influence of sensory inputs and motor demands on the control of the centre of mass velocity during gait initiation in humans. Neurosci. Lett. 2010, 469, 400–404. [Google Scholar] [CrossRef]
- Hansson, E.E.; Beckman, A.; Hakansson, A. Effect of vision, proprioception, and the position of the vestibular organ on postural sway. Acta Otolaryngol. 2010, 130, 1358–1363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marigold, D.S.; Eng, J.J. The relationship of asymmetric weight-bearing with postural sway and visual reliance in stroke. Gait Posture 2006, 23, 249–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobo, A.A.; Joshua, A.M.; Nayak, A.; Mithra, P.P.; Misri, Z.; Pai, S. Effect of compelled body weight shift (cbws) therapy in comparison to proprioceptivetraining on functional balance, gait, andmuscle strength among acute stroke subjects. Ann. Neurosci. 2021, 28, 162–169. [Google Scholar] [CrossRef]
- Lobo, A.A.; Joshua, A.M.; Nayak, A. Effects of compelled body weight shift therapy on weight-bearing symmetry, balance and gait in patients with stroke: A narrative review. Crit. Rev.™ Phys. Rehabil. Med. 2021, 33, 45–64. [Google Scholar] [CrossRef]
- Cha, J.H.; Kim, N.H.; Cha, Y.J. Effect of proprioceptive stimulation induced by footplate during center of pressure movement tracking training on the balance abilities of patients with chronic hemiplegic stroke: A randomized, controlled, pilot study. Top. Stroke Rehabil. 2020, 27, 38–43. [Google Scholar] [CrossRef]
- Wrisley, D.M.; Kumar, N.A. Functional gait assessment: Concurrent, discriminative, and predictive validity in community-dwelling older adults. Phys. Ther. 2010, 90, 761–773. [Google Scholar] [CrossRef] [Green Version]
- Suputtitada, A.; Yooktanan, P.; Rarerng-Ying, T. Effect of partial body weight support treadmill training in chronic stroke patients. J. Med. Assoc.Thai. 2004, 87 (Suppl. S2), S107–S111. [Google Scholar]
- Ivey, F.M.; Hafer-Macko, C.E.; Macko, R.F. Task-oriented treadmill exercise training in chronic hemiparetic stroke. J. Rehabil. Res. Dev. 2008, 45, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, B.; Parvataneni, K.; Olney, S.J. A comparison of gait biomechanics and metabolic requirements of overground and treadmill walking in people with stroke. Clin. Biomech. 2009, 24, 729–734. [Google Scholar] [CrossRef]
- Alhirsan, S.M.; Capo-Lugo, C.E.; Brown, D.A. Effects of different types of augmented feedback on intrinsic motivation and walking speed performance in post-stroke: A study protocol. Contemp. Clin. Trials Commun. 2021, 24, 100863. [Google Scholar] [CrossRef]
- Lin, S.; Mann, J.; Mansfield, A.; Wang, R.H.; Harris, J.E.; Taati, B. Investigating the feasibility and acceptability of real-time visual feedback in reducing compensatory motions during self-administered stroke rehabilitation exercises: A pilot study with chronic stroke survivors. J. Rehabil. Assist. Technol. Eng. 2019, 6, 2055668319831631. [Google Scholar] [CrossRef] [PubMed]
- Ray, C.T.; Horvat, M.; Croce, R.; Mason, R.C.; Wolf, S.L. The impact of vision loss on postural stability and balance strategies in individuals with profound vision loss. Gait Posture 2008, 28, 58–61. [Google Scholar] [CrossRef]
- Tsaklis, P.V.; Grooten, W.J.; Franzen, E. Effects of weight-shift training on balance control and weight distribution in chronic stroke: A pilot study. Top. Stroke Rehabil. 2012, 19, 23–31. [Google Scholar] [CrossRef]
- Mahmoudi, Z.; Mohammadi, R.; Sadeghi, T.; Kalbasi, G. The effects of electrical stimulation of lower extremity muscles on balance in stroke patients: A systematic review of literatures. J. Stroke Cerebrovasc. Dis. 2021, 30, 105793. [Google Scholar] [CrossRef] [PubMed]
- Satjanitikun, A.; Pichaiyongwongdee, S.; Jalayondeja, C. Correlation between weight transfer on paretic limb while standing in three directions and fugl-meyer assessment for lower extremities in individuals with stroke. J. Med. Assoc. Thai. 2015, 98 (Suppl. S5), S1–S5. [Google Scholar] [PubMed]
- Knutson, J.S.; Hansen, K.; Nagy, J.; Bailey, S.N.; Gunzler, D.D.; Sheffler, L.R.; Chae, J. Contralaterally controlled neuromuscular electrical stimulation for recovery of ankle dorsiflexion: A pilot randomized controlled trial in patients with chronic post-stroke hemiplegia. Am. J. Phys. Med. Rehabil. 2013, 92, 656–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohapatra, S.; Eviota, A.C.; Ringquist, K.L.; Muthukrishnan, S.R.; Aruin, A.S. Compelled body weight shift technique to facilitate rehabilitation of individuals with acute stroke. ISRN Rehabil. 2012, 2012, 328018. [Google Scholar] [CrossRef] [Green Version]
- Aphiphaksakul, P.; Siriphorn, A. Home-based exercise using balance disc and smartphone inclinometer application improves balance and activity of daily living in individuals with stroke: A randomized controlled trial. PLoS ONE 2022, 17, e0277870. [Google Scholar] [CrossRef] [PubMed]
- van Dijk, M.M.; Meyer, S.; Sandstad, S.; Wiskerke, E.; Thuwis, R.; Vandekerckhove, C.; Myny, C.; Ghosh, N.; Beyens, H.; Dejaeger, E.; et al. A cross-sectional study comparing lateral and diagonal maximum weight shift in people with stroke and healthy controls and the correlation with balance, gait and fear of falling. PLoS ONE 2017, 12, e0183020. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| BT-ESG (n = 29) | BTG (n = 30) | χ2/t | p | |
|---|---|---|---|---|
| Age (year) | 66.24 ± 7.01 | 68.87 ± 7.30 | 1.409 | 0.164 |
| Height (cm) | 163.48 ± 7.46 | 161.93 ± 10.20 | 0.664 | 0.509 |
| Weight (kg) | 60.50 ± 8.01 | 60.93 ± 8.64 | 0.199 | 0.843 |
| Body mass index (point) | 22.60 ± 2.34 | 23.16 ± 1.81 | 1.033 | 0.306 |
| Duration of stroke (month) | 14.17 ± 5.87 | 16.33 ± 5.84 | 1.417 | 0.162 |
| MMSE | 25.83 ± 1.23 | 25.53 ± 1.01 | 1.008 | 0.318 |
| MBI | 52.99 ± 8.52 | 54.92 ± 8.96 | 0.846 | 0.401 |
| Gender (male/female) | 16/13 | 17/13 | 0.013 | 0.908 |
| Paretic side (right/left) | 15/14 | 20/10 | 0.243 | 1.364 |
| Stroke type (infarction/hemorrhage) | 19/10 | 18/12 | 0.661 | 0.192 |
| BT-ESG (n = 29) | BTG (n = 30) | Time F(p) | Interaction F(p) | Effect Size (d) | CI for Differences | |||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| EO M-L speed (mm/s) | Pre | 4.08 ± 1.36 | 4.12 ± 1.36 | |||||
| Post | 2.93 ± 0.66 | 3.56 ± 1.02 | 50.691 | 6.115 | −1.07 | −0.11 | ||
| Pre–Post | −1.15 ± 1.01 * | −0.56 ± 0.83 * | (0.000) | (0.016) | 0.64 | |||
| EO A-P speed (mm/s) | Pre | 5.99 ± 1.49 | 6.17 ± 1.28 | |||||
| Post | 4.70 ± 1.42 | 5.50 ± 1.33 | 127.546 | 12.789 | −0.97 | −0.27 | ||
| Pre–Post | −1.30 ± 0.76 * | −0.67 ± 0.57 * | (0.000) | (0.001) | 0.93 | |||
| EO Velocity moment (mm2/s) | Pre | 4.33 ± 1.41 | 4.28 ± 1.17 | |||||
| Post | 2.84 ± 1.40 | 3.52 ± 1.24 | 108.358 | 11.436 | −1.16 | −0.30 | ||
| Pre–Post | −1.48 ± 0.69 * | −0.76 ± 0.94 * | (0.000) | (0.001) | 0.88 | |||
| EC M-L speed (mm/s) | Pre | 4.35 ± 1.36 | 4.39 ± 0.97 | |||||
| Post | 3.21 ± 0.93 | 3.88 ± 1.11 | 83.943 | 12.052 | −0.99 | −0.26 | ||
| Pre–Post | −1.14 ± 0.75 * | −0.51 ± 0.63 * | (0.000) | (0.001) | 0.90 | |||
| EC A-P speed (mm/s) | Pre | 5.92 ± 1.76 | 5.57 ± 0.81 | |||||
| Post | 5.02 ± 1.42 | 5.11 ± 0.91 | 91.159 | 9.877 | −0.73 | −0.16 | ||
| Pre–Post | −0.09 ± 0.57 * | −0.46 ± 0.53 * | (0.000) | (0.003) | 0.82 | |||
| EC Velocity moment (mm2/s) | Pre | 5.02 ± 1.96 | 4.61 ± 1.79 | |||||
| Post | 3.69 ± 1.47 | 4.02 ± 1.68 | 64.438 | 9.766 | −1.22 | −0.27 | ||
| Pre–Post | −1.33 ± 0.94 * | −0.58 ± 0.88 * | (0.000) | (0.003) | 0.81 | |||
| BT-ESG (n = 29) | BTG (n = 30) | Time F(p) | Interaction F(p) | Effect Size (d) | CI for Differences | |||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| TUG (sec) | Pre | 36.05 ± 4.41 | 34.58 ± 4.58 | |||||
| Post | 30.99 ± 3.99 | 32.48 ± 5.11 | 0.552 | 12.014 | −4.67 | −1.25 | ||
| Pre–Post | −5.06 ± 2.74 * | −2.10 ± 3.72 * | (0.000) | (0.000) | 0.90 | |||
| BBS (point) | Pre | 28.69 ± 6.89 | 29.70 ± 7.37 | |||||
| Post | 34.86 ± 6.45 | 31.03 ± 6.75 | 56.721 | 23.577 | 2.84 | 6.83 | ||
| Pre–Post | 6.17 ± 4.71 * | 1.33 ± 2.71 * | (0.000) | (0.000) | 1.26 | |||
| FRT (cm) | Pre | 14.56 ± 3.73 | 12.89 ± 3.53 | |||||
| Post | 17.99 ± 3.82 | 13.32 ± 3.84 | 51.188 | 30.922 | 1.92 | 4.08 | ||
| Pre–Post | 3.43 ± 2.72 * | 0.43 ± 1.13 * | (0.000) | (0.022) | 1.45 | |||
| BT-ESG (n = 29) | BTG (n = 30) | Time F(p) | Interaction F(p) | Effect Size (d) | CI for Differences | |||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| FMA (point) | Pre | 15.10 ± 3.03 | 14.74 ± 3.22 | |||||
| Post | 19.84 ± 4.57 | 15.87 ± 2.64 | 74.366 | 28.130 | 2.25 | 4.97 | ||
| Pre–Post | 4.74 ± 3.39 * | 1.13 ± 1.53 * | (0.000) | (0.000) | 1.38 | |||
| MBI (score) | Pre | 52.99 ± 8.52 | 54.92 ± 8.96 | |||||
| Post | 60.79 ± 12.58 | 57.01 ± 8.10 | 71.552 | 23.817 | 2.04 | 9.37 | ||
| Pre–Post | 7.80 ± 5.72 * | 2.09 ± 8.10 * | (0.000) | (0.000) | 0.81 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K. Balance Training with Weight Shift-Triggered Electrical Stimulation for Stroke Patients: A Randomized Controlled Trial. Brain Sci. 2023, 13, 225. https://doi.org/10.3390/brainsci13020225
Lee K. Balance Training with Weight Shift-Triggered Electrical Stimulation for Stroke Patients: A Randomized Controlled Trial. Brain Sciences. 2023; 13(2):225. https://doi.org/10.3390/brainsci13020225
Chicago/Turabian StyleLee, Kyeongjin. 2023. "Balance Training with Weight Shift-Triggered Electrical Stimulation for Stroke Patients: A Randomized Controlled Trial" Brain Sciences 13, no. 2: 225. https://doi.org/10.3390/brainsci13020225