
The Associations between Results in Different Domains of Cognitive and Psychomotor Abilities Measured in Medical Students †
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Intelligence Testing
2.3. Cognitive and Psychomotor Performance Testing
2.4. Data Collection and Statistical Analysis
3. Results
3.1. Performance on the Raven’s APM and CRD-Series of Study Participants
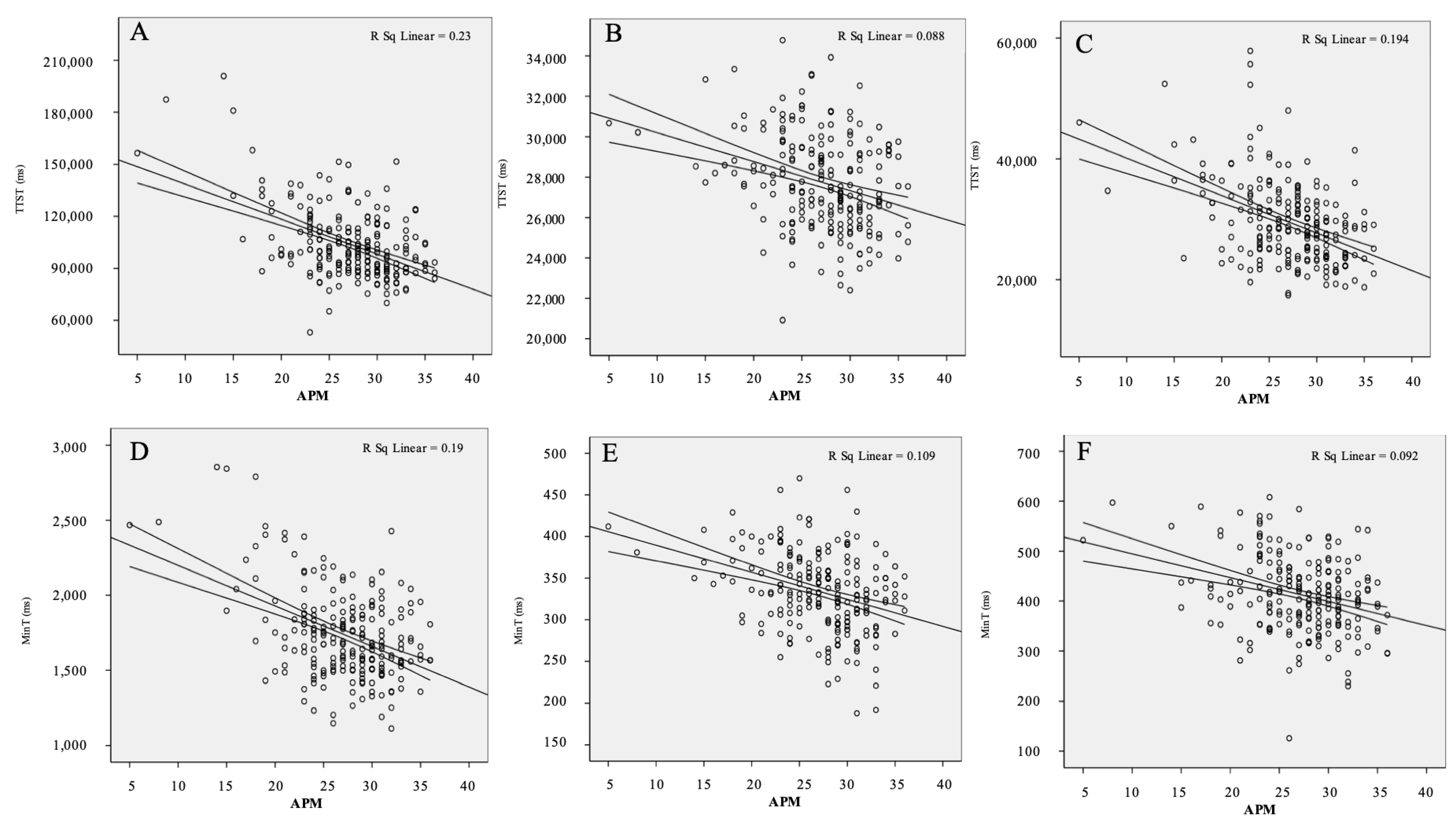
3.2. Association between Performance on Raven’s APM Intelligence Test and CRD-Series Tests
3.3. The Contribution of Age, Gender, and CRD-Series Test Results to APM Score
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kiesewetter, J.; Ebersbach, R.; Gorlitz, A.; Holzer, M.; Fischer, M.R.; Schmidmaier, R. Cognitive problem solving patterns of medical students correlate with success in diagnostic case solutions. PLoS ONE 2013, 8, e71486. [Google Scholar] [CrossRef] [Green Version]
- Ferrer, E.; Whitaker, K.J.; Steele, J.S.; Green, C.T.; Wendelken, C.; Bunge, S.A. White matter maturation supports the development of reasoning ability through its influence on processing speed. Dev. Sci. 2013, 16, 941–951. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, E.; O’Hare, E.D.; Bunge, S.A. Fluid reasoning and the developing brain. Front. Neurosci. 2009, 3, 46–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kail, R.; Salthouse, T.A. Processing speed as a mental capacity. Acta Psychol. 1994, 86, 199–225. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Park, E.H. Relationship of Working Memory, Processing Speed, and Fluid Reasoning in Psychiatric Patients. Psychiatry Investig. 2018, 15, 1154–1161. [Google Scholar] [CrossRef]
- Bates, T.; Stough, C. Processing speed, attention, and intelligence: Effects of spatial attention on decision time in high and low IQ subjects. Personal. Individ. Differ. 1997, 23, 861–868. [Google Scholar] [CrossRef]
- Jensen, A.R. Individual differences in the Hick paradigm. In Speed of Information Processing and Intelligence; Vernon, P.A., Ed.; Ablex: Norwood, NJ, USA, 1987. [Google Scholar]
- Colom, R.; Karama, S.; Jung, R.E.; Haier, R.J. Human intelligence and brain networks. Dialogues Clin Neurosci. 2010, 12, 489–501. [Google Scholar] [CrossRef]
- Gottfredson, L.S. Intelligence: Is it the epidemiologists’ elusive “fundamental cause” of social class inequalities in health? J. Pers. Soc. Psychol. 2004, 86, 174–199. [Google Scholar] [CrossRef] [Green Version]
- Gottfredson, L.S. g: Highly General and Highly Practical; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2002. [Google Scholar]
- Strenze, T. Intelligence and socioeconomic success: A meta-analytic review of longitudinal research. Intelligence 2007, 35, 401–426. [Google Scholar] [CrossRef]
- Hegelund, E.R.; Gronkjaer, M.; Osler, M.; Dammeyer, J.; Flensborg-Madsen, T.; Mortensen, E.L. The influence of educational attainment on intelligence. Intelligence 2020, 78, 101419. [Google Scholar] [CrossRef]
- Ritchie, S.J.; Bates, T.C.; Deary, I.J. Is education associated with improvements in general cognitive ability, or in specific skills? Dev. Psychol. 2015, 51, 573–582. [Google Scholar] [CrossRef]
- Ritchie, S.J.; Tucker-Drob, E.M. How Much Does Education Improve Intelligence? A Meta-Analysis. Psychol. Sci. 2018, 29, 1358–1369. [Google Scholar] [CrossRef] [Green Version]
- Sternberg, R.J.; Wong, C.H.; Sternberg, K. The Relation of Tests of Scientific Reasoning to Each Other and to Tests of General Intelligence. J. Intell. 2019, 7, 20. [Google Scholar] [CrossRef] [Green Version]
- Neubauer, A.C.; Riemann, R.; Mayer, R.; Angleitner, A. Intelligence and reaction times in the Hick, Sternberg and Posner paradigms. Personal. Individ. Differ. 1997, 22, 885–894. [Google Scholar] [CrossRef]
- Johnson, W.; Bouchard, T.J.; Krueger, R.F.; McGue, M.; Gottesman, I.I. Just one g: Consistent results from three test batteries. Intelligence 2004, 32, 319. [Google Scholar] [CrossRef]
- Burkart, J.M.; Schubiger, M.N.; van Schaik, C.P. The evolution of general intelligence. Behav. Brain. Sci. 2017, 40, e195. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, F.L.; Hunter, J. General mental ability in the world of work: Occupational attainment and job performance. J. Pers. Soc. Psychol. 2004, 86, 162–173. [Google Scholar] [CrossRef] [Green Version]
- Schubert, A.L.; Hagemann, D.; Frischkorn, G.T.; Herpertz, S.C. Faster, but not smarter: An experimental analysis of the relationship between mental speed and mental abilities. Intelligence 2018, 71, 66–75. [Google Scholar] [CrossRef]
- Mohn, C.; Sundet, K.; Rund, B.R. The relationship between IQ and performance on the MATRICS consensus cognitive battery. Schizophr. Res. Cogn. 2014, 1, 96–100. [Google Scholar] [CrossRef] [Green Version]
- Lusic Kalcina, L.; Pavlinac Dodig, I.; Pecotic, R.; Valic, M.; Dogas, Z. Psychomotor Performance in Patients with Obstructive Sleep Apnea Syndrome. Nat. Sci. Sleep 2020, 12, 183–195. [Google Scholar] [CrossRef] [Green Version]
- Pavlinac Dodig, I.; Kristo, D.; Lusic Kalcina, L.; Pecotic, R.; Valic, M.; Dogas, Z. The effect of age and gender on cognitive and psychomotor abilities measured by computerized series tests: A cross-sectional study. Croat. Med. J. 2020, 61, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Pecotic, R.; Dodig, I.P.; Valic, M.; Galic, T.; Kalcina, L.L.; Ivkovic, N.; Dogas, Z. Effects of CPAP therapy on cognitive and psychomotor performances in patients with severe obstructive sleep apnea: A prospective 1-year study. Sleep Breath. 2019, 23, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Jastrzębski, J.; Ociepka, M.; Chuderski, A. Fluid reasoning is equivalent to relation processing. Intelligence 2020, 82, 101489. [Google Scholar] [CrossRef]
- Drenovac, M. An analysis of some attributes of the dynamics of mental processing. Rev. Psychol. 2001, 8, 61–67. [Google Scholar]
- West, R.; Murphy, K.J.; Armilio, M.L.; Craik, F.I.; Stuss, D.T. Lapses of intention and performance variability reveal age-related increases in fluctuations of executive control. Brain Cogn. 2002, 49, 402–419. [Google Scholar] [CrossRef]
- Stuss, D.T.; Pogue, J.; Buckle, L.; Bondar, J. Characterization of stability of performance in patients with traumatic brain injury: Variability and consistency on reaction time tests. Neuropsychology 1994, 8, 316–324. [Google Scholar] [CrossRef]
- Guilford, J. The Nature of Human Intelligence; McGraw-Hill Book Company: New York, NY, USA, 1973. [Google Scholar]
- Brophy, D.R. Comparing the Attributes, Activities, and Performance of Divergent, Convergent, and Combination Thinkers. Creat. Res. J. 2001, 13, 439–455. [Google Scholar] [CrossRef]
- de Vink, I.C.; Willemsen, R.H.; Lazonder, A.W.; Kroesbergen, E.H. Creativity in mathematics performance: The role of divergent and convergent thinking. Br. J. Educ. Psychol. 2022, 92, 484–501. [Google Scholar] [CrossRef]
- Jain, A.; Bansal, R.; Kumar, A.; Singh, K.D. A comparative study of visual and auditory reaction times on the basis of gender and physical activity levels of medical first year students. Int. J. Appl. Basic Med. Res. 2015, 5, 124–127. [Google Scholar] [CrossRef] [Green Version]
- Vogel, S.; Schwabe, L. Learning and memory under stress: Implications for the classroom. NPJ Sci. Learn. 2016, 1, 16011. [Google Scholar] [CrossRef] [Green Version]
- Nechita, F.; Nechita, D.; Pîrlog, M.C.; Rogoveanu, I. Stress in medical students. Rom. J. Morphol. Embryol. 2014, 55, 1263–1266. [Google Scholar]
- Tyng, C.M.; Amin, H.U.; Saad, M.N.M.; Malik, A.S. The Influences of Emotion on Learning and Memory. Front. Psychol. 2017, 8, 1454. [Google Scholar] [CrossRef]
- Rahman, S.A.; Sullivan, J.P.; Barger, L.K.; St Hilaire, M.A.; O’Brien, C.S.; Stone, K.L.; Lockley, S.W.; ROSTERS STUDY GROUP. Extended Work Shifts and Neurobehavioral Performance in Resident-Physicians. Pediatrics 2021, 147, e2020009936. [Google Scholar] [CrossRef]
- Maltese, F.; Adda, M.; Bablon, A.; Hraeich, S.; Guervilly, C.; Lehingue, S.; Papazian, L. Night shift decreases cognitive performance of ICU physicians. Intensive Care Med. 2016, 42, 393–400. [Google Scholar] [CrossRef]
- Raven, J.; Raven, J. Raven Progressive Matrices. In Handbook of Nonverbal Assessment; McCallum, R.S., Ed.; Kluwer Academic/Plenum Publishers: New York, NY, USA, 2003. [Google Scholar] [CrossRef]
- Ceci, S.J. On the relation between microlevel processing efficiency and macrolevel measures of intelligence: Some arguments against current reductionism. Intelligence 1990, 14, 141–150. [Google Scholar] [CrossRef]
- Jogan, M.; Stocker, A.A. Signal Integration in Human Visual Speed Perception. J. Neurosci. 2015, 35, 9381–9390. [Google Scholar] [CrossRef] [Green Version]
- Zakharov, I.M.; Voronin, I.A.; Ismatullina, V.I.; Malykh, S.B. The relationship between visual recognition memory and intelligence. In Proceedings of the Fifth Annual International Conference—Early Childhood Care and Education, Moscow, Russia, 12–14 May; 2016; Volume 233, pp. 313–317. [Google Scholar] [CrossRef] [Green Version]
- Mous, S.E.; Schoemaker, N.K.; Blanken, L.M.; Thijssen, S.; van der Ende, J.; Polderman, T.J.; White, T. The association of gender, age, and intelligence with neuropsychological functioning in young typically developing children: The Generation R study. Appl. Neuropsychol. Child. 2017, 6, 22–40. [Google Scholar] [CrossRef]
- Galic, T.; Bozic, J.; Pecotic, R.; Ivkovic, N.; Valic, M.; Dogas, Z. Improvement of Cognitive and Psychomotor Performance in Patients with Mild to Moderate Obstructive Sleep Apnea Treated with Mandibular Advancement Device: A Prospective 1-Year Study. J. Clin. Sleep Med. 2016, 12, 177–186. [Google Scholar] [CrossRef] [Green Version]
- Arevalo-Rodriguez, I.; Smailagic, N.; Roque, I.F.M.; Ciapponi, A.; Sanchez-Perez, E.; Giannakou, A.; Cullum, S. Mini-Mental State Examination (MMSE) for the detection of Alzheimer’s disease and other dementias in people with mild cognitive impairment (MCI). Cochrane Database Syst. Rev. 2015, 3, CD010783. [Google Scholar] [CrossRef]
- Bieliauskas, L.A.; Depp, C.; Kauszler, M.L.; Steinberg, B.A.; Lacy, M. IQ and scores on the Mini-Mental State Examination (MMSE). Aging Neuropsychol. Cogn. 2000, 7, 227–229. [Google Scholar] [CrossRef]
- Domen, A.C.; van de Weijer, S.C.F.; Jaspers, M.W.; Denys, D.; Nieman, D.H. The validation of a new online cognitive assessment tool: The MyCognition Quotient. Int. J. Methods Psychiatr. Res. 2019, 28, e1775. [Google Scholar] [CrossRef]
- Warner, M.H.; Ernst, J.; Townes, B.D.; Peel, J.; Preston, M. Relationships between IQ and neuropsychological measures in neuropsychiatric populations: Within-laboratory and cross-cultural replications using WAIS and WAIS-R. J. Clin. Exp. Neuropsychol. 1987, 9, 545–562. [Google Scholar] [CrossRef] [PubMed]
- Raven, J.; Raven, J.C.; Court, J.H. Priručnik za Ravenove Progresivne Matrice i Ljestvice Rječnika; Naklada Slap: Jastrebarsko, Croatia, 1999. [Google Scholar]
- Steiner-Hofbauer, V.; Katz, H.W.; Grundnig, J.S.; Holzinger, A. Female participation or "feminization" of medicine. Wien. Med. Wochenschr. 2022, 2, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Buczyłowska, D.; Ronniger, P.; Melzer, J.; Petermann, F. Sex Similarities and Differences in Intelligence in Children Aged Two to Eight: Analysis of SON-R 2-8 Scores. J. Intell. 2019, 7, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ardila, A.; Rosselli, M.; Matute, E.; Inozemtseva, O. Gender differences in cognitive development. Dev. Psychol. 2011, 47, 984–990. [Google Scholar] [CrossRef] [Green Version]
- Jäncke, L. Sex/gender differences in cognition, neurophysiology, and neuroanatomy. F1000Research 2018, 7, F1000. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (N = 224) | |||
|---|---|---|---|
| Age (years) | 21 (19–31) | ||
| Croatian program, N (%) | 171 (76.3) | ||
| English program, N (%) | 53 (23.7) | ||
| Cognitive test results | |||
| Raven’s APM score | 27.12 ± 4.85 | ||
| CRD testing results | CRD11 | CRD311 | CRD411 |
| TTST (s) | 104.38 ± 20.54 | 27.81 ± 2.41 | 29.52 ± 6.87 |
| MinT (s) | 1.74 ± 0.30 | 0.34 ± 0.05 | 0.41 ± 0.08 |
| SB (s) | 19.93 ± 7.57 | 4.02 ± 1.01 | 4.94 ± 0.20 |
| EB (s) | 23.56 ± 9.28 | 3.71 ± 0.98 | 10.12 ± 4.02 |
| TB (s) | 43.49 ± 14.78 | 7.73 ± 1.84 | 15.06 ± 5.54 |
| NoErr | 2.92 ± 2.65 | 0 ± 0 | 8.38 ± 5.54 |
| CRD11 | CRD311 | CRD411 | ||||
|---|---|---|---|---|---|---|
| r | p 1 | r | p 1 | r | p 1 | |
| TTST | −0.48 | <0.001 | −0.30 | <0.001 | −0.44 | <0.001 |
| MinT | −0.44 | <0.001 | −0.33 | <0.001 | −0.30 | <0.001 |
| SB | −0.41 | <0.001 | 0.12 | 0.073 | −0.41 | <0.001 |
| EB | −0.24 | <0.001 | 0.13 | 0.052 | −0.34 | <0.001 |
| TB | −0.36 | <0.001 | 0.14 | 0.036 | −0.40 | <0.001 |
| NoErr | −0.08 | 0.233 | −0.15 | 0.025 | ||
| R2 | p * | β | t | p * | |
|---|---|---|---|---|---|
| Age | 0.279 | <0.001 | −0.132 | −1.901 | 0.059 |
| Gender | 0.089 | 1.278 | 0.203 | ||
| CRD11 | |||||
| TTST | −0.182 | −2.650 | 0.009 | ||
| MinT | −0.037 | −0.531 | 0.596 | ||
| CRD311 | |||||
| TTST | 0.052 | 0.746 | 0.457 | ||
| MinT | −0.158 | −2.297 | 0.023 | ||
| CRD411 | |||||
| TTST | −0.215 | −3.147 | 0.002 | ||
| MinT | <0.001 | 0.007 | 0.994 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pavlinac Dodig, I.; Qazzafi, A.; Lusic Kalcina, L.; Demirovic, S.; Pecotic, R.; Valic, M.; Dogas, Z. The Associations between Results in Different Domains of Cognitive and Psychomotor Abilities Measured in Medical Students. Brain Sci. 2023, 13, 185. https://doi.org/10.3390/brainsci13020185
Pavlinac Dodig I, Qazzafi A, Lusic Kalcina L, Demirovic S, Pecotic R, Valic M, Dogas Z. The Associations between Results in Different Domains of Cognitive and Psychomotor Abilities Measured in Medical Students. Brain Sciences. 2023; 13(2):185. https://doi.org/10.3390/brainsci13020185
Chicago/Turabian StylePavlinac Dodig, Ivana, Aisha Qazzafi, Linda Lusic Kalcina, Sijana Demirovic, Renata Pecotic, Maja Valic, and Zoran Dogas. 2023. "The Associations between Results in Different Domains of Cognitive and Psychomotor Abilities Measured in Medical Students" Brain Sciences 13, no. 2: 185. https://doi.org/10.3390/brainsci13020185