
Combined Depth and Subdural Electrodes for Lateralization of the Ictal Onset Zone in Mesial Temporal Lobe Epilepsy with Hippocampal Sclerosis

Abstract
:1. Introduction
2. Material and Methods
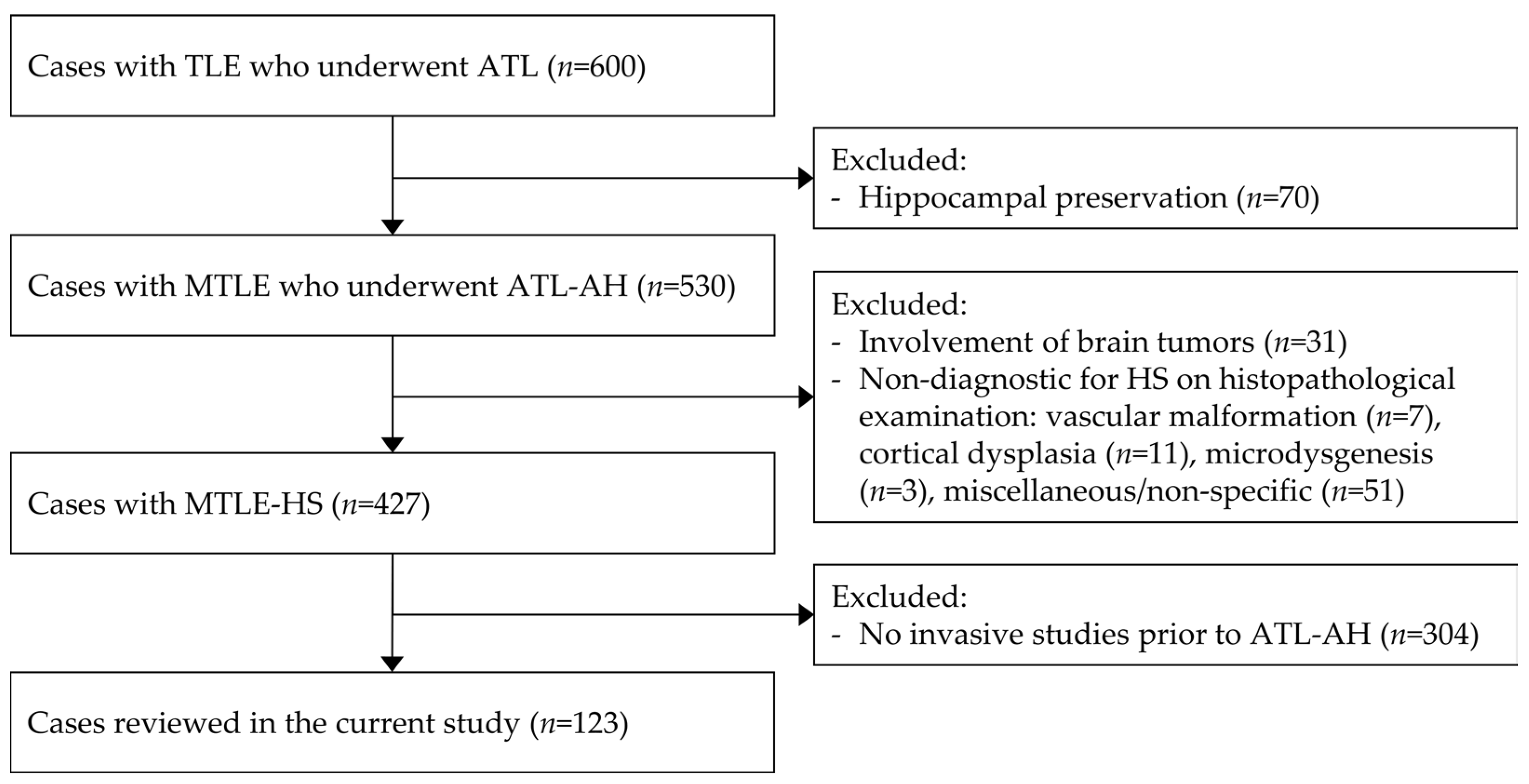
2.1. Study Population
2.2. Clinical Assessment and Surgical Interventions
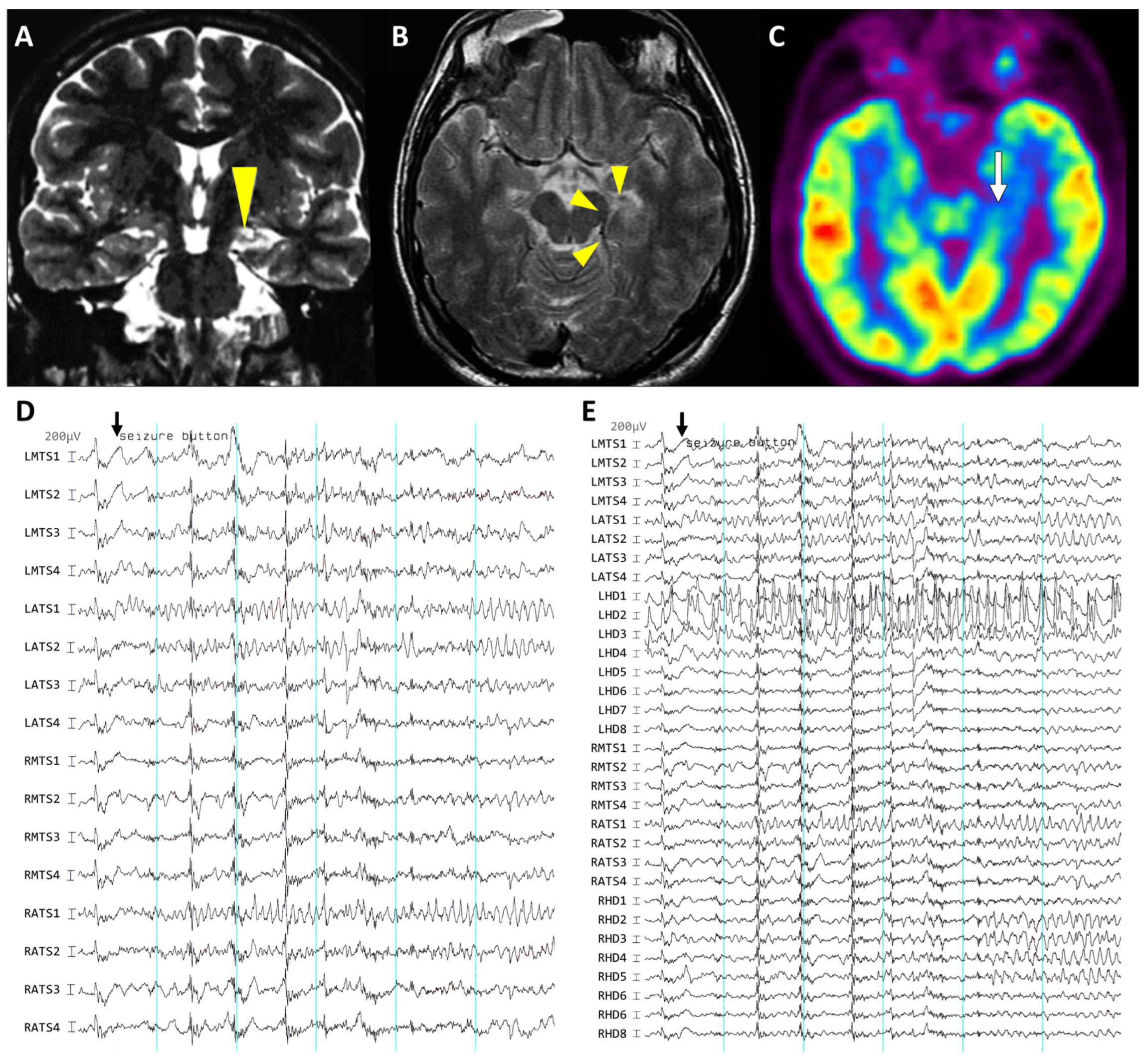
2.2.1. Presurgical Evaluations
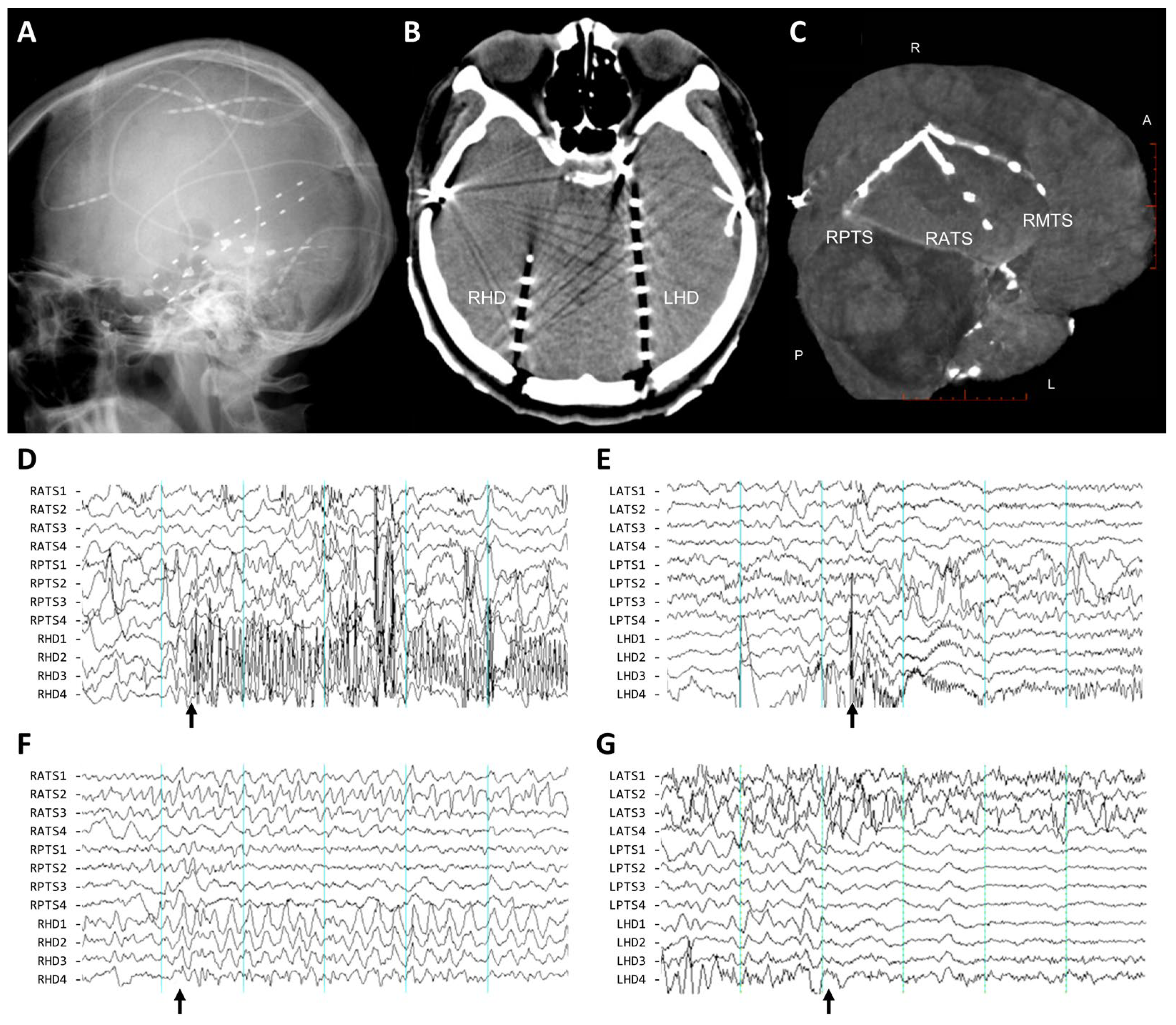
2.2.2. Surgical Procedures for Invasive Studies
2.2.3. Clinical Assessment of Intracranial EEG Recording
2.2.4. Surgical Treatment and Outcome Evaluation
2.3. Characterization of the Ictal Onset Patterns of Depth and Subdural Electrodes
2.4. Statistical Consideration
3. Results
3.1. Clinical Characteristics of MTLE-HS
3.2. Electrographic Patterns at Ictal Onset
3.3. Distribution of Involved Electrodes and False Lateralization
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Riney, K.; Bogacz, A.; Somerville, E.; Hirsch, E.; Nabbout, R.; Scheffer, I.E.; Zuberi, S.M.; Alsaadi, T.; Jain, S.; French, J.; et al. International League Against Epilepsy classification and definition of epilepsy syndromes with onset at a variable age: Position statement by the ILAE Task Force on Nosology and Definitions. Epilepsia 2022, 63, 1443–1474. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, S.R.; Nair, D.; Gross, R.E.; Gonzalez-Martinez, J. Tracking a changing paradigm and the modern face of epilepsy surgery: A comprehensive and critical review on the hunt for the optimal extent of resection in mesial temporal lobe epilepsy. Epilepsia 2019, 60, 1768–1793. [Google Scholar] [CrossRef] [PubMed]
- Salanova, V.; Markand, O.; Worth, R. Temporal lobe epilepsy: Analysis of failures and the role of reoperation. Acta Neurol. Scand. 2005, 111, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Ryvlin, P.; Kahane, P. The hidden causes of surgery-resistant temporal lobe epilepsy: Extratemporal or temporal plus. Curr. Opin. Neurol. 2005, 18, 125–127. [Google Scholar] [CrossRef]
- Barba, C.; Rheims, S.; Minotti, L.; Guénot, M.; Hoffmann, D.; Chabardès, S.; Isnard, J.; Kahane, P.; Ryvlin, P. Temporal plus epilepsy is a major determinant of temporal lobe surgery failures. Brain 2016, 139, 444–451. [Google Scholar] [CrossRef]
- Lopez-Gonzalez, M.; Gonzalez-Martinez, J.; Jehi, L.; Kotagal, P.; Warbel, A.; Bingaman, W. Epilepsy surgery of the temporal lobe in pediatric population: A retrospective analysis. Neurosurgery 2012, 70, 684–692. [Google Scholar] [CrossRef]
- Thadani, V.; Williamson, P.; Berger, R.; Spencer, S.; Spencer, D.; Novelly, R.; Sass, K.; Kim, J.; Mattson, R. Successful epilepsy surgery without intracranial EEG recording: Criteria for patient selection. Epilepsia 1995, 36, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Wieser, H.; ILAE Commission on Neurosurgery of Epilepsy. ILAE Commission Report. Mesial temporal lobe epilepsy with hippocampal sclerosis. Epilepsia 2004, 45, 695–714. [Google Scholar] [CrossRef] [PubMed]
- Ravat, S.; Rao, P.; Iyer, V.; Muzumdar, D.; Shah, U.; Shah, S.; Jain, N.; Godge, Y. Surgical outcomes with non-invasive presurgical evaluation in MRI determined bilateral mesial temporal sclerosis: A retrospective cohort study. Int. J. Surg. 2016, 36, 429–435. [Google Scholar] [CrossRef]
- Kovac, S.; Vakharia, V.; Scott, C.; Diehl, B. Invasive epilepsy surgery evaluation. Seizure 2017, 44, 125–136. [Google Scholar] [CrossRef] [PubMed]
- Spencer, S.S.; Spencer, D.D.; Williamson, P.D.; Mattson, R. Combined depth and subdural electrode investigation in uncontrolled epilepsy. Neurology 1990, 40, 74–79. [Google Scholar] [CrossRef]
- Behrens, E.; Zentner, J.; van Roost, D.; Hufnagel, A.; Elger, C.; Schramm, J. Subdural and depth electrodes in the presurgical evaluation of epilepsy. Acta Neurochir. 1994, 128, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Takayama, Y.; Ikegaya, N.; Iijima, K.; Kimura, Y.; Yokosako, S.; Muraoka, N.; Kosugi, K.; Kaneko, Y.; Yamamoto, T.; Iwasaki, M. Single-Institutional Experience of Chronic Intracranial Electroencephalography Based on the Combined Usage of Subdural and Depth Electrodes. Brain Sci. 2021, 11, 307. [Google Scholar] [CrossRef] [PubMed]
- Joswig, H.; Lau, J.; Abdallat, M.; Parrent, A.; MacDougall, K.; McLachlan, R.; Burneo, J.; Steven, D. Stereoelectroencephalography Versus Subdural Strip Electrode Implantations: Feasibility, Complications, and Outcomes in 500 Intracranial Monitoring Cases for Drug-Resistant Epilepsy. Neurosurgery 2020, 87, E23–E30. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Katz, J.; Anderson, M.; Mansouri, A.; Remick, M.; Ibrahim, G.; Abel, T. Method of invasive monitoring in epilepsy surgery and seizure freedom and morbidity: A systematic review. Epilepsia 2019, 60, 1960–1972. [Google Scholar] [CrossRef]
- Spencer, S.S.; Guimaraes, P.; Katz, A.; Kim, J.; Spencer, D. Morphological patterns of seizures recorded intracranially. Epilepsia 1992, 33, 537–545. [Google Scholar] [CrossRef]
- Fisher, R.S.; Cross, J.H.; French, J.A.; Higurashi, N.; Hirsch, E.; Jansen, F.E.; Lagae, L.; Moshe, S.L.; Peltola, J.; Roulet Perez, E.; et al. Operational classification of seizure types by the International League Against Epilepsy: Position Paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017, 58, 522–530. [Google Scholar] [CrossRef]
- Schmeiser, B.; Hammen, T.; Steinhoff, B.J.; Zentner, J.; Schulze-Bonhage, A. Long-term outcome characteristics in mesial temporal lobe epilepsy with and without associated cortical dysplasia. Epilepsy Res. 2016, 126, 147–156. [Google Scholar] [CrossRef]
- Alsaadi, T.M.; Laxer, K.D.; Barbaro, N.M.; Marks, W.J., Jr.; Garcia, P.A. False lateralization by subdural electrodes in two patients with temporal lobe epilepsy. Neurology 2001, 57, 532–534. [Google Scholar] [CrossRef]
- Mintzer, S.; Cendes, F.; Soss, J.; Andermann, F.; Engel, J., Jr.; Dubeau, F.; Olivier, A.; Fried, I. Unilateral hippocampal sclerosis with contralateral temporal scalp ictal onset. Epilepsia 2004, 45, 792–802. [Google Scholar] [CrossRef]
- Fujimoto, A.; Masuda, H.; Homma, J.; Sasagawa, M.; Kameyama, S. False lateralization of mesial temporal lobe epilepsy by noninvasive neurophysiological examinations. Neurol. Med. Chir. 2006, 46, 518–521. [Google Scholar] [CrossRef]
- Adamolekun, B.; Afra, P.; Boop, F.A. False lateralization of seizure onset by scalp EEG in neocortical temporal lobe epilepsy. Seizure 2011, 20, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Tezer, F.I.; Dericioglu, N.; Bozkurt, G.; Bilginer, B.; Akalan, N.; Saygi, S. Epilepsy surgery in patients with unilateral mesial temporal sclerosis and contralateral scalp ictal onset. Turk. Neurosurg. 2011, 21, 549–554. [Google Scholar] [CrossRef]
- Park, Y.D.; Murro, A.M.; King, D.W.; Gallagher, B.B.; Smith, J.R.; Yaghmai, F. The significance of ictal depth EEG patterns in patients with temporal lobe epilepsy. Electroencephalogr. Clin. Neurophysiol. 1996, 99, 412–415. [Google Scholar] [CrossRef]
- Eisenschenk, S.; Gilmore, R.L.; Cibula, J.E.; Roper, S.N. Lateralization of temporal lobe foci: Depth versus subdural electrodes. Clin. Neurophysiol. 2001, 112, 836–844. [Google Scholar] [CrossRef] [PubMed]
- Schuh, L.A.; Henry, T.R.; Ross, D.A.; Smith, B.J.; Elisevich, K.; Drury, I. Ictal spiking patterns recorded from temporal depth electrodes predict good outcome after anterior temporal lobectomy. Epilepsia 2000, 41, 316–319. [Google Scholar] [CrossRef] [PubMed]
- Dolezalova, I.; Brazdil, M.; Hermanova, M.; Horakova, I.; Rektor, I.; Kuba, R. Intracranial EEG seizure onset patterns in unilateral temporal lobe epilepsy and their relationship to other variables. Clin. Neurophysiol. 2013, 124, 1079–1088. [Google Scholar] [CrossRef]
- Jimenez-Jimenez, D.; Nekkare, R.; Flores, L.; Chatzidimou, K.; Bodi, I.; Honavar, M.; Mullatti, N.; Elwes, R.D.; Selway, R.P.; Valentin, A.; et al. Prognostic value of intracranial seizure onset patterns for surgical outcome of the treatment of epilepsy. Clin. Neurophysiol. 2015, 126, 257–267. [Google Scholar] [CrossRef]
- Cui, D.; Gao, R.; Xu, C.; Yan, H.; Zhang, X.; Yu, T.; Zhang, G. Ictal onset stereoelectroencephalography patterns in temporal lobe epilepsy: Type, distribution, and prognostic value. Acta Neurochir. 2022, 164, 555–563. [Google Scholar] [CrossRef]
- Lee, A.T.; Nichols, N.M.; Speidel, B.A.; Fan, J.M.; Cajigas, I.; Knowlton, R.C.; Chang, E.F. Modern intracranial electroencephalography for epilepsy localization with combined subdural grid and depth electrodes with low and improved hemorrhagic complication rates. J. Neurosurg. 2023, 138, 821–827. [Google Scholar] [CrossRef]
- Park, S.H.; Jung, I.H.; Chang, K.W.; Oh, M.K.; Chang, J.W.; Kim, S.H.; Kang, H.C.; Kim, H.D.; Chang, W.S. Epidural grid, a new methodology of invasive intracranial EEG monitoring: A technical note and experience of a single center. Epilepsy Res. 2022, 182, 106912. [Google Scholar] [CrossRef] [PubMed]
- Enatsu, R.; Bulacio, J.; Najm, I.; Wyllie, E.; So, N.K.; Nair, D.R.; Foldvary-Schaefer, N.; Bingaman, W.; Gonzalez-Martinez, J. Combining stereo-electroencephalography and subdural electrodes in the diagnosis and treatment of medically intractable epilepsy. J. Clin. Neurosci. 2014, 21, 1441–1445. [Google Scholar] [CrossRef] [PubMed]
- McGovern, R.A.; Ruggieri, P.; Bulacio, J.; Najm, I.; Bingaman, W.E.; Gonzalez-Martinez, J.A. Risk analysis of hemorrhage in stereo-electroencephalography procedures. Epilepsia 2019, 60, 571–580. [Google Scholar] [CrossRef]
- Mathon, B.; Bielle, F.; Samson, S.; Plaisant, O.; Dupont, S.; Bertrand, A.; Miles, R.; Nguyen-Michel, V.H.; Lambrecq, V.; Calderon-Garciduenas, A.L.; et al. Predictive factors of long-term outcomes of surgery for mesial temporal lobe epilepsy associated with hippocampal sclerosis. Epilepsia 2017, 58, 1473–1485. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Case | Sex/Age, year | Onset Age (Duration), year | Handedness | Risk Factors | Seizure Frequency, /mo | Seizure Type † | Preoperative Imaging Studies | Invasive Study | Surgical Intervention | Dual Pathology | |||
| Structural Abnormality | Perfusion (Ictal SPECT) | Metabolism (FDG-PET) | Duration, day | Number of Events ‡ | |||||||||
| 1 | F/42 | 6 (36) | Lt. | Enceph. | 1–2 | FBTCS | Lt. HA | . | . | 12 | 3 (3) | Lt. ATL | . |
| 2 | M/34 | 17 (15) | Rt. | FC | 1–2 | FBTCS | Rt. HS | . | . | 5 | 3 (1) | Rt. ATL | . |
| 3 | F/38 | 29 (9) | Lt. | . | 1–2 | FBTCS | Lt. HS | . | . | 7 | 5 (2) | Lt. ATL | . |
| 4 | M/17 | 5 (12) | Rt. | FC | 1–2 | FIAS | Rt. HA | ↑Rt. T | . | 3 | 4 (0) | Rt. ATL | CD |
| 5 | M/31 | 11 (20) | Rt. | . | >4 | FBTCS | Rt. HS | ↑Lt. T | . | 5 | 6 (4) | Rt. ATL | . |
| 6 | M/29 | 14 (15) | Rt. | FC | 1–2 | FBTCS | Lt. HS | . | . | 7 | 2 (2) | Lt. ATL | . |
| 7 | M/44 | 31 (13) | Lt. | FC | 3–4 | FBTCS | Lt. HS | ↑Lt. T | . | 6 | 5 (4) | Lt. ATL | . |
| 8 | F/28 | 13 (15) | Rt. | Enceph. | 3–4 | FIAS | Lt. HS | ↑Lt. T | ↓Lt. T | 6 | 5 (0) | Lt. ATL | . |
| 9 | M/21 | 2 (16) | Ambidex. | FC | <1 | FBTCS | Rt. HS | . | ↓Lt. T | 7 | 2 (1) | Lt. ATL | . |
| 10 | M/28 | 18 (10) | Rt. | . | 2–3 | FBTCS | Lt. HS | ↑Lt. T | ↓Lt. T | 4 | 5 (5) | Lt. ATL | . |
| 11 | F/35 | 34 (1) | Rt. | . | 3–4 | FBTCS | Lt. HS | ↑Rt. T | ↓Rt. T | 5 | 6 (4) | Lt. ATL | CD |
| 12 | M/21 | 9 (12) | Lt. | FC | 2–3 | FBTCS | Lt. HS | . | . | 6 | 3 (2) | Lt. ATL | CD |
| 13 | F/30 | 3 (27) | Rt. | Trauma | 1–2 | FBTCS | Rt. HS | ↑Lt. T | . | 5 | 5 (5) | Rt. ATL | . |
| 14 | F/54 | 35 (19) | Rt. | Enceph. | 1–2 | FBTCS | Lt. HS | . | . | 4 | 3 (1) | Lt. ATL | . |
| 15 | F/22 | 5 (25) | Rt. | . | 1–2 | FBTCS | Rt. HS | . | ↓Rt. T | 6 | 3 (3) | Rt. ATL | CD |
| 16 | M/39 | 16 (24) | Rt. | Enceph. | 1–2 | FIAS | . | . | . | 6 | 5 (0) | Rt. ATL | . |
| 17 | F/18 | 6 (12) | Rt. | FC | >4 | FBTCS | Lt. HS | ↑Rt. T | . | 7 | 3 (3) | Lt. ATL | . |
| 18 | M/28 | 25 (3) | Rt. | FC | >4 | FBTCS | Rt. HS | ↑Rt. T | ↓Rt. T | 3 | 5 (5) | Rt. ATL | . |
| 19 | M/34 | 24 (11) | Rt. | FC | >4 | FBTCS | Rt. HS | ↑Rt. T | ↓Rt. T | 6 | 3 (2) | Rt. ATL | . |
| 20 | M/29 | 14 (15) | Rt. | . | 1–2 | FBTCS | . | ↑Rt. T | ↓Rt. T | 7 | 3 (3) | Rt. ATL | . |
| 21 | F/36 | 26 (10) | Ambidex. | . | >4 | FBTCS | . | ↑Rt. T | ↓Rt. T | 3 | 5 (5) | Rt. ATL | MD |
| 22 | F/53 | 39 (14) | Rt. | FC | 2–3 | FBTCS | . | . | ↓Rt. T | 6 | 5 (5) | Rt. ATL | . |
| 23 | F/37 | 5 (32) | Rt. | FC | 1–2 | FBTCS | Rt. HS | ↑Rt. T | ↓Rt. T | 6 | 3 (3) | Rt. ATL | . |
| 24 | F/27 | 1 (19) | Lt. | FC | 2–3 | FBTCS | Rt. HA | . | . | 6 | 4 (4) | Rt. ATL | . |
| 25 | F/31 | 26 (4) | Ambidex. | . | 3–4 | FBTCS | Lt. HS | . | . | 7 | 3 (3) | Lt. ATL | . |
| Seizure Events | Cases † | |||
|---|---|---|---|---|
| Seizure Remission | Refractory | Seizure Remission | Refractory | |
| N | 99 | 21 | 25 | 8 |
| Preceding epileptiform discharges | ||||
| Present | 49 (49) | 5 (24) | 17 (68) | 3 (38) |
| Ictal onset frequency | ||||
| 8 Hz or higher | 88 (89) | 14 (67) | 24 (96) | 6 (75) |
| Ictal onset pattern | ||||
| Fast spike trains | 38 (38) | 4 (19) | 13 (52) | 1 (13) |
| Low-voltage fast activity | 33 (33) | 10 (48) | 7 (28) | 5 (63) |
| Rhythmic slow activity | 12 (12) | 7 (33) | 5 (20) | 4 (50) |
| Electrodecremental activity | 16 (16) | . | 22 (88) | . |
| Distribution of electrodes | ||||
| Depth electrode only | 47 (47) | 2 (10) | 15 (60) | 2 (25) |
| Depth and medial strip electrodes | 44 (44) | 9 (43) | 14 (56) | 4 (50) |
| Lateral strip electrodes | 3 (3) | 8 (38) | 3 (12) | 3 (38) |
| Diffuse widespread | 5 (5) | 2 (10) | 2 (8) | 1 (13) |
| Interhemispheric propagation | ||||
| Early (within five seconds) | 9 (9) | 1 (5) | 4 (16) | 1 (13) |
| Late (above five seconds) | 61 (62) | 13 (62) | 21 (84) | 6 (75) |
| None | 29 (29) | 7 (33) | 12 (48) | 2 (25) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Kang, J.K.; Lee, S.A.; Hong, S.H. Combined Depth and Subdural Electrodes for Lateralization of the Ictal Onset Zone in Mesial Temporal Lobe Epilepsy with Hippocampal Sclerosis. Brain Sci. 2023, 13, 1547. https://doi.org/10.3390/brainsci13111547
Kim J, Kang JK, Lee SA, Hong SH. Combined Depth and Subdural Electrodes for Lateralization of the Ictal Onset Zone in Mesial Temporal Lobe Epilepsy with Hippocampal Sclerosis. Brain Sciences. 2023; 13(11):1547. https://doi.org/10.3390/brainsci13111547
Chicago/Turabian StyleKim, Junhyung, Joong Koo Kang, Sang Ahm Lee, and Seok Ho Hong. 2023. "Combined Depth and Subdural Electrodes for Lateralization of the Ictal Onset Zone in Mesial Temporal Lobe Epilepsy with Hippocampal Sclerosis" Brain Sciences 13, no. 11: 1547. https://doi.org/10.3390/brainsci13111547