
Working Memory-Related Neurofunctional Correlates Associated with the Frontal Lobe in Children with Familial vs. Non-Familial Attention Deficit/Hyperactivity Disorder

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. The n-Back Task
2.3. Image Acquisition
2.4. Individual-Level fMRI Data Preprocessing
2.5. Region of Interest (ROI) Selection and Definition
2.6. Laterality Analyses
2.7. Statistical Analyses
3. Results
3.1. Demographic and Task Performance Measures
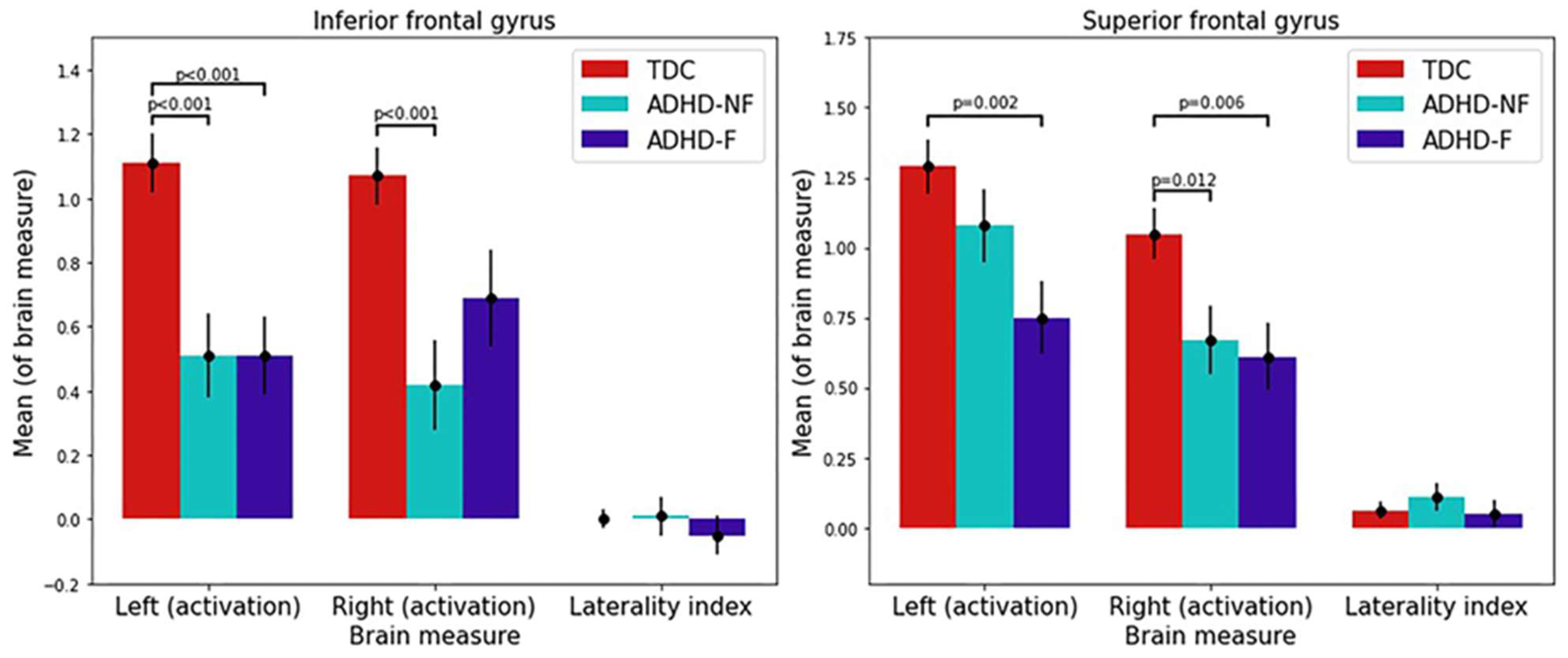
3.2. ROI-Based Activation and LI Analyses
3.3. Brain–Behavior Correlation Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barkley, R.A. Major life activity and health outcomes associated with attention-deficit/hyperactivity disorder. J. Clin. Psychiatry 2002, 63 (Suppl. 12), 10–15. [Google Scholar] [PubMed]
- Wong, A.; Landes, S.D. Expanding Understanding of Racial-Ethnic Differences in ADHD Prevalence Rates among Children to Include Asians and Alaskan Natives/American Indians. J. Atten. Disord. 2022, 26, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Polanczyk, G.; de Lima, M.S.; Horta, B.L.; Biederman, J.; Rohde, L.A. The worldwide prevalence of ADHD: A systematic review and metaregression analysis. Am. J. Psychiatry 2007, 164, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Baeyens, D.; Roeyers, H.; Walle, J.V. Subtypes of attention-deficit/hyperactivity disorder (ADHD): Distinct or related disorders across measurement levels? Child. Psychiatry Hum. Dev. 2006, 36, 403–417. [Google Scholar] [CrossRef]
- Chhabildas, N.; Pennington, B.F.; Willcutt, E.G. A comparison of the neuropsychological profiles of the DSM-IV subtypes of ADHD. J. Abnorm. Child. Psychol. 2001, 29, 529–540. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Weibman, D.; Halperin, J.M.; Li, X. A Review of Heterogeneity in Attention Deficit/Hyperactivity Disorder (ADHD). Front. Hum. Neurosci. 2019, 13, 42. [Google Scholar] [CrossRef] [PubMed]
- Mackie, S.; Shaw, P.; Lenroot, R.; Pierson, R.; Greenstein, D.K.; Nugent, T.F., 3rd; Sharp, W.S.; Giedd, J.N.; Rapoport, J.L. Cerebellar development and clinical outcome in attention deficit hyperactivity disorder. Am. J. Psychiatry 2007, 164, 647–655. [Google Scholar] [CrossRef]
- Halperin, J.M.; Schulz, K.P. Revisiting the role of the prefrontal cortex in the pathophysiology of attention-deficit/hyperactivity disorder. Psychol. Bull. 2006, 132, 560–581. [Google Scholar] [CrossRef]
- Willcutt, E.G.; Doyle, A.E.; Nigg, J.T.; Faraone, S.V.; Pennington, B.F. Validity of the executive function theory of attention-deficit/hyperactivity disorder: A meta-analytic review. Biol. Psychiatry 2005, 57, 1336–1346. [Google Scholar] [CrossRef]
- Nigg, J.T.; Willcutt, E.G.; Doyle, A.E.; Sonuga-Barke, E.J. Causal heterogeneity in attention-deficit/hyperactivity disorder: Do we need neuropsychologically impaired subtypes? Biol. Psychiatry 2005, 57, 1224–1230. [Google Scholar] [CrossRef]
- Yap, K.H.; Abdul Manan, H.; Sharip, S. Heterogeneity in brain functional changes of cognitive processing in ADHD across age: A systematic review of task-based fMRI studies. Behav. Brain Res. 2021, 397, 112888. [Google Scholar] [CrossRef]
- Faraone, S.V.; Perlis, R.H.; Doyle, A.E.; Smoller, J.W.; Goralnick, J.J.; Holmgren, M.A.; Sklar, P. Molecular genetics of attention-deficit/hyperactivity disorder. Biol. Psychiatry 2005, 57, 1313–1323. [Google Scholar] [CrossRef]
- Riglin, L.; Collishaw, S.; Thapar, A.K.; Dalsgaard, S.; Langley, K.; Smith, G.D.; Stergiakouli, E.; Maughan, B.; O’Donovan, M.C.; Thapar, A. Association of Genetic Risk Variants with Attention-Deficit/Hyperactivity Disorder Trajectories in the General Population. JAMA Psychiatry 2016, 73, 1285–1292. [Google Scholar] [CrossRef]
- Larsson, H.; Asherson, P.; Chang, Z.; Ljung, T.; Friedrichs, B.; Larsson, J.O.; Lichtenstein, P. Genetic and environmental influences on adult attention deficit hyperactivity disorder symptoms: A large Swedish population-based study of twins. Psychol. Med. 2013, 43, 197–207. [Google Scholar] [CrossRef]
- Pingault, J.B.; Viding, E.; Galera, C.; Greven, C.U.; Zheng, Y.; Plomin, R.; Rijsdijk, F. Genetic and Environmental Influences on the Developmental Course of Attention-Deficit/Hyperactivity Disorder Symptoms From Childhood to Adolescence. JAMA Psychiatry 2015, 72, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Sprich, S.; Biederman, J.; Crawford, M.H.; Mundy, E.; Faraone, S.V. Adoptive and biological families of children and adolescents with ADHD. J. Am. Acad. Child. Adolesc. Psychiatry 2000, 39, 1432–1437. [Google Scholar] [CrossRef] [PubMed]
- Coghill, D.R.; Seth, S.; Matthews, K. A comprehensive assessment of memory, delay aversion, timing, inhibition, decision making and variability in attention deficit hyperactivity disorder: Advancing beyond the three-pathway models. Psychol. Med. 2014, 44, 1989–2001. [Google Scholar] [CrossRef] [PubMed]
- Adamo, N.; Di Martino, A.; Esu, L.; Petkova, E.; Johnson, K.; Kelly, S.; Castellanos, F.X.; Zuddas, A. Increased response-time variability across different cognitive tasks in children with ADHD. J. Atten. Disord. 2014, 18, 434–446. [Google Scholar] [CrossRef] [PubMed]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef]
- Baddeley, A. Working memory. Science 1992, 255, 556–559. [Google Scholar] [CrossRef]
- Owens, M.M.; Allgaier, N.; Hahn, S.; Yuan, D.; Albaugh, M.; Adise, S.; Chaarani, B.; Ortigara, J.; Juliano, A.; Potter, A.; et al. Multimethod investigation of the neurobiological basis of ADHD symptomatology in children aged 9–10: Baseline data from the ABCD study. Transl. Psychiatry 2021, 11, 64. [Google Scholar] [CrossRef] [PubMed]
- Castellanos, F.X.; Tannock, R. Neuroscience of attention-deficit/hyperactivity disorder: The search for endophenotypes. Nat. Rev. Neurosci. 2002, 3, 617–628. [Google Scholar] [CrossRef] [PubMed]
- Diamond, A. Attention-deficit disorder (attention-deficit/ hyperactivity disorder without hyperactivity): A neurobiologically and behaviorally distinct disorder from attention-deficit/hyperactivity disorder (with hyperactivity). Dev. Psychopathol. 2005, 17, 807–825. [Google Scholar] [CrossRef] [PubMed]
- Kasper, L.J.; Alderson, R.M.; Hudec, K.L. Moderators of working memory deficits in children with attention-deficit/hyperactivity disorder (ADHD): A meta-analytic review. Clin. Psychol. Rev. 2012, 32, 605–617. [Google Scholar] [CrossRef] [PubMed]
- Mattfeld, A.T.; Whitfield-Gabrieli, S.; Biederman, J.; Spencer, T.; Brown, A.; Fried, R.; Gabrieli, J.D. Dissociation of working memory impairments and attention-deficit/hyperactivity disorder in the brain. Neuroimage Clin. 2016, 10, 274–282. [Google Scholar] [CrossRef]
- Zdorovtsova, N.; Jones, J.; Akarca, D.; Benhamou, E.; The Calm, T.; Astle, D.E. Exploring neural heterogeneity in inattention and hyperactivity. Cortex 2023, 164, 90–111. [Google Scholar] [CrossRef]
- Brocki, K.C.; Randall, K.D.; Bohlin, G.; Kerns, K.A. Working memory in school-aged children with attention-deficit/hyperactivity disorder combined type: Are deficits modality specific and are they independent of impaired inhibitory control? J. Clin. Exp. Neuropsychol. 2008, 30, 749–759. [Google Scholar] [CrossRef]
- Rapport, M.D.; Alderson, R.M.; Kofler, M.J.; Sarver, D.E.; Bolden, J.; Sims, V. Working memory deficits in boys with attention-deficit/hyperactivity disorder (ADHD): The contribution of central executive and subsystem processes. J. Abnorm. Child. Psychol. 2008, 36, 825–837. [Google Scholar] [CrossRef]
- Alderson, R.M.; Kasper, L.J.; Hudec, K.L.; Patros, C.H. Attention-deficit/hyperactivity disorder (ADHD) and working memory in adults: A meta-analytic review. Neuropsychology 2013, 27, 287–302. [Google Scholar] [CrossRef]
- Kobel, M.; Bechtel, N.; Weber, P.; Specht, K.; Klarhofer, M.; Scheffler, K.; Opwis, K.; Penner, I.K. Effects of methylphenidate on working memory functioning in children with attention deficit/hyperactivity disorder. Eur. J. Paediatr. Neurol. 2009, 13, 516–523. [Google Scholar] [CrossRef]
- Kobel, M.; Bechtel, N.; Specht, K.; Klarhofer, M.; Weber, P.; Scheffler, K.; Opwis, K.; Penner, I.K. Structural and functional imaging approaches in attention deficit/hyperactivity disorder: Does the temporal lobe play a key role? Psychiatry Res. 2010, 183, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Massat, I.; Slama, H.; Kavec, M.; Linotte, S.; Mary, A.; Baleriaux, D.; Metens, T.; Mendlewicz, J.; Peigneux, P. Working memory-related functional brain patterns in never medicated children with ADHD. PLoS ONE 2012, 7, e49392. [Google Scholar] [CrossRef] [PubMed]
- Friedman, N.P.; Miyake, A.; Young, S.E.; DeFries, J.C.; Corley, R.P.; Hewitt, J.K. Individual differences in executive functions are almost entirely genetic in origin. J. Exp. Psychol. Gen. 2008, 137, 201–225. [Google Scholar] [CrossRef]
- Bidwell, L.C.; Willcutt, E.G.; Defries, J.C.; Pennington, B.F. Testing for neuropsychological endophenotypes in siblings discordant for attention-deficit/hyperactivity disorder. Biol. Psychiatry 2007, 62, 991–998. [Google Scholar] [CrossRef] [PubMed]
- Coolidge, F.L.; Thede, L.L.; Young, S.E. Heritability and the comorbidity of attention deficit hyperactivity disorder with behavioral disorders and executive function deficits: A preliminary investigation. Dev. Neuropsychol. 2000, 17, 273–287. [Google Scholar] [CrossRef]
- van Ewijk, H.; Heslenfeld, D.J.; Luman, M.; Rommelse, N.N.; Hartman, C.A.; Hoekstra, P.; Franke, B.; Buitelaar, J.K.; Oosterlaan, J. Visuospatial working memory in ADHD patients, unaffected siblings, and healthy controls. J. Atten. Disord. 2014, 18, 369–378. [Google Scholar] [CrossRef]
- van Lieshout, M.; Luman, M.; Schweren, L.J.S.; Twisk, J.W.R.; Faraone, S.V.; Heslenfeld, D.J.; Hartman, C.A.; Hoekstra, P.J.; Franke, B.; Buitelaar, J.K.; et al. The Course of Neurocognitive Functioning and Prediction of Behavioral Outcome of ADHD Affected and Unaffected Siblings. J. Abnorm. Child. Psychol. 2019, 47, 405–419. [Google Scholar] [CrossRef]
- Chang, Z.; Lichtenstein, P.; Asherson, P.J.; Larsson, H. Developmental twin study of attention problems: High heritabilities throughout development. JAMA Psychiatry 2013, 70, 311–318. [Google Scholar] [CrossRef]
- Barkley, R.A. Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychol. Bull. 1997, 121, 65–94. [Google Scholar] [CrossRef]
- Brauer, H.; Ziegler, C.; Dempfle, A.; Freitag, C.; Siniatchkin, M.; Krauel, K.; Prehn-Kristensen, A. Transcranial direct current stimulation in ADHD–First results of the trial E-StimADHD. Brain Stimul. Basic Transl. Clin. Res. Neuromodul. 2023, 16, 170–171. [Google Scholar] [CrossRef]
- Khaksarian, M.; Mirr, I.; Kordian, S.; Nooripour, R.; Ahangari, N.; Masjedi-Arani, A. A comparison of methylphenidate (MPH) and combined methylphenidate with Crocus sativus (Saffron) in the treatment of children and adolescents with ADHD: A randomized, double-blind, parallel-group, clinical trial. Iran. J. Psychiatry Behav. Sci. 2021, 15, e108390. [Google Scholar] [CrossRef]
- Bralten, J.; Greven, C.U.; Franke, B.; Mennes, M.; Zwiers, M.P.; Rommelse, N.N.; Hartman, C.; van der Meer, D.; O’Dwyer, L.; Oosterlaan, J.; et al. Voxel-based morphometry analysis reveals frontal brain differences in participants with ADHD and their unaffected siblings. J. Psychiatry Neurosci. 2016, 41, 272–279. [Google Scholar] [CrossRef]
- Casey, B.J.; Epstein, J.N.; Buhle, J.; Liston, C.; Davidson, M.C.; Tonev, S.T.; Spicer, J.; Niogi, S.; Millner, A.J.; Reiss, A.; et al. Frontostriatal connectivity and its role in cognitive control in parent-child dyads with ADHD. Am. J. Psychiatry 2007, 164, 1729–1736. [Google Scholar] [CrossRef] [PubMed]
- Godinez, D.A.; Willcutt, E.G.; Burgess, G.C.; Depue, B.E.; Andrews-Hanna, J.R.; Banich, M.T. Familial risk and ADHD-specific neural activity revealed by case-control, discordant twin pair design. Psychiatry Res. 2015, 233, 458–465. [Google Scholar] [CrossRef]
- Baboli, R.; Cao, M.; Halperin, J.M.; Li, X. Distinct Thalamic and Frontal Neuroanatomical Substrates in Children with Familial vs. Non-Familial Attention-Deficit/Hyperactivity Disorder (ADHD). Brain Sci. 2022, 13, 46. [Google Scholar] [CrossRef] [PubMed]
- Thompson, W.K.; Barch, D.M.; Bjork, J.M.; Gonzalez, R.; Nagel, B.J.; Nixon, S.J.; Luciana, M. The structure of cognition in 9 and 10 year-old children and associations with problem behaviors: Findings from the ABCD study’s baseline neurocognitive battery. Dev. Cogn. Neurosci. 2019, 36, 100606. [Google Scholar] [CrossRef] [PubMed]
- Karcher, N.R.; Barch, D.M. The ABCD study: Understanding the development of risk for mental and physical health outcomes. Neuropsychopharmacology 2021, 46, 131–142. [Google Scholar] [CrossRef]
- Feldstein Ewing, S.W.; Bjork, J.M.; Luciana, M. Implications of the ABCD study for developmental neuroscience. Dev. Cogn. Neurosci. 2018, 32, 161–164. [Google Scholar] [CrossRef]
- Garavan, H.; Bartsch, H.; Conway, K.; Decastro, A.; Goldstein, R.Z.; Heeringa, S.; Jernigan, T.; Potter, A.; Thompson, W.; Zahs, D. Recruiting the ABCD sample: Design considerations and procedures. Dev. Cogn. Neurosci. 2018, 32, 16–22. [Google Scholar] [CrossRef]
- Gershon, R.C.; Wagster, M.V.; Hendrie, H.C.; Fox, N.A.; Cook, K.F.; Nowinski, C.J. NIH toolbox for assessment of neurological and behavioral function. Neurology 2013, 80, S2–S6. [Google Scholar] [CrossRef]
- Kaufman, J.; Birmaher, B.; Brent, D.; Rao, U.; Flynn, C.; Moreci, P.; Williamson, D.; Ryan, N. Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): Initial reliability and validity data. J. Am. Acad. Child. Adolesc. Psychiatry 1997, 36, 980–988. [Google Scholar] [CrossRef] [PubMed]
- Barch, D.M.; Albaugh, M.D.; Avenevoli, S.; Chang, L.; Clark, D.B.; Glantz, M.D.; Hudziak, J.J.; Jernigan, T.L.; Tapert, S.F.; Yurgelun-Todd, D.; et al. Demographic, physical and mental health assessments in the adolescent brain and cognitive development study: Rationale and description. Dev. Cogn. Neurosci. 2018, 32, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Kobak, K.A.; Kratochvil, C.; Stanger, C.; Kaufman, J. Computerized screening of comorbidity in adolescents with substance or psychiatric disorders. In Anxiety Disorders and Depression; Department of Health and Human Services: La Jolaa, CA, USA, 2013. [Google Scholar]
- Kariuki, S.M.; Newton, C.; Abubakar, A.; Bitta, M.A.; Odhiambo, R.; Phillips Owen, J. Evaluation of Psychometric Properties and Factorial Structure of ADHD Module of K-SADS-PL in Children From Rural Kenya. J. Atten. Disord. 2020, 24, 2064–2071. [Google Scholar] [CrossRef] [PubMed]
- de la Pena, F.R.; Villavicencio, L.R.; Palacio, J.D.; Felix, F.J.; Larraguibel, M.; Viola, L.; Ortiz, S.; Rosetti, M.; Abadi, A.; Montiel, C.; et al. Validity and reliability of the kiddie schedule for affective disorders and schizophrenia present and lifetime version DSM-5 (K-SADS-PL-5) Spanish version. BMC Psychiatry 2018, 18, 193. [Google Scholar] [CrossRef]
- Conners, C.K.; Erhardt, D.; Sparrow, E.P. Conners’ Adult ADHD Rating Scales (CAARS): Technical Manual; Multi-Health Systems: North Tonawanda, NY, USA, 1999. [Google Scholar]
- Veale, J.F. Edinburgh Handedness Inventory—Short Form: A revised version based on confirmatory factor analysis. Laterality 2014, 19, 164–177. [Google Scholar] [CrossRef]
- Petersen, A.C.; Crockett, L.; Richards, M.; Boxer, A. A self-report measure of pubertal status: Reliability, validity, and initial norms. J. Youth Adolesc. 1988, 17, 117–133. [Google Scholar] [CrossRef]
- Achenbach, T.; Maruish, M. The Use of Psychological Testing for Treatment Planning and Outcomes Assessment; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 1999; pp. 429–466. [Google Scholar]
- Casey, B.J.; Cannonier, T.; Conley, M.I.; Cohen, A.O.; Barch, D.M.; Heitzeg, M.M.; Soules, M.E.; Teslovich, T.; Dellarco, D.V.; Garavan, H.; et al. The Adolescent Brain Cognitive Development (ABCD) study: Imaging acquisition across 21 sites. Dev. Cogn. Neurosci. 2018, 32, 43–54. [Google Scholar] [CrossRef]
- Yaple, Z.; Arsalidou, M. N-back Working Memory Task: Meta-analysis of Normative fMRI Studies with Children. Child. Dev. 2018, 89, 2010–2022. [Google Scholar] [CrossRef]
- Hagler, D.J., Jr.; Hatton, S.; Cornejo, M.D.; Makowski, C.; Fair, D.A.; Dick, A.S.; Sutherland, M.T.; Casey, B.J.; Barch, D.M.; Harms, M.P.; et al. Image processing and analysis methods for the Adolescent Brain Cognitive Development Study. Neuroimage 2019, 202, 116091. [Google Scholar] [CrossRef]
- Jenkinson, M.; Bannister, P.; Brady, M.; Smith, S. Improved optimization for the robust and accurate linear registration and motion correction of brain images. Neuroimage 2002, 17, 825–841. [Google Scholar] [CrossRef]
- Fonov, V.; Evans, A.C.; Botteron, K.; Almli, C.R.; McKinstry, R.C.; Collins, D.L.; Brain Development Cooperative, G. Unbiased average age-appropriate atlases for pediatric studies. Neuroimage 2011, 54, 313–327. [Google Scholar] [CrossRef] [PubMed]
- Fonov, V.S.; Evans, A.C.; McKinstry, R.C.; Almli, C.R.; Collins, D. Unbiased nonlinear average age-appropriate brain templates from birth to adulthood. NeuroImage 2009, 47, S102. [Google Scholar] [CrossRef]
- Woolrich, M.W.; Ripley, B.D.; Brady, M.; Smith, S.M. Temporal autocorrelation in univariate linear modeling of FMRI data. Neuroimage 2001, 14, 1370–1386. [Google Scholar] [CrossRef] [PubMed]
- Woo, C.W.; Krishnan, A.; Wager, T.D. Cluster-extent based thresholding in fMRI analyses: Pitfalls and recommendations. Neuroimage 2014, 91, 412–419. [Google Scholar] [CrossRef]
- Martinussen, R.; Hayden, J.; Hogg-Johnson, S.; Tannock, R. A meta-analysis of working memory impairments in children with attention-deficit/hyperactivity disorder. J. Am. Acad. Child. Adolesc. Psychiatry 2005, 44, 377–384. [Google Scholar] [CrossRef]
- Davis, T.; LaRocque, K.F.; Mumford, J.A.; Norman, K.A.; Wagner, A.D.; Poldrack, R.A. What do differences between multi-voxel and univariate analysis mean? How subject-, voxel-, and trial-level variance impact fMRI analysis. Neuroimage 2014, 97, 271–283. [Google Scholar] [CrossRef]
- Woolrich, M.W.; Behrens, T.E.; Beckmann, C.F.; Jenkinson, M.; Smith, S.M. Multilevel linear modelling for FMRI group analysis using Bayesian inference. Neuroimage 2004, 21, 1732–1747. [Google Scholar] [CrossRef]
- Rolls, E.T.; Huang, C.C.; Lin, C.P.; Feng, J.; Joliot, M. Automated anatomical labelling atlas 3. Neuroimage 2020, 206, 116189. [Google Scholar] [CrossRef]
- Rorden, C.; Brett, M. Stereotaxic display of brain lesions. Behav. Neurol. 2000, 12, 191–200. [Google Scholar] [CrossRef]
- Hull, R.; Vaid, J. Laterality and language experience. Laterality 2006, 11, 436–464. [Google Scholar] [CrossRef]
- Detre, J.A.; Maccotta, L.; King, D.; Alsop, D.C.; Glosser, G.; D’Esposito, M.; Zarahn, E.; Aguirre, G.K.; French, J.A. Functional MRI lateralization of memory in temporal lobe epilepsy. Neurology 1998, 50, 926–932. [Google Scholar] [CrossRef]
- Hutsler, J.; Galuske, R.A. Hemispheric asymmetries in cerebral cortical networks. Trends Neurosci. 2003, 26, 429–435. [Google Scholar] [CrossRef]
- Strauss, E.; Kosaka, B.; Wada, J. The neurobiological basis of lateralized cerebral function. A review. Hum. Neurobiol. 1983, 2, 115–127. [Google Scholar] [PubMed]
- Seghier, M.L. Laterality index in functional MRI: Methodological issues. Magn. Reson. Imaging 2008, 26, 594–601. [Google Scholar] [CrossRef]
- He, N.; Palaniyappan, L.; Linli, Z.; Guo, S. Abnormal hemispheric asymmetry of both brain function and structure in attention deficit/hyperactivity disorder: A meta-analysis of individual participant data. Brain Imaging Behav. 2022, 16, 54–68. [Google Scholar] [CrossRef] [PubMed]
- Buracas, G.T.; Fine, I.; Boynton, G.M. The relationship between task performance and functional magnetic resonance imaging response. J. Neurosci. 2005, 25, 3023–3031. [Google Scholar] [CrossRef]
- Xia, M.; Wang, J.; He, Y. BrainNet Viewer: A network visualization tool for human brain connectomics. PLoS ONE 2013, 8, e68910. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.J.; Wagner, A.D. Cognitive control and right ventrolateral prefrontal cortex: Reflexive reorienting, motor inhibition, and action updating. Ann. N. Y. Acad. Sci. 2011, 1224, 40–62. [Google Scholar] [CrossRef]
- Rubia, K.; Smith, A.B.; Brammer, M.J.; Taylor, E. Right inferior prefrontal cortex mediates response inhibition while mesial prefrontal cortex is responsible for error detection. Neuroimage 2003, 20, 351–358. [Google Scholar] [CrossRef]
- Hampshire, A.; Chamberlain, S.R.; Monti, M.M.; Duncan, J.; Owen, A.M. The role of the right inferior frontal gyrus: Inhibition and attentional control. Neuroimage 2010, 50, 1313–1319. [Google Scholar] [CrossRef]
- Liakakis, G.; Nickel, J.; Seitz, R.J. Diversity of the inferior frontal gyrus—A meta-analysis of neuroimaging studies. Behav. Brain Res. 2011, 225, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.E.; Jonides, J. Neuroimaging analyses of human working memory. Proc. Natl. Acad. Sci. USA 1998, 95, 12061–12068. [Google Scholar] [CrossRef] [PubMed]
- Duncan, J. An adaptive coding model of neural function in prefrontal cortex. Nat. Rev. Neurosci. 2001, 2, 820–829. [Google Scholar] [CrossRef] [PubMed]
- Corbetta, M.; Shulman, G.L. Control of goal-directed and stimulus-driven attention in the brain. Nat. Rev. Neurosci. 2002, 3, 201–215. [Google Scholar] [CrossRef] [PubMed]
- Jonides, J.; Smith, E.E.; Koeppe, R.A.; Awh, E.; Minoshima, S.; Mintun, M.A. Spatial working memory in humans as revealed by PET. Nature 1993, 363, 623–625. [Google Scholar] [CrossRef]
- Owen, A.M.; McMillan, K.M.; Laird, A.R.; Bullmore, E. N-back working memory paradigm: A meta-analysis of normative functional neuroimaging studies. Hum. Brain Mapp. 2005, 25, 46–59. [Google Scholar] [CrossRef]
- Conklin, H.M.; Luciana, M.; Hooper, C.J.; Yarger, R.S. Working memory performance in typically developing children and adolescents: Behavioral evidence of protracted frontal lobe development. Dev. Neuropsychol. 2007, 31, 103–128. [Google Scholar] [CrossRef]
- Sergeant, J.A.; Geurts, H.; Huijbregts, S.; Scheres, A.; Oosterlaan, J. The top and the bottom of ADHD: A neuropsychological perspective. Neurosci. Biobehav. Rev. 2003, 27, 583–592. [Google Scholar] [CrossRef]
- Andreou, P.; Neale, B.M.; Chen, W.; Christiansen, H.; Gabriels, I.; Heise, A.; Meidad, S.; Muller, U.C.; Uebel, H.; Banaschewski, T.; et al. Reaction time performance in ADHD: Improvement under fast-incentive condition and familial effects. Psychol. Med. 2007, 37, 1703–1715. [Google Scholar] [CrossRef]
- Bush, G. Cingulate, frontal, and parietal cortical dysfunction in attention-deficit/hyperactivity disorder. Biol. Psychiatry 2011, 69, 1160–1167. [Google Scholar] [CrossRef]
- Rubia, K. “Cool” inferior frontostriatal dysfunction in attention-deficit/hyperactivity disorder versus “hot” ventromedial orbitofrontal-limbic dysfunction in conduct disorder: A review. Biol. Psychiatry 2011, 69, e69–e87. [Google Scholar] [CrossRef]
- Max, J.E.; Fox, P.T.; Lancaster, J.L.; Kochunov, P.; Mathews, K.; Manes, F.F.; Robertson, B.A.; Arndt, S.; Robin, D.A.; Lansing, A.E. Putamen lesions and the development of attention-deficit/hyperactivity symptomatology. J. Am. Acad. Child. Adolesc. Psychiatry 2002, 41, 563–571. [Google Scholar] [CrossRef]
- Cortese, S.; Kelly, C.; Chabernaud, C.; Proal, E.; Di Martino, A.; Milham, M.P.; Castellanos, F.X. Toward systems neuroscience of ADHD: A meta-analysis of 55 fMRI studies. Am. J. Psychiatry 2012, 169, 1038–1055. [Google Scholar] [CrossRef]
- Samea, F.; Soluki, S.; Nejati, V.; Zarei, M.; Cortese, S.; Eickhoff, S.B.; Tahmasian, M.; Eickhoff, C.R. Brain alterations in children/adolescents with ADHD revisited: A neuroimaging meta-analysis of 96 structural and functional studies. Neurosci. Biobehav. Rev. 2019, 100, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Petrides, M. Lateral prefrontal cortex: Architectonic and functional organization. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2005, 360, 781–795. [Google Scholar] [CrossRef] [PubMed]
- Miller, B.L.; Cummings, J.L. The Human Frontal Lobes: Functions and Disorders, 3rd ed.; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- Wager, T.D.; Smith, E.E. Neuroimaging studies of working memory: A meta-analysis. Cogn. Affect. Behav. Neurosci. 2003, 3, 255–274. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; He, W.; Wu, J.; Zhang, J.; Jin, Z.; Li, L. A coordinate-based meta-analysis of the n-back working memory paradigm using activation likelihood estimation. Brain Cogn. 2019, 132, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Dickstein, S.G.; Bannon, K.; Castellanos, F.X.; Milham, M.P. The neural correlates of attention deficit hyperactivity disorder: An ALE meta-analysis. J. Child. Psychol. Psychiatry 2006, 47, 1051–1062. [Google Scholar] [CrossRef] [PubMed]
- Rubia, K. Cognitive Neuroscience of Attention Deficit Hyperactivity Disorder (ADHD) and Its Clinical Translation. Front. Hum. Neurosci. 2018, 12, 100. [Google Scholar] [CrossRef]
- Quinn, P.O.; Madhoo, M. A review of attention-deficit/hyperactivity disorder in women and girls: Uncovering this hidden diagnosis. Prim. Care Companion CNS Disord. 2014, 16, 27250. [Google Scholar] [CrossRef]
- Vilgis, V.; Yee, D.; Silk, T.J.; Vance, A. Distinct Neural Profiles of Frontoparietal Networks in Boys with ADHD and Boys with Persistent Depressive Disorder. Cogn. Affect. Behav. Neurosci. 2022, 22, 1183–1198. [Google Scholar] [CrossRef] [PubMed]
- Czerniak, S.M.; Sikoglu, E.M.; King, J.A.; Kennedy, D.N.; Mick, E.; Frazier, J.; Moore, C.M. Areas of the brain modulated by single-dose methylphenidate treatment in youth with ADHD during task-based fMRI: A systematic review. Harv. Rev. Psychiatry 2013, 21, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Monden, Y.; Dan, H.; Nagashima, M.; Dan, I.; Tsuzuki, D.; Kyutoku, Y.; Gunji, Y.; Yamagata, T.; Watanabe, E.; Momoi, M.Y. Right prefrontal activation as a neuro-functional biomarker for monitoring acute effects of methylphenidate in ADHD children: An fNIRS study. Neuroimage Clin. 2012, 1, 131–140. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TDC (N = 186) | ADHD (N = 176) | Test Statistic | p | |
|---|---|---|---|---|
| Sex | χ2(1) = 3.528 | 0.06 | ||
| Female | 89 | 67 | ||
| Male | 97 | 109 | ||
| Race | χ2(3) = 0.898 | 0.826 | ||
| White American | 144 | 133 | ||
| Black American | 17 | 16 | ||
| Mixed | 17 | 21 | ||
| Other | 8 | 6 | ||
| Handedness | χ2(2) = 1.222 | 0.543 | ||
| Right | 157 | 141 | ||
| Left | 9 | 12 | ||
| Both | 20 | 23 | ||
| Age (in months) (Mean (SD)) | 119.87 (6.82) | 119.09 (7.84) | t(347.029) = 1.008 + | 0.314 |
| Parents combined income (Mean score (SD)) | 7.70 (2.19) (N = 176) | 7.67 (1.98) (N = 167) | t(341) = 0.150 | 0.881 |
| Primary parent education status (in years) (Mean (SD)) | 16.35 (2.19) | 16.48 (2.04) | t(360) = −0.550 | 0.583 |
| IQ | ||||
| Picture vocabulary (Mean (SD)) | 108.18 (15.15) (N = 184) | 108.96 (18.92) (N = 174) | t(331.293) = −0.426 + | 0.670 |
| Matrix reasoning (Mean (SD)) | 10.45 (2.74) (N = 180) | 9.91 (3.08) (N = 174) | t(352) = 1.749 | 0.081 |
| Pubertal developmental scale (Mean score (SD)) | 1.61 (0.77) | 1.58 (0.76) | t(360) = 0.347 | 0.729 |
| Behavioral measures | ||||
| CBCL attention problems T-score (Mean (SD)) | 50.50 (1.051) | 63.55 (8.172) | t(180.484) = −21.024 + | <0.001 |
| CBCL ADHD T-score (Mean (SD)) | 50.28 (0.798) | 62.57 (7.911) | t(178.373) = −20.501 + | <0.001 |
| KSADS-5 inattention score (Mean (SD)) | 0.763 (1.466) | 20.835 (5.381) | t(199.518) = −47.839 + | <0.001 |
| KSADS-5 hyperactivity score (Mean (SD)) | 0.194 (0.611) | 17.761 (8.6315) | t(176.659) = −26.938 + | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, X.; Motwani, C.; Cao, M.; Martin, E.; Halperin, J.M. Working Memory-Related Neurofunctional Correlates Associated with the Frontal Lobe in Children with Familial vs. Non-Familial Attention Deficit/Hyperactivity Disorder. Brain Sci. 2023, 13, 1469. https://doi.org/10.3390/brainsci13101469
Li X, Motwani C, Cao M, Martin E, Halperin JM. Working Memory-Related Neurofunctional Correlates Associated with the Frontal Lobe in Children with Familial vs. Non-Familial Attention Deficit/Hyperactivity Disorder. Brain Sciences. 2023; 13(10):1469. https://doi.org/10.3390/brainsci13101469
Chicago/Turabian StyleLi, Xiaobo, Chirag Motwani, Meng Cao, Elizabeth Martin, and Jeffrey M. Halperin. 2023. "Working Memory-Related Neurofunctional Correlates Associated with the Frontal Lobe in Children with Familial vs. Non-Familial Attention Deficit/Hyperactivity Disorder" Brain Sciences 13, no. 10: 1469. https://doi.org/10.3390/brainsci13101469