
Application of Immersive Virtual-Reality-Based Puzzle Games in Elderly Patients with Post-Stroke Cognitive Impairment: A Pilot Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Assessments and Questionnaire
2.4. VR Equipment
2.4.1. VR Integrity System Construction
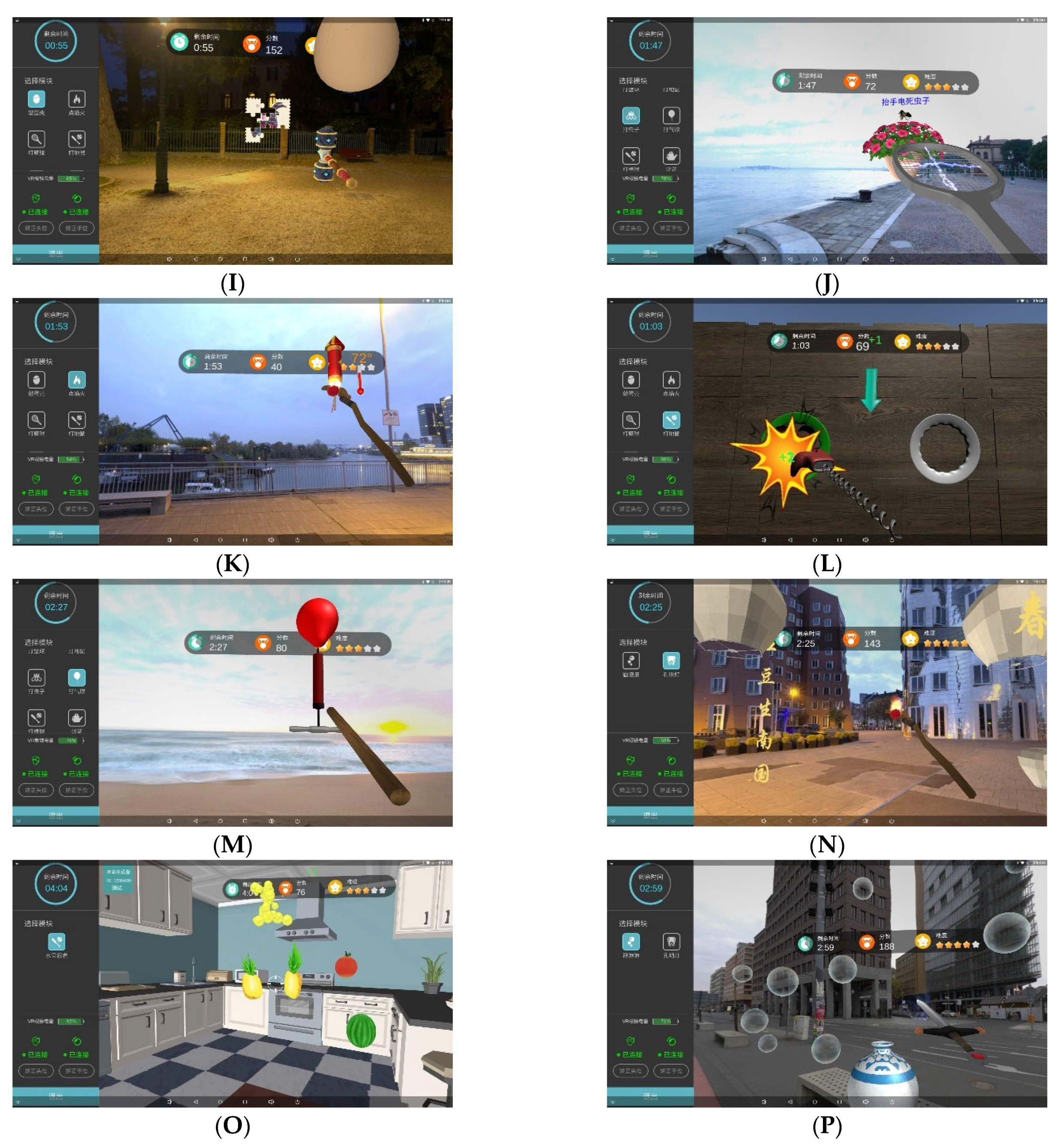
2.4.2. Scene Modeling
2.5. Statistical Analysis
3. Results
3.1. Baseline Clinical Data
3.2. Results of the Cognitive Evaluation
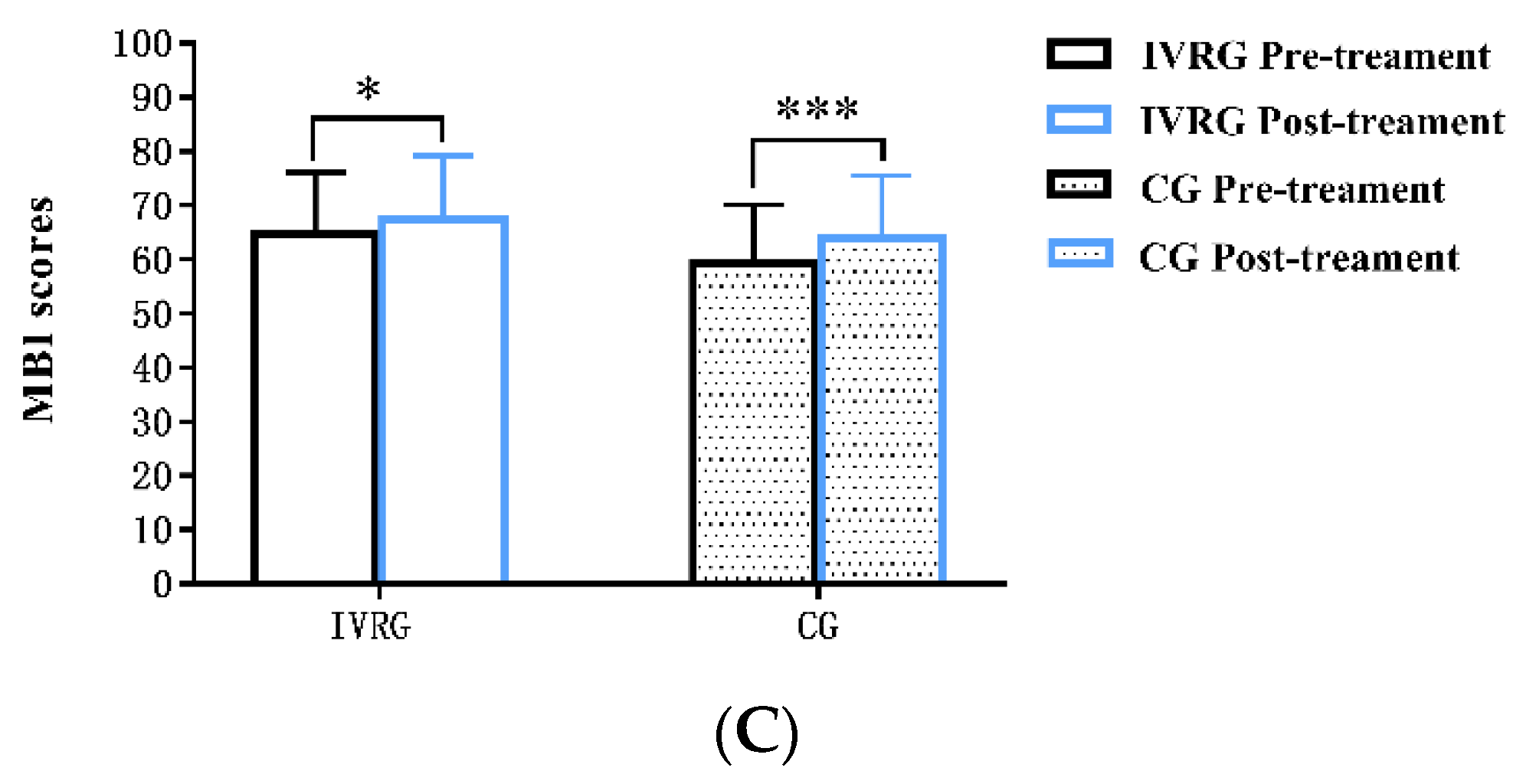
3.3. Self-Report Questionnaire
3.4. Side Effects
4. Discussion
4.1. Effectiveness of IVR-Based Puzzle Games
4.2. Feasibility and Safety of IVR in Elderly Stroke Patients
4.3. Limitations and Prospects
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zheng, Z. From the past to the future: What we learn from China’s 2020 Census. China Popul. Dev. Stud. 2021, 5, 101–106. [Google Scholar] [CrossRef]
- Lo, J.W.; Crawford, J.D.; Desmond, D.W.; Bae, H.J.; Lim, J.S.; Godefroy, O.; Roussel, M.; Kang, Y.; Jahng, S.; Kohler, S.; et al. Long-Term Cognitive Decline After Stroke: An Individual Participant Data Meta-Analysis. Stroke 2022, 53, 1318–1327. [Google Scholar] [CrossRef] [PubMed]
- Pendlebury, S.T.; Rothwell, P.M. Incidence and prevalence of dementia associated with transient ischaemic attack and stroke: Analysis of the population-based Oxford Vascular Study. Lancet Neurol. 2019, 18, 248–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altieri, M.; Di Piero, V.; Pasquini, M.; Gasparini, M.; Vanacore, N.; Vicenzini, E.; Lenzi, G.L. Delayed poststroke dementia: A 4-year follow-up study. Neurology 2004, 62, 2193–2197. [Google Scholar] [CrossRef]
- Hurford, R.; Charidimou, A.; Fox, Z.; Cipolotti, L.; Werring, D.J. Domain-specific trends in cognitive impairment after acute ischaemic stroke. J. Neurol. 2013, 260, 237–241. [Google Scholar] [CrossRef]
- Hénon, H.; Pasquier, F.; Leys, D. Poststroke Dementia. Cerebrovasc. Dis. 2006, 22, 61–70. [Google Scholar] [CrossRef]
- Morley, J.E. An Overview of Cognitive Impairment. Clin. Geriatr. Med. 2018, 34, 505–513. [Google Scholar] [CrossRef]
- Miotto, E.C.; Bazan, P.R.; Batista, A.X.; Conforto, A.B.; Figueiredo, E.G.; Martin, M.; Avolio, I.B.; Amaro, E.J.; Teixeira, M.J. Corrigendum: Behavioral and Neural Correlates of Cognitive Training and Transfer Effects in Stroke Patients. Front. Neurol. 2021, 12, 785008. [Google Scholar] [CrossRef]
- Unverzagt, F.W.; Guey, L.T.; Jones, R.N.; Marsiske, M.; King, J.W.; Wadley, V.G.; Crowe, M.; Rebok, G.W.; Tennstedt, S.L. ACTIVE cognitive training and rates of incident dementia. J. Int. Neuropsychol. Soc. 2012, 18, 669–677. [Google Scholar] [CrossRef] [Green Version]
- Parsons, T.D. Virtual Reality for Enhanced Ecological Validity and Experimental Control in the Clinical, Affective and Social Neurosciences. Front. Hum. Neurosci. 2015, 9, 660. [Google Scholar] [CrossRef]
- Huang, K. Exergaming Executive Functions: An Immersive Virtual Reality-Based Cognitive Training for Adults Aged 50 and Older. Cyberpsychol. Behav. Soc. Netw. 2020, 23, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Wang, Y.; Yao, M.Z.; Tang, Q.; Yang, Y. The Effects of Viewing an Uplifting 360-Degree Video on Emotional Well-Being Among Elderly Adults and College Students Under Immersive Virtual Reality and Smartphone Conditions. Cyberpsychol. Behav. Soc. Netw 2020, 23, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Niki, K.; Yahara, M.; Inagaki, M.; Takahashi, N.; Watanabe, A.; Okuda, T.; Ueda, M.; Iwai, D.; Sato, K.; Ito, T. Immersive Virtual Reality Reminiscence Reduces Anxiety in the Oldest-Old Without Causing Serious Side Effects: A Single-Center, Pilot, and Randomized Crossover Study. Front. Hum. Neurosci. 2020, 14, 598161. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.C.; Wang, H.K.; Wu, R.M.; Lo, C.S.; Lin, K.H. Home-based virtual reality balance training and conventional balance training in Parkinson’s disease: A randomized controlled trial. J. Med. Assoc. 2016, 115, 734–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muhla, F.; Clanche, F.; Duclos, K.; Meyer, P.; Maiaux, S.; Colnat-Coulbois, S.; Gauchard, G.C. Impact of using immersive virtual reality over time and steps in the Timed Up and Go test in elderly people. PLoS ONE 2020, 15, e0229594. [Google Scholar] [CrossRef] [Green Version]
- Muhla, F.; Duclos, K.; Clanche, F.; Meyer, P.; Maiaux, S.; Colnat-Coulbois, S.; Gauchard, G.C. Does the Management of Visual and Audible Motion Information during an Immersive Virtual Reality Timed Up and Go Test Impact Locomotor Performance in the Elderly? Gerontology 2022, 68, 456–464. [Google Scholar] [CrossRef]
- Kiper, P.; Szczudlik, A.; Agostini, M.; Opara, J.; Nowobilski, R.; Ventura, L.; Tonin, P.; Turolla, A. Virtual Reality for Upper Limb Rehabilitation in Subacute and Chronic Stroke: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2018, 99, 834–842. [Google Scholar] [CrossRef]
- Laver, K.E.; George, S.; Thomas, S.; Deutsch, J.E.; Crotty, M. Virtual reality for stroke rehabilitation. Cochrane Database Syst. Rev. 2017, 11, CD008349. [Google Scholar] [CrossRef] [Green Version]
- Olk, B.; Dinu, A.; Zielinski, D.J.; Kopper, R. Measuring visual search and distraction in immersive virtual reality. R. Soc. Open. Sci. 2018, 5, 172331. [Google Scholar] [CrossRef] [Green Version]
- Huang, L.C.; Yang, Y.H. The Long-term Effects of Immersive Virtual Reality Reminiscence in People With Dementia: Longitudinal Observational Study. JMIR Serious Games 2022, 10, e36720. [Google Scholar] [CrossRef]
- Maeng, S.; Hong, J.P.; Kim, W.; Kim, H.; Cho, S.; Kang, J.M.; Na, K.; Oh, S.; Park, J.W.; Bae, J.N.; et al. Effects of Virtual Reality-Based Cognitive Training in the Elderly with and without Mild Cognitive Impairment. Psychiatry Investig. 2021, 18, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Manera, V.; Petit, P.; Derreumaux, A.; Orvieto, I.; Romagnoli, M.; Lyttle, G.; David, R.; Robert, P.H. ‘Kitchen and cooking,’a serious game for mild cognitive impairment and Alzheimer’s disease: A pilot study. Front. Aging Neurosci. 2015, 7, 00024. [Google Scholar] [CrossRef] [PubMed]
- Chesham, A.; Gerber, S.M.; Schütz, N.; Saner, H.; Gutbrod, K.; Müri, R.M.; Nef, T.; Urwyler, P. Search and Match Task: Development of a Taskified Match-3 Puzzle Game to Assess and Practice Visual Search. JMIR Serious Games 2019, 7, e13620. [Google Scholar] [CrossRef] [PubMed]
- Krebs, C.; Falkner, M.; Niklaus, J.; Persello, L.; Kloppel, S.; Nef, T.; Urwyler, P. Application of Eye Tracking in Puzzle Games for Adjunct Cognitive Markers: Pilot Observational Study in Older Adults. JMIR Serious Games 2021, 9, e24151. [Google Scholar] [CrossRef]
- Nef, T.; Chesham, A.; Schutz, N.; Botros, A.A.; Vanbellingen, T.; Burgunder, J.M.; Mullner, J.; Martin, M.R.; Urwyler, P. Development and Evaluation of Maze-Like Puzzle Games to Assess Cognitive and Motor Function in Aging and Neurodegenerative Diseases. Front. Aging Neurosci. 2020, 12, 87. [Google Scholar] [CrossRef] [Green Version]
- Dong, Q.; Guo, Q.; Luo, B.; Xu, Y. Expert consensus on the management of cognitive impairment after stroke. Chin. J. Stroke 2017, 12, 519–531. [Google Scholar]
- Rogers, J.M.; Duckworth, J.; Middleton, S.; Steenbergen, B.; Wilson, P.H. Elements virtual rehabilitation improves motor, cognitive, and functional outcomes in adult stroke: Evidence from a randomized controlled pilot study. J. Neuroeng. Rehabil. 2019, 16, 56. [Google Scholar] [CrossRef] [Green Version]
- Huang, L.; Chen, K.L.; Lin, B.Y.; Tang, L.; Zhao, Q.H.; Lv, Y.R.; Guo, Q.H. Chinese version of Montreal Cognitive Assessment Basic for discrimination among different severities of Alzheimer’s disease. Neuropsychiatr. Dis. Treat. 2018, 14, 2133–2140. [Google Scholar] [CrossRef] [Green Version]
- Ziad, S.; Nasreddine, M.; Natalie, A.; Phillips, P.; Dirian, B.V.R.B. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar]
- Mateen, B.A.; Bussas, M.; Doogan, C.; Waller, D.; Saverino, A.; Kiraly, F.J.; Playford, E.D. The Trail Making test: A study of its ability to predict falls in the acute neurological in-patient population. Clin. Rehabil. 2018, 32, 1396–1405. [Google Scholar] [CrossRef]
- Rosano, C.; Newman, A.B.; Katz, R.; Hirsch, C.H.; Kuller, L.H. Association between lower digit symbol substitution test score and slower gait and greater risk of mortality and of developing incident disability in well-functioning older adults. J. Am. Geriatr. Soc. 2008, 56, 1618–1625. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.; Wang, J.; Fan, H.; Yao, J.; Chen, N.; Duan, J.; Zou, Y. Norm development of the Chinese edition of Wechsler Adult Intelligence Scale-Fourth Edition. Chin. Ment. Health J. 2017, 31, 635–641. [Google Scholar]
- Manly, J.J.; Jacobs, D.M.; Sano, M.; Bell, K.; Merchant, C.A.; Small, S.A.; Stern, Y. Effect of literacy on neuropsychological test performance in nondemented, education-matched elders. J. Int. Neuropsychol. Soc. 1999, 5, 191–202. [Google Scholar] [CrossRef] [PubMed]
- Collin, C.; Wade, D.T.; Davies, S.; Horne, V. The Barthel ADL Index: A reliability study. Int. Disabil. Stud. 1988, 10, 61–63. [Google Scholar] [CrossRef]
- Hachinski, V.; Iadecola, C.; Petersen, R.C.; Breteler, M.M.; Nyenhuis, D.L.; Black, S.E.; Powers, W.J.; Decarli, C.; Merino, J.G.; Kalaria, R.N.; et al. National Institute of Neurological Disorders and Stroke-Canadian Stroke Network vascular cognitive impairment harmonization standards. Stroke 2006, 37, 2220–2241. [Google Scholar] [CrossRef]
- Zhao, Q.; Guo, Q.; Hong, Z. Clustering and switching during a semantic verbal fluency test contribute to differential diagnosis of cognitive impairment. Neurosci. Bull. 2013, 29, 75–82. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.; Vanclay, F.; Cooper, B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J. Clin. Epidemiol. 1989, 42, 703–709. [Google Scholar] [CrossRef]
- Zhang, Q.; Fu, Y.; Lu, Y.; Zhang, Y.; Huang, Q.; Yang, Y.; Zhang, K.; Li, M. Impact of Virtual Reality-Based Therapies on Cognition and Mental Health of Stroke Patients: Systematic Review and Meta-analysis. J. Med. Internet. Res. 2021, 23, e31007. [Google Scholar] [CrossRef]
- Alvarez, J.A.; Emory, E. Executive function and the frontal lobes: A meta-analytic review. Neuropsychol. Rev. 2006, 16, 17–42. [Google Scholar] [CrossRef]
- You, S.H.; Jang, S.H.; Kim, Y.H.; Hallett, M.; Ahn, S.H.; Kwon, Y.H.; Kim, J.H.; Lee, M.Y. Virtual reality-induced cortical reorganization and associated locomotor recovery in chronic stroke: An experimenter-blind randomized study. Stroke 2005, 36, 1166–1171. [Google Scholar] [CrossRef] [Green Version]
- Carrieri, M.; Petracca, A.; Lancia, S.; Basso, M.S.; Brigadoi, S.; Spezialetti, M.; Ferrari, M.; Placidi, G.; Quaresima, V. Prefrontal Cortex Activation Upon a Demanding Virtual Hand-Controlled Task: A New Frontier for Neuroergonomics. Front. Hum. Neurosci. 2016, 10, 53. [Google Scholar] [CrossRef] [Green Version]
- García-Betances, R.I.; Arredondo Waldmeyer, M.T.; Fico, G.; Cabrera-Umpiérrez, M.F. A Succinct Overview of Virtual Reality Technology Use in Alzheimer’s Disease. Front. Aging Neurosci. 2015, 7, 00080. [Google Scholar]
- Monteiro-Junior, R.S.; Vaghetti, C.A.; Nascimento, O.J.; Laks, J.; Deslandes, A.C. Exergames: Neuroplastic hypothesis about cognitive improvement and biological effects on physical function of institutionalized older persons. Neural. Regen. Res. 2016, 11, 201–204. [Google Scholar] [CrossRef] [PubMed]
- Flannery, R.J. Treating learned helplessness in the elderly dementia patient: Preliminary inquiry. Am. J. Alzheimer’s Dis. Other Demen 2002, 17, 345–349. [Google Scholar] [CrossRef]
- Park, M.J.; Kim, D.J.; Lee, U.; Na, E.J.; Jeon, H.J. A Literature Overview of Virtual Reality (VR) in Treatment of Psychiatric Disorders: Recent Advances and Limitations. Front. Psychiatry 2019, 10, 505. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Chen, G.; Xie, Y.; Chen, Z. Aging Effect on Visuomotor Adaptation: Mediated by Cognitive Decline. Front. Aging Neurosci. 2021, 13, 742928. [Google Scholar] [CrossRef] [PubMed]
- Campos, J.L.; Marusic, U.; Mahoney, J.R. Editorial: The intersection of cognitive, motor, and sensory processing in aging: Links to functional outcomes, Volume I. Front. Aging Neurosci. 2022, 14, 1009532. [Google Scholar] [CrossRef]
- Bauer, A.C.; M.Andringa, G. The Potential of Immersive Virtual Reality for Cognitive Training in Elderly. Gerontology 2020, 66, 614–623. [Google Scholar] [CrossRef] [PubMed]
- Freiherr, J.; Lundstrom, J.N.; Habel, U.; Reetz, K. Multisensory integration mechanisms during aging. Front. Hum. Neurosci. 2013, 7, 863. [Google Scholar] [CrossRef] [Green Version]
- Htut, T.Z.; Hiengkaew, V.; Jalayondeja, C.; Vongsirinavarat, M. Effects of physical, virtual reality-based, and brain exercise on physical, cognition, and preference in older persons: A randomized controlled trial. Eur. Rev. Aging Phys. Act. 2018, 15, 10. [Google Scholar] [CrossRef]
- Ohura, T.; Hase, K.; Nakajima, Y.; Nakayama, T. Validity and reliability of a performance evaluation tool based on the modified Barthel Index for stroke patients. BMC Med. Res. Methodol. 2017, 17, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kober, S.E.; Wood, G.; Hofer, D.; Kreuzig, W.; Kiefer, M.; Neuper, C. Virtual reality in neurologic rehabilitation of spatial disorientation. J. Neuroeng. Rehabil. 2013, 10, 17. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.R.; Chun, M.H.; Kim, L.S.; Park, J.Y. Effect of Virtual Reality on Cognition in Stroke Patients. Ann. Rehabil. Med. 2011, 35, 450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cunha, N.M.D.; Nguyen, D.; Naumovski, N.; Mckune, A.J.; Kellett, J.; Georgousopoulou, E.N.; Frost, J.; Isbel, S. A Mini-Review of Virtual Reality-Based Interventions to Promote Well-Being for People Living with Dementia and Mild Cognitive Impairment. Gerontology 2019, 65, 430–440. [Google Scholar]
- Gamito, P.; Oliveira, J.; Coelho, C.; Morais, D.; Lopes, P.; Pacheco, J.; Brito, R.; Soares, F.; Santos, N.; Barata, A.F. Cognitive training on stroke patients via virtual reality-based serious games. Disabil. Rehabil. 2017, 39, 385–388. [Google Scholar] [CrossRef] [PubMed]
- Optale, G.; Urgesi, C.; Busato, V.; Marin, S.; Piron, L.; Priftis, K.; Gamberini, L.; Capodieci, S.; Bordin, A. Controlling Memory Impairment in Elderly Adults Using Virtual Reality Memory Training: A Randomized Controlled Pilot Study. Neurorehabilit. Neural. Repair. 2010, 24, 348–357. [Google Scholar] [CrossRef]
- Huygelier, H.; Schraepen, B.; van Ee, R.; Vanden Abeele, V.; Gillebert, C.R. Acceptance of immersive head-mounted virtual reality in older adults. Sci. Rep. 2019, 9, 4519. [Google Scholar] [CrossRef] [Green Version]
- Plechatá, A.; Sahula, V.; Fayette, D.; Fajnerová, I. Age-Related Differences With Immersive and Non-immersive Virtual Reality in Memory Assessment. Front. Psychol. 2019, 10, 1330. [Google Scholar] [CrossRef]
- Wiley, E.; Khattab, S.; Tang, A. Examining the effect of virtual reality therapy on cognition post-stroke: A systematic review and meta-analysis. Disabil. Rehabil. Assist. Technol. 2022, 17, 50–60. [Google Scholar] [CrossRef]
- Jonsdottir, J.; Baglio, F.; Gindri, P.; Isernia, S.; Castiglioni, C.; Gramigna, C.; Palumbo, G.; Pagliari, C.; Di Tella, S.; Perini, G.; et al. Virtual Reality for Motor and Cognitive Rehabilitation From Clinic to Home: A Pilot Feasibility and Efficacy Study for Persons With Chronic Stroke. Front. Neurol. 2021, 12, 601131. [Google Scholar] [CrossRef]
- Broeren, J.; Claesson, L.; Goude, D.; Rydmark, M.; Sunnerhagen, K.S. Virtual Rehabilitation in an Activity Centre for Community-Dwelling Persons with Stroke. Cerebrovasc. Dis. 2008, 26, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Morganti, F. Virtual interaction in cognitive neuropsychology. Stud. Health Technol. Inf. 2004, 99, 55–70. [Google Scholar]
- Baker, S.; Waycott, J.; Robertson, E.; Carrasco, R.; Neves, B.B.; Hampson, R.; Vetere, F. Evaluating the use of interactive virtual reality technology with older adults living in residential aged care. Inf. Process. Manag. 2020, 57, 102105. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IVRG n = 15 | CG n = 15 | T | p Value | |
|---|---|---|---|---|
| Age (Years) | 74.93 ± 6.81 | 73.40 ± 7.5 | 0.586 | 0.562 |
| Male/Female | 9/6 | 8/7 | 1 a | |
| Time since onset (months) | 42.93 ± 34.54 | 29.27 ± 36.51 | 1.053 | 0.301 |
| Type, n (%) | 0.427 a | |||
| Cerebral infarction | 12(80) | 9(60) | ||
| Cerebral hemorrhage | 3(20) | 6(40) |
| IVRG (n = 15) | CG (n = 15) | T/Z | p-Value | |
|---|---|---|---|---|
| MOCA | 21.47 ± 2.67 | 21.27 ± 2.76 | 0.202 | 0.842 a |
| TMT A(s) | 155 ± 67.48 | 159.4 ± 97.33 | 0.144 | 0.887 a |
| MBI | 64.67 ± 11.41 | 59.33 ± 10.83 | 1.313 | 0.200 a |
| DSST | 14,6 | 12,12 | 0.956 | 0.339 b |
| FDST | 7,1 | 7,2 | 0.441 | 0.659 b |
| BDST | 4,1 | 4,1 | 0.334 | 0.738 b |
| VFT | 14,5 | 11,6 | 1.494 | 0.135 b |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Z.; He, Z.; Yuan, J.; Lin, H.; Fu, C.; Zhang, Y.; Wang, N.; Li, G.; Bu, J.; Chen, M.; et al. Application of Immersive Virtual-Reality-Based Puzzle Games in Elderly Patients with Post-Stroke Cognitive Impairment: A Pilot Study. Brain Sci. 2023, 13, 79. https://doi.org/10.3390/brainsci13010079
Liu Z, He Z, Yuan J, Lin H, Fu C, Zhang Y, Wang N, Li G, Bu J, Chen M, et al. Application of Immersive Virtual-Reality-Based Puzzle Games in Elderly Patients with Post-Stroke Cognitive Impairment: A Pilot Study. Brain Sciences. 2023; 13(1):79. https://doi.org/10.3390/brainsci13010079
Chicago/Turabian StyleLiu, Zhilan, Zhijie He, Jing Yuan, Hua Lin, Conghui Fu, Yan Zhang, Nian Wang, Guo Li, Jing Bu, Mei Chen, and et al. 2023. "Application of Immersive Virtual-Reality-Based Puzzle Games in Elderly Patients with Post-Stroke Cognitive Impairment: A Pilot Study" Brain Sciences 13, no. 1: 79. https://doi.org/10.3390/brainsci13010079