
Repetitive Transcranial Magnetic Stimulation of the Brain Region Activated by Motor Imagery Involving a Paretic Wrist and Hand for Upper-Extremity Motor Improvement in Severe Stroke: A Preliminary Study
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
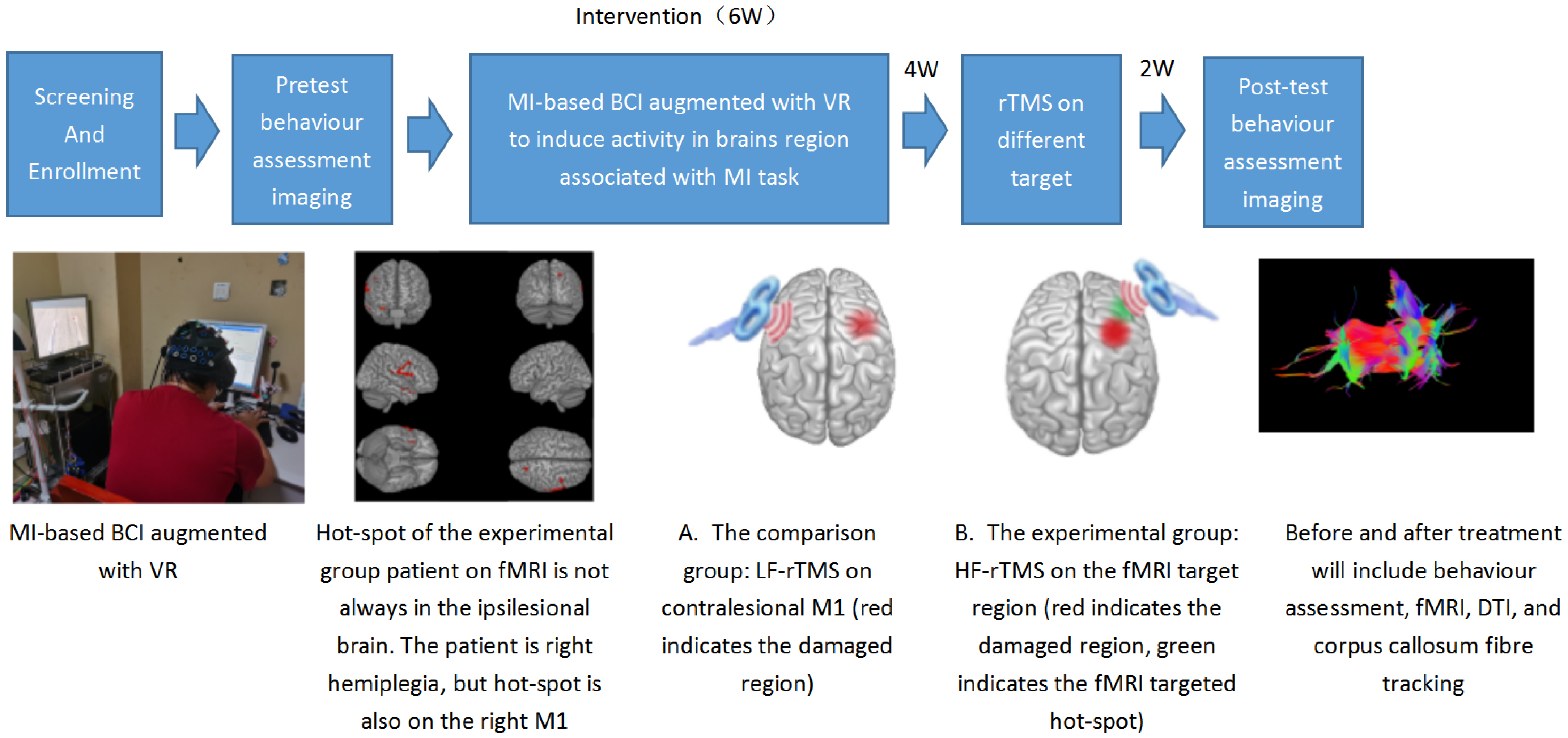
2.2. Intervention
2.2.1. Inducing Neural Activity in Associated Brain Regions during Motor Imagery Involving a Paretic Wrist and Hand
2.2.2. Activated Brain Regions during MI Tasks Determined Using fMRI
2.2.3. Transcranial Magnetic Stimulation
Measurement of Cortical Excitability
Repetitive TMS
2.3. Assessments
2.3.1. Primary Outcome
2.3.2. Secondary Outcomes
2.3.3. Commissural Fibres across the Corpus Callosum
2.4. Statistical Analysis
3. Results
3.1. Participants
3.2. Activated Brain Regions during Motor Imagery Tasks and the Stimulation Target
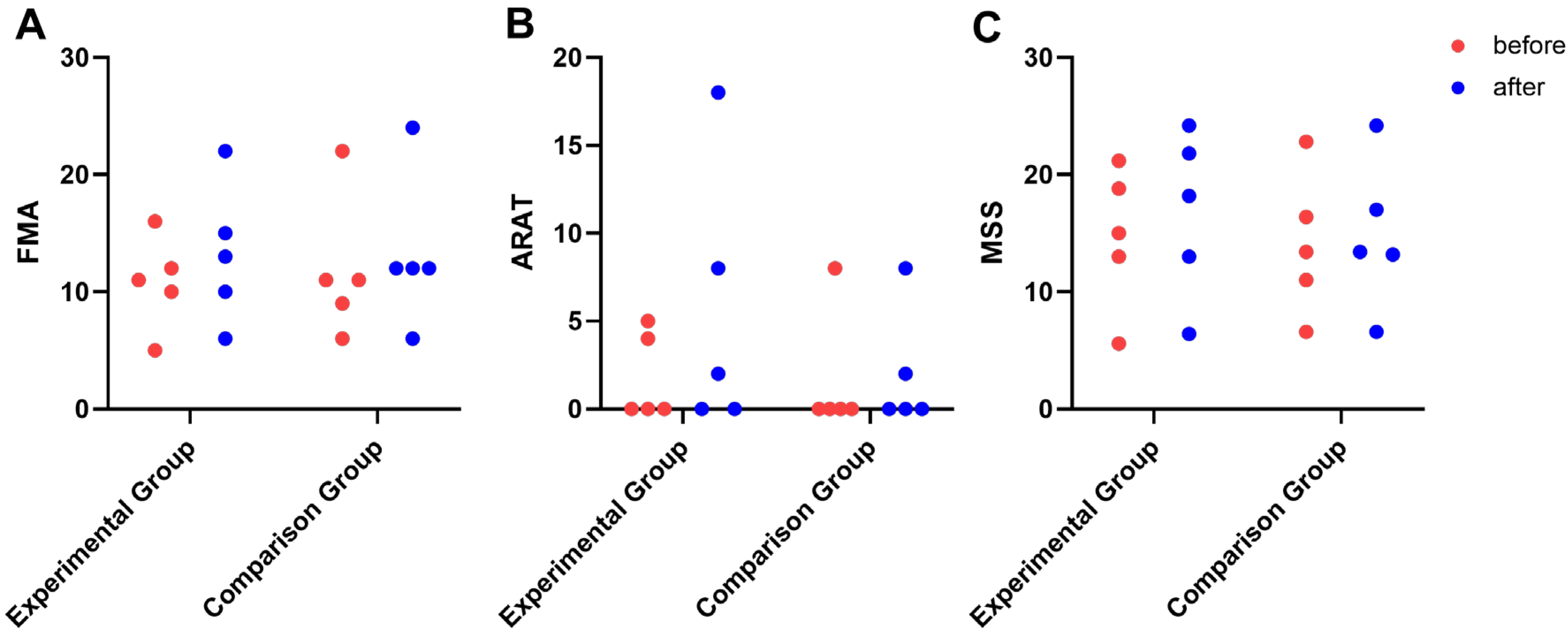
3.3. Behavioural Outcome Metrics
3.4. Commissural Fibres across the Corpus Callosum
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2020 Update: A Report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [PubMed]
- Chen, W.W.; Gao, R.L.; Liu, L.S.; Zhu, M.L.; Wang, W.; Wang, Y.J.; Wu, Z.S.; Li, H.J.; Gu, D.F.; Yang, Y.J. Summary of China Cardiovascular Disease Report 2016. Chin. Circ. J. 2017, 32, 521–530. [Google Scholar]
- Pollock, A.; Farmer, S.E.; Brady, M.C.; Langhorne, P.; Mead, G.E.; Mehrholz, J.; van Wijck, F. Interventions for improving upper limb function after stroke. Cochrane Db Syst Rev. 2014, 2014, CD010820. [Google Scholar] [CrossRef] [PubMed]
- Stinear, C.M.; Lang, C.E.; Zeiler, S.; Byblow, W.D. Advances and challenges in stroke rehabilitation. Lancet Neurol. 2020, 19, 348–360. [Google Scholar] [CrossRef] [PubMed]
- Broeks, J.G.; Lankhorst, G.J.; Rumping, K.; Prevo, A.J. The long-term outcome of arm function after stroke: Results of a follow-up study. Disabil. Rehabil. 1999, 21, 357–364. [Google Scholar] [CrossRef]
- Fitzgerald, P.B.; Fountain, S.; Daskalakis, Z.J. A comprehensive review of the effects of rTMS on motor cortical excitability and inhibition. Clin. Neurophysiol. 2006, 117, 2584–2596. [Google Scholar] [CrossRef]
- Hildesheim, F.E.; Silver, A.N.; Dominguez-Vargas, A.U.; Andrushko, J.W.; Edwards, J.D.; Dancause, N.; Thiel, A. Predicting Individual Treatment Response to rTMS for Motor Recovery After Stroke: A Review and the CanStim Perspective. Front. Rehabil. Sci. 2022, 3, 795335. [Google Scholar] [CrossRef]
- Wang, Q.; Zhang, D.; Zhao, Y.Y.; Hai, H.; Ma, Y.W. Effects of high-frequency repetitive transcranial magnetic stimulation over the contralesional motor cortex on motor recovery in severe hemiplegic stroke: A randomized clinical trial. Brain Stimul. 2020, 13, 979–986. [Google Scholar] [CrossRef]
- Dionisio, A.; Duarte, I.C.; Patricio, M.; Castelo-Branco, M. The Use of Repetitive Transcranial Magnetic Stimulation for Stroke Rehabilitation: A Systematic Review. J. Stroke Cerebrovasc. 2018, 27, 1–31. [Google Scholar] [CrossRef]
- Guo, Z.; Jin, Y.; Bai, X.; Jiang, B.; He, L.; Mcclure, M.A.; Mu, Q. Distinction of High- and Low-Frequency Repetitive Transcranial Magnetic Stimulation on the Functional Reorganization of the Motor Network in Stroke Patients. Neural Plast. 2021, 2021, 8873221. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Li, K.; Chen, Q.; Yin, J.; Bai, D. Repetitive Transcranial Magnetic Stimulation on Motor Recovery for Patients with Stroke: A PRISMA Compliant Systematic Review and Meta-analysis. Am. J. Phys. Med. Rehab. 2020, 99, 99–108. [Google Scholar] [CrossRef]
- Lefaucheur, J.P.; Aleman, A.; Baeken, C.; Benninger, D.H.; Brunelin, J.; Di Lazzaro, V.; Filipovic, S.R.; Grefkes, C.; Hasan, A.; Hummel, F.C.; et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): An update (2014–2018). Clin. Neurophysiol. 2020, 131, 474–528. [Google Scholar] [CrossRef] [PubMed]
- Salehi, D.N.; Kamali, F.; Shariat, A.; Jaberzadeh, S. Comparison of Transcallosal Inhibition Between Hemispheres and Its Relationship with Motor Behavior in Patients with Severe Upper Extremity Impairment After Subacute Stroke. J. Stroke Cerebrovasc. 2022, 31, 106469. [Google Scholar] [CrossRef] [PubMed]
- Di Pino, G.; Pellegrino, G.; Assenza, G.; Capone, F.; Ferreri, F.; Formica, D.; Ranieri, F.; Tombini, M.; Ziemann, U.; Rothwell, J.C.; et al. Modulation of brain plasticity in stroke: A novel model for neurorehabilitation. Nat. Rev. Neurol. 2014, 10, 597–608. [Google Scholar] [CrossRef]
- Lin, Y.L.; Potter-Baker, K.A.; Cunningham, D.A.; Li, M.; Sankarasubramanian, V.; Lee, J.; Jones, S.; Sakaie, K.; Wang, X.; Machado, A.G.; et al. Stratifying chronic stroke patients based on the influence of contralesional motor cortices: An inter-hemispheric inhibition study. Clin. Neurophysiol. 2020, 131, 2516–2525. [Google Scholar] [CrossRef] [PubMed]
- Ietswaart, M.; Johnston, M.; Dijkerman, H.C.; Joice, S.; Scott, C.L.; Macwalter, R.S.; Hamilton, S.J. Mental practice with motor imagery in stroke recovery: Randomized controlled trial of efficacy. Brain 2011, 134, 1373–1386. [Google Scholar] [CrossRef]
- Decety, J. Neural representations for action. Rev. Neurosci. 1996, 7, 285–297. [Google Scholar] [CrossRef] [PubMed]
- Decety, J.; Jeannerod, M.; Prablanc, C. The timing of mentally represented actions. Behav. Brain Res. 1989, 34, 35–42. [Google Scholar] [CrossRef]
- Hu, Y.Q.; Gao, T.H.; Li, J.; Tao, J.C.; Bai, Y.L.; Lu, R.R. Motor Imagery-Based Brain-Computer Interface Combined with Multimodal Feedback to Promote Upper Limb Motor Function after Stroke: A Preliminary Study. Evid.-Based Compl. Alt. 2021, 2021, 1116126. [Google Scholar] [CrossRef]
- Lu, R.R.; Zheng, M.X.; Li, J.; Gao, T.H.; Hua, X.Y.; Liu, G.; Huang, S.H.; Xu, J.G.; Wu, Y. Motor imagery based brain-computer interface control of continuous passive motion for wrist extension recovery in chronic stroke patients. Neurosci. Lett. 2020, 718, 134727. [Google Scholar] [CrossRef]
- Tzourio-Mazoyer, N.; Landeau, B.; Papathanassiou, D.; Crivello, F.; Etard, O.; Delcroix, N.; Mazoyer, B.; Joliot, M. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage 2002, 15, 273–289. [Google Scholar] [CrossRef] [PubMed]
- Groppa, S.; Oliviero, A.; Eisen, A.; Quartarone, A.; Cohen, L.G.; Mall, V.; Kaelin-Lang, A.; Mima, T.; Rossi, S.; Thickbroom, G.W.; et al. A practical guide to diagnostic transcranial magnetic stimulation: Report of an IFCN committee. Clin. Neurophysiol. 2012, 123, 858–882. [Google Scholar] [CrossRef] [Green Version]
- Ferraro, M.; Demaio, J.H.; Krol, J.; Trudell, C.; Rannekleiv, K.; Edelstein, L.; Christos, P.; Aisen, M.; England, J.; Fasoli, S.; et al. Assessing the motor status score: A scale for the evaluation of upper limb motor outcomes in patients after stroke. Neurorehab. Neural Repair 2002, 16, 283–289. [Google Scholar] [CrossRef]
- van der Knaap, L.J.; van der Ham, I.J. How does the corpus callosum mediate interhemispheric transfer? A review. Behav. Brain Res. 2011, 223, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.C.; Dewanjee, P.; Tran, G.; Quinlan, E.B.; Dodakian, L.; Mckenzie, A.; See, J.; Cramer, S.C. Role of corpus callosum integrity in arm function differs based on motor severity after stroke. Neuroimage Clin. 2017, 14, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.C.; O’Donnell, M.; Handlery, K.; Winstein, C.J. Skilled Reach Performance Correlates with Corpus Callosum Structural Integrity in Individuals with Mild Motor Impairment After Stroke: A Preliminary Investigation. Neurorehab. Neural Repair 2017, 31, 657–665. [Google Scholar] [CrossRef] [Green Version]
- Wahl, M.; Lauterbach-Soon, B.; Hattingen, E.; Jung, P.; Singer, O.; Volz, S.; Klein, J.C.; Steinmetz, H.; Ziemann, U. Human motor corpus callosum: Topography, somatotopy, and link between microstructure and function. J. Neurosci. 2007, 27, 12132–12138. [Google Scholar] [CrossRef] [Green Version]
- Malouin, F.; Richards, C.L.; Jackson, P.L.; Lafleur, M.F.; Durand, A.; Doyon, J. The Kinesthetic and Visual Imagery Questionnaire (KVIQ) for assessing motor imagery in persons with physical disabilities: A reliability and construct validity study. J. Neurol. Phys. Ther. 2007, 31, 20–29. [Google Scholar] [CrossRef]
- Veerbeek, J.M.; van Wegen, E.; van Peppen, R.; van der Wees, P.J.; Hendriks, E.; Rietberg, M.; Kwakkel, G. What is the evidence for physical therapy poststroke? A systematic review and meta-analysis. PLoS ONE 2014, 9, e87987. [Google Scholar]
- Dimyan, M.A.; Cohen, L.G. Neuroplasticity in the context of motor rehabilitation after stroke. Nat. Rev. Neurol. 2011, 7, 76–85. [Google Scholar] [CrossRef]
- Rossi, S.; Hallett, M.; Rossini, P.M.; Pascual-Leone, A. Safety, ethical considerations, and application guidelines for the use of transcranial magnetic stimulation in clinical practice and research. Clin. Neurophysiol. 2009, 120, 2008–2039. [Google Scholar] [CrossRef]
- Corti, M.; Patten, C.; Triggs, W. Repetitive transcranial magnetic stimulation of motor cortex after stroke: A focused review. Am. J. Phys. Med. Rehab. 2012, 91, 254–270. [Google Scholar] [CrossRef] [Green Version]
- Harvey, R.L.; Edwards, D.; Dunning, K.; Fregni, F.; Stein, J.; Laine, J.; Rogers, L.M.; Vox, F.; Durand-Sanchez, A.; Bockbrader, M.; et al. Randomized Sham-Controlled Trial of Navigated Repetitive Transcranial Magnetic Stimulation for Motor Recovery in Stroke. Stroke 2018, 49, 2138–2146. [Google Scholar] [CrossRef]
- Li, X.; Lin, Y.L.; Cunningham, D.A.; Wolf, S.L.; Sakaie, K.; Conforto, A.B.; Machado, A.G.; Mohan, A.; O’Laughlin, K.; Wang, X.; et al. Repetitive Transcranial Magnetic Stimulation of the Contralesional Dorsal Premotor Cortex for Upper Extremity Motor Improvement in Severe Stroke: Study Protocol for a Pilot Randomized Clinical Trial. Cerebrovasc. Dis. 2022, 51, 557–564. [Google Scholar] [CrossRef]
- Chang, P.W.; Lu, C.F.; Chang, S.T.; Tsai, P.Y. Functional Near-Infrared Spectroscopy as a Target Navigator for rTMS Modulation in Patients with Hemiplegia: A Randomized Control Study. Neurol. Ther. 2022, 11, 103–121. [Google Scholar] [CrossRef]
- Ward, N.S. Mechanisms underlying recovery of motor function after stroke. Postgrad. Med. J. 2005, 81, 510–514. [Google Scholar] [CrossRef] [Green Version]
- Pundik, S.; Mccabe, J.P.; Hrovat, K.; Fredrickson, A.E.; Tatsuoka, C.; Feng, I.J.; Daly, J.J. Recovery of post stroke proximal arm function, driven by complex neuroplastic bilateral brain activation patterns and predicted by baseline motor dysfunction severity. Front. Hum. Neurosci. 2015, 9, 394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferbert, A.; Priori, A.; Rothwell, J.C.; Day, B.L.; Colebatch, J.G.; Marsden, C.D. Interhemispheric inhibition of the human motor cortex. J. Physiol. 1992, 453, 525–546. [Google Scholar] [CrossRef] [PubMed]
- Fling, B.W.; Benson, B.L.; Seidler, R.D. Transcallosal sensorimotor fiber tract structure-function relationships. Hum. Brain Mapp. 2013, 34, 384–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grefkes, C.; Nowak, D.A.; Eickhoff, S.B.; Dafotakis, M.; Kust, J.; Karbe, H.; Fink, G.R. Cortical connectivity after subcortical stroke assessed with functional magnetic resonance imaging. Ann. Neurol. 2008, 63, 236–246. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Participant | Group | Sex | Age (y) | Diagnosis | Affected UE | Post-Stroke Duration (mo) |
|---|---|---|---|---|---|---|
| 1 | Experimental | M | 43 | Haemorrhagic | Left | 8 |
| 2 | Experimental | M | 68 | Ischaemic | Left | 16 |
| 3 | Experimental | M | 42 | Haemorrhagic | Left | 20 |
| 4 | Experimental | M | 75 | Ischaemic | Left | 6 |
| 5 | Experimental | F | 58 | Haemorrhagic | Right | 7 |
| 6 | Comparison | M | 65 | Haemorrhagic | Left | 11 |
| 7 | Comparison | M | 32 | Haemorrhagic | Left | 6 |
| 8 | Comparison | M | 56 | Ischaemic | Right | 8 |
| 9 | Comparison | M | 66 | Ischaemic | Left | 7 |
| 10 | Comparison | M | 41 | Haemorrhagic | Left | 20 |
| Affected Hemisphere | Activated Brain Regions in fMRI | Activated Brain Regions Converted According to 10–20 International System | Activated Brain Regions | |
|---|---|---|---|---|
| Participant 1 | Right | Mainly in the right premotor cortex (BA 6) and precentral gyrus (M1, BA 4) | FC4 |  |
| Participant 2 | Left | Mainly in the right precentral gyrus (M1, BA 4), premotor cortex, and supplementary motor cortex (SMA, BA 6) | C2 |  |
| Participant 3 | Right | Mainly in the left precentral gyrus (M1, BA 4) and premotor cortex (BA 6) | C3 |  |
| Participant 4 | Right | Mainly in the left precentral gyrus (M1, BA 4) and premotor cortex (BA 6) | C1 |  |
| Participant 5 | Right | Mainly in the right precentral gyrus (M1, BA 4) and premotor cortex (BA 6) | C1 |  |
| Participant | Group | Pre MSS | Post MSS | Pre FMA | Post FMA | Pre ARAT | Post ARAT | Pre AROM Flexion | Post AROM Flexion | Pre AROM Extension | Post AROM Extension |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Experimental | 18.80 | 21.80 | 12.00 | 15.00 | 4.00 | 18.00 | 0° | 0° | 0° | 0° |
| 2 | Experimental | 13.00 | 13.00 | 10.00 | 10.00 | 0.00 | 0.00 | 0° | 0° | 0° | 0° |
| 3 | Experimental | 15.00 | 18.20 | 11.00 | 13.00 | 0.00 | 2.00 | 0° | 20° | 0° | 0° |
| 4 | Experimental | 21.20 | 24.20 | 16.00 | 22.00 | 5.00 | 8.00 | 0° | 60° | 0° | 25° |
| 5 | Experimental | 5.60 | 6.40 | 5.00 | 6.00 | 0.00 | 0.00 | 0° | 0° | 0° | 0° |
| 6 | Comparison | 16.40 | 17.00 | 11.00 | 12.00 | 0.00 | 0.00 | 0° | 20° | 0° | 0° |
| 7 | Comparison | 22.80 | 24.20 | 22.00 | 24.00 | 8.00 | 8.00 | 0° | 10° | 0° | 20° |
| 8 | Comparison | 11.00 | 13.20 | 9.00 | 12.00 | 0.00 | 2.00 | 0° | 0° | 0° | 0° |
| 9 | Comparison | 6.60 | 6.60 | 6.00 | 6.00 | 0.00 | 0.00 | 0° | 0° | 0° | 0° |
| 10 | Comparison | 13.40 | 13.40 | 11.00 | 12.00 | 0.00 | 0.00 | 0° | 0° | 0° | 0° |
| Experimental Group | Comparison Group | ||||||
|---|---|---|---|---|---|---|---|
| Baseline | Post rTMS | Baseline | Post rTMS | Sig. a | Sig. b | Sig. c | |
| FA | 0.53 ± 0.05 | 0.56 ± 0.06 | 0.55 ± 0.04 | 0.56 ± 0.06 | 0.059 | 0.828 | 0.909 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, T.; Hu, Y.; Zhuang, J.; Bai, Y.; Lu, R. Repetitive Transcranial Magnetic Stimulation of the Brain Region Activated by Motor Imagery Involving a Paretic Wrist and Hand for Upper-Extremity Motor Improvement in Severe Stroke: A Preliminary Study. Brain Sci. 2023, 13, 69. https://doi.org/10.3390/brainsci13010069
Gao T, Hu Y, Zhuang J, Bai Y, Lu R. Repetitive Transcranial Magnetic Stimulation of the Brain Region Activated by Motor Imagery Involving a Paretic Wrist and Hand for Upper-Extremity Motor Improvement in Severe Stroke: A Preliminary Study. Brain Sciences. 2023; 13(1):69. https://doi.org/10.3390/brainsci13010069
Chicago/Turabian StyleGao, Tianhao, Yiqian Hu, Jie Zhuang, Yulong Bai, and Rongrong Lu. 2023. "Repetitive Transcranial Magnetic Stimulation of the Brain Region Activated by Motor Imagery Involving a Paretic Wrist and Hand for Upper-Extremity Motor Improvement in Severe Stroke: A Preliminary Study" Brain Sciences 13, no. 1: 69. https://doi.org/10.3390/brainsci13010069