

Alterations in Corticocortical Vestibular Network Functional Connectivity Are Associated with Decreased Balance Ability in Elderly Individuals with Mild Cognitive Impairment
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Balance Ability Assessment
2.3. Functional Magnetic Resonance Imaging Acquisition
2.4. Functional Network Construction
2.5. Statistical Analysis
3. Results
3.1. Subject Characteristics
3.2. Function Connection Analysis Results
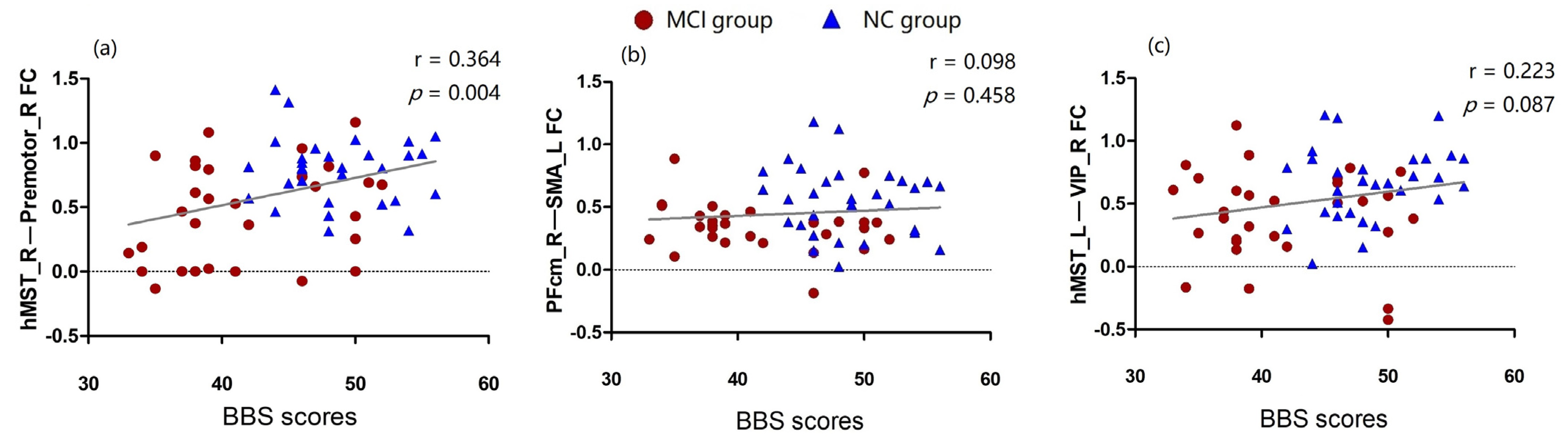
3.3. Correlation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Abbreviations | Full Name |
| MCI | Mild Cognitive Impairment |
| NC | Normal Cognitive Control |
| CVN | Corticocortical Vestibular Network |
| BBS | Berg Balance Scale |
| MoCA | Montreal Cognitive Assessment |
| MRI | Magnetic Resonance Imaging |
| ROI | Region Of Interest |
| CSv | Cingulate Sulcus Visual |
| VIP | Ventral Intraparietal Area |
| MNI | Montreal Neurological Institute |
| FDR | False Discovery Rate Corrected |
| SMA | Supplementary Motor Area |
| hMST | Human Medial Superior Temporal Area |
| PF | Prefrontal Cortex |
| PFcm | Medial Prefrontal Cortex |
| VPS | Visual Posterior Sylvian Area |
| ECG | Electrocardiogram |
| SD | Standard Deviation |
References
- Tinetti, M.E.; Speechley, M.; Ginter, S.F. Risk factors for falls among elderly persons living in the community. N. Engl. J. Med. 1988, 319, 1701–1707. [Google Scholar] [CrossRef] [PubMed]
- Bergen, G.; Stevens, M.R.; Burns, E.R. Falls and Fall Injuries Among Adults Aged ≥65 Years—United States, 2014. Morb. Mortal. Wkly. Rep. 2016, 65, 993–998. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Falls in Older People: Assessing Risk and Prevention (NICE Clinical Guideline 161). 2013. Available online: www.nice.org.uk/guidance/cg161 (accessed on 1 September 2022).
- Yardley, L.; Smith, H. A prospective study of the relationship between feared consequences of falling and avoidance of activity in community-living older people. Gerontologist 2002, 42, 17–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delbaere, K.; Crombez, G.; Vanderstraeten, G.; Willems, T.; Cambier, D. Fear-related avoidance of activities, falls and physical frailty. A prospective community-based cohort study. Age Ageing 2004, 33, 368–373. [Google Scholar] [CrossRef] [Green Version]
- Lach, H.W.; Harrison, B.E.; Phongphanngam, S. Falls and Fall Prevention in Older Adults with Early-Stage Dementia: An Integrative Review. Res. Gerontol. Nurs. 2017, 10, 139–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansai, J.H.; Andrade, L.P.; Masse, F.; Gonçalves, J.; Takahashi, A.; Vale, F.; Rebelatto, J.R. Risk Factors for Falls in Older Adults with Mild Cognitive Impairment and Mild Alzheimer Disease. J. Geriatr. Phys. Ther. 2019, 42, E116–E121. [Google Scholar] [CrossRef]
- Van Dijk, P.T.; Meulenberg, O.G.; van de Sande, H.J.; Habbema, J.D. Falls in dementia patients. Gerontologist 1993, 33, 200–204. [Google Scholar] [CrossRef]
- Delbaere, K.; Kochan, N.A.; Close, J.C.; Menant, J.C.; Sturnieks, D.L.; Brodaty, H.; Sachdev, P.S.; Lord, S.R. Mild cognitive impairment as a predictor of falls in community-dwelling older people. Am. J. Geriatr. Psychiatry 2012, 20, 845–853. [Google Scholar] [CrossRef]
- Tyrovolas, S.; Koyanagi, A.; Lara, E.; Santini, Z.I.; Haro, J.M. Mild cognitive impairment is associated with falls among older adults: Findings from the Irish Longitudinal Study on Ageing (TILDA). Exp. Gerontol. 2016, 75, 42–47. [Google Scholar] [CrossRef]
- Mitchell, R.; Draper, B.; Brodaty, H.; Close, J.; Ting, H.P.; Lystad, R.; Harris, I.; Harvey, L.; Sherrington, C.; Cameron, I.D.; et al. An 11-year review of hip fracture hospitalisations, health outcomes, and predictors of access to in-hospital rehabilitation for adults ≥ 65 years living with and without dementia: A population-based cohort study. Osteoporos. Int. 2020, 31, 465–474. [Google Scholar] [CrossRef]
- Yoon, B.; Choi, S.H.; Jeong, J.H.; Park, K.W.; Kim, E.J.; Hwang, J.; Jang, J.; Kim, J.H.; Hong, J.Y.; Lee, J.; et al. Balance and Mobility Performance Along the Alzheimer’s Disease Spectrum. J. Alzheimers Dis. 2020, 73, 633–644. [Google Scholar] [CrossRef] [PubMed]
- Kuan, Y.C.; Huang, L.K.; Wang, Y.H.; Hu, C.J.; Tseng, I.J.; Chen, H.C.; Lin, L.F. Balance and gait performance in older adults with early-stage cognitive impairment. Eur. J. Phys. Rehabil. Med. 2021, 57, 560–567. [Google Scholar] [CrossRef] [PubMed]
- Cronin, T.; Arshad, Q.; Seemungal, B.M. Vestibular Deficits in Neurodegenerative Disorders: Balance, Dizziness, and Spatial Disorientation. Front. Neurol. 2017, 8, 538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noohi, F.; Kinnaird, C.; De Dios, Y.; Kofman, I.S.; Wood, S.J.; Bloomberg, J.; Mulavara, A.; Sienko, K.H.; Polk, T.A.; Seidler, R.D. Age Differences in Vestibular Brain Connectivity Are Associated With Balance Performance. Front. Aging Neurosci. 2020, 12, 566331. [Google Scholar] [CrossRef] [PubMed]
- Stiles, L.; Smith, P.F. The vestibular-basal ganglia connection: Balancing motor control. Brain Res. 2015, 1597, 180–188. [Google Scholar] [CrossRef]
- Atomi, T.; Noriuchi, M.; Oba, K.; Atomi, Y.; Kikuchi, Y. Self-recognition of one’s own fall recruits the genuine bodily crisis-related brain activity. PLoS ONE 2014, 9, e115303. [Google Scholar] [CrossRef] [Green Version]
- Cullen, K.E. The vestibular system: Multimodal integration and encoding of self-motion for motor control. Trends Neurosci. 2012, 35, 185–196. [Google Scholar] [CrossRef] [Green Version]
- Malcolm, B.R.; Foxe, J.J.; Butler, J.S.; De Sanctis, P. The aging brain shows less flexible reallocation of cognitive resources during dual-task walking: A mobile brain/body imaging (MoBI) study. NeuroImage 2015, 117, 230–242. [Google Scholar] [CrossRef] [Green Version]
- Makizako, H.; Shimada, H.; Doi, T.; Park, H.; Yoshida, D.; Uemura, K.; Tsutsumimoto, K.; Liu-Ambrose, T.; Suzuki, T. Poor balance and lower gray matter volume predict falls in older adults with mild cognitive impairment. BMC Neurol. 2013, 13, 102. [Google Scholar] [CrossRef] [Green Version]
- Ide, R.; Ota, M.; Hada, Y.; Watanabe, S.; Takahashi, T.; Tamura, M.; Nemoto, K.; Arai, T. Dynamic balance deficit and the neural network in Alzheimer’s disease and mild cognitive impairment. Gait. Postur. 2022, 93, 252–258. [Google Scholar] [CrossRef]
- Seidler, R.D.; Bernard, J.A.; Burutolu, T.B.; Fling, B.W.; Gordon, M.T.; Gwin, J.T.; Kwak, Y.; Lipps, D.B. Motor control and aging: Links to age-related brain structural, functional, and biochemical effects. Neurosci. Biobehav. Rev. 2010, 34, 721–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, R.C. Mild cognitive impairment as a diagnostic entity. J. Intern. Med. 2004, 256, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Berg, K.O.; Maki, B.E.; Williams, J.I.; Holliday, P.J.; Wood-Dauphinee, S.L. Clinical and laboratory measures of postural balance in an elderly population. Arch. Phys. Med. Rehabil. 1992, 73, 1073–1080. [Google Scholar] [PubMed]
- Fang, T.C.; Chen, C.M.; Chang, M.H.; Wu, C.H.; Guo, Y.J. Altered Functional Connectivity and Sensory Processing in Blepharospasm and Hemifacial Spasm: Coexistence and Difference. Front. Neurol. 2021, 12, 759869. [Google Scholar] [CrossRef] [PubMed]
- Raiser, T.M.; Flanagin, V.L.; Duering, M.; van Ombergen, A.; Ruehl, R.M.; Zu Eulenburg, P. The human corticocortical vestibular network. NeuroImage 2020, 223, 117362. [Google Scholar] [CrossRef]
- Grüsser, O.J.; Pause, M.; Schreiter, U. Localization and responses of neurons in the parieto-insular vestibular cortex of awake monkeys (Macaca fascicularis). J. Physiol. 1990, 430, 537–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grüsser, O.J.; Pause, M.; Schreiter, U. Vestibular neurons in the Parieto-insular cortex of monkeys (Macaca fascicularis): Visual and neck receptor responses. J. Physiol. 1990, 430, 559–583. [Google Scholar] [CrossRef] [Green Version]
- Schaafsma, S.J.; Duysens, J. Neurons in the ventral intraparietal area of awake macaque monkey closely resemble neurons in the dorsal part of the medial superior temporal area in responses to optic flow patterns. J. Neurophysiol. 1996, 76, 4056–4068. [Google Scholar] [CrossRef] [Green Version]
- Gu, Y.; Watkins, P.V.; Angelaki, D.E.; DeAngelis, G.C. Visual and nonvisual contributions to three-dimensional heading selectivity in the medial superior temporal area. J. Neurosci. 2006, 26, 73–85. [Google Scholar] [CrossRef] [Green Version]
- Gu, Y.; Angelaki, D.E.; Deangelis, G.C. Neural correlates of multisensory cue integration in macaque MSTd. Nat. Neurosci. 2008, 11, 1201–1210. [Google Scholar] [CrossRef]
- Gu, Y.; Deangelis, G.C.; Angelaki, D.E. Causal links between dorsal medial superior temporal area neurons and multisensory heading perception. J. Neurosci. 2012, 32, 2299–2313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wild, B.; Treue, S. Primate extrastriate cortical area MST: A gateway between sensation and cognition. J. Neurophysiol. 2021, 125, 1851–1882. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, C.; Baltaretu, B.R.; Crawford, J.D.; Bremmer, F. A Causal Role of Area hMST for Self-Motion Perception in Humans. Cereb. Cortex Commun. 2020, 1, tgaa042. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, Y.; Sugawara, S.K.; Fukunaga, M.; Hamano, Y.H.; Sadato, N.; Nishimura, Y. The dorsal premotor cortex encodes the step-by-step planning processes for goal-directed motor behavior in humans. NeuroImage 2022, 256, 119221. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.; DeAngelis, G.C.; Angelaki, D.E. Representation of vestibular and visual cues to self-motion in ventral intraparietal cortex. J. Neurosci. 2011, 31, 12036–12052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Li, S.; Jiang, D.; Chen, A. Response Properties of Interneurons and Pyramidal Neurons in Macaque MSTd and VPS Areas During Self-Motion. Front. Neural Circuits 2018, 12, 105. [Google Scholar] [CrossRef] [PubMed]
- Welniarz, Q.; Gallea, C.; Lamy, J.C.; Méneret, A.; Popa, T.; Valabregue, R.; Béranger, B.; Brochard, V.; Flamand-Roze, C.; Trouillard, O.; et al. The supplementary motor area modulates interhemispheric interactions during movement preparation. Hum. Brain Mapp. 2019, 40, 2125–2142. [Google Scholar] [CrossRef] [Green Version]
- Lima, C.F.; Krishnan, S.; Scott, S.K. Roles of Supplementary Motor Areas in Auditory Processing and Auditory Imagery. Trends Neurosci. 2016, 39, 527–542. [Google Scholar] [CrossRef] [Green Version]
- Bremmer, F.; Klam, F.; Duhamel, J.R.; Ben Hamed, S.; Graf, W. Visual-vestibular interactive responses in primate ventral intraparietal area (VIP). Eur. J. Neurosci. 2002, 16, 1569–1586. [Google Scholar] [CrossRef]
- Bremmer, F.; Duhamel, J.R.; Ben Hamed, S.; Graf, W. Heading encoding in the macaque ventral intraparietal area (VIP). Eur. J. Neurosci. 2002, 16, 1554–1568. [Google Scholar] [CrossRef]
- Schlack, A.; Hoffmann, K.P.; Bremmer, F. Interaction of linear vestibular and visual stimulation in the macaque ventral intraparietal area (VIP). Eur. J. Neurosci. 2022, 16, 1877–1886. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.; Gu, Y.; Liu, S.; DeAngelis, G.C.; Angelaki, D.E. Evidence for a Causal Contribution of Macaque Vestibular, But Not Intraparietal, Cortex to Heading Perception. J. Neurosci. 2016, 36, 3789–3798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurata, K. Movement-related activity in the periarcuate cortex of monkeys during coordinated eye and hand movements. J. Neurophysiol. 2017, 118, 3293–3310. [Google Scholar] [CrossRef] [Green Version]
- Cardin, V.; Smith, A.T. Sensitivity of human visual and vestibular cortical regions to egomotion-compatible visual stimulation. Cereb. Cortex. 2010, 20, 1964–1973. [Google Scholar] [CrossRef] [Green Version]
- Cardin, V.; Smith, A.T. Sensitivity of human visual cortical area V6 to stereoscopic depth gradients associated with self-motion. J. Neurophysiol. 2011, 106, 1240–1249. [Google Scholar] [CrossRef] [Green Version]
- Kosse, N.M.; De Groot, M.H.; Vuillerme, N.; Hortobágyi, T.; Lamoth, C.J.C. Factors related to the high fall rate in long-term care residents with dementia. Int. Psychogeriatr. 2015, 27, 803–814. [Google Scholar] [CrossRef] [PubMed]
- Allum, J.H.J. Recovery of vestibular ocular reflex function and balance control after a unilateral peripheral vestibular deficit. Front. Neurol. 2012, 3, 83. [Google Scholar] [CrossRef] [Green Version]
- Peterka, R.J. Sensorimotor integration in human postural control. J. Neurophysiol. 2002, 88, 1097–1118. [Google Scholar] [CrossRef] [Green Version]
- Agrawal, Y.; Carey, J.P.; Della Santina, C.C.; Schubert, M.C.; Minor, L.B. Disorders of balance and vestibular function in US adults: Data from the National Health and Nutrition Examination Survey, 2001–2004. Arch. Intern. Med. 2009, 169, 938–944. [Google Scholar] [CrossRef]
- Whitney, S.L.; Marchetti, G.F.; Pritcher, M.; Furman, J.M. Gaze stabilization and gait performance in vestibular dysfunction. Gait. Postur. 2009, 29, 194–198. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | MCI (N = 30) | NC (N = 30) | χ2/t Value | p-Value |
|---|---|---|---|---|
| Sex (M/F) | 14/16 | 16/14 | 0.267 | 0.606 |
| Age (years): mean ± SD | 66.73 ± 5.20 | 67.50 ± 5.67 | −0.546 | 0.587 |
| Education level (years): Mean ± SD | 9.53 ± 2.80 | 9.40 ± 2.58 | 0.192 | 0.849 |
| MoCA (scores): mean ± SD | 21.13 ± 2.46 | 27.60 ± 1.28 | −12.782 | <0.001 |
| BBS (scores): mean ± SD | 41.70 ± 5.93 | 48.67 ± 4.16 | −5.269 | <0.001 |
| Compare | Analysis Unit | T | p-unc | p-FDR | |
|---|---|---|---|---|---|
| Seed | Target | ||||
| NC < MCI | Left periarcuate/SMA | Right Area 2V | −2.68 | 0.009524 | 0.079966 |
| Left hMST | Left Area 6/premotor | −2.61 | 0.011444 | 0.072479 | |
| NC > MCI | Right hMST | Right Area 6/premotor | 3.85 | 0.000300 | 0.005707 * |
| Right hMST | Left PF/area 7 | 2.57 | 0.012911 | 0.122658 | |
| Right hMST | Right CSv | 2.28 | 0.026072 | 0.165124 | |
| Right PFcm/VPS | Left periarcuate/SMA | 3.26 | 0.001883 | 0.035785 * | |
| Right PFcm/VPS | Left VIP | 2.05 | 0.044867 | 0.275219 | |
| Left periarcuate/SMA | Right PF/area 7 | 2.57 | 0.012626 | 0.079823 | |
| Left PF/area 7 | Right PF/area 7 | 2.36 | 0.021922 | 0.164857 | |
| Left PF/area 7 | Left hMST | 2.26 | 0.027363 | 0.103979 | |
| Left PF/area 7 | Right periarcuate/SMA | 2.16 | 0.034707 | 0.164876 | |
| Left hMST | Right VIP | 3.00 | 0.003958 | 0.048749 * | |
| Left hMST | Left VIP | 2.91 | 0.005131 | 0.097498 | |
| Left hMST | Left area 2V | 2.43 | 0.018107 | 0.086009 | |
| Right VIP | Left PFcm/VPS | 2.52 | 0.014564 | 0.113398 | |
| Right VIP | Right periarcuate/SMA | 2.44 | 0.017905 | 0.125867 | |
| Right VIP | Right CSv | 2.16 | 0.034913 | 0.165835 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xia, R.; Ren, J.; Li, X.; Liu, J.; Dai, Y.; Kuang, Y.; Wu, Z.; Chen, S. Alterations in Corticocortical Vestibular Network Functional Connectivity Are Associated with Decreased Balance Ability in Elderly Individuals with Mild Cognitive Impairment. Brain Sci. 2023, 13, 63. https://doi.org/10.3390/brainsci13010063
Xia R, Ren J, Li X, Liu J, Dai Y, Kuang Y, Wu Z, Chen S. Alterations in Corticocortical Vestibular Network Functional Connectivity Are Associated with Decreased Balance Ability in Elderly Individuals with Mild Cognitive Impairment. Brain Sciences. 2023; 13(1):63. https://doi.org/10.3390/brainsci13010063
Chicago/Turabian StyleXia, Rui, Jinxin Ren, Xingjie Li, Jun Liu, Yalan Dai, Yuxing Kuang, Zhuguo Wu, and Shangjie Chen. 2023. "Alterations in Corticocortical Vestibular Network Functional Connectivity Are Associated with Decreased Balance Ability in Elderly Individuals with Mild Cognitive Impairment" Brain Sciences 13, no. 1: 63. https://doi.org/10.3390/brainsci13010063