
Contingency Management for Treatment of Cannabis Use Disorder in Co-Occurring Mental Health Disorders: A Systematic Review

Abstract
:1. Introduction
2. Methods
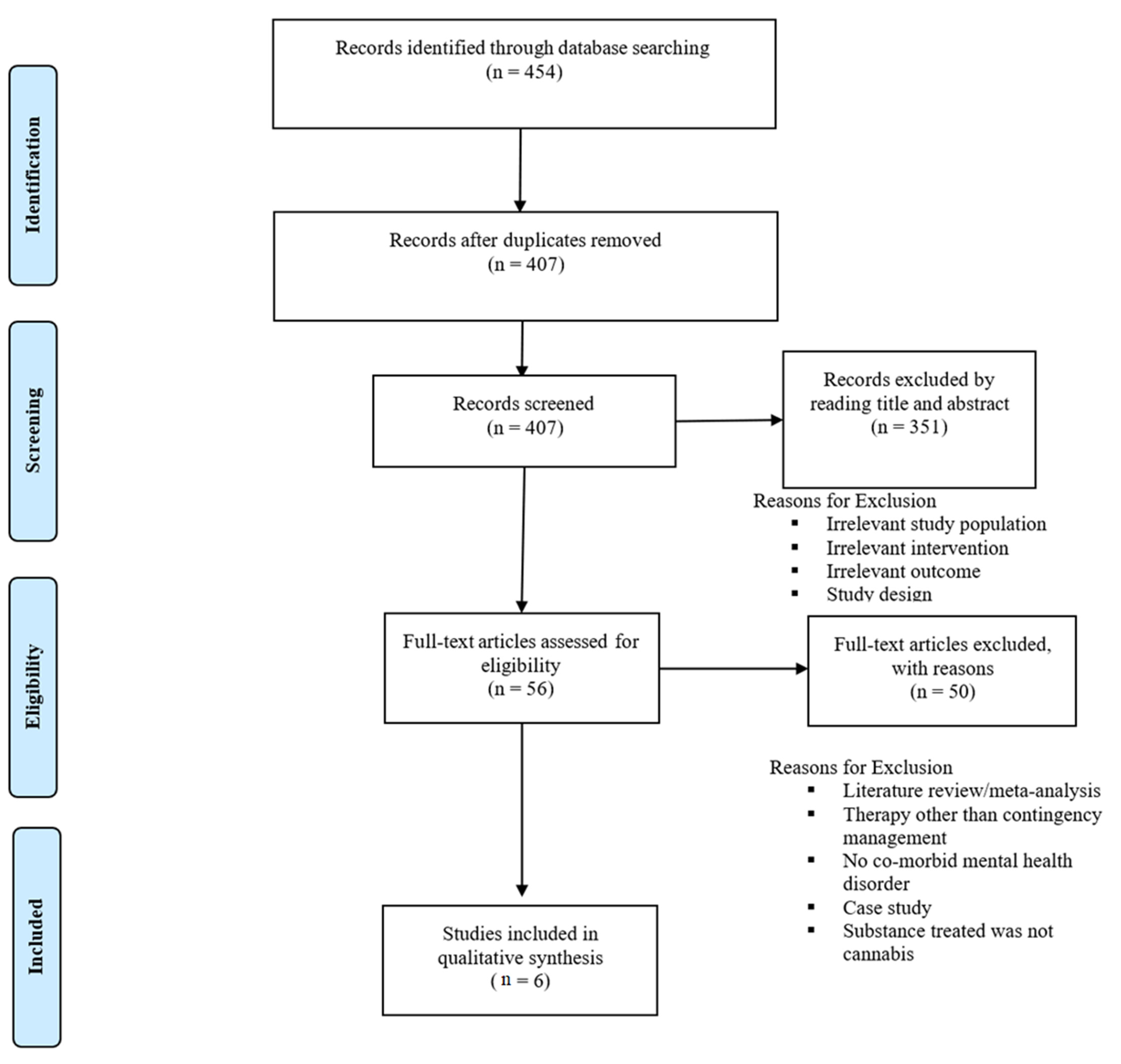
2.1. Search Strategy and Selection Criteria
2.2. Data Extraction and Risk of Bias
3. Results
3.1. Study Characteristics
3.2. Schizophrenia and Schizoaffective Disorder
3.3. Major Depressive Disorder (MDD)
4. Discussion
5. Strengths and Limitations
6. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations: Office on Drugs and Crime. World Drug Report 2021. Available online: www.unodc.org/unodc/en/data-and-analysis/wdr2021.html (accessed on 20 November 2022).
- Hasin, D.S.; Kerridge, B.T.; Saha, T.D.; Huang, B.; Pickering, R.; Smith, S.M.; Jung, J.; Zhang, H.; Grant, B.F. Prevalence and Correlates of DSM-5 Cannabis Use Disorder, 2012–2013: Findings from the National Epidemiologic Survey on Alcohol and Related Conditions-III. Am. J. Psychiatry 2016, 173, 588–599. [Google Scholar] [CrossRef] [PubMed]
- Lai, H.M.X.; Sitharthan, T. Exploration of the Comorbidity of Cannabis Use Disorders and Mental Health Disorders among Inpatients Presenting to All Hospitals in New South Wales, Australia. Am. J. Drug Alcohol Abus. 2012, 38, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Hasin, D.; Walsh, C. Cannabis Use, Cannabis Use Disorder, and Comorbid Psychiatric Illness: A Narrative Review. J. Clin. Med. 2020, 10, 15. [Google Scholar] [CrossRef] [PubMed]
- Lev-Ran, S.; Le Foll, B.; McKenzie, K.; George, T.P.; Rehm, J. Cannabis Use and Cannabis Use Disorders among Individuals with Mental Illness. Compr. Psychiatry 2013, 54, 589–598. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Wu, L.-T. Sex Differences in Cannabis Use Disorder Diagnosis Involved Hospitalizations in the United States. J. Addict. Med. 2017, 11, 357–367. [Google Scholar] [CrossRef]
- Gorelick, D.A. Psychiatric Comorbidity of Cannabis Use Disorder. In Cannabis Use Disorders; Montoya, I.D., Weiss, S.R.B., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 113–125. [Google Scholar] [CrossRef]
- Bahorik, A.L.; Leibowitz, A.; Sterling, S.A.; Travis, A.; Weisner, C.; Satre, D.D. Patterns of Marijuana Use among Psychiatry Patients with Depression and Its Impact on Recovery. J. Affect. Disord. 2017, 213, 168–171. [Google Scholar] [CrossRef] [Green Version]
- Bricker, J.B.; Russo, J.; Stein, M.B.; Sherbourne, C.; Craske, M.; Schraufnagel, T.J.; Roy-Byrne, P. Does Occasional Cannabis Use Impact Anxiety and Depression Treatment Outcomes?: Results from a Randomized Effectiveness Trial. Depress. Anxiety 2007, 24, 392–398. [Google Scholar] [CrossRef]
- Agrawal, A.; Nurnberger, J.I.; Lynskey, M.T. Cannabis Involvement in Individuals with Bipolar Disorder. Psychiatry Res. 2011, 185, 459–461. [Google Scholar] [CrossRef] [Green Version]
- Polkosnik, G.L.; Sorkhou, M.; George, T.P. Effects of Cannabis Use on Psychotic and Mood Symptoms: A Systematic Review. Can. J. Addict. 2021, 12, 10. [Google Scholar] [CrossRef]
- Schoeler, T.; Monk, A.; Sami, M.B.; Klamerus, E.; Foglia, E.; Brown, R.; Camuri, G.; Altamura, A.C.; Murray, R.; Bhattacharyya, S. Continued versus Discontinued Cannabis Use in Patients with Psychosis: A Systematic Review and Meta-Analysis. Lancet Psychiatry 2016, 3, 215–225. [Google Scholar] [CrossRef] [Green Version]
- Strakowski, S.M.; DelBello, M.P.; Fleck, D.E.; Adler, C.M.; Anthenelli, R.M.; Keck, P.E.; Arnold, L.M.; Amicone, J. Effects of Co-Occurring Cannabis Use Disorders on the Course of Bipolar Disorder after a First Hospitalization for Mania. Arch. Gen. Psychiatry 2007, 64, 57–64. [Google Scholar] [CrossRef] [Green Version]
- Hunt, G.E.; Siegfried, N.; Morley, K.; Brooke-Sumner, C.; Cleary, M. Psychosocial Interventions for People with Both Severe Mental Illness and Substance Misuse. Cochrane Database Syst. Rev. 2019, 2019, CD001088. [Google Scholar] [CrossRef] [Green Version]
- Benishek, L.A.; Dugosh, K.L.; Kirby, K.C.; Matejkowski, J.; Clements, N.T.; Seymour, B.L.; Festinger, D.S. Prize-Based Contingency Management for the Treatment of Substance Abusers: A Meta-Analysis. Addiction 2014, 109, 1426–1436. [Google Scholar] [CrossRef] [Green Version]
- Schierenberg, A.; van Amsterdam, J.; van den Brink, W.; Goudriaan, A.E. Efficacy of Contingency Management for Cocaine Dependence Treatment: A Review of the Evidence. Curr. Drug Abus. Rev. 2012, 5, 320–331. [Google Scholar] [CrossRef]
- Secades-Villa, R.; Aonso-Diego, G.; García-Pérez, Á.; González-Roz, A. Effectiveness of Contingency Management for Smoking Cessation in Substance Users: A Systematic Review and Meta-Analysis. J. Consult. Clin. Psychol. 2020, 88, 951–964. [Google Scholar] [CrossRef]
- Budney, A.J.; Moore, B.A.; Rocha, H.L.; Higgins, S.T. Clinical Trial of Abstinence-Based Vouchers and Cognitive-Behavioral Therapy for Cannabis Dependence. J. Consult. Clin. Psychol. 2006, 74, 307–316. [Google Scholar] [CrossRef]
- Miguel, A.Q.C.; Madruga, C.S.; Cogo-Moreira, H.; Yamauchi, R.; Simões, V.; da Silva, C.J.; McPherson, S.; Roll, J.M.; Laranjeira, R.R. Contingency Management Is Effective in Promoting Abstinence and Retention in Treatment among Crack Cocaine Users in Brazil: A Randomized Controlled Trial. Psychol. Addict. Behav. 2016, 30, 536–543. [Google Scholar] [CrossRef]
- Petry, N.M.; Alessi, S.M.; Ledgerwood, D.M. A Randomized Trial of Contingency Management Delivered by Community Therapists. J. Consult. Clin. Psychol. 2012, 80, 286–298. [Google Scholar] [CrossRef] [Green Version]
- Destoop, M.; Docx, L.; Morrens, M.; Dom, G. Meta-Analysis on the Effect of Contingency Management for Patients with Both Psychotic Disorders and Substance Use Disorders. J. Clin. Med. 2021, 10, 616. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLOS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucatch, A.M.; Kloiber, S.M.; Meyer, J.H.; Rizvi, S.J.; George, T.P. Effects of Extended Cannabis Abstinence in Major Depressive Disorder. Can. J. Addict. 2020, 11, 33. [Google Scholar] [CrossRef]
- Rabin, R.A.; Barr, M.S.; Goodman, M.S.; Herman, Y.; Zakzanis, K.K.; Kish, S.J.; Kiang, M.; Remington, G.; George, T.P. Effects of Extended Cannabis Abstinence on Cognitive Outcomes in Cannabis Dependent Patients with Schizophrenia vs Non-Psychiatric Controls. Neuropsychopharmacology 2017, 42, 2259–2271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabin, R.A.; Kozak, K.; Zakzanis, K.K.; Remington, G.; George, T.P. Effects of Extended Cannabis Abstinence on Clinical Symptoms in Cannabis Dependent Schizophrenia Patients versus Non-Psychiatric Controls. Schizophr. Res. 2018, 194, 55–61. [Google Scholar] [CrossRef]
- Sigmon, S.C.; Steingard, S.; Badger, G.J.; Anthony, S.L.; Higgins, S.T. Contingent Reinforcement of Marijuana Abstinence among Individuals with Serious Mental Illness: A Feasibility Study. Exp. Clin. Psychopharmacol. 2000, 8, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Sigmon, S.C.; Higgins, S.T. Voucher-Based Contingent Reinforcement of Marijuana Abstinence among Individuals with Serious Mental Illness. J. Subst. Abus. Treat. 2006, 30, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Sorkhou, M.; Rabin, R.A.; Rabin, J.S.; Kloiber, S.; McIntyre, R.S.; George, T.P. Effects of 28 Days of Cannabis Abstinence on Cognition in Major Depressive Disorder: A Pilot Study. Am. J. Addict. 2022, 31, 454–462. [Google Scholar] [CrossRef]
- González-Roz, A.; Secades-Villa, R. Contingency Management for Smokers with Mental Health Disorders and Smoking-Sensitive Conditions Caused or Exacerbated by Tobacco Use: A Review of Existing Studies, Intervention Parameters, and Research Priorities. In Exp. Clin. Psychopharmacol. Available online: http://pubmed.ncbi.nlm.nih.gov (accessed on 20 November 2022). [CrossRef]
- Petry, N.M.; Alessi, S.M.; Rash, C.J. A Randomized Study of Contingency Management in Cocaine-Dependent Patients with Severe and Persistent Mental Health Disorders. Drug Alcohol Depend. 2013, 130, 234–237. [Google Scholar] [CrossRef]
- González-Roz, A.; Secades-Villa, R.; Alonso-Pérez, F. Effects of Combining Contingency Management with Behavioral Activation for Smokers with Depression. Addict. Res. Theory 2019, 27, 114–121. [Google Scholar] [CrossRef]
- Carpenter, V.L.; Hertzberg, J.S.; Kirby, A.C.; Calhoun, P.S.; Moore, S.D.; Dennis, M.F.; Dennis, P.A.; Dedert, E.A.; Hair, L.P.; Beckham, J.C. Multicomponent Smoking Cessation Treatment Including Mobile Contingency Management in Homeless Veterans. J. Clin. Psychiatry 2015, 76, 959–964. [Google Scholar] [CrossRef]
- Hicks, T.A.; Thomas, S.P.; Wilson, S.M.; Calhoun, P.S.; Kuhn, E.R.; Beckham, J.C. A Preliminary Investigation of a Relapse Prevention Mobile Application to Maintain Smoking Abstinence Among Individuals With Posttraumatic Stress Disorder. J. Dual Diagn. 2017, 13, 15–20. [Google Scholar] [CrossRef]
- Medenblik, A.M.; Mann, A.M.; Beaver, T.A.; Dedert, E.A.; Wilson, S.M.; Calhoun, P.S.; Beckham, J.C. Treatment Outcomes of a Multi-Component Mobile Health Smoking Cessation Pilot Intervention for People with Schizophrenia. J. Dual Diagn. 2020, 16, 420–428. [Google Scholar] [CrossRef]
- Lowe, D.J.E.; Sasiadek, J.D.; Coles, A.S.; George, T.P. Cannabis and Mental Illness: A Review. Eur. Arch. Psychiatry Clin. Neurosci. 2019, 269, 107–120. [Google Scholar] [CrossRef]
- Cooke, M.E.; Gilman, J.M.; Lamberth, E.; Rychik, N.; Tervo-Clemmens, B.; Evins, A.E.; Schuster, R.M. Assessing Changes in Symptoms of Depression and Anxiety During Four Weeks of Cannabis Abstinence Among Adolescents. Front. Psychiatry 2021, 12, 689957. [Google Scholar] [CrossRef]
- Schuster, R.M.; Gilman, J.; Schoenfeld, D.; Evenden, J.; Hareli, M.; Ulysse, C.; Nip, E.; Hanly, A.; Zhang, H.; Evins, A.E. One Month of Cannabis Abstinence in Adolescents and Young Adults Is Associated With Improved Memory. J. Clin. Psychiatry 2018, 79, 17m11977. [Google Scholar] [CrossRef]
- Schuster, R.M.; Hanly, A.; Gilman, J.; Budney, A.; Vandrey, R.; Evins, A.E. A Contingency Management Method for 30-Days Abstinence in Non-Treatment Seeking Young Adult Cannabis Users. Drug Alcohol Depend. 2016, 167, 199–206. [Google Scholar] [CrossRef] [Green Version]
- Carroll, K.M.; Kosten, T.R.; Rounsaville, B.J. Choosing a Behavioral Therapy Platform for Pharmacotherapy of Substance Users. Drug Alcohol Depend. 2004, 75, 123–134. [Google Scholar] [CrossRef] [Green Version]
- Allsop, D.J.; Dunlop, A.J.; Saddler, C.; Rivas, G.R.; McGregor, I.S.; Copeland, J. Changes in Cigarette and Alcohol Use during Cannabis Abstinence. Drug Alcohol Depend. 2014, 138, 54–60. [Google Scholar] [CrossRef]
- Copersino, M.L.; Boyd, S.J.; Tashkin, D.P.; Huestis, M.A.; Heishman, S.J.; Dermand, J.C.; Simmons, M.S.; Gorelick, D.A. Quitting Among Non-Treatment-Seeking Marijuana Users: Reasons and Changes in Other Substance Use. Am. J. Addict. 2006, 15, 297–302. [Google Scholar] [CrossRef]
- Rabin, R.A.; Dermody, S.S.; George, T.P. Changes in Tobacco Consumption in Cannabis Dependent Patients with Schizophrenia versus Non-Psychiatric Controls during 28-Days of Cannabis Abstinence. Drug Alcohol Depend. 2018, 185, 181–188. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference | Aim | Study Design | Type of Contingency Management | Sample Characteristics (% Male) | Scale Used for SUD Diagnosis | SUD Outcome | SUD Findings | Scale Used for Psychiatric Diagnosis | Mental Health Outcome | Symptom Findings |
|---|---|---|---|---|---|---|---|---|---|---|
| Lucatch et al., 2020 [24] | To understand the effects of cannabis abstinence on clinical symptoms of depression in individuals with CUD and MDD | Within subject, feasibility, successive cohort | Monetary | N = 11 (27.3%M) | DSM-5 | THC-COOH levels; urinalysis, MWC | Cr-THC-COOH levels significantly declined over the 28-day abstinence period across all participants, statistically significant changes in withdrawal severity over time; post-hoc test revealed a significant increase in withdrawal symptoms between weeks 1 and 2 | DSM-5 | BAI, HAM-D, SHAPS | Reductions in THC were significantly associated with reductions in depression and anhedonia scores over time, while a non-significant trend was determined for reductions in anxiety scores |
| Sigmon et al., 2000 [25] | To examine the sensitivity of cannabis use to monetary incentives among individuals with schizophrenia and other serious mental illness | Within subject, crossover, feasibility, successive cohort | Monetary | N = 18 (100%M) | DSM-III-R | THC-COOH levels; urinalysis | The average total number and consecutive number of marijuana-negative specimens obtained were greater during the conditions wherein participants received monetary reinforcement contingent on abstinence than in the baseline conditions | DSM-IV | BPRS | No significant changes in psychiatric symptom severity in either baseline or incentive conditions |
| Sigmon & Higgins, 2006 [26] | To determine the efficacy of voucher-based contingency management in reducing marijuana use in individuals with schizophrenia, schizoaffective disorder, or other serious mental illnesses | Within-subject, reversal design | Voucher | N = 7 (86%M) | DSM-IV | Urinalysis using Abuscreen ONTRAK | Compared to the other conditions, the percentage of negative urine tests were significantly greater during the voucher intervention | DSM-IV | N/A | N/A |
| Rabin et al., 2017 [27] | To determine the effects of cannabis abstinence on cognition in patients with schizophrenia and co-occurring cannabis dependence | Within subject, feasibility, successive cohort | Monetary | N = 39 (100%M) | DSM-IV-TR | THC-COOH levels; urinalysis | Participant abstinence rates were not significantly different between patients with schizophrenia and non-psychiatric control groups: 42.1% of patients (8/19) and 55% of controls (11/20) successfully achieved abstinence verification criteria | DSM-IV-TR | HVLT, SDR, Digit Span Forwards and Backwards, CPT-II, TMT, grooved pegboard, BART, KDDT, SARS, BARS, AIMS | Patients with schizophrenia who successfully abstained demonstrated improvements in verbal memory and learning; however, findings were insignificant when correcting for multiple comparisons No changes in SARS, BARS, or AIMS scores between baseline and day 28 in patient abstainers and non-abstainers |
| Rabin et al., 2018 [28] | To determine the effects of cannabis abstinence on clinical symptoms in patients with schizophrenia and co-occurring cannabis dependence | Within subject, feasibility, successive cohort | Monetary | N = 39 (100%M) | DSM-IV-TR | THC-COOH levels; urinalysis, TLFB | Abstaining and relapsing patients and controls, demonstrated a significant decrease in self-reported cannabis consumption over the 28-day study period (patient and control abstainers, p < 0.001; and patient and control relapsers, p < 0.01) | DSM-IV-TR | PANSS, CDSS, HAM-D | PANSS scores remained constant across the abstinence period in both abstaining and non-abstaining patients Significant main effect of time on CDSS scores between abstainers and non-abstainers; insignificant abstinence status x time interaction No significant effect of time on HAM-D scores |
| Sorkhou et al., 2022 [29] | To determine whether a 28-day period of cannabis abstinence is associated with improvements in cognition in patients with MDD and comorbid CUD | Within subject, feasibility, successive cohort | Monetary | N = 11 (27.3%M) | DSM-5 | THC-COOH levels; urinalysis | Cr-THC-COOH levels significantly declined over the 28-day abstinence period across all participants. Moreover, 8/11 (72.7%) participants met pre-specified criteria for 28 days of cannabis abstinence. In the three participants who failed to meet abstinence (lapsers), Cr-THC-COOH levels decreased substantially (~93%) from Day 0 to Day 28 | DSM-5 | HVLT, CPT, TMT-A, TMT-B, SDR-30, DS-Forwards, DS-Backwards | Visual search speed, selective attention, and VSWM improved over the study period; improvements were not associated with changes in cannabis metabolite levels from baseline to endpoint |
| Reference | Bias Due to Confounding | Bias in Selection of Participants into the Study | Bias in Classification of Interventions | Bias Due to Deviations from Intended Interventions | Bias Due to Missing Data | Bias in Measurement of Outcomes | Bias in Selection of the Reported Result | Overall RoB |
|---|---|---|---|---|---|---|---|---|
| Lucatch et al., 2020 [24] | Critical | Low | Serious | Low | Serious | Serious | Low | Critical |
| Rabin et al., 2017 [27] | Moderate | Low | Serious | Low | Low | Serious | Low | Serious |
| Rabin et al., 2018 [28] | Moderate | Low | Serious | Low | Low | Serious | Low | Serious |
| Sigmon et al., 2000 [25] | Moderate | Low | Low | Low | Serious | Serious | Moderate | Serious |
| Sigmon & Higgins, 2006 [26] | Moderate | Low | Low | Low | Moderate | Serious | Low | Serious |
| Sorkhou et al., 2022 [29] | Critical | Low | Serious | Low | Serious | Serious | Low | Critical |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodas, J.D.; Sorkhou, M.; George, T.P. Contingency Management for Treatment of Cannabis Use Disorder in Co-Occurring Mental Health Disorders: A Systematic Review. Brain Sci. 2023, 13, 36. https://doi.org/10.3390/brainsci13010036
Rodas JD, Sorkhou M, George TP. Contingency Management for Treatment of Cannabis Use Disorder in Co-Occurring Mental Health Disorders: A Systematic Review. Brain Sciences. 2023; 13(1):36. https://doi.org/10.3390/brainsci13010036
Chicago/Turabian StyleRodas, Justyne D., Maryam Sorkhou, and Tony P. George. 2023. "Contingency Management for Treatment of Cannabis Use Disorder in Co-Occurring Mental Health Disorders: A Systematic Review" Brain Sciences 13, no. 1: 36. https://doi.org/10.3390/brainsci13010036