
Camrelizumab-Induced Isolate Abducens Neuritis: A Rare Ophthalmic Immune-Related Adverse Events

Abstract
:1. Introduction
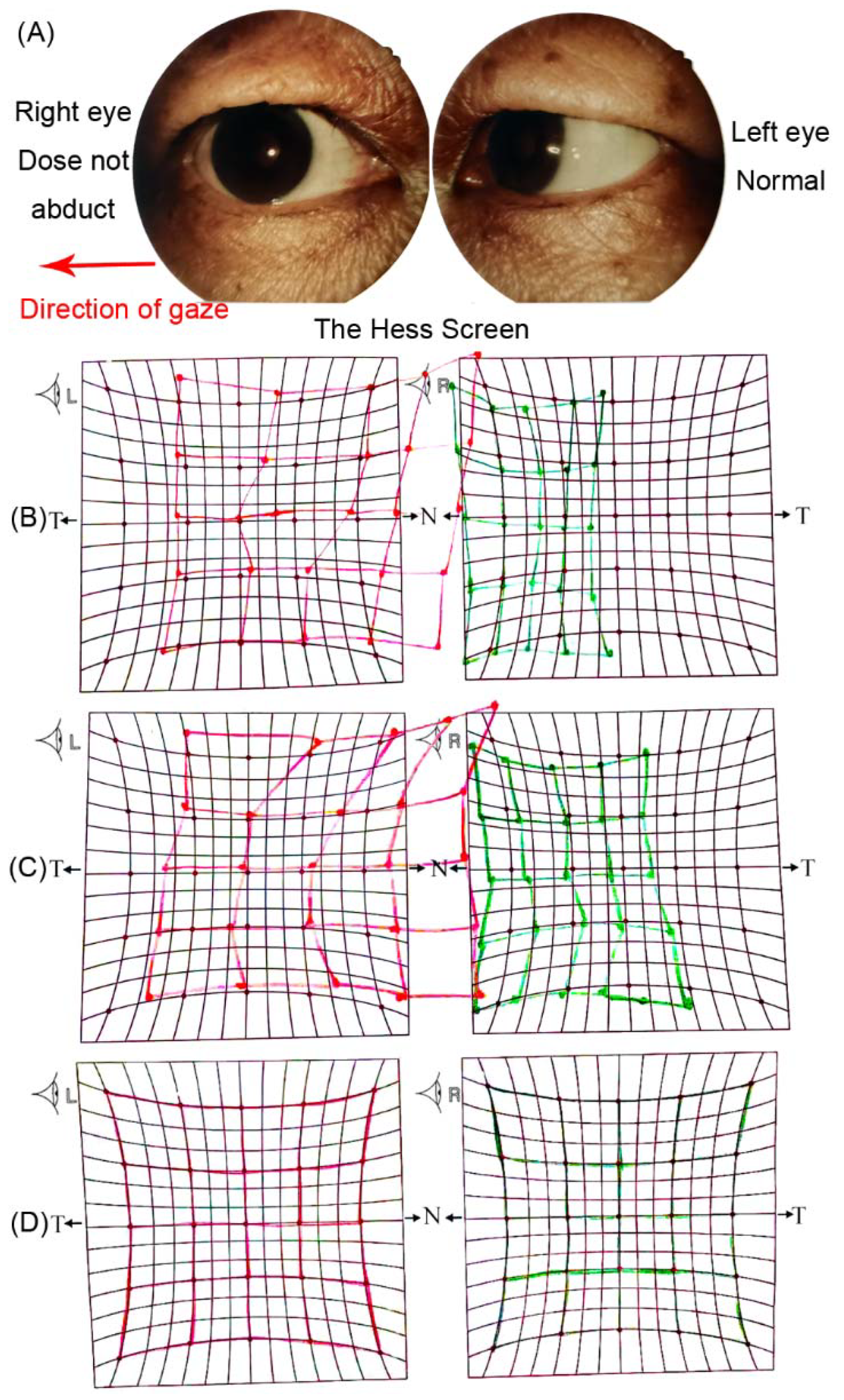
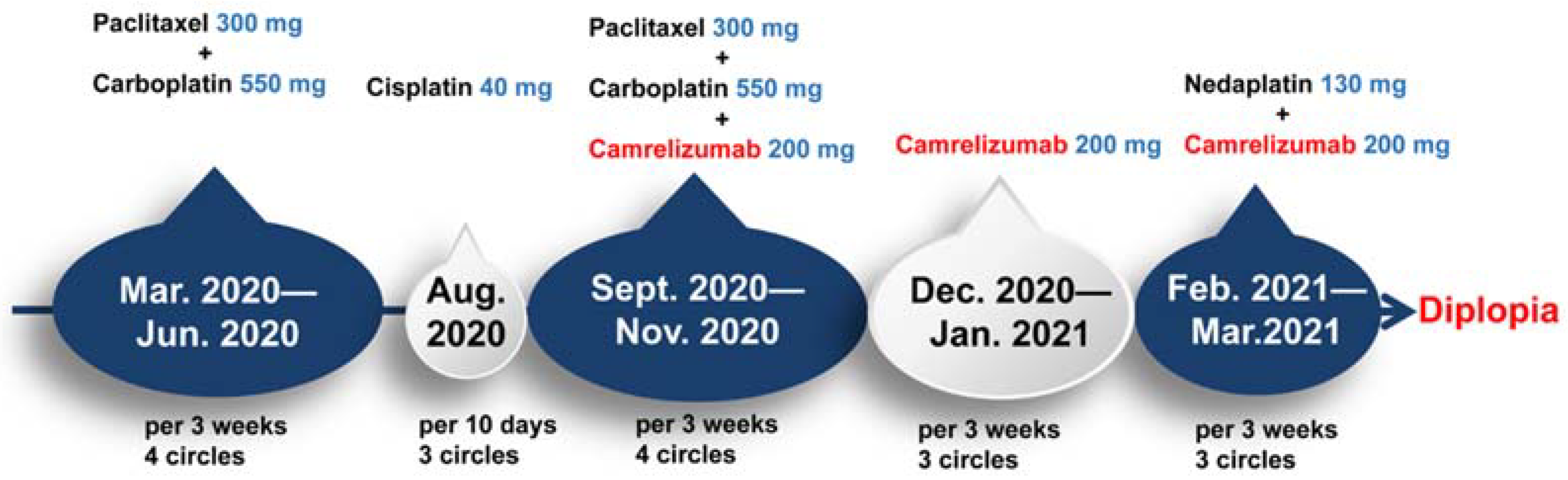
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Richards, B.W.; Jones, F.R., Jr.; Younge, B.R. Causes and prognosis in 4278 cases of paralysis of the oculomotor, trochlear, and abducens cranial nerves. Am. J. Ophthalmol. 1992, 113, 489–496. [Google Scholar] [CrossRef]
- Moster, M.L.; Savino, P.J.; Sergott, R.C.; Bosley, T.M.; Schatz, N.J. Isolated sixth-nerve palsies in younger adults. Arch. Ophthalmol. 1984, 102, 1328–1330. [Google Scholar] [CrossRef] [PubMed]
- Ribas, A.; Wolchok, J.D. Cancer immunotherapy using checkpoint blockade. Science 2018, 359, 1350–1355. [Google Scholar] [CrossRef] [PubMed]
- Markham, A.; Keam, S.J. Correction to: Camrelizumab: First Global Approval. Drugs 2019, 79, 1497. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, L.L.; Aguiar, P.N., Jr.; Park, R.; Edelman Saul, E.; Haaland, B.; de Lima Lopes, G. Comparative Efficacy and Safety of Programmed Death-1 Pathway Inhibitors in Advanced Gastroesophageal Cancers: A Systematic Review and Network Meta-Analysis of Phase III Clinical Trials. Cancers 2021, 13, 2614. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Lou, A.; Yu, J. Immune checkpoint inhibitor-related pneumonitis induced by camrelizumab: A case report and review of literature. Ann. Palliat. Med. 2021, 10, 8460–8466. [Google Scholar] [CrossRef] [PubMed]
- Tan, Y.; Ye, Y.; Chen, L. Fatal immune-related hepatitis with intrahepatic cholestasis and pneumonia associated with camrelizumab: A case report and literature review. Open Med. 2021, 16, 553–557. [Google Scholar] [CrossRef]
- Liang, S.; Yang, J.; Lin, Y.; Li, T.; Zhao, W.; Zhao, J.; Dong, C. Immune Myocarditis Overlapping with Myasthenia Gravis due to Anti-PD-1 Treatment for a Chordoma Patient: A Case Report and Literature Review. Front. Immunol. 2021, 12, 682262. [Google Scholar] [CrossRef]
- Bai, J.; Li, D.; Yang, P.; Xu, K.; Wang, Y.; Li, Q.; Liu, J.; Du, W.; Zhang, F.; Feng, R. Camrelizumab-Related Myocarditis and Myositis with Myasthenia Gravis: A Case Report and Literature Review. Front. Oncol. 2021, 11, 778185. [Google Scholar] [CrossRef]
- Dalvin, L.A.; Shields, C.L.; Orloff, M.; Sato, T.; Shields, J.A. Checkpoint Inhibitor Immune Therapy: Systemic Indications and Ophthalmic Side Effects. Retina 2018, 38, 1063–1078. [Google Scholar] [CrossRef] [PubMed]
- Dow, E.R.; Yung, M.; Tsui, E. Immune Checkpoint Inhibitor-associated Uveitis: Review of Treatments and Outcomes. Ocul. Immunol. Inflamm. 2020, 29, 203–211. [Google Scholar] [CrossRef]
- Vogrig, A.; Muñiz-Castrillo, S.; Joubert, B.; Picard, G.; Rogemond, V.; Skowron, F.; Egri, M.; Desestret, V.; Tilikete, C.; Psimaras, D.; et al. Cranial Nerve Disorders Associated with Immune Checkpoint Inhibitors. Neurology 2021, 96, e866–e875. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, L.; Goldinger, S.M.; Hofmann, L.; Loquai, C.; Ugurel, S.; Thomas, I.; Schmidgen, M.I.; Gutzmer, R.; Utikal, J.S.; Göppner, D.; et al. Neurological, respiratory, musculoskeletal, cardiac and ocular side-effects of anti-PD-1 therapy. Eur. J. Cancer 2016, 60, 210–225. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.M.; Seleme, N.; Chen, J.J.; Zekeridou, A.; Sechi, E.; Walsh, R.D.; Beebe, J.D.; Sabbagh, O.; Mejico, L.J.; Gratton, S.; et al. Neuro-Ophthalmic Complications in Patients Treated with CTLA-4 and PD-1/PD-L1 Checkpoint Blockade. J. Neuro-Ophthalmol. Off. J. N. Am. Neuro-Ophthalmol. Soc. 2021, 41, 519–530. [Google Scholar] [CrossRef] [PubMed]
- Park, K.A.; Min, J.H.; Oh, S.Y.; Kim, B.J. Idiopathic third and sixth cranial nerve neuritis. Jpn. J. Ophthalmol. 2019, 63, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Park, K.A.; Oh, S.Y.; Min, J.H.; Kim, B.J.; Kim, Y. Cause of acquired onset of diplopia due to isolated third, fourth, and sixth cranial nerve palsies in patients aged 20 to 50 years in Korea: A high resolution magnetic resonance imaging study. J. Neurol. Sci. 2019, 407, 116546. [Google Scholar] [CrossRef] [PubMed]
- Peters, G.B., 3rd; Bakri, S.J.; Krohel, G.B. Cause and prognosis of nontraumatic sixth nerve palsies in young adults. Ophthalmology 2002, 109, 1925–1928. [Google Scholar] [CrossRef]
- Dubey, D.; David, W.S.; Reynolds, K.L.; Chute, D.F.; Clement, N.F.; Cohen, J.V.; Lawrence, D.P.; Mooradian, M.J.; Sullivan, R.J.; Guidon, A.C. Severe Neurological Toxicity of Immune Checkpoint Inhibitors: Growing Spectrum. Ann. Neurol. 2020, 87, 659–669. [Google Scholar] [CrossRef] [PubMed]
- Vogrig, A.; Muñiz-Castrillo, S.; Joubert, B.; Picard, G.; Rogemond, V.; Marchal, C.; Chiappa, A.M.; Chanson, E.; Skowron, F.; Leblanc, A.; et al. Central nervous system complications associated with immune checkpoint inhibitors. J. Neurol. Neurosurg. Psychiatry 2020, 91, 772–778. [Google Scholar] [CrossRef] [PubMed]
- Touat, M.; Maisonobe, T.; Knauss, S.; Ben Hadj Salem, O.; Hervier, B.; Auré, K.; Szwebel, T.A.; Kramkimel, N.; Lethrosne, C.; Bruch, J.F.; et al. Immune checkpoint inhibitor-related myositis and myocarditis in patients with cancer. Neurology 2018, 91, e985–e994. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/Year | Gender | Age | Tumour | Anti-PD-1 | Treatment of irAE | Outcome of irAE | Other irAE |
|---|---|---|---|---|---|---|---|
| Vogrig, [12] 2021 | Male | 63 | Melanoma | Ipilimumab- pembrolizumab | pause of ICIs oral corticosteroids | Resolved | autoimmune colitis |
| Male | 82 | Melanoma | Nivolumab | pause of nivolumab prednisone (1 mg/kg/day) | Resolved | facial nerve palsy | |
| Zimmer, [13] 2016 | Male | 83 | Melanoma | Nivolumab | pause of nivolumab Methylprednisolone (1 mg/kg/day) | Resolved | facial nerve palsy |
| Sun, [14] 2021 | Male | 52 | Melanoma | Ipilimumab/ nivolumab | Methylprednisolone; prednisone | Improved | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hou, Y.; Su, Q.; Tang, S.; Li, H. Camrelizumab-Induced Isolate Abducens Neuritis: A Rare Ophthalmic Immune-Related Adverse Events. Brain Sci. 2022, 12, 1242. https://doi.org/10.3390/brainsci12091242
Hou Y, Su Q, Tang S, Li H. Camrelizumab-Induced Isolate Abducens Neuritis: A Rare Ophthalmic Immune-Related Adverse Events. Brain Sciences. 2022; 12(9):1242. https://doi.org/10.3390/brainsci12091242
Chicago/Turabian StyleHou, Yanli, Qiang Su, Simeng Tang, and Hongyang Li. 2022. "Camrelizumab-Induced Isolate Abducens Neuritis: A Rare Ophthalmic Immune-Related Adverse Events" Brain Sciences 12, no. 9: 1242. https://doi.org/10.3390/brainsci12091242