
Altered Regional Homogeneity and Amplitude of Low-Frequency Fluctuations Induced by Electroconvulsive Therapy for Adolescents with Depression and Suicidal Ideation

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Clinical Assessment
2.3. Electroconvulsive Therapy
2.4. Rs-fMRI Acquisition
2.5. Image Preprocessing
2.6. Calculation of ReHo and ALFF
2.7. Statistical Analysis
3. Results
3.1. Clinical Outcomes
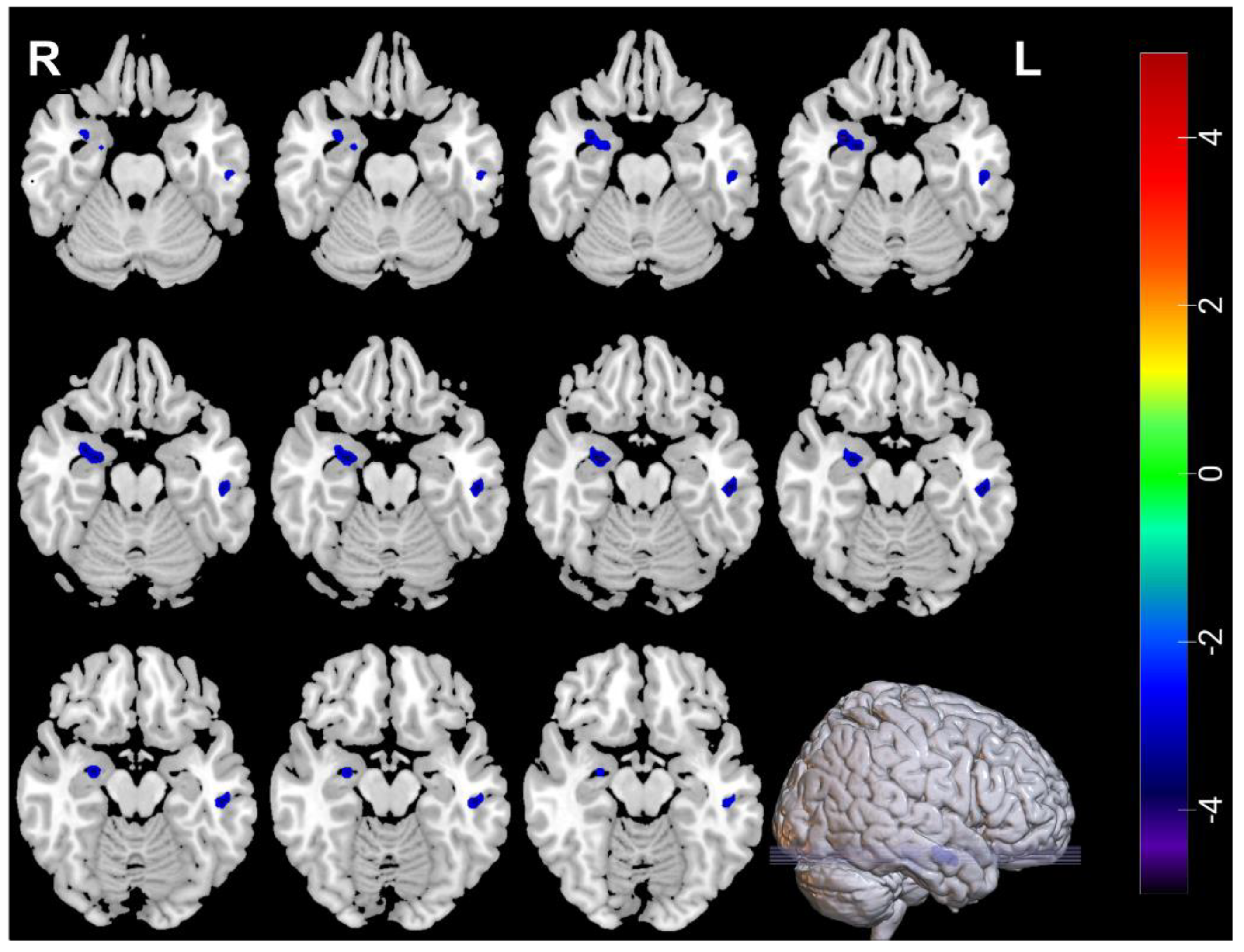
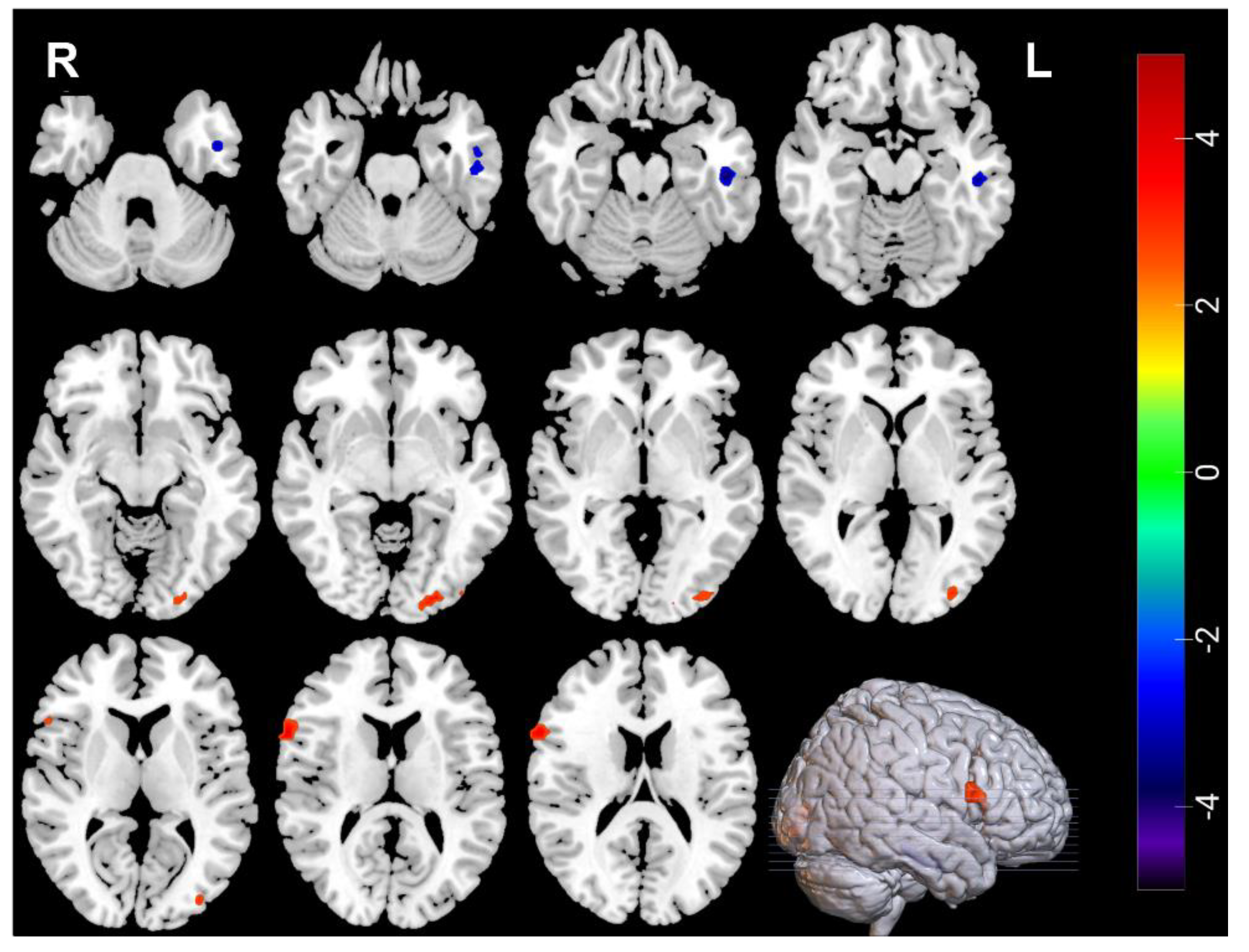
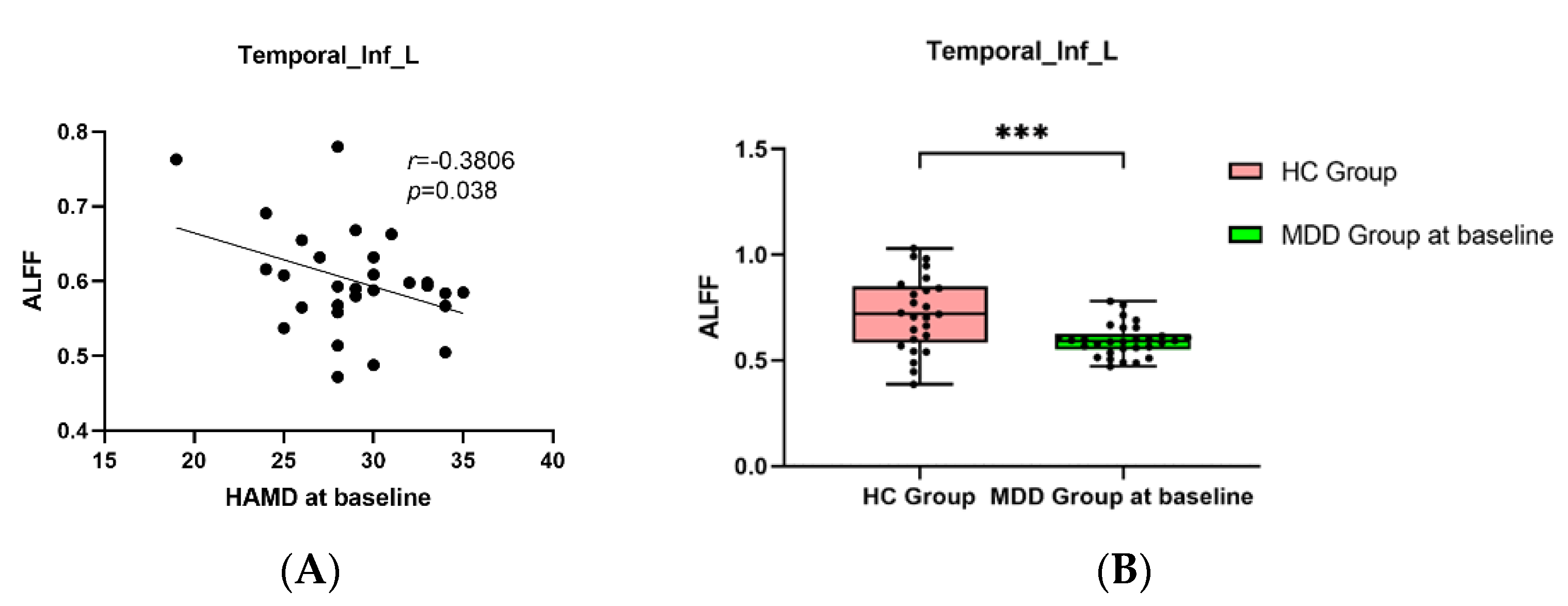
3.2. Neuroimaging Comparisons between MDDs at Baseline and HCs
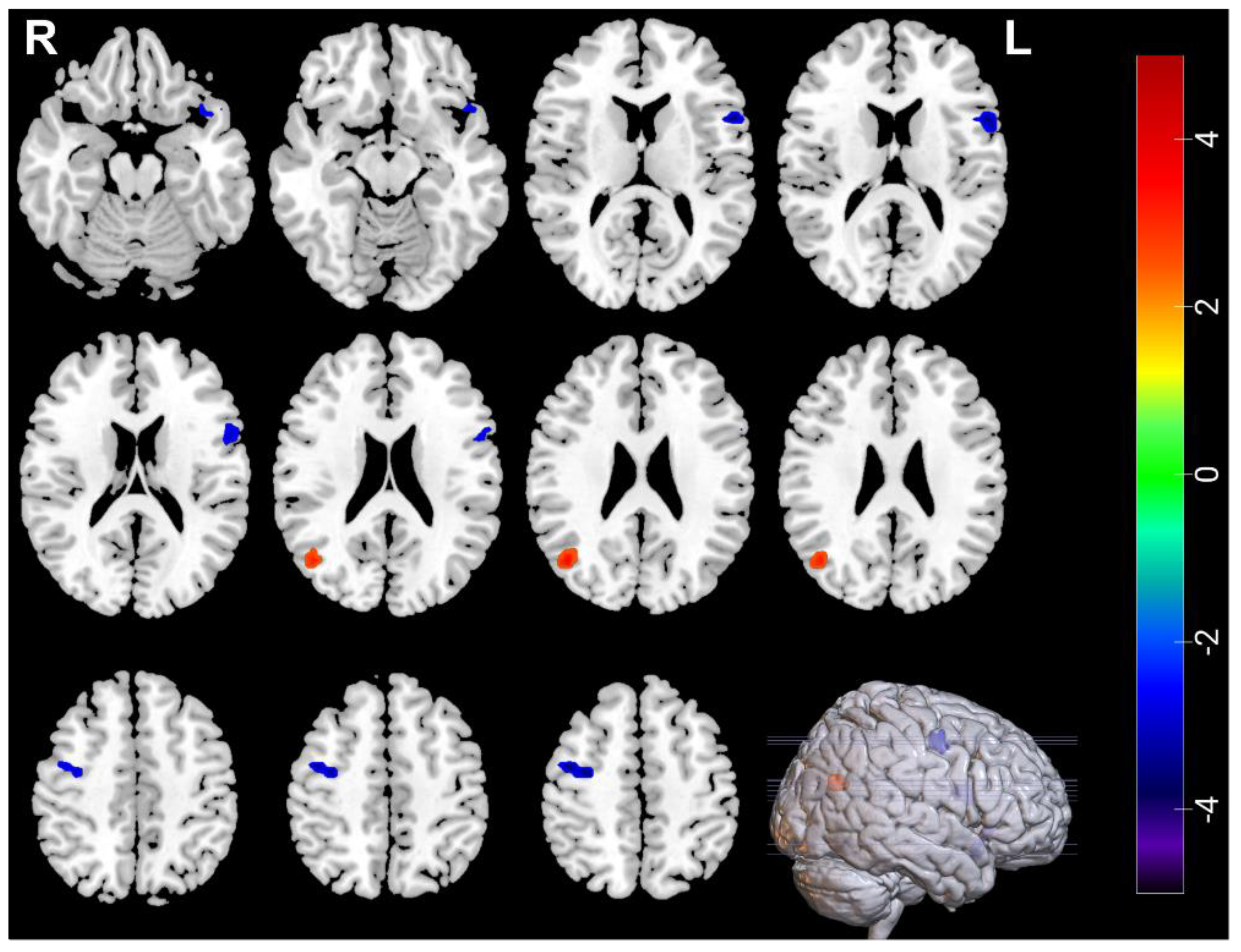
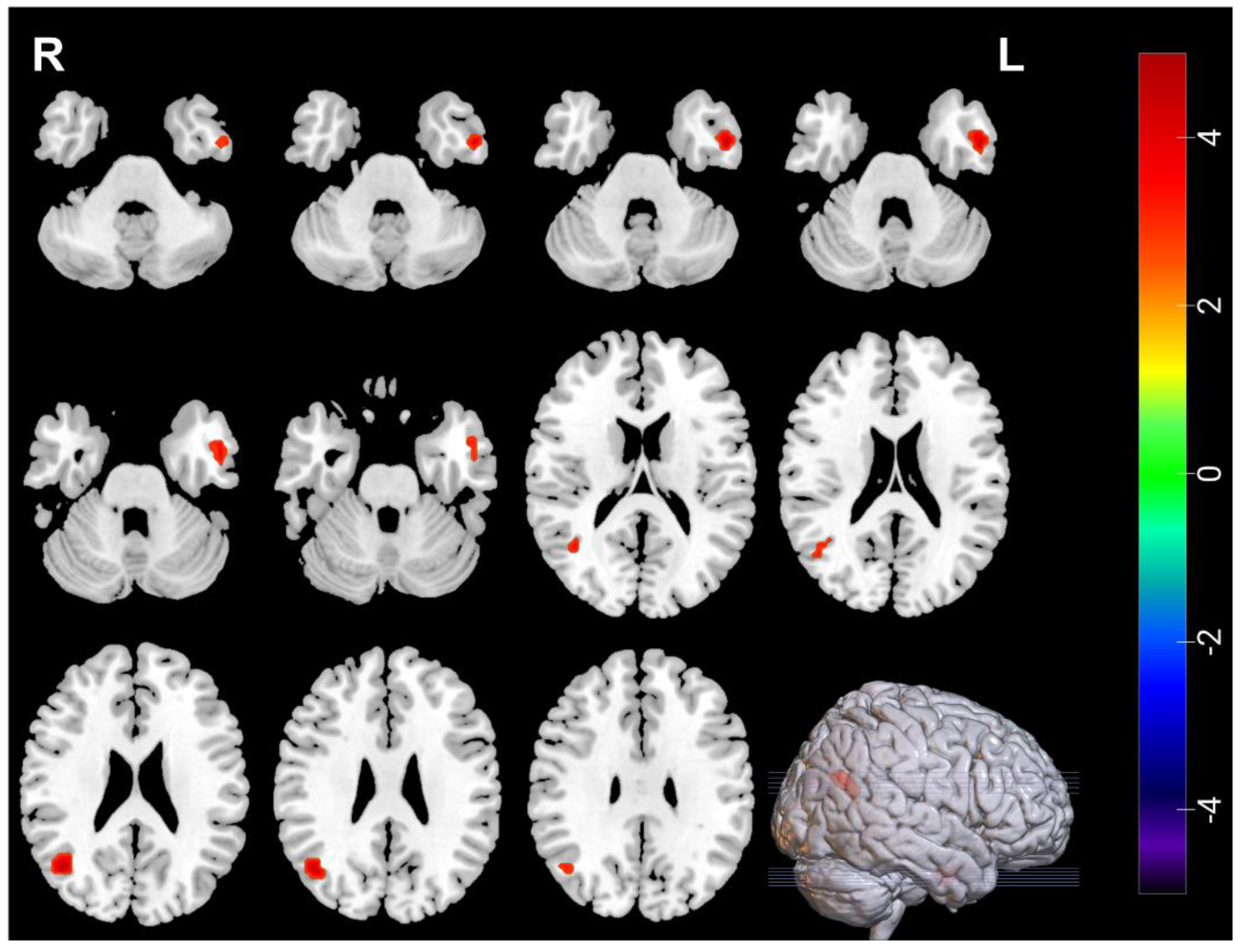
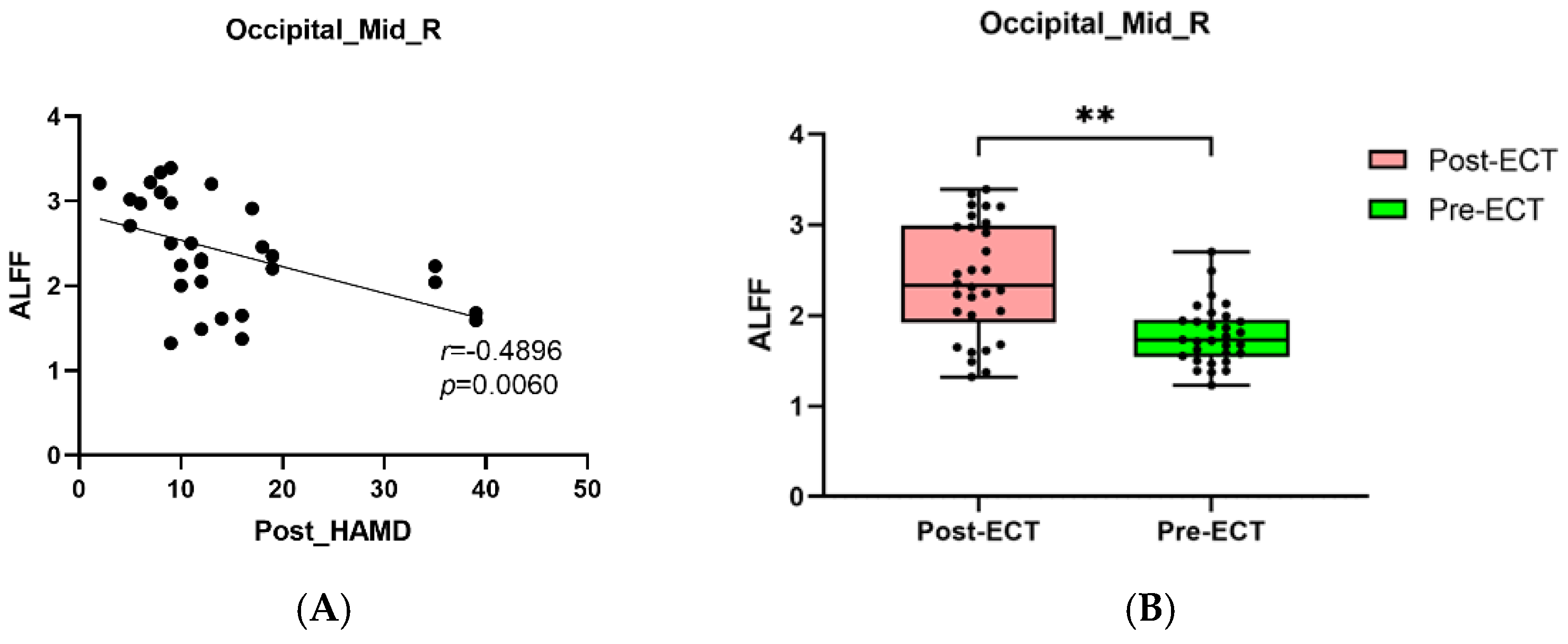
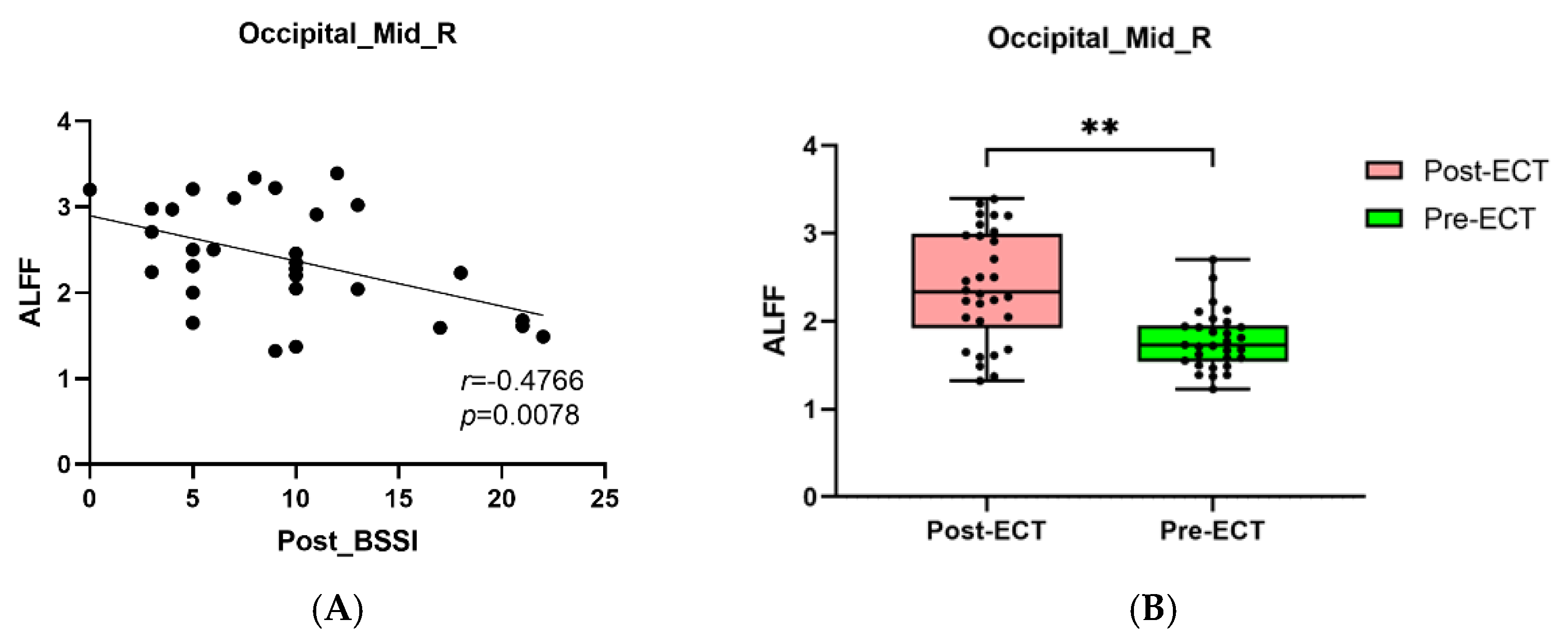
3.3. Neuroimaging Comparisons in MDDs Pre/Post-ECT
3.4. Pearson Correlation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miller, L.; Campo, J.V. Depression in Adolescents. N. Engl. J. Med. 2021, 385, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Avenevoli, S.; Swendsen, J.; He, J.P.; Burstein, M.; Merikangas, K.R. Major depression in the national comorbidity survey-adolescent supplement: Prevalence, correlates, and treatment. J. Am. Acad. Child. Adolesc. Psychiatry 2015, 54, 37–44.e2. [Google Scholar] [CrossRef]
- Sarkisian, K.L.; Van Hulle, C.A.; Goldsmith, H.H. Brooding, Inattention, and Impulsivity as Predictors of Adolescent Suicidal Ideation. J. Abnorm. Child Psychol. 2019, 47, 333–344. [Google Scholar] [CrossRef]
- Wang, Y.; Xiao, S.; Guo, X.; Hu, M. A systematic review and meta-analysis of related factors of suicide ideation among Chinese middle and high school students. Chin. Ment. Health J. 2019, 33, 464–469. [Google Scholar]
- Miller, A.B.; McLaughlin, K.A.; Busso, D.S.; Brueck, S.; Peverill, M.; Sheridan, M.A. Neural correlates of emotion regulation and adolescent suicidal ideation. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2018, 3, 125–132. [Google Scholar] [CrossRef]
- Levi-Belz, Y.; Gavish-Marom, T.; Barzilay, S.; Apter, A.; Carli, V.; Hoven, C.; Sarchiapone, M.; Wasserman, D. Psychosocial factors correlated with undisclosed suicide attempts to significant others: Findings from the adolescence SEYLE study. Suicide Life Threat. Behav. 2019, 49, 759–773. [Google Scholar] [CrossRef]
- Klonsky, E.D.; May, A.M.; Safer, B.Y. Suicide, suicide attempts, and suicidal ideation. Annu. Rev. Clin. Psychol. 2016, 12, 307–330. [Google Scholar] [CrossRef]
- Zhang, Y.Y.; Lei, Y.T.; Song, Y.; Lu, R.R.; Duan, J.L.; Prochaska, J.J. Gender differences in suicidal ideation and health-risk behaviors among high school students in Beijing, China. J. Glob. Health 2019, 9, e010604. [Google Scholar] [CrossRef]
- Rush, A.J.; Trivedi, M.H.; Wisniewski, S.R.; Nierenberg, A.A.; Stewart, J.W.; Warden, D.; Niederehe, G.; Thase, M.E.; Lavori, P.W.; Lebowitz, B.D.; et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: A STAR*D report. Am. J. Psychiatry 2006, 163, 1905–1917. [Google Scholar] [CrossRef]
- Husain, M.M.; Rush, A.J.; Fink, M.; Knapp, R.; Petrides, G.; Rummans, T.; Biggs, M.M.; O’Connor, K.; Rasmussen, K.; Litle, M.; et al. Speed of response and remission in major depressive disorder with acute electroconvulsive therapy (ECT): A Consortium for Research in ECT (CORE) report. J. Clin. Psychiatry 2004, 65, 485–491. [Google Scholar] [CrossRef]
- McCall, W.V. Finally, Evidence for Continuation Electroconvulsive Therapy in Major Depressive Disorder. J. ECT 2016, 32, 221. [Google Scholar] [CrossRef] [PubMed]
- Ghaziuddin, N.; Kutcher, S.P.; Knapp, P.; Bernet, W.; Arnold, V.; Beitchman, J.; Benson, R.S.; Bukstein, O.; Kinlan, J.; Kinlan, J.; et al. Practice parameter for use of electroconvulsive therapy with adolescents. J. Am. Acad. Child. Adolesc. Psychiatry 2004, 43, 1521–1539. [Google Scholar] [CrossRef] [PubMed]
- Hořínková, J.; Bartečků, E.; Kališová, L. The Practice of Electroconvulsive Therapy in Children and Adolescents in the Czech Republic. J. ECT 2021, 37, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Hoop, J.G.; Smyth, A.C.; Roberts, L.W. Ethical issues in psychiatric research on children and adolescents. Child. Adolesc. Psychiatr. Clin. N. Am. 2008, 17, 127–148. [Google Scholar] [CrossRef]
- Puffer, C.C.; Wall, C.A.; Huxsahl, J.E.; Frye, M.A. A 20-year practice review of electroconvulsive therapy in adolescents. J. Child. Adolesc. Psychopharmacol. 2016, 26, 632–636. [Google Scholar] [CrossRef]
- Mitchell, S.; Hassan, E.; Ghaziuddin, N. A follow-up study of electroconvulsive therapy in children and adolescents. J. ECT 2018, 34, 40–44. [Google Scholar] [CrossRef]
- Nugent, A.C.; Martinez, A.; D’Alfonso, A.; Zarate, C.A.; Theodore, W.H. The relationship between glucose metabolism, resting-state fMRI BOLD signal, and GABA (A)-binding potential: A preliminary study in healthy subjects and those with temporal lobe epilepsy. J. Cereb. Blood Flow Metab. 2015, 35, 583–591. [Google Scholar] [CrossRef]
- Daniel, P.C.; Marta, C.; Joan, A.C.; Colleen, L.; Diego, P.; Carles, S.M.; Cardoner, N. A multimetric systematic review of fMRI findings in patients with MDD receiving ECT. Prog. Neuropsychopharmacol. Biol. Psychiatry 2020, 108, 110178. [Google Scholar] [CrossRef]
- Lan, M.J.; Rizk, M.M.; Pantazatos, S.P.; Falcone, H.R.; Miller, J.M.; Sublette, M.E.; Oquendo, M.A.; Keilp, J.G.; Mann, J.J. Resting-state amplitude of low-frequency fluctuation is associated with suicidal ideation. Depress. Anxiety 2019, 36, 433–441. [Google Scholar] [CrossRef]
- Liu, Y.; Du, L.; Li, Y.; Liu, H.; Zhao, W.; Liu, D.; Zeng, J.; Li, X.; Fu, Y.; Qiu, H.; et al. Antidepressant effects of electroconvulsive therapy correlate with subgenual anterior cingulate activity and connectivity in depression. Medicine 2015, 94, e2033. [Google Scholar] [CrossRef]
- Zang, Y.; Jiang, T.; Lu, Y.; He, Y.; Tian, L. Regional homogeneity approach to fMRI data analysis. Neuroimage 2004, 22, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Long, X.; Zang, Y.; Wang, L.; Hallett, M.; Li, K.; Chan, P. Regional homogeneity changes in patients with Parkinson’s disease. Hum. Brain Mapp. 2009, 30, 1502–1510. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.Z.; Li, D.M.; Kuang, W.H.; Zhang, T.J.; Lui, S.; Huang, X.Q.; Chan, R.C.; Kemp, G.J.; Gong, Q.Y. Abnormal regional spontaneous neural activity in treatment-refractory depression revealed by resting-state fMRI. Hum. Brain Mapp. 2011, 32, 1290–1299. [Google Scholar] [CrossRef]
- Kong, X.M.; Xu, S.X.; Sun, Y.; Wang, K.Y.; Wang, C.; Zhang, J.; Xia, J.X.; Zhang, L.; Tan, B.J.; Xie, X.H. Electroconvulsive therapy changes the regional resting state function measured by regional homogeneity (ReHo) and amplitude of low frequency fluctuations (ALFF) in elderly major depressive disorder patients: An exploratory study. Psychiatry Res. Neuroimaging 2017, 264, 13–21. [Google Scholar] [CrossRef]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef]
- Beck, A.T.; Kovacs, M.; Weissman, A. Assessment of suicidal intention: The scale for suicide ideation. J. Consult. Clin. Psychol. 1979, 47, 343–352. [Google Scholar] [CrossRef]
- Zhao, J.P.; Zheng, Y.P. Reliability and validity of Hamilton Depression Scale assessed in 329 Chinese depression patients. Chin. Ment. Health J. 1992, 5, 214–216. [Google Scholar]
- Li, X.Y.; Phillips, M.R.; Tong, Y.S.; Li, K.J.; Zhang, Y.L.; Zhang, Y.P. Reliability and validity of the Chinese version of Beck Suicide Ideation Scale (BSI-CV) in adult community reMDDents. Chin. Ment. Health J. 2010, 24, 250–255. [Google Scholar] [CrossRef]
- Kendall, M.G. Rank Correlation Methods, 5th ed.; Oxford University Press: Oxford, UK, 1990. [Google Scholar]
- Dai, Z.; Yan, C.; Wang, Z.; Wang, J.; Xia, M.; Li, K.; He, Y. Discriminative analysis of early Alzheimer’s disease using multi-modal imaging and multi-level characterization with multi-classifier (M3). Neuroimage 2012, 59, 2187–2195. [Google Scholar] [CrossRef]
- Zang, Y.F.; He, Y.; Zhu, C.Z.; Cao, Q.J.; Sui, M.Q.; Liang, M.; Tian, L.X.; Jiang, T.Z.; Wang, Y.F. Altered baseline brain activity in children with ADHD revealed by resting-state functional MRI. Brain Dev. 2007, 29, 83–91. [Google Scholar] [CrossRef]
- Monkul, E.S.; Hatch, J.P.; Nicoletti, M.A.; Spence, S.; Brambilla, P.; Lacerda, A.L.T.; Sassi, R.B.; Mallinger, A.G.; Keshavan, M.S.; Soares, J.C. Fronto-limbic brain structures in suicidal and non-suicidal female patients with major depressive disorder. Mol. Psychiatry 2007, 12, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Wagner, G.; Koch, K.; Schachtzabel, C.; Schultz, C.C.; Sauer, H.; Schlösser, R.G. Structural brain alterations in patients with major depressive disorder and high risk for suicide: Evidence for a distinct neurobiological entity? Neuroimage 2011, 54, 1607–1614. [Google Scholar] [CrossRef] [PubMed]
- Willeumier, K.; Taylor, D.V.; Amen, D.G. Decreased cerebral blood flow in the limbicand prefrontal cortex using SPECT imaging in a cohort of completed suicides. Transl. Psychiatry 2011, 1, e28. [Google Scholar] [CrossRef] [PubMed]
- Jollant, F.; Lawrence, N.S.; Giampietro, V.; Brammer, M.J.; Fullana, M.A.; Drapier, D.; Courtet, P.; Phillips, M.L. Orbitofrontal cortex response toangry faces in men with histories of suicide attempts. Am. J. Psychiatry 2008, 165, 740–748. [Google Scholar] [CrossRef]
- Jollant, F.; Lawrence, N.S.; Olie, E.; O’Daly, O.; Malafosse, A.; Courtet, P.; Phillips, M.L. Decreased activation of lateral orbitofrontal cortex during risky choices under uncertainty is associated with disadvantageous decision-making and suicidal behavior. Neuroimage 2010, 51, 1275–1281. [Google Scholar] [CrossRef]
- Pan, L.A.; Phillips, M.L. Toward identification of neural markers of suicide risk in adolescents. Neuropsychopharmacology 2014, 39, 236. [Google Scholar] [CrossRef]
- Zhang, R.; Wei, S.N.; Chang, M.; Jiang, X.W.; Tang, Y.Q.; Wang, F. Dorsolateral and ventrolateral prefrontal cortex structural changes relative to suicidal ideation in patients with depression. Acta Neuropsychiatr. 2020, 32, 84–91. [Google Scholar] [CrossRef]
- Lee, Y.J.; Park, S.Y.; Sung, L.Y.; Kim, J.H.; Choi, J.; Oh, K.; Hahn, S.W. Reduced left ventrolateral prefrontal cortex activation during verbal fluency tasks is associated with suicidal ideation severity in medication-naïve young adults with major depressive disorder: A functional near-infrared spectroscopy study. Psychiatry Res. Neuroimaging 2021, 312, 111288. [Google Scholar] [CrossRef]
- Liu, J.; Ren, L.; Womer, F.Y.; Wang, J.; Fan, G.; Jiang, W.; Blumberg, H.P.; Tang, Y.; Xu, K.; Wang, F. Alterations in amplitude of low frequency fluctuation in treatment-naïve major depressive disorder measured with resting-state fMRI. Hum. Brain Mapp. 2014, 35, 4979–4988. [Google Scholar] [CrossRef]
- Chen, C.F.; Chen, W.N.; Zhang, B. Functional alterations of the suicidal brain: A coordinate-based meta-analysis of functional imaging studies. Brain Imaging Behav. 2022, 16, 291–304. [Google Scholar] [CrossRef]
- Fan, T.T.; Wu, X.; Yao, L.; Dong, J. Abnormal baseline brain activity in suicidal and non-suicidal patients with major depressive disorder. Neurosci. Lett. 2013, 534, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Teng, C.J.; Zhou, J.; Ma, H.; Tan, Y.R.; Wu, X.; Guan, C.; Qiao, H.; Li, J.; Zhong, Y.; Wang, C.; et al. Abnormal resting state activity of left middle occipital gyrus and its functional connectivity in female patients with major depressive disorder. BMC Psychiatry 2018, 18, 370. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Tang, Y.; Zhu, Y.; Tong, S. Study of functional brain homogeneity in female patients with major depressive disorder. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 2562–2565. [Google Scholar] [CrossRef]
- Yan, M.; He, Y.; Cui, X.; Liu, F.; Li, H.; Huang, R.; Tang, Y.; Chen, J.; Zhao, J.; Xie, G.; et al. Disrupted Regional Homogeneity in Melancholic and Non-melancholic Major Depressive Disorder at Rest. Front. Psychiatry 2021, 12, 618805. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, H.L.; Frith, C.D. Functional imaging of ‘theory of mind’. Trends Cogn. Sci. 2003, 7, 77–83. [Google Scholar] [CrossRef]
- Saxe, R.; Kanwisher, N. People thinking about thinking people: The role of the temporo-parietal junction in “theory of mind”. Neuroimage 2003, 19, 1835–1842. [Google Scholar] [CrossRef]
- Huang, Q.; Xiao, M.N.; Ai, M.; Chen, J.M.; Wang, W.; Hu, L.; Cao, J.; Wang, M.; Kuang, L. Disruption of Neural Activity and Functional Connectivity in Adolescents with Major Depressive Disorder Who Engage in Non-suicidal Self-Injury: A Resting-State fMRI Study. Front. Psychiatry 2021, 12, 571532. [Google Scholar] [CrossRef]
- Ramezani, M.; Johnsrude, I.; Rasoulian, A.; Bosma, R.; Tong, R.; Hollenstein, T.; Harkness, K.; Abolmaesumi, P. Temporal-lobe morphology differs between healthy adolescents and those with early-onset of depression. Neuroimage Clin. 2014, 6, 145–155. [Google Scholar] [CrossRef]
- Du, L.; Wang, J.; Meng, B.; Yong, N.; Yang, X.; Huang, Q.; Zhang, Y.; Yang, L.; Qu, Y.; Chen, Z.; et al. Early life stress affects limited regional brain activity in depression. Sci. Rep. 2016, 6, 25338. [Google Scholar] [CrossRef]
- Hamann, S. Cognitive and neural mechanisms of emotional memory. Trends Cogn. Sci. 2001, 5, 394–400. [Google Scholar] [CrossRef]
- Sah, P.; Faber, E.S.; Lopez, D.A.M.; Power, J. The amygdaloid complex: Anatomy and physiology. Physiol. Rev. 2003, 83, 803–834. [Google Scholar] [CrossRef]
- Cullen, K.R.; Westlund, M.K.; Klimes-Dougan, B.; Mueller, B.A.; Houri, A.; Eberly, L.E.; Lim, K.O. Abnormal amygdala resting-state functional connectivity in adolescent depression. JAMA Psychiatry 2014, 71, 1138–1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Types of Medications | |
|---|---|
| Antidepressants (n = 30) | Sertraline (n = 17) |
| Fluoxetine (n = 11) | |
| Venlafaxine (n = 1) | |
| Escitalopram (n = 1) | |
| Antipsychotics (n = 26) | Quetiapine (n = 13) |
| Olanzapine (n = 8) | |
| Aripiprazole (n = 4) | |
| Risperidone (n = 1) | |
| Anti-anxiety drugs (n = 5) | Tandospirone (n = 5) |
| Others (n = 3) | Propranolol (n = 2) |
| TrihexyPhenidyl (n = 1) |
| Characteristic | HC (n = 25) | MDD (n = 30) | t-Value | p |
|---|---|---|---|---|
| Age, mean (SD), y | 15.48 (1.87) | 14.60 (1.45) | 1.962 | 0.197 * |
| Sex (male/female) | 6/19 | 8/22 | 0.222 | 0.657 # |
| Education years, mean (SD), y | 9.68 (2.21) | 8.50 (1.70) | 0.143 | 0.143 * |
| HAMD, mean (SD) | 1.60 (2.06) | 29.03 (6.02) | / | <0.001 * |
| BSSI, mean (SD) | 0 | 22.10 (5.73) | / | <0.001 * |
| Characteristic | Pre-ECT | Post-ECT | t-Value | p |
|---|---|---|---|---|
| HAMD, mean (SD) | 29.03(6.02) | 13.77(8.89) | 9.762 | <0.001 * |
| BSSI, mean (SD) | 22.10(5.73) | 8.10(6.94) | 10.734 | <0.001 * |
| Measures | Brain Regions | Voxel Size | Peak t Value | MNI Coordinates | ||
|---|---|---|---|---|---|---|
| Decreased | ||||||
| ALFF | Amygdala_R | 31 | −4.637 | 33 | 0 | −21 |
| ALFF | Temporal_Inf_L | 30 | −3.6166 | −51 | −24 | −18 |
| ReHo | Temporal_Inf_L | 45 | −4.3107 | −48 | −21 | −18 |
| Increased | ||||||
| ReHo | Frontal_Inf_Oper_R | 40 | 4.0503 | 63 | 15 | 15 |
| ReHo | Occipital_Mid_L | 41 | 3.7464 | −36 | −84 | 6 |
| Measures | Brain Regions | Voxel Size | Peak t Value | MNI Coordinates | ||
|---|---|---|---|---|---|---|
| Decreased | ||||||
| ALFF | Temporal_Pole_Sup_L | 30 | −4.0615 | −51 | 18 | −15 |
| ALFF | Frontal_Inf_Oper_L | 39 | −3.9169 | −54 | 12 | 12 |
| ALFF | Frontal_Mid_R | 34 | −4.2384 | 42 | −3 | 51 |
| Increased | ||||||
| ALFF | Occipital_Mid_R | 30 | 3.7765 | 42 | −66 | 24 |
| ReHo | Occipital_Mid_R | 46 | 4.5719 | 42 | −63 | 24 |
| ReHo | Temporal_Inf_L | 38 | 4.761 | −51 | −3 | −33 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, X.; Chen, X.; Zhou, Y.; Dai, L.; Cui, L.-B.; Yu, R.; Ai, M.; Huang, Q.; Tian, Y.; Ming, M.; et al. Altered Regional Homogeneity and Amplitude of Low-Frequency Fluctuations Induced by Electroconvulsive Therapy for Adolescents with Depression and Suicidal Ideation. Brain Sci. 2022, 12, 1121. https://doi.org/10.3390/brainsci12091121
Li X, Chen X, Zhou Y, Dai L, Cui L-B, Yu R, Ai M, Huang Q, Tian Y, Ming M, et al. Altered Regional Homogeneity and Amplitude of Low-Frequency Fluctuations Induced by Electroconvulsive Therapy for Adolescents with Depression and Suicidal Ideation. Brain Sciences. 2022; 12(9):1121. https://doi.org/10.3390/brainsci12091121
Chicago/Turabian StyleLi, Xiao, Xiaolu Chen, Yi Zhou, Linqi Dai, Long-Biao Cui, Renqiang Yu, Ming Ai, Qian Huang, Yu Tian, Mei Ming, and et al. 2022. "Altered Regional Homogeneity and Amplitude of Low-Frequency Fluctuations Induced by Electroconvulsive Therapy for Adolescents with Depression and Suicidal Ideation" Brain Sciences 12, no. 9: 1121. https://doi.org/10.3390/brainsci12091121