
Comprehensive Assessment of Acute Isolated or Prominent Dysarthria in the Emergency Department: A Neuro-Emergency Expert’s Experience beyond Stroke

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
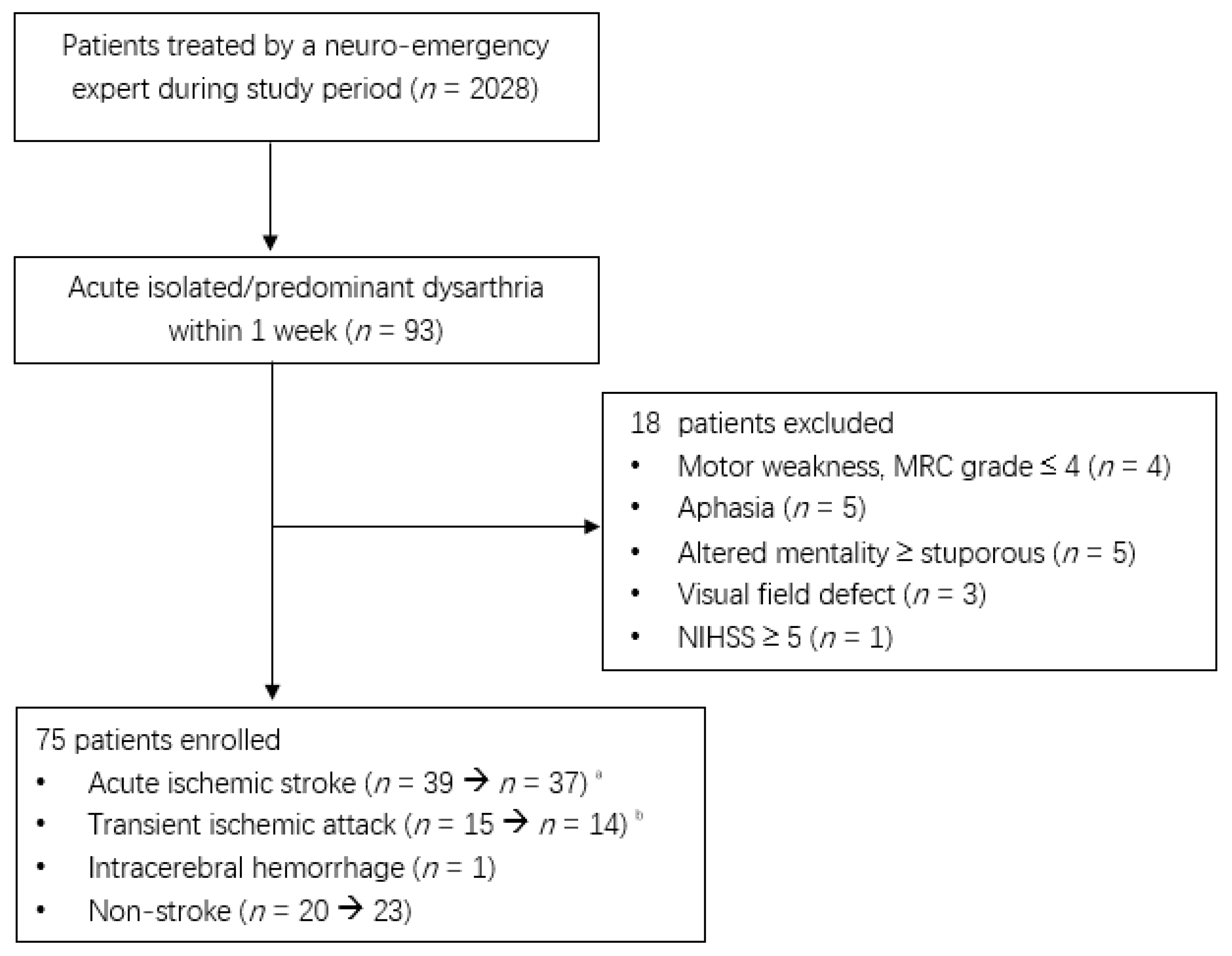
2.1. Study Design and Patient Selection
2.2. Data Collection
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stipancic, K.L.; Borders, J.C.; Brates, D.; Thibeault, S.L. Prospective Investigation of Incidence and Co-Occurrence of Dysphagia, Dysarthria, and Aphasia Following Ischemic Stroke. Am. J. Speech Lang. Pathol. 2019, 28, 188–194. [Google Scholar] [CrossRef]
- Flowers, H.L.; Silver, F.L.; Fang, J.; Rochon, E.; Martino, R. The incidence, co-occurrence, and predictors of dysphagia, dysarthria, and aphasia after first-ever acute ischemic stroke. J. Commun. Disord. 2013, 46, 238–248. [Google Scholar] [CrossRef]
- Vidovic, M.; Sinanovic, O.; Sabaskic, L.; Haticic, A.; Brkic, E. Incidence and types of speech disorders in stroke patients. Acta Clin. Croat. 2011, 50, 491–494. [Google Scholar]
- Arboix, A.; Bell, Y.; García-Eroles, L.; Massons, J.; Comes, E.; Balcells, M.; Targa, C. Clinical Study of 35 Patients With Dysarthria-Clumsy Hand Syndrome. J. Neurol. Neurosurg. Psychiatry 2004, 75, 231–234. [Google Scholar] [PubMed]
- De Cock, E.; Batens, K.; Hemelsoet, D.; Boon, P.; Oostra, K.; De Herdt, V. Dysphagia, Dysarthria and Aphasia Following a First Acute Ischaemic Stroke: Incidence and Associated Factors. Eur. J. Neurol. 2020, 27, 2014–2021. [Google Scholar] [CrossRef] [PubMed]
- Urban, P.P.; Hopf, H.C.; Zorowka, P.G.; Fleischer, S.; Andreas, J. Dysarthria and Lacunar Stroke: Pathophysiologic Aspects. Neurology 1996, 47, 1135–1141. [Google Scholar] [CrossRef] [PubMed]
- Urban, P.P.; Wicht, S.; Vukurevic, G.; Fitzek, C.; Fitzek, S.; Stoeter, P.; Massinger, C.; Hopf, H.C. Dysarthria in Acute Ischemic Stroke: Lesion Topography, Clinicoradiologic Correlation, and Etiology. Neurology 2001, 56, 1021–1027. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, K.; Kageyama, Y. Clinical Anatomic Study of Pure Dysarthria. Stroke 1991, 22, 809–812. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.S. Pure Dysarthria, Isolated Facial Paresis, or Dysarthria-Facial Paresis Syndrome. Stroke 1994, 25, 1994–1998. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.S.; Kwon, S.U.; Lee, T.G. Pure Dysarthria Due to Small Cortical Stroke. Neurology 2003, 60, 1178–1180. [Google Scholar] [CrossRef]
- Tanaka, K.; Yamada, T.; Torii, T.; Yoshimura, T.; Takase, K.; Togao, O.; Wakata, Y.; Hiwatashi, A.; Nakashima, N.; Kira, J.; et al. Pure Dysarthria and Dysarthria-Facial Paresis Syndrome Due to Internal Capsule and/or Corona Radiata Infarction. BMC Neurol. 2015, 15, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozaki, I.; Baba, M.; Narita, S.; Matsunaga, M.; Takebe, K. Pure dysarthria due to anterior internal capsule and/or corona radiata infarction: A report of five cases. J. Neurol. Neurosurg. Psychiatry 1986, 49, 1435–1437. [Google Scholar] [CrossRef] [PubMed]
- Beliavsky, A.; Perry, J.J.; Dowlatshahi, D.; Wasserman, J.; Sivilotti, M.L.; Sutherland, J.; Worster, A.; Emond, M.; Stotts, G.; Jin, A.Y.; et al. Acute Isolated Dysarthria Is Associated With a High Risk of Stroke. Cerebrovasc. Dis. Extra 2014, 4, 182–185. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.W.; Ha, S.O.; Kim, J.H.; Yang, W.S.; Park, Y.S. Experience of a Neuro-emergency Expert in the Emergency Department During One Year of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 9416. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., 3rd. Classification of Subtype of Acute Ischemic Stroke. Definitions for Use in a Multicenter Clinical Trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caplan, L.R. Ataxia in Patients With Brain Infarcts and Hemorrhages. Handb. Clin. Neurol. 2012, 103, 147–160. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Isolated Dysarthria | Prominent Dysarthria | p-Value |
|---|---|---|---|
| (n = 28) | (n = 47) | ||
| Age, years | 70.0 (58.0–79.0) | 71.0 (60.0–80.0) | 0.793 |
| Age group, years * | |||
| 40–59 | 7 (25.0) | 12 (25.5) | 0.836 |
| 60–79 | 14 (50.0) | 21 (44.7) | |
| ≥80 | 7 (25.0) | 14 (29.8) | |
| Male | 16 (57.1) | 28 (59.6) | 0.713 |
| Onset-to-door time, min | 689.0 (87.0–1350.0) | 1283.0 (411.0–4020.0) | 0.042 |
| Coexisting condition | |||
| Hypertension | 20 (71.4) | 26 (55.3) | 0.166 |
| Diabetes mellitus | 9 (32.1) | 14 (29.8) | 0.831 |
| Dyslipidemia | 5 (17.9) | 9 (19.1) | 0.890 |
| Current smoker | 4 (14.3) | 3 (6.4) | 0.413 |
| Atrial fibrillation | 0 (0.0) | 2 (4.3) | 0.526 |
| Ischemic stroke | 1 (3.6) | 1 (2.1) | 0.707 |
| Coronary artery disease | 0 (0.0) | 3 (6.4) | 0.289 |
| Chronic renal disease | 2 (7.1) | 3 (6.4) | 0.898 |
| Antithrombotic agent | |||
| Aspirin | 3 (10.7) | 10 (21.3) | 0.348 |
| Clopidogrel | 3 (10.7) | 2 (4.3) | 0.356 |
| Rivaroxaban | 0 (0.0) | 1 (2.1) | 0.437 |
| Variables | Total | Isolated Dysarthria | Prominent Dysarthria |
|---|---|---|---|
| (n = 75) | (n = 28) | (n = 47) | |
| Stroke | 52 (69.3) | 18 (64.3) | 34 (72.3) |
| AIS | 37 (49.3) | 11 (39.3) | 26 (55.3) |
| TIA | 14 (18.7) | 7 (25.0) | 7 (14.9) |
| ICH | 1 (1.3) | 0 (0.0) | 1 (2.1) |
| Non-stroke | 23 (30.7) * | 10 (35.7) * | 13 (27.7) * |
| Metabolic | 7 (9.3) | 3 (10.7) | 4 (8.5) |
| Toxic | 6 (8.0) | 4 (14.3) | 2 (4.3) |
| Brain tumor | 2 (2.7) | 1 (3.6) | 1 (2.1) |
| Parkinson disease | 2 (2.7) | 1 (3.6) | 1 (2.1) |
| Multiple sclerosis | 1 (1.3) | 0 (0.0) | 1 (2.1) |
| Seizure | 1 (1.3) | 1 (3.6) | 0 (0.0) |
| Multiple cranial neuropathy | 1 (1.3) | 0 (0.0) | 1 (2.1) |
| Aortic dissection | 1 (1.3) | 0 (0.0) | 1 (2.1) |
| Appendicitis | 1 (1.3) | 0 (0.0) | 1 (2.1) |
| Psychiatric | 1 (1.3) | 0 (0.0) | 1 (2.1) |
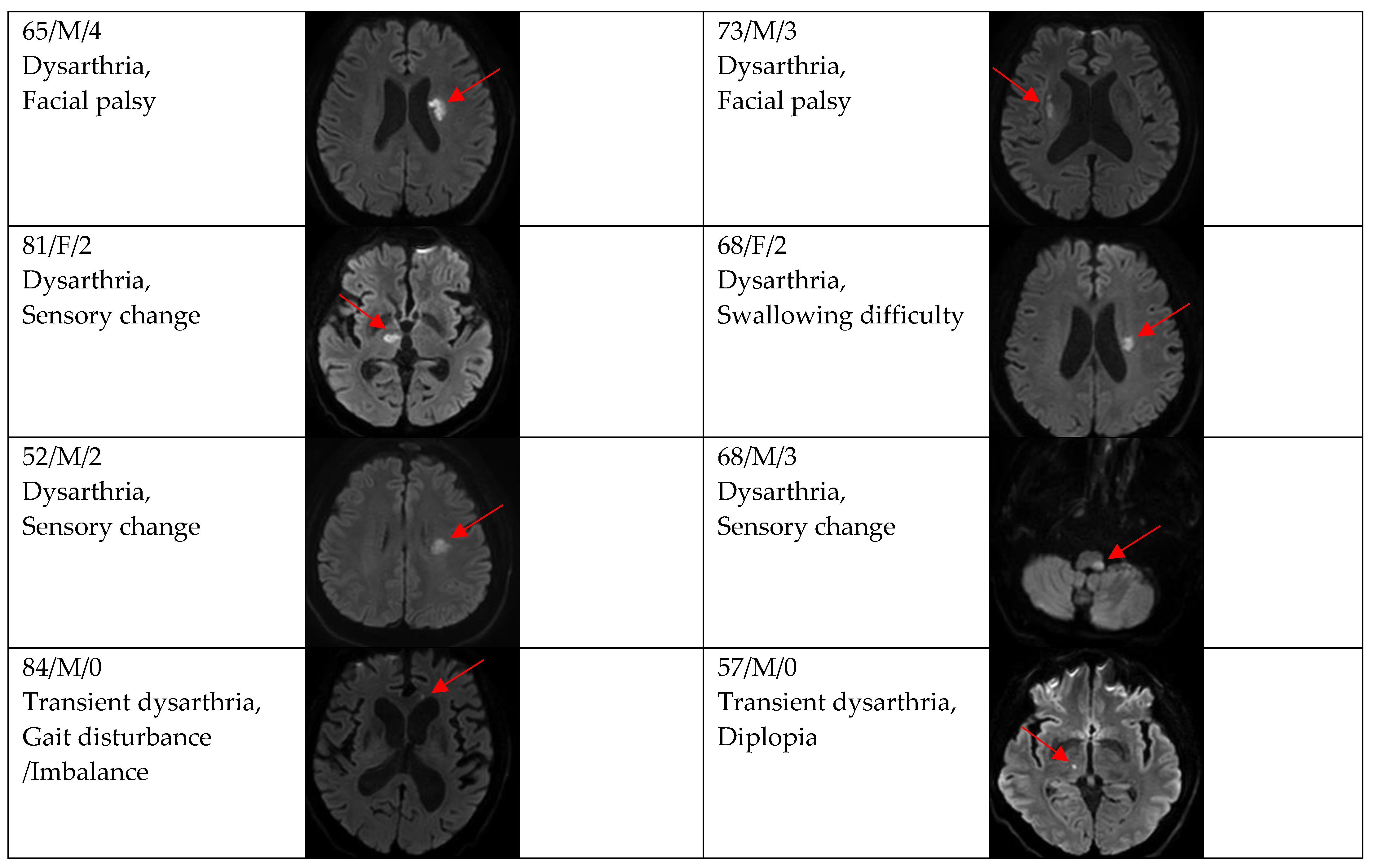
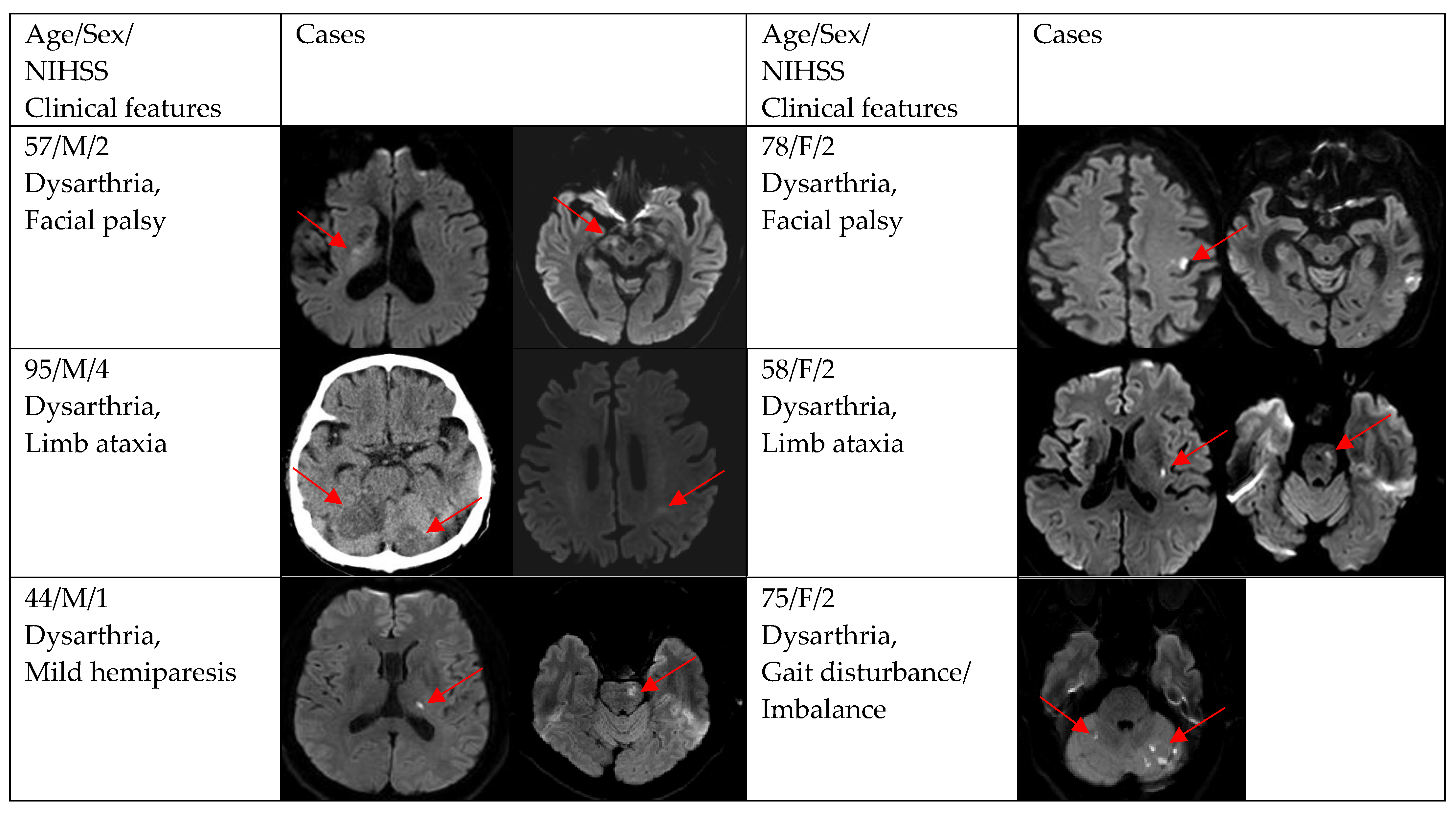
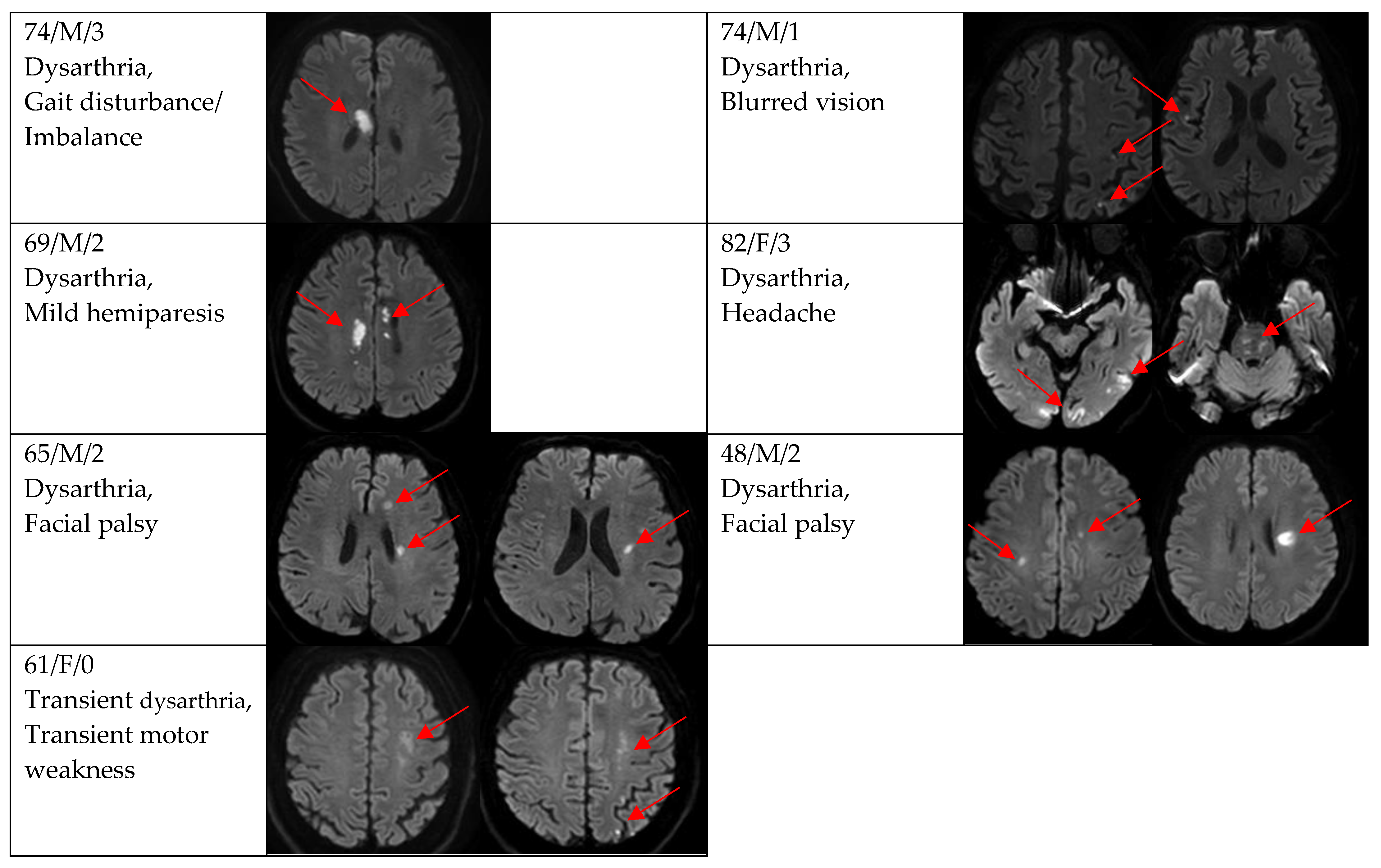
| Additional Neurologic Symptoms | Total * | Non-Stoke * | Stroke * |
|---|---|---|---|
| (n = 47) | (n = 13) | (n = 34) | |
| Gait disturbance/imbalance | 9 (19.2) | 1 (7.7) | 8 (23.5) |
| Facial palsy | 8 (17.0) | 1 (7.7) | 7 (20.6) |
| Mild hemiparesis | 5 (10.6) | 2 (15.4) | 3 (8.8) |
| Dizziness | 4 (8.5) | 3 (23.1) | 1 (2.9) |
| Limb ataxia | 3 (6.4) | 0 (0.0) | 3 (8.8) |
| Sensory change | 3 (6.4) | 0 (0.0) | 3 (8.8) |
| Transient motor weakness | 3 (6.4) | 0 (0.0) | 3 (8.8) |
| Swallowing difficulty | 2 (4.3) | 1 (7.7) | 1 (2.9) |
| Acute memory loss | 1 (2.1) | 1 (7.7) | 0 (0.0) |
| Chest pain | 1 (2.1) | 1 (7.7) | 0 (0.0) |
| Diplopia | 1 (2.1) | 0 (0.0) | 1 (2.9) |
| Fever | 1 (2.1) | 1 (7.7) | 0 (0.0) |
| Headache | 1 (2.1) | 0 (0.0) | 1 (2.9) |
| Hip pain | 1 (2.1) | 0 (0.0) | 1 (2.9) |
| Leg weakness | 1 (2.1) | 0 (0.0) | 1 (2.9) |
| Drowsy mentality | 1 (2.1) | 1 (7.7) | 0 (0.0) |
| Tongue palsy | 1 (2.1) | 1 (7.7) | 0 (0.0) |
| Blurred vision | 1 (2.1) | 0 (0.0) | 1 (2.9) |
| Variables | Isolated Dysarthria | Prominent Dysarthria | p-Value |
|---|---|---|---|
| (n = 18) | (n = 33) | ||
| Clinical diagnosis | 0.204 | ||
| Ischemic stroke | 11 (61.1) | 26 (78.8) | |
| TIA | 7 (38.9) | 7 (21.2) | |
| DWI positivity | 12 (66.7) | 29 (87.9) | 0.154 |
| Single and small lesion | 10 (83.3) | 16 (55.2) | |
| Multiple or territorial lesions | 2 (16.7) | 13 (44.8) | |
| NIHSS at admission to ED in DWI positivity | <0.001 | ||
| 0 | 2 (16.7) | 3 (10.3) | |
| 1 | 11 (83.3) | 4 (13.8) | |
| 2 | 0 (0.0) | 14 (48.3) | |
| 3 | 0 (0.0) | 5 (17.2) | |
| 4 | 0 (0.0) | 3 (10.3) | |
| TOAST in DWI positivity | 0.566 | ||
| 1 | 3 (25.0) | 7 (24.1) | |
| 2 | 8 (66.7) | 15 (51.7) | |
| 3 | 0 (0.0) | 4 (13.8) | |
| 4 | 0 (0.0) | 0 (0.0) | |
| 5 | 1 (8.3) | 3 (10.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-H.; Ha, S.-O.; Kim, J.-H.; Yang, W.-S.; Park, Y.-S.; Park, T.-J. Comprehensive Assessment of Acute Isolated or Prominent Dysarthria in the Emergency Department: A Neuro-Emergency Expert’s Experience beyond Stroke. Brain Sci. 2022, 12, 1047. https://doi.org/10.3390/brainsci12081047
Lee S-H, Ha S-O, Kim J-H, Yang W-S, Park Y-S, Park T-J. Comprehensive Assessment of Acute Isolated or Prominent Dysarthria in the Emergency Department: A Neuro-Emergency Expert’s Experience beyond Stroke. Brain Sciences. 2022; 12(8):1047. https://doi.org/10.3390/brainsci12081047
Chicago/Turabian StyleLee, Soon-Ho, Sang-Ook Ha, Jin-Hyouk Kim, Won-Seok Yang, Young-Sun Park, and Tae-Jin Park. 2022. "Comprehensive Assessment of Acute Isolated or Prominent Dysarthria in the Emergency Department: A Neuro-Emergency Expert’s Experience beyond Stroke" Brain Sciences 12, no. 8: 1047. https://doi.org/10.3390/brainsci12081047