
Diffusion Tensor Imaging Radiomics for Diagnosis of Parkinson’s Disease

 , ,
, ,
Abstract
:1. Introduction
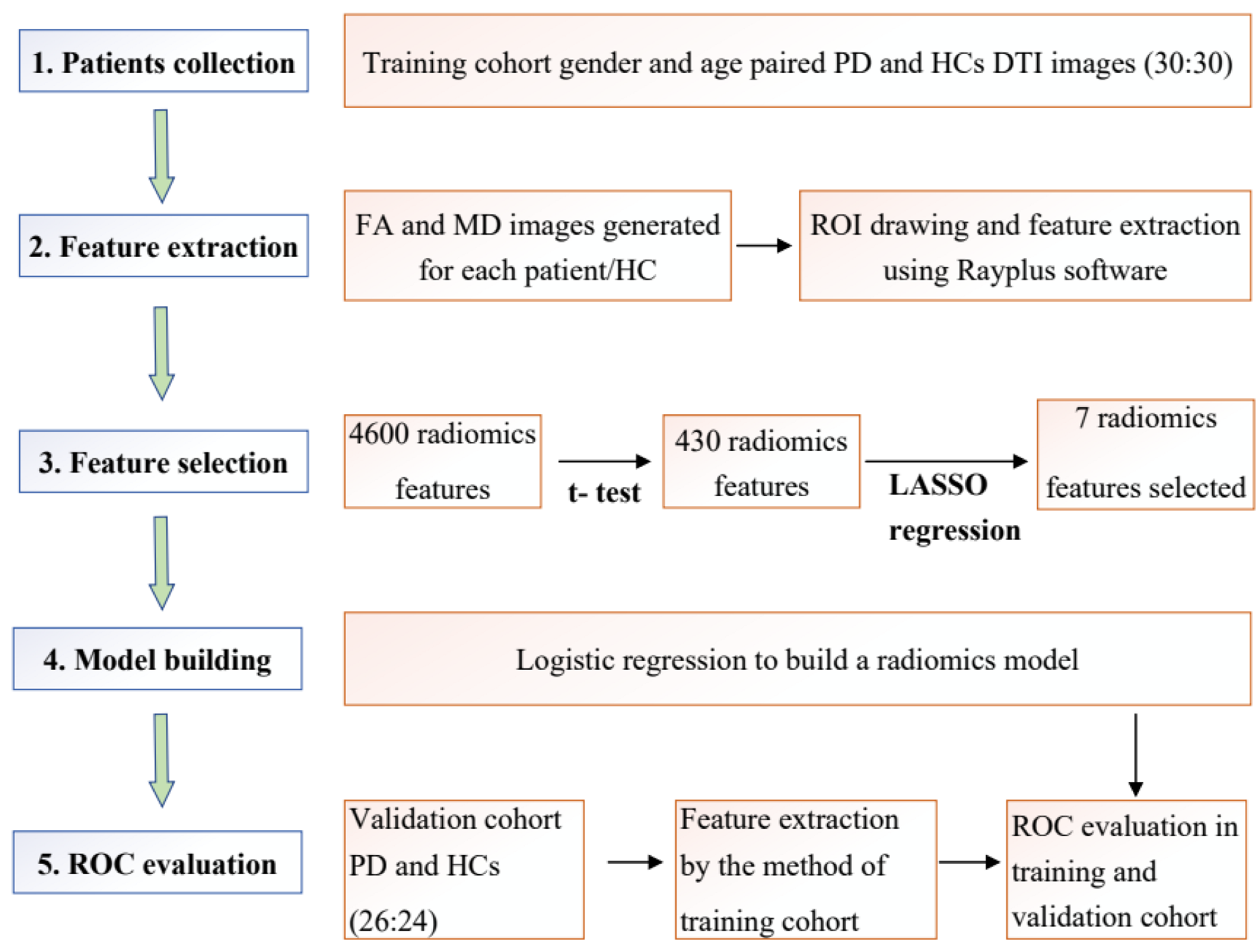
2. Methods & Materials
2.1. Patients
2.2. MRI Imaging Protocol
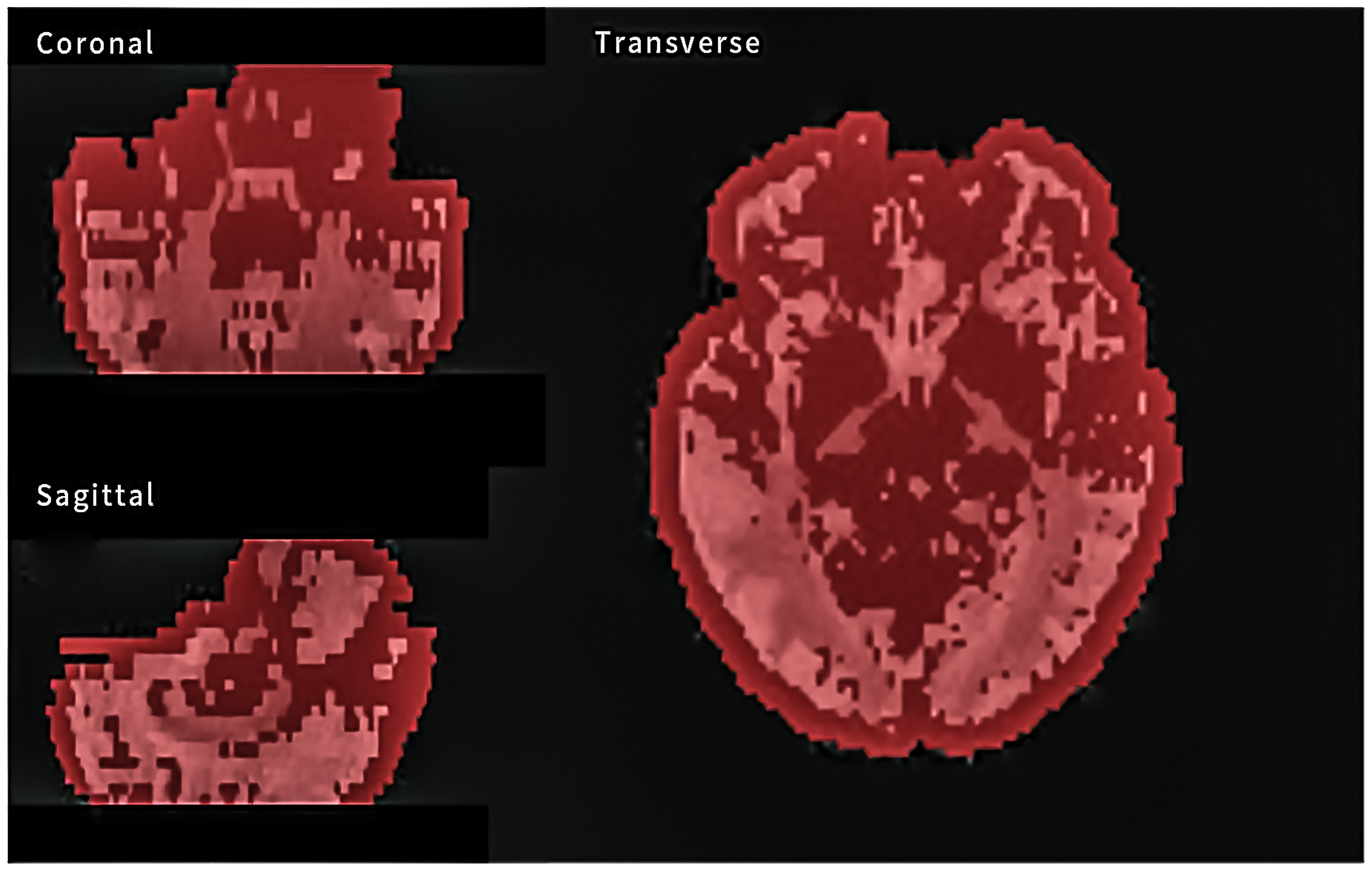
2.3. MRI Image Segmentation and Feature Extraction
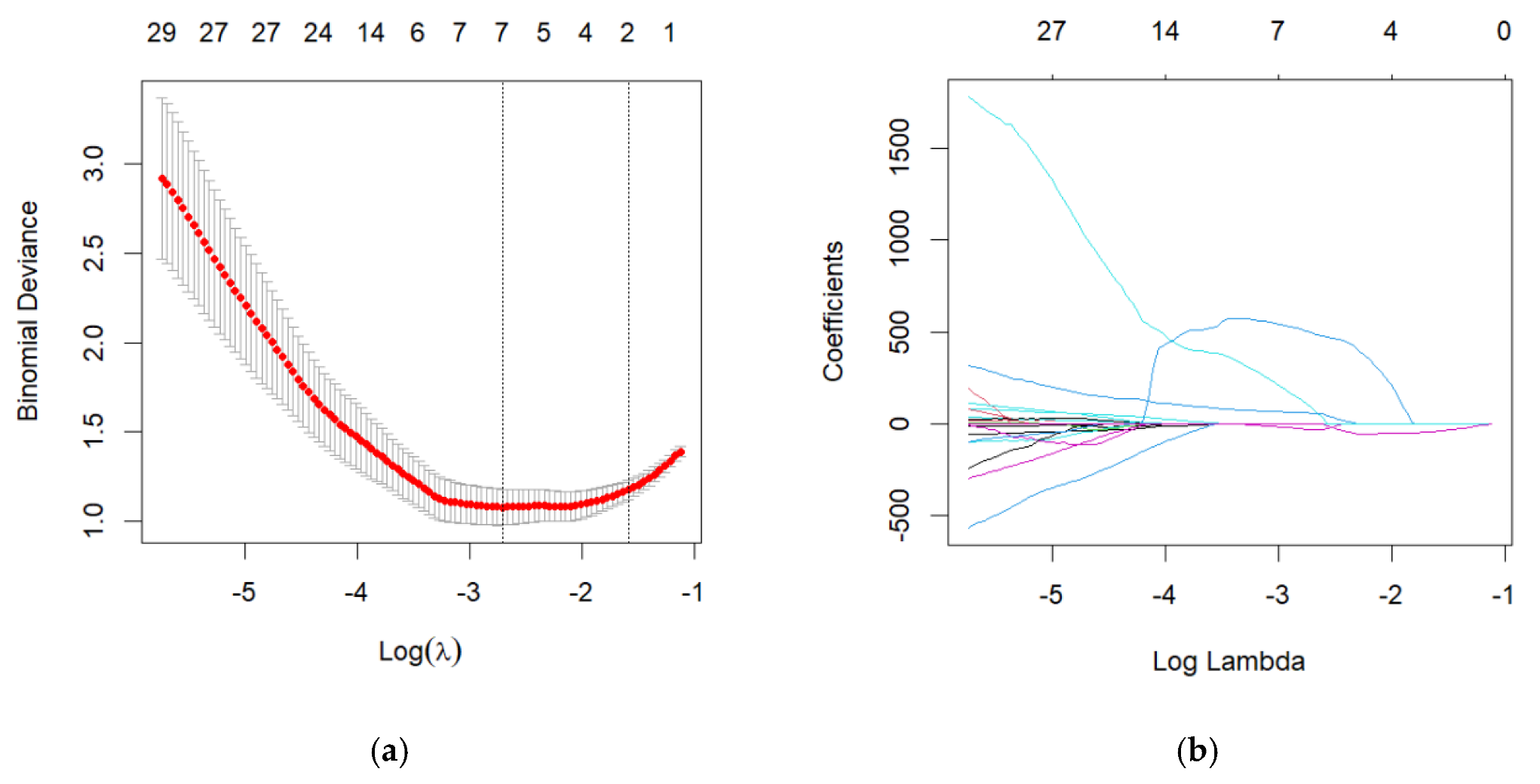
2.4. Dimensionality Reduction
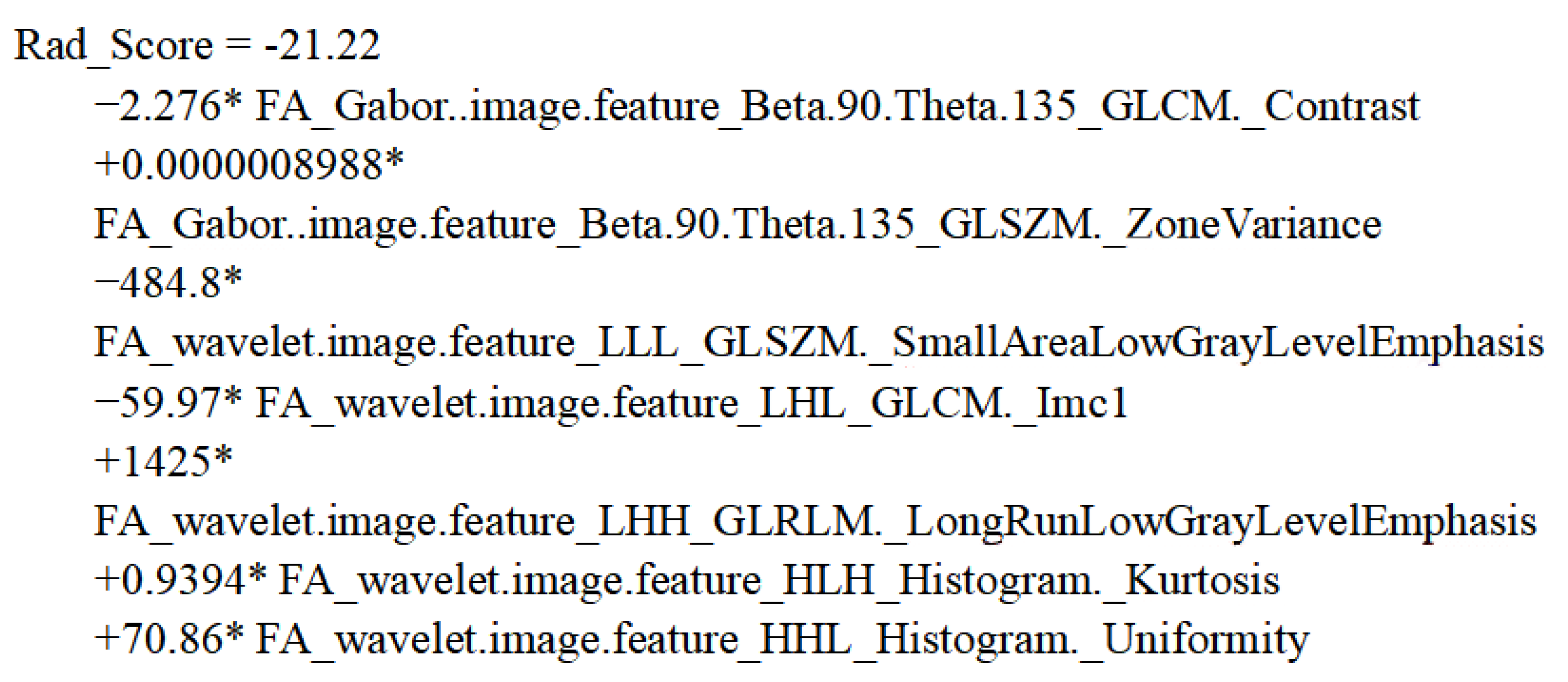
2.5. Radiomic Score Building
2.6. Statistics
3. Results
3.1. Patient Characteristics
3.2. Feature Selection
3.3. Development of the Radiomic Score
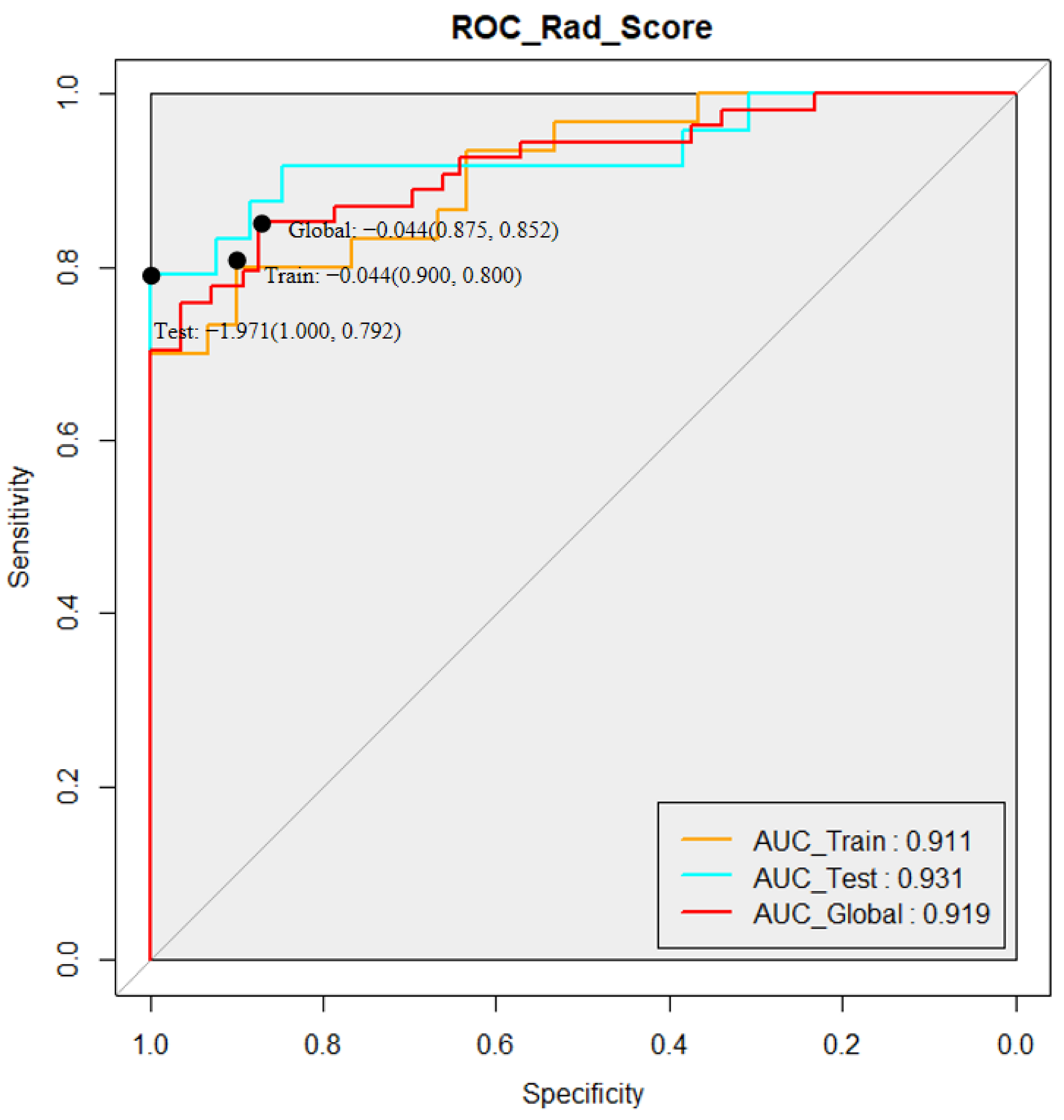
3.4. Performance of the Radiomic Model
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tolosa, E.; Wenning, G.; Poewe, W. The diagnosis of Parkinson’s disease. Lancet Neurol. 2006, 5, 75–86. [Google Scholar] [CrossRef]
- Heim, B.; Krismer, F.; De Marzi, R.; Seppi, K. Magnetic resonance imaging for the diagnosis of Parkinson’s disease. J. Neural. Transm. 2017, 124, 915–964. [Google Scholar] [CrossRef]
- Andica, C.; Kamagata, K.; Hatano, T.; Saito, Y.; Ogaki, K.; Hattori, N.; Aoki, S. MR Biomarkers of Degenerative Brain Disorders Derived From Diffusion Imaging. J. Magn. Reson. Imaging 2020, 52, 1620–1636. [Google Scholar] [CrossRef] [Green Version]
- Basser, P.J.; Mattiello, J.; LeBihan, D. MR diffusion tensor spectroscopy and imaging. Biophys. J. 1994, 66, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Shu, Z.Y.; Cui, S.J.; Wu, X.; Xu, Y.; Huang, P.; Pang, P.-P.; Zhang, M. Predicting the progression of Parkinson’s disease using conventional MRI and machine learning: An application of radiomic biomarkers in whole-brain white matter. Magn. Reson. Med. 2021, 85, 1611–1624. [Google Scholar] [CrossRef]
- Zhao, H.; Tsai, C.-C.; Zhou, M.; Liu, Y.; Chen, Y.-L.; Huang, F.; Lin, Y.-C.; Wang, J.-J. Deep learning based diagnosis of Parkinson’s Disease using diffusion magnetic resonance imaging. Brain Imaging Behav. 2022, 1–12. [Google Scholar] [CrossRef]
- Atkinson-Clement, C.; Pinto, S.; Eusebio, A.; Coulon, O. Diffusion tensor imaging in Parkinson’s disease: Review and meta-analysis. Neuroimage Clin. 2017, 16, 98–110. [Google Scholar] [CrossRef]
- Val-Laillet, D.; Aarts, E.; Weber, B.; Quaresima, V.; Stoeckel, L.E.; Alonso-Alonso, M.; Audette, M.; Malbert, C.H.; Stice, E. Neuroimaging and neuromodulation approaches to study eating behavior and prevent and treat eating disorders and obesity. Neuroimage Clin. 2015, 8, 1–31. [Google Scholar] [CrossRef]
- Meijer, F.J.; Van Rumund, A.; Tuladhar, A.M.; Aerts, M.B.; Titulaer, I.; Esselink, R.A.J.; Bloem, B.R.; Verbeek, M.; Goraj, B. Conventional 3T brain MRI and diffusion tensor imaging in the diagnostic workup of early stage parkinsonism. Neuroradiology 2015, 57, 655–669. [Google Scholar] [CrossRef] [Green Version]
- Pang, H.; Yu, Z.; Li, R.; Yang, H.; Fan, G. MRI-Based Radiomics of Basal Nuclei in Differentiating Idiopathic Parkinson’s Disease from Parkinsonian Variants of Multiple System Atrophy: A Susceptibility-Weighted Imaging Study. Front. Aging Neurosci. 2020, 12, 587250. [Google Scholar] [CrossRef]
- Shu, Z.; Pang, P.; Wu, X.; Cui, S.; Xu, Y.; Zhang, M. An Integrative Nomogram for Identifying Early-Stage Parkinson’s Disease Using Non-Motor Symptoms and White Matter-Based Radiomics Biomarkers from Whole-Brain MRI. Front. Aging Neurosci. 2020, 12, 548616. [Google Scholar] [CrossRef]
- Li, T.R.; Wu, Y.; Jiang, J.-J.; Lin, H.; Han, C.-L.; Jiang, J.-H.; Han, Y. Radiomics Analysis of Magnetic Resonance Imaging Facilitates the Identification of Preclinical Alzheimer’s Disease: An Exploratory Study. Front. Cell Dev. Biol. 2020, 8, 605734. [Google Scholar] [CrossRef]
- Liu, P.; Wang, H.; Zheng, S.; Zhang, F.; Zhang, X. Parkinson’s Disease Diagnosis Using Neostriatum Radiomic Features Based on T2-Weighted Magnetic Resonance Imaging. Front. Neurol. 2020, 11, 248. [Google Scholar] [CrossRef] [Green Version]
- Tupe-Waghmare, P.; Rajan, A.; Prasad, S.; Saini, J.; Pal, P.K.; Ingalhalikar, M. Radiomics on routine T1-weighted MRI can delineate Parkinson’s disease from multiple system atrophy and progressive supranuclear palsy. Eur. Radiol. 2021, 31, 8218–8227. [Google Scholar] [CrossRef]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef]
- Mori, S.; Zhang, J. Principles of diffusion tensor imaging and its applications to basic neuroscience research. Neuron 2006, 51, 527–539. [Google Scholar] [CrossRef] [Green Version]
- Yuan, R.; Shi, S.; Chen, J.; Cheng, G. Radiomics in RayPlus: A Web-Based Tool for Texture Analysis in Medical Images. J. Digit. Imaging 2019, 32, 269–275. [Google Scholar] [CrossRef]
- Zhang, Z.; Xiao, J.; Wu, S.; Lv, F.; Gong, J.; Jiang, L.; Yu, R.; Luo, T. Deep Convolutional Radiomic Features on Diffusion Tensor Images for Classification of Glioma Grades. J. Digit. Imaging 2020, 33, 826–837. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, T.-W.; Wu, C.-Q.; Lin, Q.; Hu, R.; Xie, C.-L.; Zuo, H.-D.; Wu, J.-L.; Mu, Q.-W.; Fu, Q.-S.; et al. Radiomics model of contrast-enhanced computed tomography for predicting the recurrence of acute pancreatitis. Eur. Radiol. 2019, 29, 4408–4417. [Google Scholar] [CrossRef]
- Huang, Y.Q.; Liang, C.-H.; He, L.; Tian, J.; Liang, C.-S.; Chen, X.; Ma, Z.-L.; Liu, Z.-Y. Development and Validation of a Radiomics Nomogram for Preoperative Prediction of Lymph Node Metastasis in Colorectal Cancer. J. Clin. Oncol. 2016, 34, 2157–2164. [Google Scholar] [CrossRef]
- Yasaka, K.; Kamagata, K.; Ogawa, T.; Hatano, T.; Takeshige-Amano, H.; Ogaki, K.; Andica, C.; Akai, H.; Kunimatsu, A.; Uchida, W.; et al. Parkinson’s disease: Deep learning with a parameter-weighted structural connectome matrix for diagnosis and neural circuit disorder investigation. Neuroradiology 2021, 63, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Mormina, E.; Arrigo, A.; Calamuneri, A.; Granata, F.; Quartarone, A.; Ghilardi, M.F.; Inglese, M.; Di Rocco, A.; Milardi, D.; Anastasi, G.P.; et al. Diffusion tensor imaging parameters’ changes of cerebellar hemispheres in Parkinson’s disease. Neuroradiology 2015, 57, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Chan, L.-L.; Rumpel, H.; Yap, K.; Lee, E.; Loo, H.-V.; Fook-Chong, S.; Yuen, Y.; Tan, E.-K. Case control study of diffusion tensor imaging in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2007, 78, 1383–1386. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Liu, X.; Wang, X.; Hu, Y.; Zeng, Q.; Lin, Z.; Xiong, N.; Feng, Y. Alterations of white matter tracts and topological properties of structural networks in hemifacial spasm. NMR Biomed. 2022, e4756. [Google Scholar] [CrossRef]
- Park, Y.W.; An, C.; Lee, J.; Han, K.; Choi, D.; Ahn, S.S.; Kim, H.; Chang, J.H.; Kim, S.H.; Lee, S.-K. Diffusion tensor and postcontrast T1-weighted imaging radiomics to differentiate the epidermal growth factor receptor mutation status of brain metastases from non-small cell lung cancer. Neuroradiology 2021, 63, 343–352. [Google Scholar] [CrossRef]
- Borkowski, K.; Krzyzak, A.T. Analysis and correction of errors in DTI-based tractography due to diffusion gradient inhomogeneity. J. Magn. Reson. 2018, 296, 5–11. [Google Scholar] [CrossRef]
- Borkowski, K.; Krzyzak, A.T. Assessment of the systematic errors caused by diffusion gradient inhomogeneity in DTI-computer simulations. NMR Biomed. 2019, 32, e4130. [Google Scholar] [CrossRef]
- Borkowski, K.; Kłodowski, K.; Figiel, H.; Krzyżak, A.T. A theoretical validation of the B-matrix spatial distribution approach to diffusion tensor imaging. Magn. Reson. Imaging 2017, 36, 1–6. [Google Scholar] [CrossRef]
- Klodowski, K.; Krzyzak, A.T. Innovative anisotropic phantoms for calibration of diffusion tensor imaging sequences. Magn. Reson. Imaging 2016, 34, 404–409. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Train Cohort | Test Cohort | HC-Train vs. PD-Train p Value | |||||
|---|---|---|---|---|---|---|---|
| PD (30) | HC (30) | All (60) | PD (26) | HC (24) | All (50) | ||
| Age (years, mean ± SD) | 57.78 ± 7.68 | 57.69 ± 7.72 | 57.83 ± 7.63 | 65.12 ± 12.54 | 38.71 ± 11.26 | 52.44 ± 17.79 | 0.2717 |
| Gender (male/female) | 15/15 | 14/16 | 29/31 | 17/9 | 12/12 | 29/21 | >0.999 |
| UPDRS | 29.87 ± 14.62 | / | / | 32.75 ± 17.36 | / | / | / |
| H&Y stage | 1.83 ± 0.77 | / | / | 2 ± 0.71 | / | / | / |
| Feature | Maps | Source | Algorithm | Class | Feature | Equation |
|---|---|---|---|---|---|---|
| No.172 | FA | Gabor | Beta.90.Theta.135 | GLCM | Contrast | |
| No.191 | FA | Gabor | Beta.90.Theta.135 | GLSZM | ZoneVariance | |
| No.242 | FA | wavelet | LLL | GLSZM | SmallAreaLowGrayLevelEmphasis | |
| No.297 | FA | wavelet | LHL | GLCM | lmc1 | |
| No.320 | FA | wavelet | LHH | GLRLM | LongRunLowGrayLevelEmphasis | |
| No.360 | FA | wavelet | HLH | Histogram | Kurtosis | |
| No.391 | FA | wavelet | HHL | Histogram | Uniformity |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.; Liu, X.; Wang, X.; Liu, H.; Lin, Z.; Xiong, N. Diffusion Tensor Imaging Radiomics for Diagnosis of Parkinson’s Disease. Brain Sci. 2022, 12, 851. https://doi.org/10.3390/brainsci12070851
Li J, Liu X, Wang X, Liu H, Lin Z, Xiong N. Diffusion Tensor Imaging Radiomics for Diagnosis of Parkinson’s Disease. Brain Sciences. 2022; 12(7):851. https://doi.org/10.3390/brainsci12070851
Chicago/Turabian StyleLi, Jingwen, Xiaoming Liu, Xinyi Wang, Hanshu Liu, Zhicheng Lin, and Nian Xiong. 2022. "Diffusion Tensor Imaging Radiomics for Diagnosis of Parkinson’s Disease" Brain Sciences 12, no. 7: 851. https://doi.org/10.3390/brainsci12070851