
High Myoinositol on Proton MR Spectroscopy Could Be a Potential Signature of Papillary Tumors of the Pineal Region—Case Report of Two Patients

 , and
, and 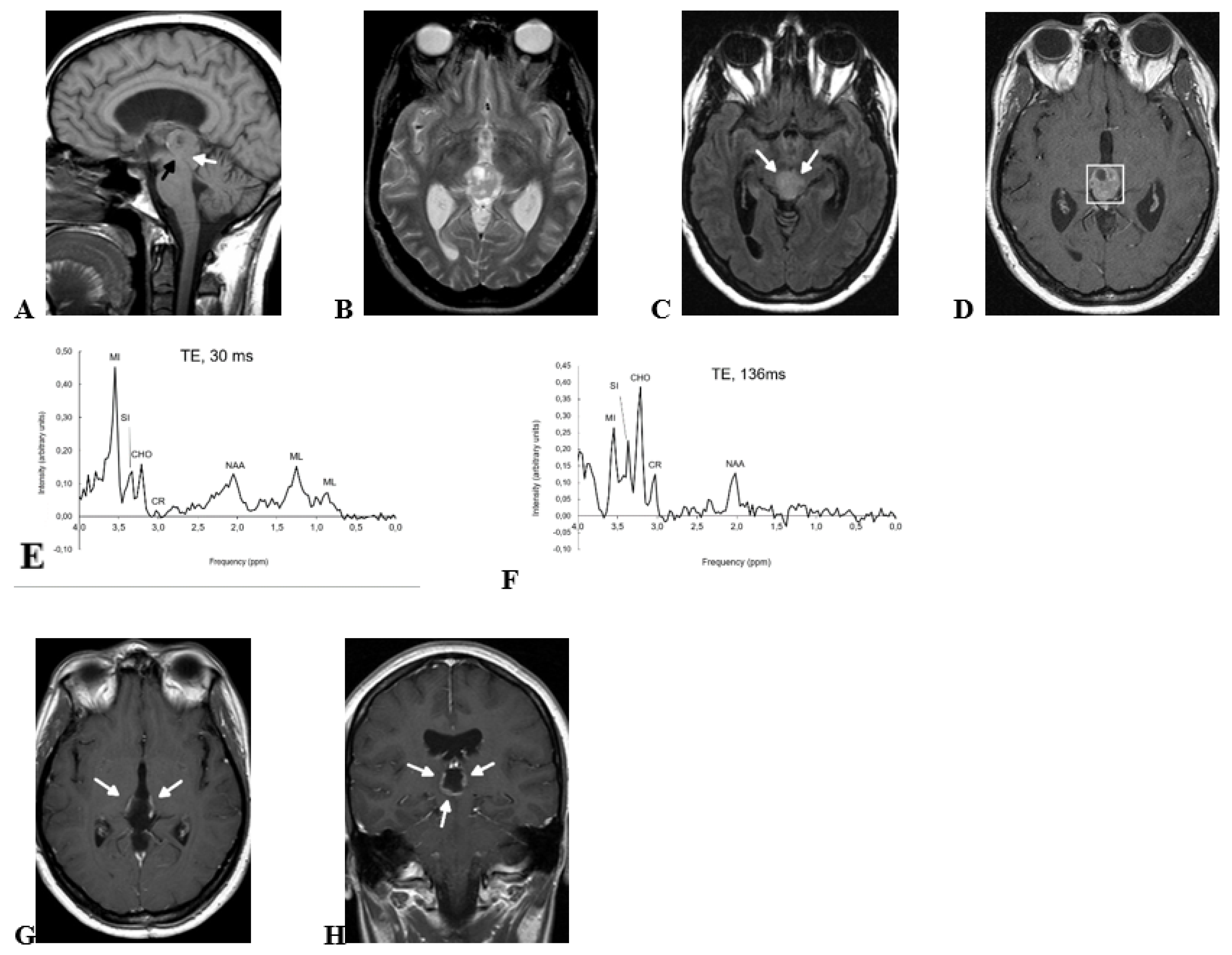{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Report
2.1. Case 1
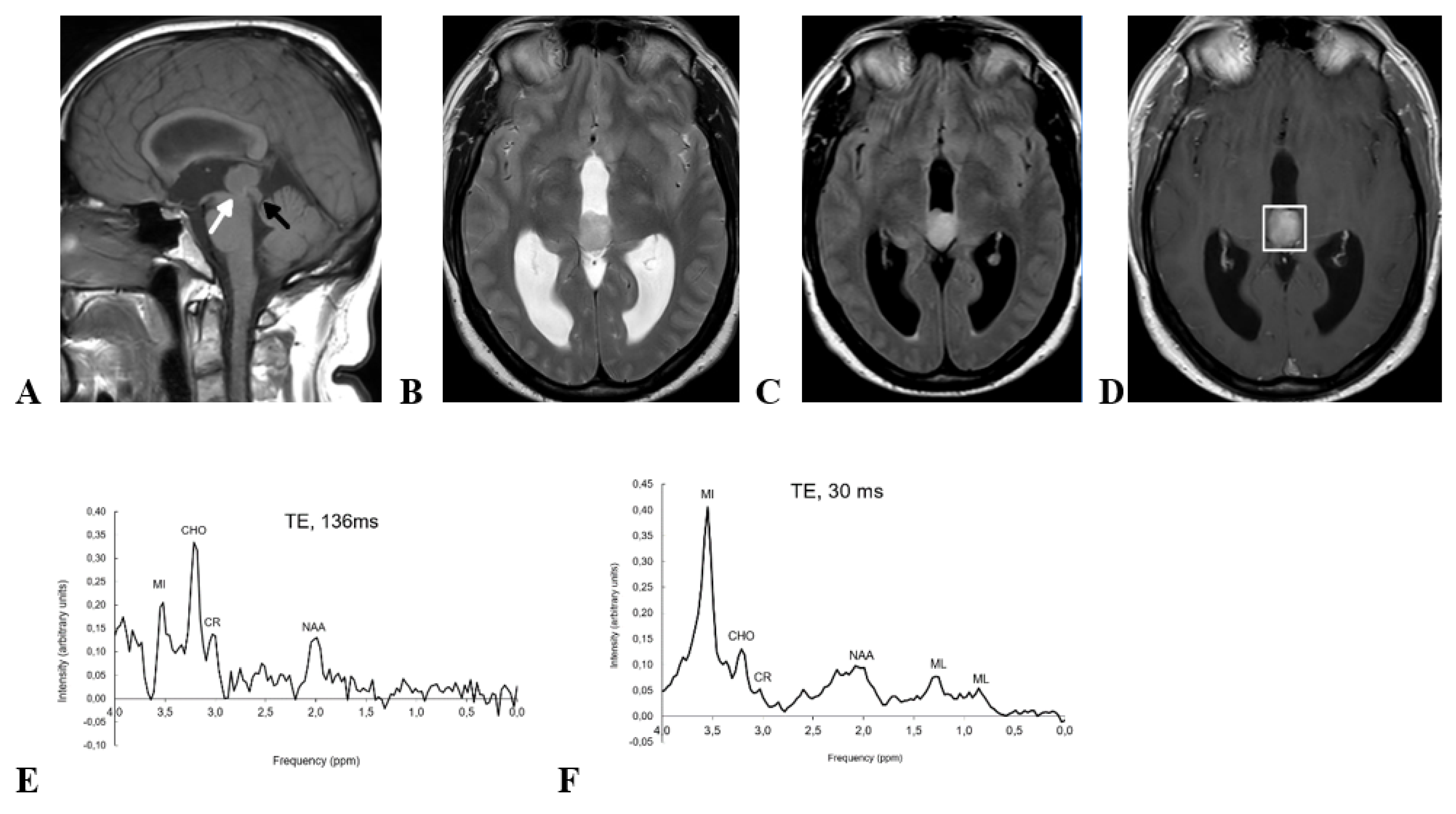
2.2. Case 2
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
References
- Hirato, J.; Nakazato, Y. Pathology of pineal region tumors. J. Neurooncol. 2001, 54, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Jouvet, A.; Fauchon, F.; Liberski, P.; Saint-Pierre, G.; Didier-Bazes, M.; Heitzmann, A.; Delisle, M.B.; Biassette, H.A.; Vincent, S.; Mikol, J.; et al. Papillary Tumor of the Pineal Region. Am. J. Surg. Pathol. 2003, 27, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Ohgaki, H.; Wiestler, O.D.; Cavenee, W.K.; Burger, P.C.; Jouvet, A.; Scheithauer, B.W.; Kleihues, P. The 2007 WHO Classification of Tumours of the Central Nervous System. Acta Neuropathol. 2007, 114, 97–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Classification of Tumours Editorial Board. World Health Organization Classification of Tumours of the Central Nervous System, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2021.
- Yamaki, V.N.; Solla, D.J.F.; Ribeiro, R.R.; da Silva, S.A.; Teixeira, M.J.; Figueiredo, E.G. Papillary Tumor of the Pineal Region: Systematic Review and Analysis of Prognostic Factors. Clin. Neurosurg. 2019, 85, E420–E429. [Google Scholar] [CrossRef] [PubMed]
- Mathkour, M.; Hanna, J.; Ibrahim, N.; Scullen, T.; Kilgore, M.D.; Werner, C.; Cormier, I.; Spencer, P.; Keen, J.R.; Bui, C.J. Papillary tumor of the pineal region in pediatric populations: An additional case and systematic review of a rare tumor entity. Clin. Neurol. Neurosurg. 2021, 201, 106404. [Google Scholar] [CrossRef] [PubMed]
- Fang, A.S.; Meyers, S.P. Magnetic resonance imaging of pineal region tumours. Insights Imaging 2013, 4, 369–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaghela, V.; Radhakrishnan, N.; Radhakrishnan, V.V.; Menon, G.; Kesavadas, C.; Thomas, B. Advanced magnetic resonance imaging with histopathological correlation in papillary tumor of pineal region: Report of a case and review of literature. Neurol. India 2010, 58, 928–932. [Google Scholar] [PubMed]
- Tate, A.R.; Underwood, J.; Acosta, D.M.; Julià-Sapé, M.; Majós, C.; Moreno-Torres, A.; Howe, F.A.; van der Graaf, M.; Lefournier, V.; Murphy, M.M.; et al. Development of a decision support system for diagnosis and grading of brain tumours using in vivo magnetic resonance single voxel spectra. NMR Biomed. 2006, 19, 411–434. [Google Scholar] [CrossRef] [PubMed]
- Barba, I.; Moreno, A.; Martínez-Pérez, I.; Tate, A.R.; Cabañas, M.E.; Baquero, M.; Capdevila, A.; Arús, C. Magnetic resonance spectroscopy of brain hemangiopericytomas: High myoinositol concentrations and discrimination from meningiomas. J. Neurosurg. 2001, 94, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Heim, S.; Sill, M.; Jones, D.T.W.; Vasiljevic, A.; Jouvet, A.; Fèvre-Montange, M.; Wesseling, P.; Beschorner, R.; Mittelbronn, M.; Kohlhof, P.; et al. Papillary tumor of the pineal region: A distinct molecular entity. Brain Pathol. 2016, 26, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Castillo, M.; Smith, J.K.; Kwock, L. Correlation of myo-inositol levels and grading of cerebral astrocytomas. AJNR Am. J. Neuroradiol. 2000, 21, 1645–1649. [Google Scholar] [PubMed]
- Bulik, M.; Jancalek, R.; Vanicek, J.; Skoch, A.; Mechl, M. Potential of MR spectroscopy for assessment of glioma grading. Clin. Neurol. Neurosurg. 2013, 115, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Stadlbauer, A.; Gruber, S.; Nimsky, C.; Fahlbusch, R.; Hammen, T.; Buslei, R.; Tomandl, B.; Moser, E.; Ganslandt, O. Preoperative grading of gliomas by using metabolite quantification with high-spatial-resolution proton MR spectroscopic imaging. Radiology 2006, 238, 958–969. [Google Scholar] [CrossRef] [PubMed]
- Nakae, S.; Murayama, K.; Sasaki, H.; Kumon, M.; Nishiyama, Y.; Ohba, S.; Adachi, K.; Nagahisa, S.; Hayashi, T.; Inamasu, J.; et al. Prediction of genetic subgroups in adult supra tentorial gliomas by pre- and intraoperative parameters. J. Neurooncol. 2017, 131, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Kumon, M.; Nakae, S.; Murayama, K.; Kato, T.; Ohba, S.; Inamasu, J.; Yamada, S.; Abe, M.; Sasaki, H.; Ohno, Y.; et al. Myoinositol to Total Choline Ratio in Glioblastomas as a Potential Prognostic Factor in Preoperative Magnetic Resonance Spectroscopy. Neurol. Med. Chir. (Tokyo) 2021, 61, 453–460. [Google Scholar] [CrossRef]
- Majós, C.; Aguilera, C.; Alonso, J.; Julià-Sapé, M.; Castañer, S.; Sanchez, J.J.; Samitier, A.; León, A.; Rovira, A.; Arús, C. Proton MR Spectroscopy Improves Discrimination between Tumor and Pseudotumoral Lesion in Solid Brain Masses. Am. J. Neuroradiol. 2009, 30, 544–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, G.; Sun, B.; Wu, Z.; Guo, Q.; Guo, Y. In vivo single-voxel proton MR spectroscopy in the differentiation of high-grade gliomas and solitary metastases. Clin. Radiol. 2004, 59, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Mora, P.; Pons, A.; Cos, M.; Camins, A.; Muntané, A.; Aguilera, C.; Arús, C.; Majós, C. Magnetic resonance spectroscopy in posterior fossa tumours: The tumour spectroscopic signature may improve discrimination in adults among haemangioblastoma, ependymal tumours, medulloblastoma, and metastasis. Eur. Radiol. 2019, 29, 2792–2801. [Google Scholar] [CrossRef] [PubMed]
- Tamrazi, B.; Nelson, M.; Blüml, S. Pineal Region Masses in Pediatric Patients. Neuroimaging Clin. N Am. 2017, 27, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Harris, L.M.; Davies, N.; Wilson, S.; MacPherson, L.; Natarajan, K.; English, M.W.; Brundler, M.-A.; Arvanitis, T.; Grundy, R.G.; Peet, A.C. Short echo time single voxel 1H magnetic resonance spectroscopy in the diagnosis and characterisation of pineal tumours in children. Pediatr. Blood Cancer 2011, 57, 972–977. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pons-Escoda, A.; Sánchez Fernández, J.J.; de Vilalta, À.; Vidal, N.; Majós, C. High Myoinositol on Proton MR Spectroscopy Could Be a Potential Signature of Papillary Tumors of the Pineal Region—Case Report of Two Patients. Brain Sci. 2022, 12, 802. https://doi.org/10.3390/brainsci12060802
Pons-Escoda A, Sánchez Fernández JJ, de Vilalta À, Vidal N, Majós C. High Myoinositol on Proton MR Spectroscopy Could Be a Potential Signature of Papillary Tumors of the Pineal Region—Case Report of Two Patients. Brain Sciences. 2022; 12(6):802. https://doi.org/10.3390/brainsci12060802
Chicago/Turabian StylePons-Escoda, Albert, Juan Jose Sánchez Fernández, Àlex de Vilalta, Noemí Vidal, and Carles Majós. 2022. "High Myoinositol on Proton MR Spectroscopy Could Be a Potential Signature of Papillary Tumors of the Pineal Region—Case Report of Two Patients" Brain Sciences 12, no. 6: 802. https://doi.org/10.3390/brainsci12060802