
NAA/Glu Ratio Associated with Suicidal Ideation in Pilot Sample of Autistic Youth and Young Adults

 , ,
, ,
Abstract
:1. Introduction
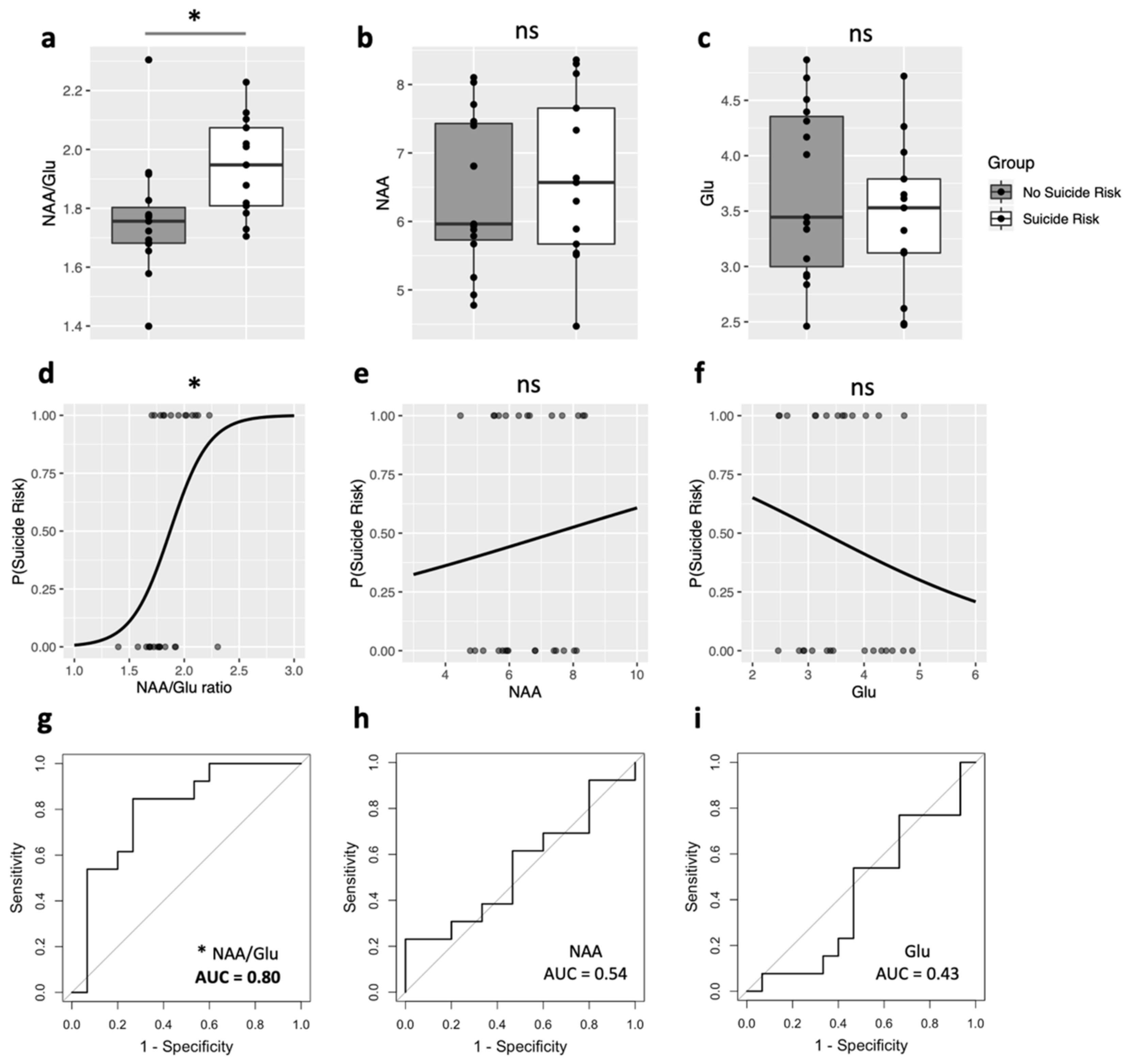
2. Results
3. Discussion
4. Materials and Methods
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blanchard, A.; Chihuri, S.; DiGuiseppi, C.G.; Li, G. Risk of Self-harm in Children and Adults With Autism Spectrum Disorder: A Systematic Review and Meta-analysis. JAMA Netw. Open 2021, 4, e2130272. [Google Scholar] [CrossRef] [PubMed]
- Mishara, B.L.; Stijelja, S. Trends in US Suicide Deaths, 1999 to 2017, in the Context of Suicide Prevention Legislation. JAMA Pediatr. 2020, 174, 499–500. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Preventing Suicide: A Global Imperative; WHO Press: Geneva, Switzerland, 2014. [Google Scholar]
- Mann, J.J.; Rizk, M.M. A Brain-Centric Model of Suicidal Behavior. Am. J. Psychiatry 2020, 177, 902–916. [Google Scholar] [CrossRef] [PubMed]
- Oquendo, M.A.; Sullivan, G.M.; Sudol, K.; Baca-Garcia, E.; Stanley, B.H.; Sublette, M.E.; Mann, J.J. Toward a biosignature for suicide. Am. J. Psychiatry 2014, 171, 1259–1277. [Google Scholar] [CrossRef] [PubMed]
- Bittšanský, M.; Výbohová, D.; Dobrota, D. Proton magnetic resonance spectroscopy and its diagnostically important metabolites in the brain. Gen. Physiol. Biophys. 2012, 31, 101–112. [Google Scholar] [CrossRef] [Green Version]
- Jollant, F.; Near, J.; Turecki, G.; Richard-Devantoy, S. Spectroscopy markers of suicidal risk and mental pain in depressed patients. Prog. Neuropsychopharmacol. Biol. Psychiatry 2016, 73, 64–71. [Google Scholar] [CrossRef]
- Clark, J.F.; Doepke, A.; Filosa, J.A.; Wardle, R.L.; Lu, A.; Meeker, T.J.; Pyne-Geithman, G.J. N-acetylaspartate as a reservoir for glutamate. Med. Hypotheses 2006, 67, 506–512. [Google Scholar] [CrossRef]
- Lewis, C.P.; Port, J.D.; Blacker, C.J.; Sonmez, A.I.; Seewoo, B.J.; Leffler, J.M.; Frye, M.A.; Croarkin, P.E. Altered anterior cingulate glutamatergic metabolism in depressed adolescents with current suicidal ideation. Transl. Psychiatry 2020, 10, 119. [Google Scholar] [CrossRef]
- Ajram, L.A.; Pereira, A.C.; Durieux, A.M.S.; Velthius, H.E.; Petrinovic, M.M.; McAlonan, G.M. The contribution of [1H] magnetic resonance spectroscopy to the study of excitation-inhibition in autism. Prog. Neuropsychopharmacol. Biol. Psychiatry 2019, 89, 236–244. [Google Scholar] [CrossRef]
- Ford, T.C.; Crewther, D.P. A Comprehensive Review of the (1)H-MRS Metabolite Spectrum in Autism Spectrum Disorder. Front. Mol. Neurosci. 2016, 9, 14. [Google Scholar] [CrossRef] [Green Version]
- Trakoshis, S.; Martínez-Cañada, P.; Rocchi, F.; Canella, C.; You, W.; Chakrabarti, B.; Ruigrok, A.N.; Bullmore, E.T.; Suckling, J.; Markicevic, M.; et al. Intrinsic excitation-inhibition imbalance affects medial prefrontal cortex differently in autistic men versus women. eLife 2020, 9, e55684. [Google Scholar] [CrossRef]
- Moriguchi, S.; Takamiya, A.; Noda, Y.; Horita, N.; Wada, M.; Tsugawa, S.; Plitman, E.; Sano, Y.; Tarumi, R.; ElSalhy, M.; et al. Glutamatergic neurometabolite levels in major depressive disorder: A systematic review and meta-analysis of proton magnetic resonance spectroscopy studies. Mol. Psychiatry 2019, 24, 952–964. [Google Scholar] [CrossRef] [Green Version]
- Martens, L.; Herrmann, L.; Colic, L.; Li, M.; Richter, A.; Behnisch, G.; Stork, O.; Seidenbecher, C.; Schott, B.H.; Walter, M. Met Carriers of the BDNF Val66Met Polymorphism Show Reduced Glx/NAA in the Pregenual ACC in Two Independent Cohorts. Sci. Rep. 2021, 11, 6742. [Google Scholar] [CrossRef]
- Moxon-Emre, I.; Daskalakis, Z.J.; Blumberger, D.M.; Croarkin, P.E.; Lyon, R.E.; Forde, N.J.; Tani, H.; Truong, P.; Lai, M.-C.; Desarkar, P.; et al. Modulation of Dorsolateral Prefrontal Cortex Glutamate/Glutamine Levels Following Repetitive Transcranial Magnetic Stimulation in Young Adults With Autism. Front. Neurosci. 2021, 15, 711542. [Google Scholar] [CrossRef]
- Croarkin, P.E.; Nakonezny, P.A.; Wall, C.A.; Murphy, L.L.; Sampson, S.M.; Frye, M.A.; Port, J.D. Transcranial magnetic stimulation potentiates glutamatergic neurotransmission in depressed adolescents. Psychiatry Res. Neuroimaging 2016, 247, 25–33. [Google Scholar] [CrossRef] [Green Version]
- Dlabac-de Lange, J.J.; Liemburg, E.J.; Bais, L.; van de Poel-Mustafayeva, A.T.; de Lange-de Klerk, E.S.M.; Knegtering, H.; Aleman, A. Effect of Bilateral Prefrontal rTMS on Left Prefrontal NAA and Glx Levels in Schizophrenia Patients with Predominant Negative Symptoms: An Exploratory Study. Brain Stimul. 2017, 10, 59–64. [Google Scholar] [CrossRef]
- Luborzewski, A.; Schubert, F.; Seifert, F.; Danker-Hopfe, H.; Brakemeier, E.-L.; Schlattmann, P.; Anghelescu, I.; Colla, M.; Bajbouj, M. Metabolic alterations in the dorsolateral prefrontal cortex after treatment with high-frequency repetitive transcranial magnetic stimulation in patients with unipolar major depression. J. Psychiatr. Res. 2007, 41, 606–615. [Google Scholar] [CrossRef]
- Zheng, H.; Jia, F.; Guo, G.; Quan, D.; Li, G.; Wu, H.; Zhang, B.; Fan, C.; He, X.; Huang, H. Abnormal Anterior Cingulate N-Acetylaspartate and Executive Functioning in Treatment-Resistant Depression After rTMS Therapy. Int. J. Neuropsychopharmacol. 2015, 18, yv059. [Google Scholar] [CrossRef]
- Ameis, S.H.; Daskalakis, Z.J.; Blumberger, D.M.; Desarkar, P.; Drmic, I.; Mabbott, D.J.; Lai, M.-C.; Croarkin, P.E.; Szatmari, P. Repetitive Transcranial Magnetic Stimulation for the Treatment of Executive Function Deficits in Autism Spectrum Disorder: Clinical Trial Approach. J. Child Adolesc. Psychopharmacol. 2017, 27, 413–421. [Google Scholar] [CrossRef]
- Ameis, S.H.; Blumberger, D.M.; Croarkin, P.E.; Mabbott, D.J.; Lai, M.-C.; Desarkar, P.; Szatmari, P.; Daskalakis, Z.J. Treatment of Executive Function Deficits in autism spectrum disorder with repetitive transcranial magnetic stimulation: A double-blind, sham-controlled, pilot trial. Brain Stimul. 2020, 13, 539–547. [Google Scholar] [CrossRef] [Green Version]
- Lord, C.; Risi, S.; Lambrecht, L.; Cook, E.H.; Leventhal, B.L.; DiLavore, P.C.; Pickles, A.; Rutter, M. The Autism Diagnostic Observation Schedule—Generic: A Standard Measure of Social and Communication Deficits Associated with the Spectrum of Autism. J. Autism. Dev. Disord. 2000, 30, 205–223. [Google Scholar] [CrossRef] [PubMed]
- Gioia, G.A.; Isquith, P.K.; Retzlaff, P.D.; Espy, K.A. Confirmatory factor analysis of the Behavior Rating Inventory of Executive Function (BRIEF) in a clinical sample. Child Neuropsychol. 2002, 8, 249–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benson, N.; Hulac, D.M.; Kranzler, J.H. Independent examination of the Wechsler Adult Intelligence Scale—Fourth Edition (WAIS-IV): What does the WAIS-IV measure? Psychol. Assess. 2010, 22, 121–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (MINI): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59, 22–33. [Google Scholar]
- Sheehan, D.V.; Sheehan, K.H.; Shytle, R.D.; Janavs, J.; Bannon, Y.; Rogers, J.E.; Milo, K.M.; Stock, S.L.; Wilkinson, B. Reliability and validity of the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID). J. Clin. Psychiatry 2010, 71, 313–326. [Google Scholar] [CrossRef]
- Baeken, C.; Lefaucheur, J.-P.; Van Schuerbeek, P. The Impact of Accelerated High Frequency rTMS on Brain Neurochemicals in Treatment-Resistant Depression: Insights from 1H MR Spectroscopy. Clin. Neurophysiol. 2017, 128, 1664–1672. [Google Scholar] [CrossRef]
- Dubin, M.J.; Mao, X.; Banerjee, S.; Goodman, Z.; Lapidus, K.A.B.; Kang, G.; Liston, C.; Shungu, D.C. Elevated Prefrontal Cortex GABA in Patients with Major Depressive Disorder after TMS Treatment Measured with Proton Magnetic Resonance Spectroscopy. J. Psychiatry Neurosci. 2016, 41, E37–E45. [Google Scholar] [CrossRef] [Green Version]
- Levitt, J.G.; Kalender, G.; O’Neill, J.; Diaz, J.P.; Cook, I.A.; Ginder, N.; Krantz, D.; Minzenberg, M.J.; Vince-Cruz, N.; Nguyen, L.D.; et al. Dorsolateral Prefrontal γ-Aminobutyric Acid in Patients with Treatment-Resistant Depression after Transcranial Magnetic Stimulation Measured with Magnetic Resonance Spectroscopy. J. Psychiatry Neurosci. 2019, 44, 386–394. [Google Scholar] [CrossRef] [Green Version]
- Michael, N.; Gösling, M.; Reutemann, M.; Kersting, A.; Heindel, W.; Arolt, V.; Pfleiderer, B. Metabolic Changes after Repetitive Transcranial Magnetic Stimulation (rTMS) of the Left Prefrontal Cortex: A Sham-Controlled Proton Magnetic Resonance Spectroscopy (1H MRS) Study of Healthy Brain. Eur. J. Neurosci. 2003, 17, 2462–2468. [Google Scholar] [CrossRef]
- Zheng, H.; Zhang, L.; Li, L.; Liu, P.; Gao, J.; Liu, X.; Zou, J.; Zhang, Y.; Liu, J.; Zhang, Z.; et al. High-Frequency rTMS Treatment Increases Left Prefrontal Myo-Inositol in Young Patients with Treatment-Resistant Depression. Prog. Neuropsychopharmacol. Biol. Psychiatry 2010, 34, 1189–1195. [Google Scholar] [CrossRef]
- Edden, R.A.E.; Puts, N.A.J.; Harris, A.D.; Barker, P.B.; John Evans, C. Gannet: A batch-processing tool for the quantitative analysis of gamma-aminobutyric acid-edited MR spectroscopy spectra. J. Magn. Reson. Imaging 2014, 40, 1445–1452. [Google Scholar] [CrossRef]
- Simpson, R.; Devenyi, G.A.; Jezzard, P.; Jay Hennessy, T.; Near, J. Advanced processing and simulation of MRS data using the FID appliance (FID-A)—An open source, MATLAB-based toolkit. Mag. Reson. Med. 2017, 77, 23–33. [Google Scholar] [CrossRef]
- Provencher, S.W. Automatic quantitation of localized in vivo 1H spectra with LCModel. NMR Biomed. 2001, 14, 260–264. [Google Scholar] [CrossRef]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.-C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef]


{kind=link}
| Suicidal Ideation (SI+) | No Suicidal Ideation (SI−) | ||
|---|---|---|---|
| (n = 13) | (n = 15) | U | |
| Age | |||
| Mean (SD) | 23.4 (5.19) | 23.1 (4.39) | |
| Median [Min, Max] | 25.0 [16.0, 33.0] | 21.0 [17.0, 31.0] | 0.98 |
| Sex | |||
| Number of males (%) | 8 (61.5%) | 13 (86.7%) | 0.20 |
| Psychotropic Medication * | |||
| Number of participants (%) | 7 (53.8%) | 10 (66.7%) | 0.70 |
| MINI | |||
| Comorbidity—other than suicide ** | |||
| Number of participants (%) | 11 (84.6%) | 3 (20.0%) | 0.002 |
| Suicide risk level *** | |||
| Low | 7 (53.8%) | - | |
| Moderate | 5 (38.5%) | - | |
| High | 1 (7.7%) | - | |
| Depression, current (2 weeks) | |||
| Number of participants (%) | 6 (46.2%) | 1 (6.7%) | 0.03 |
| Depression, recurrent | |||
| Number of participants (%) | 2 (15.4%) | 0 (0%) | 0.21 |
| Years of Education | |||
| Mean (SD) | 13.4 (2.40) | 14.9 (3.37) | 0.24 |
| Median [Min, Max] | 13.0 [10.0, 17.0] | 14.0 [11.0, 22.0] | |
| IQ—General Abilities Index | |||
| Mean (SD) | 113 (17.9) | 111 (18.3) | |
| Median [Min, Max] | 113 [77.0, 140] | 104 [79.0, 141] | 0.70 |
| BRIEF Metacognition Index | |||
| Mean (SD) | 70.2 (7.76) | 71.0 (8.83) | |
| Median [Min, Max] | 69.0 [59.0, 84.0] | 68.0 [59.0, 84.0] | 0.89 |
| BRIEF Global Composite | |||
| Mean (SD) | 67.3 (8.64) | 68.7 (8.00) | 0.70 |
| Median [Min, Max] | 67.0 [52.0, 82.0] | 66.0 [60.0, 86.0] | |
| Adaptive Functioning Composite | |||
| Mean (SD) | 75.9 (12.3) | 75.2 (7.61) | 0.87 |
| Median [Min, Max] | 79.0 [58.0, 104] | 73.0 [61.0, 89.0] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moxon-Emre, I.; Croarkin, P.E.; Daskalakis, Z.J.; Blumberger, D.M.; Lyon, R.E.; Tani, H.; Truong, P.; Lai, M.-C.; Desarkar, P.; Sailasuta, N.; et al. NAA/Glu Ratio Associated with Suicidal Ideation in Pilot Sample of Autistic Youth and Young Adults. Brain Sci. 2022, 12, 785. https://doi.org/10.3390/brainsci12060785
Moxon-Emre I, Croarkin PE, Daskalakis ZJ, Blumberger DM, Lyon RE, Tani H, Truong P, Lai M-C, Desarkar P, Sailasuta N, et al. NAA/Glu Ratio Associated with Suicidal Ideation in Pilot Sample of Autistic Youth and Young Adults. Brain Sciences. 2022; 12(6):785. https://doi.org/10.3390/brainsci12060785
Chicago/Turabian StyleMoxon-Emre, Iska, Paul E. Croarkin, Zafiris J. Daskalakis, Daniel M. Blumberger, Rachael E. Lyon, Hideaki Tani, Peter Truong, Meng-Chuan Lai, Pushpal Desarkar, Napapon Sailasuta, and et al. 2022. "NAA/Glu Ratio Associated with Suicidal Ideation in Pilot Sample of Autistic Youth and Young Adults" Brain Sciences 12, no. 6: 785. https://doi.org/10.3390/brainsci12060785