
Nomogram to Predict Cognitive State Improvement after Deep Brain Stimulation for Parkinson’s Disease

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Outcome Assessment
2.3. Statistical Analyses
3. Results
3.1. Patients
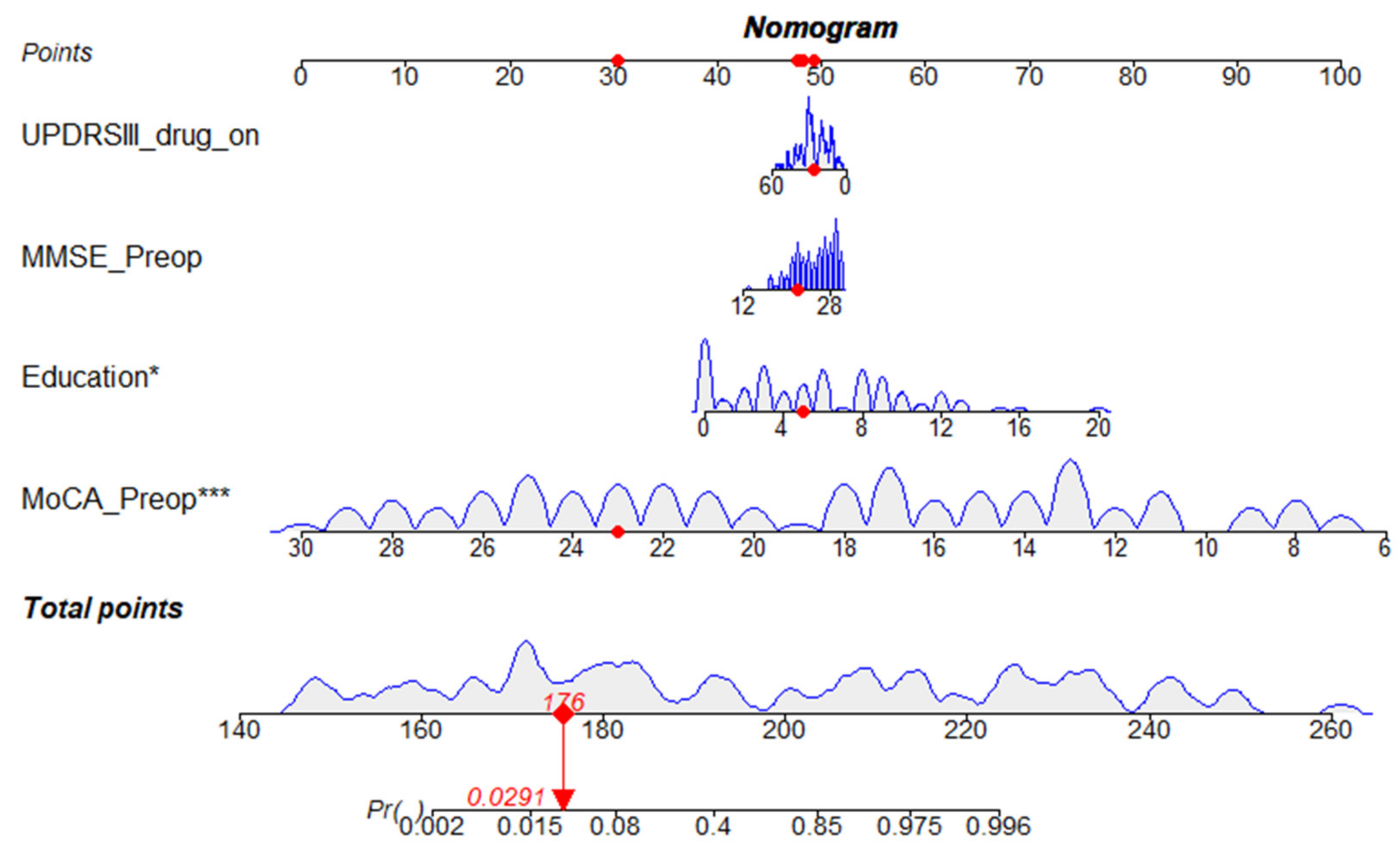
3.2. Development of the Nomogram
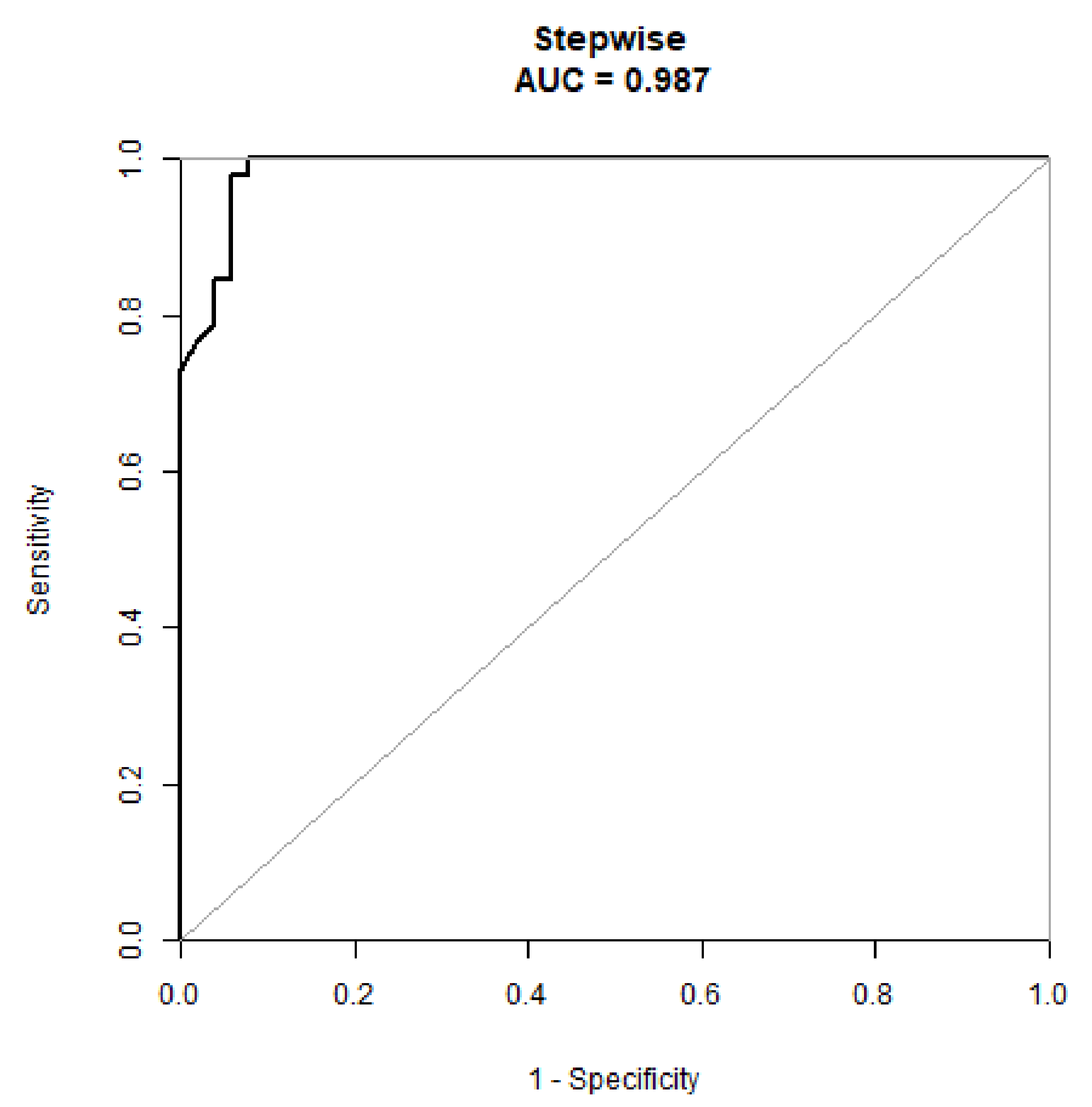
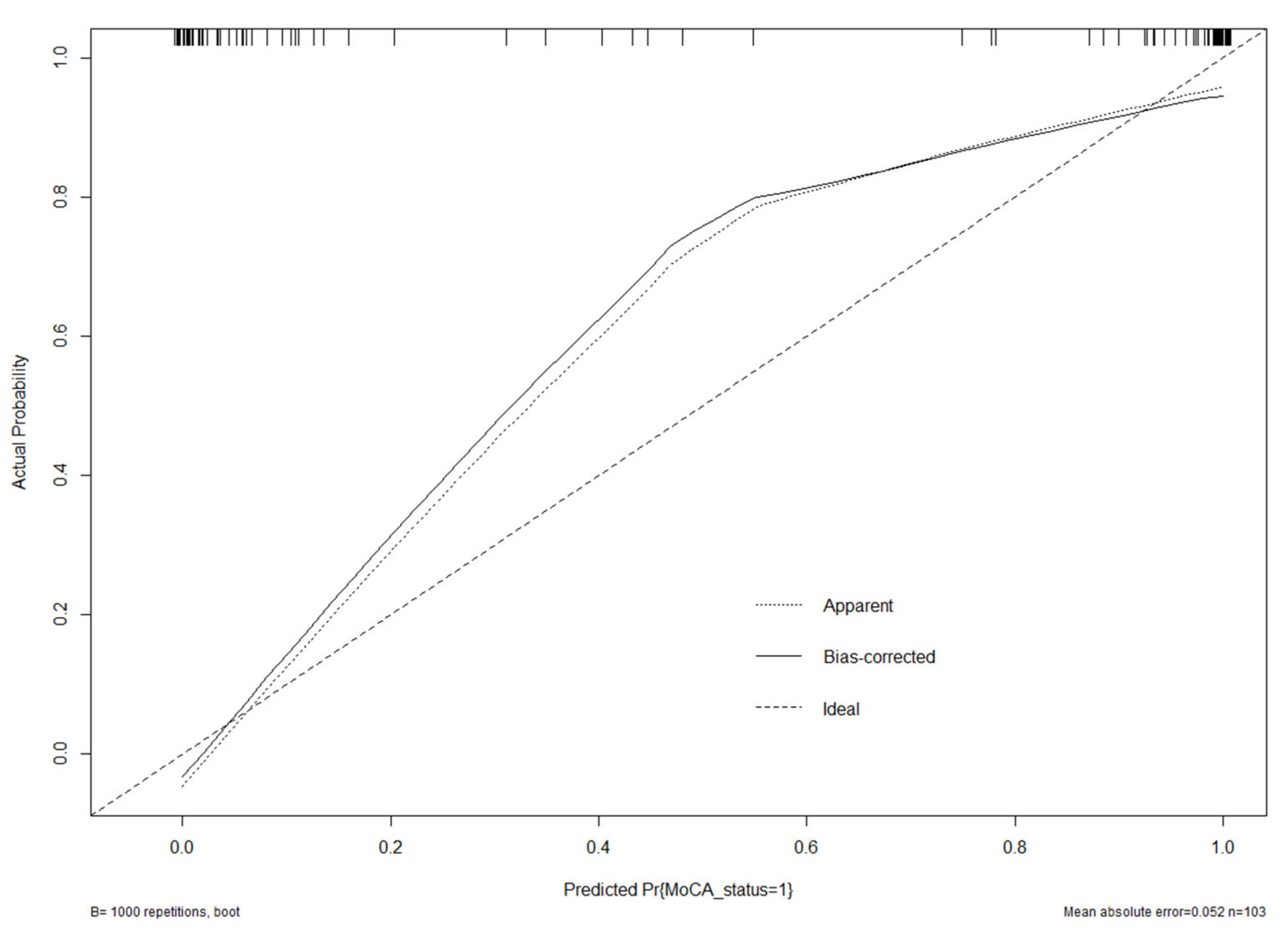
3.3. Validation of the Nomogram
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cerri, S.; Mus, L.; Blandini, F. Parkinson’s Disease in Women and Men: What’s the Difference? J. Parkinsons Dis. 2019, 9, 501–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ascherio, A.; Schwarzschild, M.A. The epidemiology of Parkinson’s disease: Risk factors and prevention. Lancet Neurol. 2016, 15, 1257–1272. [Google Scholar] [CrossRef]
- Ribault, S.; Simon, E.; Berthiller, J.; Polo, G.; Nunes, A.; Brinzeu, A.; Mertens, P.; Danaila, T.; Thobois, S.; Laurencin, C. Comparison of clinical outcomes and accuracy of electrode placement between robot-assisted and conventional deep brain stimulation of the subthalamic nucleus: A single-center study. Acta Neurochir. 2021, 163, 1327–1333. [Google Scholar] [CrossRef] [PubMed]
- Pinto, S.; Le Bas, J.F.; Castana, L.; Krack, P.; Pollak, P.; Benabid, A.L. Comparison of two techniques to postoperatively localize the electrode contacts used for subthalamic nucleus stimulation. Neurosurgery 2007, 60 (Suppl. 2), 285–292, discussion 292–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Wu, L.; Yang, C.; Xian, W.; Zheng, Y.; Zhang, C.; Hong, G.; Jiang, L.; Yang, Z.; Pei, Z.; et al. The white matter hyperintensities within the cholinergic pathways and cognitive performance in patients with Parkinson’s disease after bilateral STN DBS. J. Neurol. Sci. 2020, 418, 117121. [Google Scholar] [CrossRef]
- Farzanehfar, P.; Woodrow, H.; Horne, M. Sensor Measurements Can Characterize Fluctuations and Wearing Off in Parkinson’s Disease and Guide Therapy to Improve Motor, Non-motor and Quality of Life Scores. Frony. Aging Neurosci. 2022, 14, 852992. [Google Scholar] [CrossRef]
- Leimbach, F.; Atkinson-Clement, C.; Socorro, P.; Jahanshahi, M. The Effects of Subthalamic Nucleus Deep Brain Stimulation in Parkinson’s Disease on Associative Learning of Verbal and Non-Verbal Information by Trial and Error or with Corrective Feedback. J. Parkinsons Dis. 2022, 12, 885–896. [Google Scholar] [CrossRef]
- Wei, X.; Shen, Q.; Litvan, I.; Huang, M.; Lee, R.R.; Harrington, D.L. Internetwork Connectivity Predicts Cognitive Decline in Parkinson’s and Is Altered by Genetic Variants. Front. Aging Neurosci. 2022, 14, 853029. [Google Scholar] [CrossRef]
- Bourilhon, J.; Mullie, Y.; Olivier, C.; Cherif, S.; Belaid, H.; Grabli, D.; Czernecki, V.; Karachi, C.; Welter, M.-L. Stimulation of the pedunculopontine and cuneiform nuclei for freezing of gait and falls in Parkinson disease: Cross-over single-blinded study and long-term follow-up. Parkinsonism Relat. Disord. 2022, 96, 13–17. [Google Scholar] [CrossRef]
- Aarsland, D.; Bronnick, K.; Williams-Gray, C.; Weintraub, D.; Marder, K.; Kulisevsky, J.; Burn, D.; Barone, P.; Pagonabarraga, J.; Allcock, L.; et al. Mild cognitive impairment in Parkinson disease: A multicenter pooled analysis. Neurology 2010, 75, 1062–1069. [Google Scholar] [CrossRef]
- Ding, W.; Ding, L.J.; Li, F.F.; Han, Y.; Mu, L. Neurodegeneration and cognition in Parkinson’s disease: A review. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 2275–2281. [Google Scholar] [PubMed]
- Appleby, B.S.; Duggan, P.S.; Regenberg, A.; Rabins, P.V. Psychiatric and neuropsychiatric adverse events associated with deep brain stimulation: A meta-analysis of 10 years’ experience. Mov. Disord. 2007, 22, 1722–1728. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Meng, X.; Xiao, J.; Zhang, J.; Zhang, J. Cognitive Changes following Bilateral Deep Brain Stimulation of Subthalamic Nucleus in Parkinson’s Disease: A Meta-Analysis. BioMed Res. Int. 2016, 2016, 3596415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- David, F.J.; Munoz, M.J.; Corcos, D.M. The effect of STN DBS on modulating brain oscillations: Consequences for motor and cognitive behavior. Exp. Brain Res. 2020, 238, 1659–1676. [Google Scholar] [CrossRef]
- Smeding, H.M.; Speelman, J.D.; Huizenga, H.M.; Schuurman, P.R.; Schmand, B. Predictors of cognitive and psychosocial outcome after STN DBS in Parkinson’s Disease. J. Neurol. Neurosurg. Psychiatry 2011, 82, 754–760. [Google Scholar] [CrossRef] [Green Version]
- Lövdén, M.; Fratiglioni, L.; Glymour, M.M.; Lindenberger, U.; Tucker-Drob, E.M. Education and Cognitive Functioning Across the Life Span. Psychol. Sci. Public Interest. 2020, 21, 6–41. [Google Scholar] [CrossRef]
- Lyons, K.; McLaughlin, J.E.; Khanova, J.; Roth, M.T. Cognitive apprenticeship in health sciences education: A qualitative review. Adv. Health Sci. Educ. Theory Pract. 2017, 22, 723–739. [Google Scholar] [CrossRef]
- McSparron, J.I.; Vanka, A.; Smith, C.C. Cognitive learning theory for clinical teaching. Clin. Teach. 2019, 16, 96–100. [Google Scholar] [CrossRef]
- Beurrier, C.; Congar, P.; Bioulac, B.; Hammond, C. Subthalamic nucleus neurons switch from single-spike activity to burst-firing mode. J. Neurosc. 1999, 19, 599–609. [Google Scholar] [CrossRef]
- Knight, E.J.; Testini, P.; Min, H.-K.; Gibson, W.S.; Gorny, K.R.; Favazza, C.P.; Felmlee, J.P.; Kim, I.; Welker, K.M.; Clayton, D.A.; et al. Motor and Nonmotor Circuitry Activation Induced by Subthalamic Nucleus Deep Brain Stimulation in Patients with Parkinson Disease: Intraoperative Functional Magnetic Resonance Imaging for Deep Brain Stimulation. Mayo Clin. Proc. 2015, 90, 773–785. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.Q.; Zhuang, H.X.; Zhang, L.X.; Chen, X.; Niu, C.S.; Zhao, M. Nomogram for Predicting Postoperative Delirium After Deep Brain Stimulation Surgery for Parkinson’s Disease. World Neurosurg. 2019, 130, e551–e557. [Google Scholar] [CrossRef] [PubMed]
- Zhan, L.; Wang, X.Q.; Zhang, L.X. Nomogram Model for Predicting Risk of Postoperative Delirium After Deep Brain Stimulation Surgery in Patients Older Than 50 Years with Parkinson Disease. World Neurosurg. 2020, 139, e127–e135. [Google Scholar] [CrossRef] [PubMed]
- Frizon, L.A.; Hogue, O.; Achey, R.; Floden, D.P.; Nagel, S.; Machado, A.G.; Lobel, D.A. Quality of Life Improvement Following Deep Brain Stimulation for Parkinson Disease: Development of a Prognostic Model. Neurosurgery 2019, 85, 343–349. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lower Improvement Rate | Higher Improvement Rate | p-Value | |
|---|---|---|---|
| No. | 51 | 52 | |
| Age | 57.31 ± 7.95 | 60.67 ± 7.82 | 0.033 |
| Duration (years) | 8.86 ± 3.95 | 8.54 ± 3.67 | 0.667 |
| Education (years) | 3.13 ± 2.95 | 7.90 ± 4.29 | <0.001 |
| LED | 661.03 ± 215.73 | 658.89 ± 468.04 | 0.976 |
| Drug improvement rate | 0.55 ± 0.13 | 0.49 ± 0.15 | 0.031 |
| UPDRSIII drug off | 50.22 ± 13.10 | 57.71 ± 14.27 | 0.007 |
| UPDRSIII drug on | 22.45 ± 9.29 | 30.75 ± 11.99 | <0.001 |
| NMSS Preop | 84.63 ± 30.65 | 90.38 ± 29.38 | 0.333 |
| PDQ39 Preop | 71.47 ± 17.02 | 74.98 ± 15.41 | 0.275 |
| MOCA Preop | 23.76 ± 3.44 | 13.67 ± 3.57 | <0.001 |
| MMSE Preop | 26.88 ± 3.24 | 23.13 ± 3.25 | <0.001 |
| HAMD Preop | 14.71 ± 5.11 | 16.73 ± 7.82 | 0.124 |
| HAMA Preop | 17.47 ± 5.31 | 18.63 ± 5.45 | 0.275 |
| Gender | 0.465 | ||
| male | 33 (64.71%) | 30 (57.69%) | |
| female | 18 (35.29%) | 22 (42.31%) | |
| H-Y | 0.659 | ||
| 2 | 1 (1.96%) | 1 (1.92%) | |
| 2.5 | 9 (17.65%) | 7 (13.46%) | |
| 3 | 27 (52.94%) | 23 (44.23%) | |
| 4 | 12 (23.53%) | 16 (30.77%) | |
| 5 | 2 (3.92%) | 5 (9.62%) |
| Statistics | OR (95% CI) p-Value | |
|---|---|---|
| Age | 59.01 ± 8.03 | 1.06 (1.00, 1.11) 0.0362 |
| Gender | ||
| male | 63 (61.17%) | 1.0 |
| female | 40 (38.83%) | 1.34 (0.61, 2.98) 0.4657 |
| Education (years) | 5.54 ± 4.38 | 1.42 (1.23, 1.63) <0.0001 |
| LED | 659.95 ± 363.80 | 1.00 (1.00, 1.00) 0.9761 |
| UPDRSIII drug off | 54.00 ± 14.15 | 1.04 (1.01, 1.07) 0.0090 |
| UPDRSIII drug on | 26.64 ± 11.47 | 1.08 (1.03, 1.12) 0.0005 |
| Drug improvement rate | 0.52 ± 0.14 | 0.04 (0.00, 0.79) 0.0339 |
| MMSE Preop | 24.99 ± 3.74 | 0.70 (0.61, 0.82) <0.0001 |
| MOCA Preop | 18.67 ± 6.15 | 0.46 (0.34, 0.64) <0.0001 |
| NMSS Preop | 87.53 ± 30.01 | 1.01 (0.99, 1.02) 0.3303 |
| PDQ39 Preop | 73.24 ± 16.25 | 1.01 (0.99, 1.04) 0.2737 |
| HAMD Preop | 15.73 ± 6.66 | 1.05 (0.99, 1.12) 0.1292 |
| HAMA Preop | 18.06 ± 5.38 | 1.04 (0.97, 1.12) 0.2726 |
| Duration (years) | 8.70 ± 3.80 | 0.98 (0.88, 1.08) 0.6637 |
| H-Y | ||
| 2 | 2 (1.94%) | 1.0 |
| 2.5 | 16 (15.53%) | 0.78 (0.04, 14.75) 0.8671 |
| 3 | 50 (48.54%) | 0.85 (0.05, 14.39) 0.9115 |
| 4 | 28 (27.18%) | 1.33 (0.08, 23.54) 0.8443 |
| 5 | 7 (6.80%) | 2.50 (0.10, 62.61) 0.5771 |
| Non-Adjusted | Model I | Model II | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Education (years) | 1.42 (1.23, 1.63) | *** | 1.44 (1.23, 1.68) | *** | 1.49 (1.25, 1.77) | *** |
| Age (years) | 1.06 (1.00, 1.11) | * | 1.09 (1.01, 1.17) | * | 1.07 (0.99, 1.15) | |
| UPDRSIII drug off | 1.04 (1.01, 1.07) | ** | 1.05 (1.01, 1.09) | ** | 1.04 (1.00, 1.08) | |
| UPDRSIII drug on | 1.08 (1.03, 1.12) | *** | 1.09 (1.03, 1.14) | ** | 1.08 (1.02, 1.14) | ** |
| MoCA Preop | 0.46 (0.34, 0.64) | *** | 0.16 (0.05, 0.54) | ** | 0.14 (0.04, 0.54) | ** |
| MMSE Preop | 0.70 (0.61, 0.82) | *** | 0.60 (0.48, 0.75) | *** | 0.61 (0.49, 0.77) | *** |
| Drug improvement rate | 0.04 (0.00, 0.79) | * | 0.03 (0.00, 0.77) | * | 0.04 (0.00, 1.15) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, B.; Ni, C.; Zhang, W.; Mei, J.; Xiong, C.; Chen, P.; Jiang, M.; Niu, C. Nomogram to Predict Cognitive State Improvement after Deep Brain Stimulation for Parkinson’s Disease. Brain Sci. 2022, 12, 759. https://doi.org/10.3390/brainsci12060759
Chang B, Ni C, Zhang W, Mei J, Xiong C, Chen P, Jiang M, Niu C. Nomogram to Predict Cognitive State Improvement after Deep Brain Stimulation for Parkinson’s Disease. Brain Sciences. 2022; 12(6):759. https://doi.org/10.3390/brainsci12060759
Chicago/Turabian StyleChang, Bowen, Chen Ni, Weiwen Zhang, Jiaming Mei, Chi Xiong, Peng Chen, Manli Jiang, and Chaoshi Niu. 2022. "Nomogram to Predict Cognitive State Improvement after Deep Brain Stimulation for Parkinson’s Disease" Brain Sciences 12, no. 6: 759. https://doi.org/10.3390/brainsci12060759