
The Role of Music Therapy with Infants with Perinatal Brain Injury


Abstract
:1. Introduction
Aim
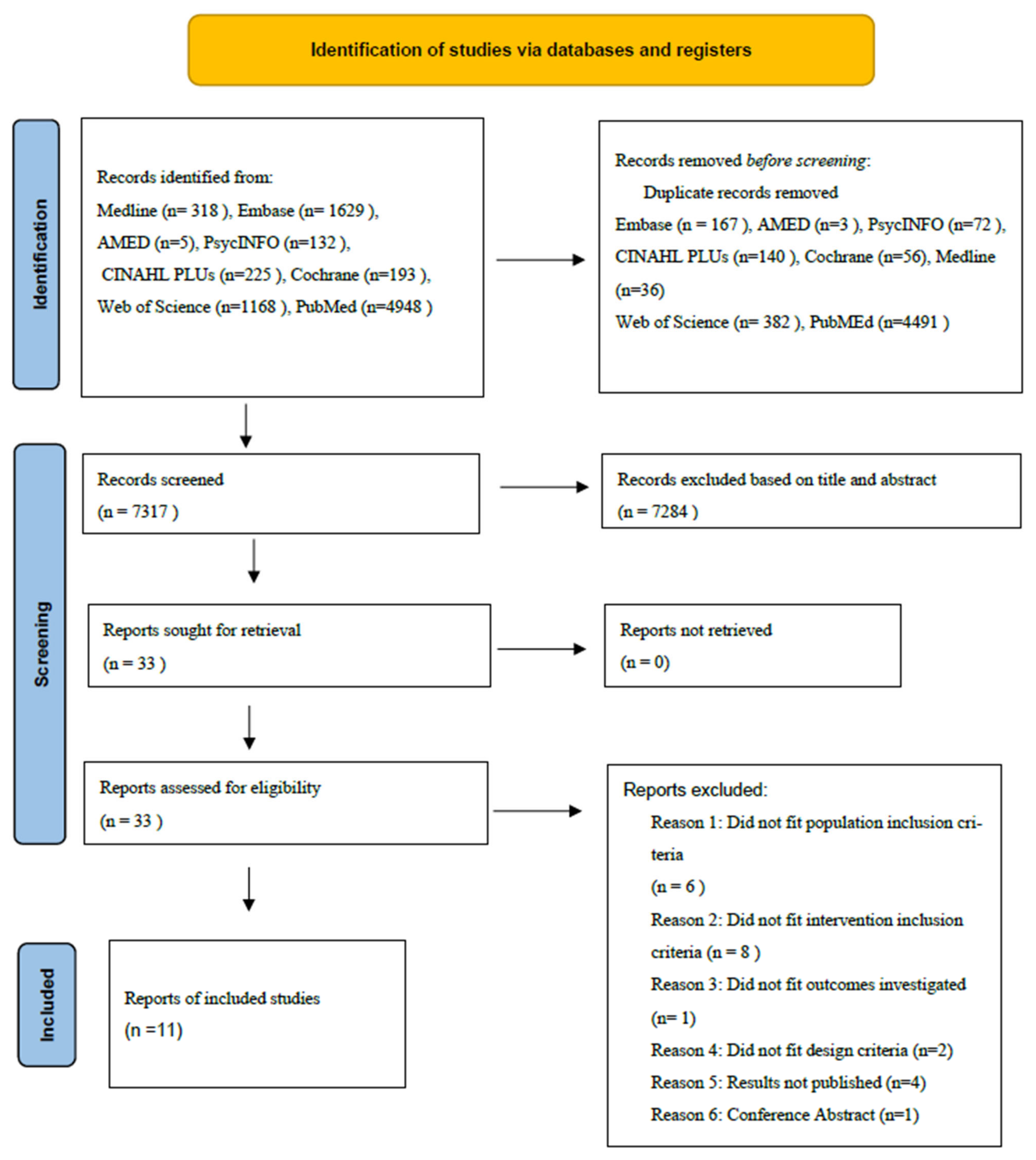
2. Methodology
2.1. Information Sources and Search Terms
- Music therapy, acoustic stimulation, auditory stimulation, music intervention, music, voice, song, sound, vocal, singing, womb sounds, heartbeat
- Neonatal, neonate, newborn, new-born, preterm, pre-term, extreme preterm, very preterm, moderate to late preterm, premature
- Brain injury, seizure, stoke, neonatal encephalopathy, traumatic brain injury, Hypoxic ischemic encephalopathy, HIE, intrapartum asphyxia, foetal brain injury or fetal, IVH, intraventricular haemorrhage, PVL, periventricular leukomalacia
2.2. Selection Process
2.3. Quality Appraisal
2.4. Subgroup Analysis
3. Results
3.1. Forms of Intervention
3.2. Immediate Impact on Newborn Physiological Parameters
3.3. The Impact of MT on Infant Neurological Parameters
3.4. Impact of MT upon Parental Anxiety
4. Discussion
4.1. The Effect of Auditory Stimulation on Infant Physiological and Neurological Parameters
4.2. The Effect of Infant Auditory Stimulation upon Parental Experience
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Quality Assessment of Included Studies



{kind=link}
{kind=link}
{kind=link}
| Selection | Comparability | Outcome | ||||||
|---|---|---|---|---|---|---|---|---|
| Study | Representativeness of the exposed cohort | Selection of the non-exposed cohort | Ascertainment of exposure | Comparability of cohorts on the basis of the design or analysis (up to 2 stars) | Assessment of outcome | Was follow up long enough for outcomes to occur | Adequacy of follow up of cohorts | Total no. of stars out of 8 |
| Doheny (2012) | 0 | * | * | ** | 0 | * | * | 6 |
References
- Gale, C.; Statnikov, Y.; Jawad, S.; Uthaya, S.N.; Modi, N. Neonatal brain injuries in England: Population-based incidence derived from routinely recorded clinical data held in the National Neonatal Research Database. Arch. Dis. Child. Fetal Neonatal Ed. 2017, 103, F301–F306. [Google Scholar] [CrossRef] [PubMed]
- Marx, V.; Nagy, E. Fetal Behavioural Responses to Maternal Voice and Touch. PLoS ONE 2015, 10, e0129118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flaks, M.K.; Malta, S.M.; Almeida, P.P.; Bueno, O.F.; Pupo, M.C.; Andreoli, S.B.; Mello, M.F.; Lacerda, A.; Mari, J.J.; Bressan, R. Attentional and executive functions are differentially affected by post-traumatic stress disorder and trauma. J. Psychiatr. Res. 2014, 48, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Stewart, K. PATTERNS—A Model for Evaluating Trauma in NICU Music Therapy: Part 1—Theory and Design. Music Med. 2009, 1, 29–40. [Google Scholar] [CrossRef]
- PEEPS-HIE. What Is HIE. 2022. Available online: https://www.peeps-hie.org/what-is-hie/ (accessed on 18 January 2022).
- Glass, H.C. Hypoxic-Ischemic Encephalopathy and Other Neonatal Encephalopathies. Contin. Lifelong Learn. Neurol. 2018, 24, 57–71. [Google Scholar] [CrossRef]
- Gale, C.S.; Jawad, S.E.; Uthaya, S.; Modi, N. Brain Injury Occurring during or Soon after Birth: A Repost for the National Maternity Ambition Commissioned by the Department of Health; National Data Analysis Unit: London, UK, 2017. [Google Scholar]
- Gotardo, J.W.; Volkmer, N.D.F.V.; Stangler, G.P.; Dornelles, A.D.; Bohrer, B.B.D.A.; Carvalho, C.G. Impact of peri-intraventricular haemorrhage and periventricular leukomalacia in the neurodevelopment of preterms: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0223427. [Google Scholar] [CrossRef]
- Chabrier, S.; Husson, B.; Dinomais, M.; Landrieu, P.; Tich, S.N.T. New insights (and new interrogations) in perinatal arterial ischemic stroke. Thromb. Res. 2011, 127, 13–22. [Google Scholar] [CrossRef] [Green Version]
- Hagberg, H.; Edwards, A.D.; Groenendaal, F. Perinatal brain damage: The term infant. Neurobiol. Dis. 2015, 92, 102–112. [Google Scholar] [CrossRef] [Green Version]
- Christ, L.; Barber, J.; Murray, A.; Dunleavy, M.; Stoller, J.; Taha, D.; Brown-Jackson, L.; McElroy, M.; Posencheg, M. Reducing Intraventricular Hemorrhage in a Level III Neonatal Intensive Care Unit. BMJ Qual. Saf. 2015, 24, 731–732. [Google Scholar] [CrossRef] [Green Version]
- Biskop, E.; Paulsdotter, T.; Westas, L.H.; Ågren, J.; Blomqvist, Y.T. Parental participation during therapeutic hypothermia for neonatal hypoxic-ischemic encephalopathy. Sex. Reprod. Health 2019, 20, 77–80. [Google Scholar] [CrossRef]
- Franck, L.S.; Cox, S.; Allen, A.; Winter, I. Measuring neonatal intensive care unit-related parental stress. J. Adv. Nurs. 2005, 49, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Pineda, R.; Bender, J.; Hall, B.; Shabosky, L.; Annecca, A.; Smith, J. Parent participation in the neonatal intensive care unit: Predictors and relationships to neurobehavior and developmental outcomes. Early Hum. Dev. 2017, 117, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Franck, L.S.; Kriz, R.M.; Bisgaard, R.; Cormier, D.M.; Joe, P.; Miller, P.S.; Kim, J.H.; Lin, C.; Sun, Y. Comparison of family centered care with family integrated care and mobile technology (mFICare) on preterm infant and family outcomes: A multi-site quasi-experimental clinical trial protocol. BMC Pediatr. 2019, 19, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ettenberger, M.; Cárdenas, C.R.; Parker, M.; Odell-Miller, H. Family-centred music therapy with preterm infants and their parents in the Neonatal Intensive Care Unit (NICU) in Colombia—A mixed-methods study. Nord. J. Music Ther. 2016, 26, 207–234. [Google Scholar] [CrossRef] [Green Version]
- BAMT. What Is Music Therapy. 2022. Available online: https://www.bamt.org/music-therapy/what-is-music-therapy (accessed on 22 December 2021).
- Loewy, J.; Stewart, K.; Dassler, A.-M.; Telsey, A.; Homel, P. The Effects of Music Therapy on Vital Signs, Feeding, and Sleep in Premature Infants. Pediatrics 2013, 131, 902–918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haslbeck, F.B. Creative music therapy with premature infants: An analysis of video footage. Nord. J. Music Ther. 2013, 23, 5–35. [Google Scholar] [CrossRef]
- Standley, J.M.; Walworth, D. Music Therapy with Premature Infants: Research and Developmental Interventions; The American Music Therapy Association, Inc.: Silver Spring, MD, USA, 2010. [Google Scholar]
- Vahdati, M.; Mohammadizadeh, M.; Talakoub, S. Effect of Kangaroo Care Combined with Music on the Mother–premature Neonate Attachment: A Randomized Controlled Trial. Iran. J. Nurs. Midwifery Res. 2017, 22, 403–407. [Google Scholar] [CrossRef]
- Standley, J.M. The effect of music and multimodal stimulation on responses of premature infants in neonatal intensive care. Pediatr. Nurs. 1999, 24, 532. [Google Scholar]
- Bieleninik, Ł.; Ghetti, C.; Gold, C. Music Therapy for Preterm Infants and Their Parents: A Meta-analysis. Pediatrics 2016, 138, e20160971. [Google Scholar] [CrossRef] [Green Version]
- Haslbeck, F.B.; Jakab, A.; Held, U.; Bassler, D.; Bucher, H.-U.; Hagmann, C. Creative music therapy to promote brain function and brain structure in preterm infants: A randomized controlled pilot study. NeuroImage: Clin. 2020, 25, 102171. [Google Scholar] [CrossRef]
- van Dokkum, N.H.; Kooi, E.M.; Berhane, B.; Ravensbergen, A.G.; Hakvoort, L.; Jaschke, A.C.; Bos, A.F. Neonatal music therapy and cerebral oxygenation in extremely and very preterm infants: A pilot study. Music. Med. 2021, 13, 91–98. [Google Scholar] [CrossRef]
- Fachner, J.; Stegemann, T. Electroencephalography and Music Therapy: On the Same Wavelength? Music Med. 2013, 5, 217–222. [Google Scholar] [CrossRef]
- Fraser, L.K.; Murtagh, F.E.; Aldridge, J.; Sheldon, T.; Gilbody, S.; Hewitt, C. Health of mothers of children with a life-limiting condition: A comparative cohort study. Arch. Dis. Child. 2021, 106, 987–993. [Google Scholar] [CrossRef] [PubMed]
- Vriezen, E.R.; Pigott, S.E. The Relationship Between Parental Report on the BRIEF and Performance-Based Measures of Executive Function in Children with Moderate to Severe Traumatic Brain Injury. Child Neuropsychol. 2002, 8, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 105906. [Google Scholar] [CrossRef]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, D142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.S.J.; Page, M.J.; Sterne, J.A.C. Revised Cochrane Risk of Bias Tool. Available online: https://www.riskofbias.info/welcome/rob-2-0-tool/current-version-of-rob-2 (accessed on 31 December 2021).
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analysis. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 31 December 2021).
- Panagiotidis, J.; Lahav, A. Simulation of prenatal maternal sounds in NICU incubators: A pilot safety and feasibility study. J. Matern. Neonatal Med. 2010, 23, 106–109. [Google Scholar] [CrossRef] [PubMed]
- Graven, S.N. Sound and the Developing Infant in the NICU: Conclusions and Recommendations for Care. J. Perinatol. 2000, 20, S88–S93. [Google Scholar] [CrossRef]
- Chorna, O.D.; Slaughter, J.C.; Wang, L.; Stark, A.R.; Maitre, N.L. A Pacifier-Activated Music Player With Mother’s Voice Improves Oral Feeding in Preterm Infants. Pediatrics 2014, 133, 462–468. [Google Scholar] [CrossRef] [Green Version]
- Chirico, G.; Cabano, R.; Villa, G.; Bigogno, A.; Ardesi, M.; Dioni, E. Randomised study showed that recorded maternal voices reduced pain in preterm infants undergoing heel lance procedures in a neonatal intensive care unit. Acta Paediatr. 2017, 106, 1564–1568. [Google Scholar] [CrossRef]
- Doheny, L.; Hurwitz, S.; Insoft, R.; Ringer, S.; Lahav, A. Exposure to biological maternal sounds improves cardiorespiratory regulation in extremely preterm infants. J. Matern. Neonatal Med. 2012, 25, 1591–1594. [Google Scholar] [CrossRef] [PubMed]
- Konar, M.C.; Islam, K.; Sil, A.; Nayek, K.; Barik, K. Effect of Music on Outcomes of Birth Asphyxia: A Randomized Controlled Trial. J. Trop. Pediatr. 2021, 67, fmab009. [Google Scholar] [CrossRef] [PubMed]
- Hummel, P.; Lawlor-Klean, P.; Weiss, M.G. Validity and reliability of the N-PASS assessment tool with acute pain. J. Perinatol. 2009, 30, 474–478. [Google Scholar] [CrossRef] [PubMed]
- Stevens, B.; Johnston, C.; Petryshen, P.; Taddio, A. Premature Infant Pain Profile: Development and Initial Validation. Clin. J. Pain 1996, 12, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Hepper, P.G.; Shahidullah, B.S. Development of fetal hearing. Arch. Dis. Childhood. Fetal Neonatal Ed. 1994, 71, F81–F87. [Google Scholar] [CrossRef] [Green Version]
- Haslbeck, F.B. Music therapy for premature infants and their parents: An integrative review. Nord. J. Music Ther. 2012, 21, 203–226. [Google Scholar] [CrossRef]
- Ettenberger, M.; Ardila, Y.M.B. Music therapy song writing with mothers of preterm babies in the Neonatal Intensive Care Unit (NICU)—A mixed-methods pilot study. Arts Psychother. 2018, 58, 42–52. [Google Scholar] [CrossRef]
- Epstein, S.; Bauer, S.; Stern, O.L.; Litmanovitz, I.; Elefant, C.; Yakobson, D.; Arnon, S. Preterm infants with severe brain injury demonstrate unstable physiological responses during maternal singing with music therapy: A randomized controlled study. Eur. J. Pediatr. 2020, 180, 1403–1412. [Google Scholar] [CrossRef]
- White-Traut, R.C.; Nelson, M.N.; Silvestri, J.M.; Patel, M.; Berbaum, M.; Gu, G.; Rey, P.M. Developmental Patterns of Physiological Response to a Multisensory Intervention in Extremely Premature and High-Risk Infants. J. Obstet. Gynecol. Neonatal Nurs. 2004, 33, 266–275. [Google Scholar] [CrossRef]
- Sa de Almeida, J.; Lordier, L.; Zollinger, B.; Kunz, N.; Bastiani, M.; Gui, L.; Adam-Darque, A.; Borradori-Tolsa, C.; Lazeyras, F.; Hüppi, P.S. Music enhances structural maturation of emotional processing neural pathways in very preterm infants. Neuroimage 2020, 207, 116391. [Google Scholar] [CrossRef]
- Lennon, E.M.; Gardner, J.M.; Karmel, B.Z.; Flory, M.J. Bayley Scales of Infant Development. In Encyclopedia of Infant and Early Childhood Development; Haith, M.M., Benson, J.B., Eds.; Academic Press: San Diego, CA, USA, 2008; pp. 145–156. [Google Scholar] [CrossRef]
- Censullo, M.; Bowler, R.; Lester, B.; Brazelton, T.B. An instrument for the measurement of infant-adult synchrony. Nurs. Res. 1987, 36, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Miles, M.S.; Funk, S.G.; Carlson, J. Parental Stressor Scale: Neonatal intensive care unit. Nurs. Res. 1993, 42, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Speilberger, C.D. Manual for the State-Trait Anxiety Inventory (STAI); Consulting Physchologists Press: Redwood City, CA, USA, 1983. [Google Scholar]
- Kraft, K.; Jaschke, A.; Ravensbergen, A.-G.; Feenstra-Weelink, A.; van Goor, M.; de Kroon, M.; Reijneveld, S.; Bos, A.; van Dokkum, N. Maternal Anxiety, Infant Stress, and the Role of Live-Performed Music Therapy during NICU Stay in The Netherlands. Int. J. Environ. Res. Public Health 2021, 18, 7077. [Google Scholar] [CrossRef] [PubMed]
- Emery, L.; Hamm, E.L.; Hague, K.; Chorna, O.; Moore-Clingenpeel, M.; Maitre, N. A randomised controlled trial of protocolised music therapy demonstrates developmental milestone acquisition in hospitalised infants. Acta Paediatr. 2018, 108, 828–834. [Google Scholar] [CrossRef] [PubMed]
- Letzkus, L.; Alonzo, C.; Connaughton, E.; Kelly, N.; Zanelli, S. A Maternal-Administered Multimodal Neonatal Bundle in Hospitalized Very Preterm Infants: A Pilot Study. Adv. Neonatal Care 2021, 21, E35–E42. [Google Scholar] [CrossRef]
- Nelson, M.N.; White-Traut, R.C.; Vasan, U.; Silvestri, J.; Comiskey, E.; Meleedy-Rey, P.; Littau, S.; Gu, G.; Patel, M. One-year outcome of auditory-tactile-visual vestibular intervention in the neonatal intensive care unit: Effects of severe prematurity and central nervous system injury. J. Child Neurol. 2001, 16, 493–498. [Google Scholar] [CrossRef]
- White-Traut, R.C.; Nelson, M.N.; Silvestri, J.M.; Patel, M.; Vasan, U.; Han, B.K.; Cunningham, N.; Burns, K.; Kopischke, K.; Bradford, L. Developmental intervention for preterm infants diagnosed with periventricular leukomalacia. Res. Nurs. Health 1999, 22, 131–143. [Google Scholar] [CrossRef]
- Yasin, F.; Women, C.; Infants University Hospital. Effect of Mozart Music on Cerebral Oxygenation and Behavioural Response of Premature Infants (July 2014–July 2015) Identifier NCT02471482. Available online: https://clinicaltrials.gov/show/NCT02471482 (accessed on 18 January 2022).
- Shokri, E. Effect If PIOMI Combine with Music Therapy on Feeding of Premature Infants, Identifier IRCT20210502051155N1. Available online: http://en.irct.ir/trial/56003 (accessed on 18 January 2022).
- Sgobbi, B.; di Circolo, O. The Effects of Recorded Music Therapy on Oral Nutrition and the Well-Being of the Italian Premature Baby: Prosepective Randomized Controlled Study Mom, Dad and Music Therapist Singing Voice. (August 2020–February 2021) Identifier: NCT04759170. Available online: https://clinicaltrials.gov/show/NCT04759170 (accessed on 18 January 2022).
- Meir Medical Center. The Combined Effects of Maternal Singing During Skin to Skin Contact (Kangaroo Care) in Preterm Infants in the Neonatal Care Unit Environment. (November 2011–November 2014) Identifier: NCT01427894. Available online: https://clinicaltrials.gov/show/NCT013427894 (accessed on 18 January 2022).
- Zimmerman, E.Z.; Norton, M.N.; McMahon, E.S.M.; Arnorld, A.B.S.; Ringer, S.A.R.; Lahav, A.L. The effects of maternal voice and biological sounds on nutrition and respiratory outcomes in preterm infants. J. Matern. -Fetal Neonatal Med. 2012, 25 (Suppl. 2), 37–38. [Google Scholar] [CrossRef]
- Corrigan, M.J.; Keeler, J.; Miller, H.D.; Ben Khallouq, B.A.; Fowler, S.B. Music therapy and retinopathy of prematurity screening: Using recorded maternal singing and heartbeat for post exam recovery. J. Perinatol. 2020, 40, 1780–1788. [Google Scholar] [CrossRef]
- Lawhon, G.; Helm, J.M.; Buehler, D.; McAnulty, G.; Kosta, S.; Alberts, J.R.; Als, H.; Mader, S.; Daly, M.; Sizun, J.; et al. NIDCAP Federation International response. Pediatrics 2013, 132, e550–e551. [Google Scholar] [CrossRef]
- Ren, H.; Zou, L.; Wang, L.; Lu, C.; Yuan, Y.; Dai, C.; Chen, W. Evaluation of the Short-Term Music Therapy on Brain Functions of Preterm Infants Using Functional Near-Infrared Spectroscopy. Front. Neurol. 2021, 12, 1634. [Google Scholar] [CrossRef] [PubMed]
- Giordano, V.; Goeral, K.; Schrage-Leitner, L.; Berger, A.; Olischar, M. The Effect of Music on aEEG Cyclicity in Preterm Neonates. Children 2021, 8, 208. [Google Scholar] [CrossRef] [PubMed]
- Pasman, J.W.; Rotteveel, J.J.; De Graaf, R.; Maassen, B.; Notermans, S.L. Detectability of auditory evoked response components in preterm infants. Early Hum. Dev. 1991, 26, 129–141. [Google Scholar] [CrossRef]
- Kisilevsky, S.; Hains, S.M.J.; Jacquet, A.Y.; Granier-Deferre, C.; Lecanuet, J.P. Maturation of fetal responses to music. Dev. Sci. 2004, 7, 550–559. [Google Scholar] [CrossRef] [PubMed]
- Partanen, E.; Kujala, T.; Tervaniemi, M.; Huotilainen, M. Prenatal Music Exposure Induces Long-Term Neural Effects. PLoS ONE 2013, 8, e78946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, C.A.; Fitch, R.H. Sex Differences in Mechanisms and Outcome of Neonatal Hypoxia-Ischemia in Rodent Models: Implications for Sex-Specific Neuroprotection in Clinical Neonatal Practice. Neurol. Res. Int. 2012, 2012, 1–9. [Google Scholar] [CrossRef]
- Harding, C.; Whiting, L.; Petty, J.; Edney, S.; Murphy, R.; Crossley, S.-L. Infant communication. How should we define this, and is it important? J. Neonatal Nurs. 2022. [Google Scholar] [CrossRef]
- Haslbeck, F.B.; Bassler, D. Clinical Practice Protocol of Creative Music Therapy for Preterm Infants and Their Parents in the Neonatal Intensive Care Unit. J. Vis. Exp. 2020, 155, e60412. [Google Scholar] [CrossRef]
- Koelsch, S. Brain correlates of music-evoked emotions. Nat. Rev. Neurosci. 2014, 15, 170–180. [Google Scholar] [CrossRef]
- Pineda, R.G.; Neil, J.; Dierker, D.; Smyser, C.D.; Wallendorf, M.; Kidokoro, H.; Reynolds, L.C.; Walker, S.; Rogers, C.; Mathur, A.M.; et al. Alterations in Brain Structure and Neurodevelopmental Outcome in Preterm Infants Hospitalized in Different Neonatal Intensive Care Unit Environments. J. Pediatr. 2013, 164, 52–60.e2. [Google Scholar] [CrossRef] [Green Version]
- Chorna, O.; Filippa, M.; De Almeida, J.S.; Lordier, L.; Monaci, M.G.; Hüppi, P.; Grandjean, D.; Guzzetta, A. Neuroprocessing Mechanisms of Music during Fetal and Neonatal Development: A Role in Neuroplasticity and Neurodevelopment. Neural Plast. 2019, 2019, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kehl, S.M.; Marca-Ghaemmaghami, L.; Haller, M.; Pichler-Stachl, E.; Bucher, H.U.; Bassler, D.; Haslbeck, F.B. Depressive Symptoms and Parent-Creative Music Therapy with Premature Infants and Their Parents: A Mixed-Method Pilot Study on Parents’ Anxiety, Stress and Infant Attachment. Int. J. Environ. Res. Public Health 2020, 18, 265. [Google Scholar] [CrossRef] [PubMed]
- Roa, E.; Ettenberger, M. Music Therapy Self-Care Group for Parents of Preterm Infants in the Neonatal Intensive Care Unit: A Clinical Pilot Intervention. Medicines 2018, 5, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnon, S.; Diamant, C.; Bauer, S.; Regev, R.; Sirota, G.; Litmanovitz, I. Maternal singing during kangaroo care led to autonomic stability in preterm infants and reduced maternal anxiety. Acta Paediatr. 2014, 103, 1039–1044. [Google Scholar] [CrossRef] [PubMed]
- Kobus, S.; Diezel, M.; Huening, B.; Dewan, M.V.; Felderhoff-Mueser, U.; Bruns, N. Parents’ Perception of Family-Centered Music Therapy with Stable Preterm Infants. Int. J. Environ. Res. Public Health 2021, 18, 12813. [Google Scholar] [CrossRef] [PubMed]
- Span, L.; van Dokkum, N.; Ravensbergen, A.-G.; Bos, A.; Jaschke, A. Combining Kangaroo Care and Live-Performed Music Therapy: Effects on Physiological Stability and Neurological Functioning in Extremely and Very Preterm Infants. Int. J. Environ. Res. Public Health 2021, 18, 6580. [Google Scholar] [CrossRef] [PubMed]
- Shoemark, H. Time Together: A Feasible Program to Promote parent-infant Interaction in the NICU. Music Ther. Perspect. 2017, 36, 6–16. [Google Scholar] [CrossRef]
- Ghetti, C.; Bieleninik, L.; Hysing, M.; Kvestad, I.; Assmus, J.; Romeo, R.; Ettenberger, M.; Arnon, S.; Vederhus, B.J.; Gaden, T.S.; et al. Longitudinal Study of music Therapy’s Effectiveness for Premature infants and their caregivers (LongSTEP): Protocol for an international randomised trial. BMJ Open 2019, 9, e025062. [Google Scholar] [CrossRef] [Green Version]
- Malloch, S.; Trevarthen, C. Communicative Musicality: Exploring the Basis of Human Companionship; Oxford University Press: Oxford, UK, 2010. [Google Scholar]

| Database | Search Strategy |
|---|---|
| PubMed | (((((((((((music* adj3 therap*)) OR ((music intervention* or music or voice or song* or sound* or vocal or singing or womb sound* or heartbeat or heart beat))) OR ((music therap* or music stimulation or acoustic therap* or acoustic stimulation or auditory stimulation or auditory therap*))) OR (singing[MeSH Terms])) OR (sound[MeSH Terms])) OR (voice[MeSH Terms])) OR ((music[MeSH Terms]))) OR (Acoustic Stimulation[MeSH Terms])) OR (Music Therapy[MeSH Terms])) AND ((infant, newborn/or infant, premature/or infant, extremely premature/[MeSH Terms]) OR ((infant or neonat* or newborn* or new-born* or preterm or pre-term or extreme* preterm or extreme* premature or very preterm or moderate to late preterm or premature)))) AND ((Brain Injuries/or Ischemic Stroke/or Stroke/or Seizures/or Brain Injuries, Traumatic/[MeSH Terms]) OR ((brain injur* or seizure* or stoke* or neonatal encephalopathy or traumatic brain injur* or hypoxic ischemic encephalopathy or HIE or intrapartum asphyxia or f?etal brain injur* or IVH or intraventricular haemorrhage or PVL or periventricular leukomalacia))) Filters: Humans |
| Population | Neonates diagnosed with any form of brain injury |
| Intervention | Any music or vocal stimulation to both infant alone and with parent present. |
| Comparator | Form of auditory stimulation Frequency and duration of intervention Music therapy alone or combined with a second intervention Gestational age |
| Outcomes | Infants: MRI results Change in oxygen saturation Change in heart rate Change in behavioural state of infant Adverse effects: physiological signs of stress Weight gain Neurodevelopment Parents: Parent–infant bonding and attachment Parental mental health Change in level of anxiety |
| Setting | Neonatal Unit |
| First Author, Year | Country | Number of Participants | Study Design | Gestation at Birth (Weeks) | Postconceptional Age at Time of Intervention | Form of Brain Injury | Intervention: From of Stimulation Received/ Lead Administrator of Invention | Duration per Session/Occurrence Study Duration | Outcomes Measured | Results |
|---|---|---|---|---|---|---|---|---|---|---|
| Chirico, G., 2017 [36] | Italy | 40 | RCT | Group 1: 29.4 ± 2.6 Control: 30.8 ± 2.4 (Mean age) | Group 1: 33.4 ± 2.0 Control: 33.3 ± 1.9 (Mean wks.) | Includes those with IVH grade I &II (percentage of population unspecified) | Exposure to recordings of mother’s voice (lullabies and nursery rhymes) Healthcare professional led | 10 min 2 times daily Study duration: 3 days | Premature infant pain profile, heart rate, oxygen saturation, blood pressure, side effects: apnoea, bradycardia, seizures and vomiting. | Infants in treatment group had lower PIPP scores (p = 0.00002) and lower decrease in oxygen saturations (p = 0.0283). No significant side effects were observed. |
| Chorna, O.D., 2014 [35] | USA | 94 | RCT | Median: Group 1: 30 Control: 30 | Percentage of 34 completed weeks: Group 1: 93% Control: 98% | White matter injury (all types): Intervention 17% Control 19% White matter injury, severe (PVL/IVH grade III and IV): Intervention 4% Control 6% | Pre-recorded mothers singing on Pacifier Activated Music player (PAM) Music therapist support for recording of mother’s voices. Intervention the activated by infant’s suck and monitored by nursing staff. | 15 min daily Study duration: 5 days | Feeding rate, suck pressure, number of completed feeds, weight on discharge | Musical intervention increased oral feeding rate (2.0 vs. 0.9 mL/min p < 0.001), oral volume intake (91.1 vs. 48.1 mL/kg/d, p = 0.001) oral feeds/day (6.5 vs 4.0, p < 0.001) and faster time to full oral feedings (31 vs. 28 d, p = 0.04) compared to controls. |
| Doheny, L., 2012 [37] | USA | 14 | Cohort | Mean 30.2 ± 2.07 | Mean wks.: 31.1 ± 2.06 | 7.1% with Grade III or IV IVH | Exposure to pre-recorded maternal voice with heartbeat Healthcare professional led. Nursing staff administered sounds avoiding parent visits and clinical exams. | Four sessions of 30 min for each observed 24 h period per week Duration of study: 24 hperiod observed for a mean period of 42.9 ± 25.07 days. | Frequency of cardiorespiratory events (CRE) | Decrease in trend in CRE with age. With maternal sounds a lower frequency of CRE were observed. This was most evident in infants ≥33 weeks postmenstrual age (p = 0.03). |
| Emery, L., 2018 [52] | USA | 24 | RCT | Median 28.5 | 49.5 weeks | IVh grade I–IV 13% | Developmental music therapy Music therapist led | Group A: 2 sessions per week for 4 weeks, a minimum of one day of no therapy between sessions Group B: 4 sessions for weeks 1 and 3, no sessions on weeks 2 and 4 Duration of study: 4 weeks | Comparison of intensive versus standard spaced protocolised music therapy on developmental milestone acquisition | Developmental MT supports developmental skill acquisition. Intensity of intervention had no effect on the degree of skill attained. |
| Epstein, S., 2020 [44] | Germany | 35 | RCT | Mean: 27 ± 2.5 | Mean wks.: Group 1: 32 ± 3.5 Control: 31 ± 2.7 | IVH grade III 45% IVH grade IV 29%, PVL 26% | Maternal singing alone compared to singing combined with skin to skin Music therapist led | Three sessions 20 min Duration of study time (days): Skin to skin group 18 ± 3.2 Skin to skin with MT 20 ± 2.1 | Oxygen Saturation, Respiratory rate, behavioural state, mothers’ anxiety (STAI score) | Skin to skin with maternal singing: Higher mean ± standard deviation (SD) LF/HF ratio (1.8 ± 0.7 vs. 1.1 ± 0.25, p = 0.01), higher mean ± SD heart rate (145 ± 15 vs. 132 ± 12 beats per minute, p = 0.04), higher median infant behaviour state (NIDCAP manual for naturalistic observation and the Brazelton Neonatal Behavioural Assessment) score (3 (2–5) vs. 1 (1–3), p = 0.03) and higher mean ± SD maternal anxiety (state-trait anxiety inventory) score (39.1 ± 10.4 vs. 31.5 ± 7.3, p = 0.04) |
| Konar, M.C., 2021 [38] | India | 3095 | RCT | Group A: 34.3 ± 3.1 Group B: 34.5 ± 3.0 | Not stated | Stages of HIE Experimental group: I 50.8% II 34.5% III 14.7% Control group: I 50.2% II 34.7% III 11.6% | Exposure to recordings of Rabindra Sangeet (guitar) Healthcare professional led on the unit/caregiver led after discharge. | 4 sessions daily 25–30 min Duration of study time: On the unit: Experimental group 13.1 ± 2.3 Control 16 ± 2.1 Followed up after discharge at 3, 6, 12, 18, and 24 months. | Hospital stay, oxygen dependency, refractory convulsion, apnoea, cumbersome method, pain score (N-PASS), motor neurodevelopmental quotient (DASII) | Mean hospital stay, oxygen dependency, requirement of mechanical ventilation and frequency of apnoea and pain score were lower with music intervention. Additionally, the group receiving musical intervention showed better neurodevelopmental results at all stages (3, 6, 12, 18 and 24 months) |
| Letzkus, L., 2021 [53] | USA | 11 | Feasibility | Median 27 ±2.85 ± 2.85 | Different stages of bundle started at different ages: 23–25 week- Vocal soothing, Scent exchange, comforting touch 26–28 weeks: addition of kangaroo care 29–32 weeks: infant massage when deemed appropriate | IVH 58.3% (Total n = 7: unilateral IVH n = 4, bilateral IVH n = 3. Grade I/II n = 6, Grade II/III n = 1) Cystic periventricular leukomalacia 16.6% | Maternal vocal soothing as part of NICU-bundle (vocal soothing, scent exchange, comforting touch) Healthcare professional with familiarity of the Family Nuture Intervention led. Additional education in the form of intervention and method flip book. | Minimum 5 days per week. Duration of study: Median 8 weeks | Feasibility of carrying out bundle 5 days/week, Maternal stress and anxiety, Short-term Motor outcomes (GMA/HINE) | Vocal soothing, scent exchange and comforting touch were performed at or above the predetermined goal of 71% of time (5/7 days), kangaroo care and infant massage were not. Decrease in maternal stress, anxiety and depression during the study. |
| Nelson, M.N., 2001 [54] | USA | 37 | RCT | Mean VLBW Experimental: 25.45 ± 1.13 Control: 25.60 ± 1.52 PVL: Experimental: 27.20 ± 2.82 Control: 27.27 ± 2.37 | Mean VLBW Experimental: 33.64 ± 0.5 Control: 33.60 ± 0.98 PVL: Experimental: 33.40 ±1.07 Control: 33.64 ± 0.92 | IVH (grade III/IV) Or IVH (grade III/IV) with PVL Or PVL alone. | Spoken female voice as part of auditory-tactile- visual-vestibular Intervention Caregiver led. | Two sessions daily/5 days per week 15 min 70% of infants completed the intervention for 12 months | One year developmental outcomes Mother-infant interactions (Dyadic Mutuality Code and Nursing Feeding assessment scale) | PVL was associated with poorer development regardless of group assignment. Experimental infants had 23% fewer cerebral palsy diagnoses at 1 year. No significant difference between VLBW group and PVL group in early mother-infant interaction. |
| Sa de Almeida, 2020 [46] | Switzerland | 45 | RCT | Mean: FT: 39.2 ± 1.3 PTM: 28.58 ± 2.3 PTC: 28.30 ± 2.3 | From 33 weeks until discharge Age at MRI: FT: 39.54 PTM: 40.15 ± 0.6 PTC: 40.48 ± 0.6 | IVH grade I and II included (Percentage) FT: 0 PTM: 26.7% PTC: 6.7% | Exposure to music by Vollenweider (instrumental) through headphones Healthcare professional led. | Eight minutes for a mean 4.84 ± 1.18 per week Total duration of days on study unspecified. | White matter maturation, T2-weighted image (amygdala volumetric analysis) | Improvement in white-matter maturation in acoustic regions, external capsule/claustrum/extreme capsule and uncinate fasciculus as well as larger amygdala volumes in preterm infants exposed to music intervention. |
| White-Traut, R., 1999 [55] | USA | 30 | RCT | Mean wks. Control: 29.7 ± 2.06 Experimental: 27.9 ± 2.33 | Mean wks. Control: 33.7 ± 0.59 Experimental: 33.5 ± 0.74 | PVL Acute/Cystic Control: 6/9 Experimental 9/6 | Female voice as part of multisensory intervention (auditory, tactile, visual and vestibular) Research assistant led | Fifteen minutes twice a day, 5 days a week Duration of study: 4 weeks | Neurobehavior (Brazelton neonatal behavioural assessment scale) and neurodevelopment (Bayley scales of infant development) | Experimental group demonstrated a significant shift from sleep to alert during the intervention. No injury was sustained by the experimental group. Average hospital stay of the experimental group was 9 days shorter than controls. |
| White-Traut, R., 2003 [45] | USA | 37 | RCT | Mean wks. Group 1: 26.29 ± 2.239 Control: 26.75 ± 2.236 | Mean wks. Group 1: 33.524 ± 0.814 Control: 33.625 ± 0.885 | PVL/IVH grade III/IV/PVL&IVH grade III/IV | Female voice as part of multisensory intervention (voice with eye contact and stroking followed by rocking) Research assistant led | Twice daily until discharge 15 min in total per intervention Observed for 2 weeks (33–35 postconceptional age) | Heart rate, respiratory rate, haemoglobin oxygen saturation | Those without central nervous system injury demonstrated a decrease in resting mean heart rate with stable respiratory rate and oxygen saturation. Infants with PVL showed increase in heart rate post-intervention. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ormston, K.; Howard, R.; Gallagher, K.; Mitra, S.; Jaschke, A. The Role of Music Therapy with Infants with Perinatal Brain Injury. Brain Sci. 2022, 12, 578. https://doi.org/10.3390/brainsci12050578
Ormston K, Howard R, Gallagher K, Mitra S, Jaschke A. The Role of Music Therapy with Infants with Perinatal Brain Injury. Brain Sciences. 2022; 12(5):578. https://doi.org/10.3390/brainsci12050578
Chicago/Turabian StyleOrmston, Kirsty, Rachel Howard, Katie Gallagher, Subhabrata Mitra, and Arthur Jaschke. 2022. "The Role of Music Therapy with Infants with Perinatal Brain Injury" Brain Sciences 12, no. 5: 578. https://doi.org/10.3390/brainsci12050578