
Opicapone Improves Global Non-Motor Symptoms Burden in Parkinson’s Disease: An Open-Label Prospective Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Data Analysis
2.2. Standard Protocol Approvals, Registrations, and Patient Consents
2.3. Data Availability
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Dorsey, E.R.; Bloem, B.R. The Parkinson Pandemic—A Call to Action. JAMA Neurol. 2018, 75, 9–10. [Google Scholar] [CrossRef] [PubMed]
- Tolosa, E.; Gaig, C.; Santamaría, J.; Compta, Y. Diagnosis and the premotor phase of Parkinson’s disease. Neurology 2009, 72 (Suppl. 7), 12–20. [Google Scholar] [CrossRef] [PubMed]
- Bloem, B.R.; Okun, M.S.; Klein, C. Parkinson’s disease. Lancet 2021, 397, 2284–2303. [Google Scholar] [CrossRef]
- Santos García, D.; de Deus Fonticoba, T.; Suárez Castro, E.; Borrué, C.; Mata, M.; Solano Vila, B.; Cots Foraster, A.; Álvarez Sauco, M.; Coppadis Study Group. Non-motor symptoms burden, mood, and gait problems are the most significant factors contributing to a poor quality of life in non-demented Parkinson’s disease patients: Results from the COPPADIS Study Cohort. Parkinsonism Relat. Disord. 2019, 66, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Seppi, K.; Weintraub, D.; Coelho, M.; Perez-Lloret, S.; Fox, S.H.; Katzenschlager, R.; Hametner, E.-M.; Poewe, W.; Rascol, O.; Goetz, C.G.; et al. The Movement Disorder Society Evidence-Based Medicine Review Update: Treatments for the non-motorsymptoms of Parkinson’s disease. Mov. Disord. 2011, 26 (Suppl. 3), S42–S80. [Google Scholar] [CrossRef]
- Santos García, D.; De Deus Fonticoba, T.; Paz González, J.M.; Bartolome, C.C.; Aymerich, V.; Enriquez, M.; Suárez, E.; Jesus, S.; Aguilar, M.; Pastor, P.; et al. Staging Parkinson’s Disease Combining Motor and Nonmotor Symptoms Correlates with Disability and Quality of Life. Parkinsons Dis 2021, 2021, 8871549. [Google Scholar] [CrossRef] [PubMed]
- Santos-García, D.; de Deus, T.; Cores, C.; Canfield, H.; Paz González, J.M.; Miro, C.M.; Aymerich, L.V.; Suarez, E.; Jesus, S.; Coppadis Study Group; et al. Predictors of Global Non-Motor Symptoms Burden Progression in Parkinson’s Disease. Results from the COPPADIS Cohort at 2-Year Follow-Up. J. Pers. Med. 2021, 11, 626. [Google Scholar] [CrossRef]
- Santos-García, D.; de Deus Fonticoba, T.; Suárez Castro, E.; McAfee, D.; Catalán, F.; Alonso-Frech, C.; Villanueva, S.; Jesús, P.; Mir, M.; Aguilar, P.; et al. Non-motor symptom burden is strongly correlated to motor complications in patients with Parkinson’s disease. Eur. J. Neurol 2020, 27, 1210–1223. [Google Scholar] [CrossRef]
- Magalona, S.C.; Rasetti, R.; Chen, J.; Chem, Q.; Gold, I.; Decot, H.; Callicott, J.H.; Berman, K.F.; Apud, J.A.; Weinberger, D.R.; et al. Effect of tolcapone on brain activity during a variable attentional control task: A double-blind, placebo-controlled, counter-balanced trial in healthy volunteers. CNS Drugs 2013, 27, 663–673. [Google Scholar] [CrossRef] [Green Version]
- Apud, J.A.; Mattay, V.; Chen, J.; Kolachana, B.S.; Callicot, J.H.; Rasetti, R.; Alce, G.; Iudicello, J.E.; Akbar, N.; Ega, M.F.; et al. Tolcapone improves cognition and cortical information processing in normal human subjects. Neuropsychopharmacology 2007, 32, 1011–1020. [Google Scholar] [CrossRef]
- Reichmann, H.; Lees, A.; Rocha, J.F.; Magalhães, D.; Soares-da-Silva, P.; OPTIPARK investigators. Effectiveness and safety of opicapone in Parkinson’s disease patients with motor fluctuations: The OPTIPARK open-label study. Transl. Neurodegener. 2020, 9, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiss, L.E.; Ferreira, H.S.; Torrão, L.; Bonifácio, M.J.; Palma, P.N.; Soares-da-Silva, P.; Learmonth, D.A. Discovery of a long-acting, peripherally selective inhibitor of catechol-O-methyltransferase. J. Med. Chem. 2010, 53, 3396–3411. [Google Scholar] [CrossRef] [PubMed]
- Fabbri, M.; Rosa, M.M.; Ferreira, J.J. Clinical pharmacology review of opicapone for the treatment of Parkinson’s disease. Neurodegener. Dis. Manag. 2016, 6, 349–362. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, J.J.; Lees, A.; Rocha, J.F.; Poewe, W.; Rascol, O.; Soares-da-Silva, P.; Bi-Park 1 Investigators. Opicapone as an adjunct to levodopa in patients with Parkinson’s disease and end-of-dose motor fluctuations: A randomised, double-blind, controlled trial. Lancet Neurol. 2016, 15, 154–165. [Google Scholar] [CrossRef]
- Lees, A.J.; Ferreira, J.; Rascol, O.; Poewe, W.; Rocha, J.-F.; McCrory, M.; Soares-da-Silva, P.; BIPARK-2 Study Investigators. Opicapone as Adjunct to Levodopa Therapy in Patients with Parkinson Disease and Motor Fluctuations: A Randomized Clinical Trial. JAMA Neurol. 2017, 74, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Costa, R.; Oliveira, C.; Pinto, R.; Lopes, N.; Nunes, T.; Rocha, F.; Soares-da-Silva, P. Opicapone long-term efficacy and safety in Parkinson´s disease BIPARK-II study: A one year open-label follow up. J. Neurol. 2014, 261, S119. [Google Scholar]
- Gama, H.; Ferreira, J.; Lees, A. Evaluation of the safety and tolerability of opicapone in the treatment of Parkinson´s disease and motor fluctuations: Analysis of pooled Phase III studies. Eur. J. Neurol. 2015, 22, 611. [Google Scholar]
- Oliveira, C.; Lees, A.; Ferreira, J. Evaluation of non-motor symptoms in opicapone treated Parkinson’s disease patients: Results from a double-blind, randomized, controlled-study and open-label extention. Eur. J. Neurol. 2015, 22, 191. [Google Scholar]
- Hughes, A.J.; Daniel, S.E.; Kilford, L.; Lees, A.J. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: A clinico-pathological study of 100 cases. J. Neurol. Neurosurg. Psychiatry 1992, 55, 181–184. [Google Scholar] [CrossRef] [Green Version]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression and mortality. Neurology 1967, 17, 427–442. [Google Scholar] [CrossRef] [Green Version]
- Fahn, S.; Elton, R.L.; Members of the UPDRS Development Committee. Unified Parkinson’s Disease Rating Scale. Recent Developments in Parkinson’s Disease; Fahn, S., Marsden, C.D., Calne, D.B., Goldstein, M., Eds.; Macmillan Health Care Information: Florham Park, NJ, USA, 1987; Volume 2, pp. 153–164. [Google Scholar]
- Giladi, N.; Shabtai, H.; Simon, E.S.; Biran, S.; Tal, J.; Korczyn, A.D. Construction of freezing of gait questionnaire for patients with Parkinsonism. Parkinsonism Relat. Disord. 2000, 6, 165–170. [Google Scholar] [CrossRef]
- Chaudhuri, K.R.; Martinez-Martin, P.; Brown, R.G.; Sethi, K.; Stocchi, F.; Odin, P.; Abe, K.; MacPhee, G.; MacMahon, D.; Barone, P.; et al. The metric properties of a novel non-motor symptoms scale for Parkinson’s disease: Results from an international pilot study. Mov Disord. 2007, 22, 1901–1911. [Google Scholar] [CrossRef] [PubMed]
- Chaudhuri, K.R.; Pal, S.; DiMarco, A.; Whately-Smith, C.; Bridgman, K.; Mathew, R.; Pezzela, F.R.; Forbes, A.; Hög, B.; Trenkwalder, C. The Parkinson’s disease sleep scale: A new instrument for assessing sleep and nocturnal disability in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2002, 73, 629–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Starkstein, S.E.; Mayberg, H.S.; Preziosi, T.J.; Andrezejewski, P.; Leiguarda, R.; Robinson, R.G. Reliability, validity, and clinical correlates of apathy in Parkinson’s disease. J. Neuropsychiatry Clin. Neurosci. 1992, 4, 134–139. [Google Scholar]
- Chaudhuri, K.R.; Rizos, A.; Trenkwalder, C.; Rascol, O.; Pal, S.; Martino, D.; Carrol, C.; Paviour, D.; Faluo-Pecurariou, C.; Kessel, B.; et al. King’s Parkinson’s disease pain scale, the first scale for pain in PD: An international validation. Mov. Disord. 2015, 30, 1623–1631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burckhardt, C.S.; Jones, K.D. Adult measures of pain: The McGill Pain Questionnaire (MPQ), Rheumatoid Arthritis Pain Scale (RAPS), Short Form McGill Pain Questionnaire (SF-MPQ), Verbal Descriptive Scale (VDS), Visual Analog Scale (VAS), and West Haven-Yale Multidisciplinary Pain Inventory (WHYMPI). Arthritis Rheum. 2003, 49, S96–S104. [Google Scholar]
- Schwab, R.S.; England, A.C. Projection Technique for Evaluating Surgery in Parkinson’s Disease. In Proceedings of the Third Symposium on Parkinson’s Disease, Edinburgh, UK, 20–22 May 1968; E. & S. Livingstone: Edinburgh, UK, 1969; pp. 152–157. [Google Scholar]
- Jenkinson, C.; Fitzpatrick, R.; Peto, V.; Greenhall, R.; Hyman, N. The Parkinson’s Disease Questionnaire (PDQ-39): Development and validation of a Parkinson’s disease summary index score. Age Ageing 1997, 26, 353–357. [Google Scholar] [CrossRef] [Green Version]
- Guy, W. ECDEU Assessment Manual for Psychopharmacology; National Institute of Mental Health. Psychopharmacology Research Branch, Division of Extramural Research Programs, Ed.; U.S. Deptartment of Health, Education and Welfare, Public Health Service, Alcohol, Drug Abuse and Mental Health Administration, National Institute of Mental Health, Psychopharmacology Research Branch, Division of Extramural Research Programs: Rockville, MD, USA, 1976; pp. 218–222. [Google Scholar]
- Schade, S.; Mollenhauer, B.; Trenkwalder, C. Levodopa Equivalent Dose Conversion Factors: An Updated Proposal Including Opicapone and Safinamide. Mov. Disord. Clin. Pract. 2020, 7, 343–345. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Martin, P.; Rodriguez-Blazquez, C.; Kurtis, M.M.; Chaudhuri, K.R.; NMSS Validation Group. The impact of non-motor symptoms on health-related quality of life of patients with Parkinson’s disease. Mov. Disord. 2011, 26, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Chaudhuri, K.R.; Schapira, A.H. Non-motor symptoms of Parkinson’s disease: Dopaminergic pathophysiology and treatment. Lancet. Neurol. 2009, 8, 464–474. [Google Scholar] [CrossRef]
- Mattay, V.; Tessitore, A.; Callicott, J.; Bertolino, A.; Goldberg, T.E.; Chase, T.N.; Daniel, H.; Weinberger, D.R. Dopaminergic modulation of cortical function in patients with Parkinson’s disease. Ann. Neurol. 2002, 51, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Barone, P.; Scarzella, L.; Marconi, R.; Antonini, A.; Morgante, L.; Bracco, F.; Zappia, M.; Musch, B.; The Depression/Parkinson Italian Study Group. Pramipexole versus sertraline in the treatment of depression in Parkinson’s disease: A national multicenter parallel group randomized study. J. Neurol. 2006, 253, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Pajarín, G.; Sesar, Á.; Jiménez Martín, I.; Ares, B.; Castro, A. Continuous subcutaneous apomorphine infusion in the early phase of advanced Parkinson’s disease: A prospective study of 22 patients. Clin. Park. Relat. Disord. 2021, 6, 100129. [Google Scholar] [CrossRef] [PubMed]
- Trenkwalder, C.; Kies, B.; Rudzinska, M.; Fine, J.; Nikl, J.; Honczarenko, K.; Dioszeghy, P.; Hill, D.; Anderson, T.; Myllyla, V.; et al. Rotigotine effects on early morning motor function and sleep in Parkinson’s disease: A double-blind, randomized, placebo-controlled study (RECOVER). Mov. Disord. 2011, 26, 90–99. [Google Scholar] [CrossRef] [PubMed]
- Müller, T.; TANIMOS Study Investigators. Tolcapone addition improves Parkinson’s disease associated nonmotor symptoms. Ther. Adv. Neurol. Disord. 2014, 7, 77–82. [Google Scholar] [CrossRef] [Green Version]
- Artusi, C.A.; Sarro, L.; Imbalzano, G.; Fabbri, M.; Lopiano, L. Safety and efficacy of tolcapone in Parkinson’s disease: Systematic review. Eur. J. Clin. Pharmacol. 2021, 77, 817–829. [Google Scholar] [CrossRef]
- Martínez-Fernández, R.; Schmitt, E.; Martinez-Martin, P.; Krack, P. The hidden sister of motor fluctuations in Parkinson’s disease: A review on nonmotor fluctuations. Mov. Disord. 2016, 31, 1080–1094. [Google Scholar] [CrossRef]
- Witjas, T.; Kaphan, E.; Azulay, J.P.; Blin, O.; Ceccaldi, M.; Pouget, J.; Poncet, M.; Ali Chérif, A. Nonmotor fluctuations in Parkinson’s disease: Frequent and disabling. Neurology 2002, 59, 408–413. [Google Scholar] [CrossRef]
- Jenner, P.; Rocha, J.F.; Ferreira, J.J.; Rascol, O.; Soares-da-Silva, P. Redefining the strategy for the use of COMT inhibitors in Parkinson’s disease: The role of opicapone. Expert Rev. Neurother. 2021, 2, 1019–1033. [Google Scholar] [CrossRef]
- Takeda, A.; Takahashi, R.; Tsuboi, Y.; Nomoto, M.; Maeda, T.; Nishimura, A.; Yoshida, K.; Hattori, N. Randomized, controlled study of opicapone in Japanese Parkinson’s patients with motor fluctuations. Mov. Disord. 2021, 36, 415–423. [Google Scholar] [CrossRef]
- Lees, A.J.; Ferreira, J.; Rascol, O.; Reichmann, H.; Stocchi, F.; Tolosa, E.; Poewe, W. Opicapone for the management of end-of-dose motor fluctuations in patients with Parkinson’s disease treated with L-DOPA. Expert Rev. Neurother. 2017, 17, 649–659. [Google Scholar] [CrossRef] [PubMed]
- Fabbri, M.; Ferreira, J.J.; Lees, A.; Stocchi, F.; Poewe, W.; Tolosa, E.; Rascol, O. Opicapone for the treatment of Parkinson’s disease: A review of a new licensed medicine. Mov. Disord. 2018, 33, 1528–1539. [Google Scholar] [CrossRef] [PubMed]
- Scott, L.J. Opicapone: A review in Parkinson’s disease. CNS Drugs 2021, 35, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Santos García, D.; Labandeira Guerra, C.; Yáñez Baña, R.; Cimas Hernando, M.I.; López, I.C.; Paz Gonález, J.M.; Alonso Losada, M.G.; González Palmás, M.J.; Miró, C.M. Safinamide Improves Non-Motor Symptoms Burden in Parkinson’s Disease: An Open-Label Prospective Study. Brain Sci. 2021, 11, 316. [Google Scholar] [CrossRef] [PubMed]
- López-Ariztegui, N.; Mata-Alvarez Santullano, M.; Tegel, I.; Almedia, F.; Sarasa, P.; Rojo, R.; Rico-Villademoros, F.; Abril Jaramillo, J.; Bermejo, P.; Borrúe, C.; et al. Opicapona para el tratamiento de la enfermedad de Parkinson: Datos de vida real en España (Opicapone for the treatment of Parkinson’s disease: Real-life data in Spain). Rev. Neurol. 2021, 73, 1–14. [Google Scholar]
- Smulders, K.; Dale, M.L.; Carlson-Kuhta, P.; Nutt, J.G.; Horak, F.B. Pharmacological treatment in Parkinson’s disease: Effects on gait. Parkinsonism Relat. Disord. 2016, 31, 3–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Napolitano, A.; Del Dotto, P.; Petrozzi, L.; Dell’Agnello, G.; Bellini, G.; Gambaccini, G.; Bonuccelli, U. Pharmacokinetics and pharmacodynamics of L-Dopa after acute and 6-week tolcapone administration in patients with Parkinson’s disease. Clin. Neuropharmacol. 1999, 22, 24–29. [Google Scholar] [CrossRef]
- Ondo, W.G.; Hunter, C.; Vuong, K.D.; Jankovic, J. The pharmacokinetic and clinical effects of tolcapone on a single dose of sublingual apomorphine in Parkinson’s disease. Parkinsonism Relat. Disord. 2000, 6, 237–240. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Age | 63.3 ± 7.91 (48–77) | Time from symptoms onset | 7.48 ± 4.22 (2–20) |
| Gender (males) (%) | 60.6 | ||
| Ethnicity (%) | Motor fluctuations (%) | 97 | |
| - Caucasian | 97 | Dyskinesia (%) | 42.4 |
| - Other | 3 | ||
| Treatment for PD (%): | |||
| Civil status (%): | - Levodopa | 100 | |
| - Married | 78.8 | - MAO-B inhibitor | 63.6 |
| - Widowed | 3 | - Dopamine agonists: | 66.7 |
| - Single | 6.1 | * Pramipexole | 33.3 |
| - Divorced | 9.1 | * Ropinirole | 12.1 |
| - Other | 3 | * Rotigotine | 21.2 |
| - Amantadine | 9.1 | ||
| Living style (%) | - Anticholinergic drug | 3 | |
| - With the partner | 75.8 | ||
| - With another family member | 6.1 | L-dopa daily dose (mg) | 648.46 ± 372.44 (200–1792) |
| - With a son/daughter | 6.1 | DA daily dose (mg) | 162.84 ± 161.03 (0–630) |
| - Other | 12 | LEDD (mg) | 820.89 ± 323.31 (350–1812) |
| Habitat (%): | Other treatments (%): | ||
| - Rural (<5.000) | 21.2 | - Antidepressant | 24.2 |
| - Semiurban (5.000–20.000) | 24.2 | - Benzodiazepine | 36.4 |
| - Urban (>20.000) | 54.6 | - Antipsychotic | 0 |
| - Analgesic | 21.2 | ||
| Comorbidities (%): | |||
| - Arterial hypertension | 39.4 | Number of anti-PD drugs | 2.75 ± 1.14 (1–5) |
| - Diabetes mellitus | 15.2 | Number of non-PD drugs | 2.51 ± 2.56 (0–9) |
| - Dyslipemia | 27.3 | Total number of drugs | 5.24 ± 2.92 (1–11) |
| - Hiperuricemia | 3 | Number of pills for PD | 5.82 ± 1.6 (3–9) |
| - Cardiomyopathy | 6 | N. of pills for other cause | 2.54 ± 2.69 (0–9.5) |
| - Cardiac arrhythmia | 12.1 | Total number of pills | 8.37 ± 3.24 (3–18.5) |
| - Smoking | 9.1 | ||
| - Alcohol consumption | 18.2 |
| V0 | V2 | Cohen’s d | ∆ V0–V2 | p | |
|---|---|---|---|---|---|
| MOTOR ASSESSMENT | |||||
| H&Y-OFF | 2.5 [2, 3] | N. A. | N. A. | N. A. | N. A. |
| H&Y-ON | 2 [1.5, 2] | N. A. | N. A. | N. A. | N. A. |
| UPDRS-III-ON | 21.61 ± 13.17 | N. A. | N. A. | N. A. | N. A. |
| UPDRS-IV | 4.48 ± 2.09 | 3.87 ± 2.5 | −0.38 | −13.6% | 0.083 |
| FOGQ | 7.42 ± 5.62 | 6.03 ± 5.41 | −0.56 | −18.7% | 0.018 |
| NON MOTOR ASSESSMENT | |||||
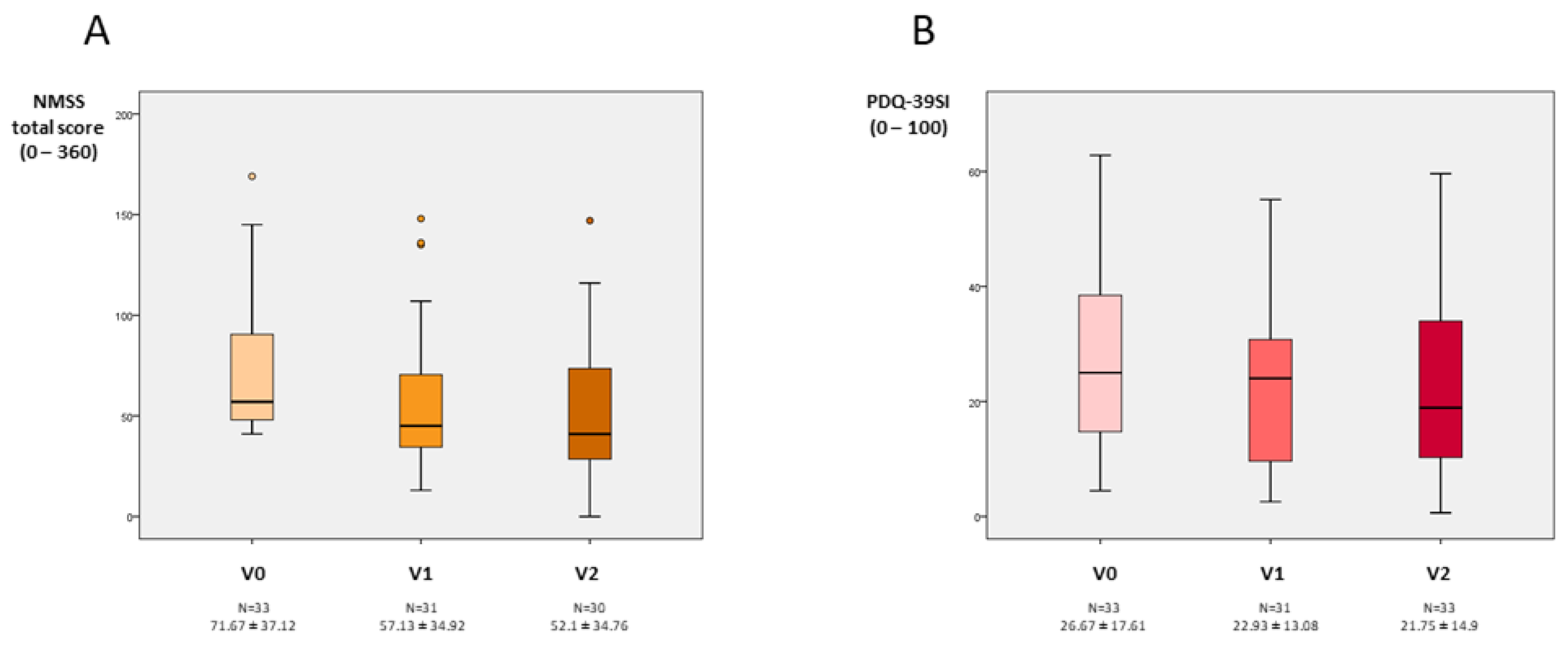
| NMSS total score | 71.67 ± 37.12 | 52.1 ± 34.76 | −0.97 | −27.3% | 0.002 |
| - Cardiovascular | 5.3 ± 9.21 | 4.03 ± 6.03 | −0.24 | −23.9% | 0.346 |
| - Sleep/fatigue | 33.08 ± 19.02 | 19.82 ± 16.4 | −1.06 | −40.1% | <0.0001 |
| - Mood/apathy | 22.22 ± 22.58 | 11.87 ± 14.82 | −0.87 | −46.6% | 0.001 |
| - Perceptual symptoms | 1.59 ± 4.76 | 1.88 ± 4.5 | +0.12 | +18.2% | 0.334 |
| - Attention/memory | 13.55 ± 15.8 | 8.6 ± 19.62 | −0.32 | −36.5% | 0.091 |
| - Gastrointestinal symptoms | 19.44 ± 16.27 | 15.41 ± 16.36 | −0.56 | −20.7% | 0.029 |
| - Urinary symptoms | 32.57 ± 26.01 | 34.49 ± 26.02 | +0.09 | +5.8% | 0.726 |
| - Sexual dysfunction | 15.78 ± 26.2 | 22.98 ± 30.97 | +0.43 | +45.6% | 0.099 |
| - Miscellaneous | 21.96 ± 18.56 | 12.09 ± 14.11 | −0.65 | −44.94% | 0.021 |
| PDSS | 104.62 ± 22.51 | 108.48 ± 26.86 | +0.24 | +3.6% | 0.267 |
| AS | 13.76 ± 8.4 | 14.6 ± 8.71 | +0.11 | +6.1% | 0.801 |
| KPPS | 14.33 ± 13.5 | 10.47 ± 9.62 | −0.44 | −26.9% | 0.075 |
| - Musculoskeletal pain | 4.06 ± 3.46 | 3.47 ± 3.53 | −0.14 | −14.5% | 0.474 |
| - Chronic pain | 1.76 ± 3.51 | 0.63 ± 1.75 | −0.12 | −64.2% | 0.073 |
| - Fluctuation-related pain | 2.7 ± 4.24 | 1.23 ± 2.55 | −0.06 | −54.4% | 0.133 |
| - Nocturnal pain | 4.18 ± 6.44 | 2.93 ± 4.2 | −0.34 | −29.9% | 0.266 |
| - Oro-facial pain | 0.52 ± 1.46 | 0.43 ± 1.61 | −0.09 | −17.3% | 0.524 |
| - Discoloration, edema/swelling | 0.18 ± 0.72 | 0.53 ± 1.47 | +0.38 | +194.4% | 0.109 |
| - Radicular pain | 0.94 ± 2.35 | 1.23 ± 2.73 | +0.09 | +30.8% | 0.878 |
| VAS-PAIN | 4.09 ± 3.11 | 4.55 ± 2.5 | +0.41 | +11.2% | 0.187 |
| QOL AND AUTONOMY | |||||
| PDQ-39SI | 26.67 ± 17.61 | 21.75 ± 14.9 | −0.99 | −18.4% | 0.001 |
| - Mobility | 26.74 ± 19.62 | 24.16 ± 24.68 | −0.45 | −9.6% | 0.064 |
| - Activities of daily living | 26.01 ± 20.46 | 23.61 ± 19.82 | −0.33 | −8.9% | 0.130 |
| - Emotional well-being | 36.74 ± 26.95 | 26.94 ± 21.49 | −0.83 | −26.7% | 0.004 |
| - Stigmatization | 22.72 ± 27.41 | 14.37 ± 20.77 | −0.75 | −36.7% | 0.009 |
| - Social support | 12.37 ± 18.76 | 9.44 ± 15.43 | −0.39 | −23.6% | 0.244 |
| - Cognition | 28.41 ± 19.45 | 24.16 ± 25.2 | −0.25 | −14.9% | 0.306 |
| - Communication | 17.17 ± 20.61 | 16.94 ± 18.63 | −0.09 | −1.3% | 0.895 |
| - Pain and discomfort | 34.34 ± 21.52 | 23.33 ± 19.98 | −0.67 | −32.1% | 0.023 |
| ADLS | 80 ± 13.91 | 82.33 ± 14.54 | −0.35 | −2.9% | 0.197 |
| N | |
|---|---|
| Total AEs, N | 13 |
| - Dyskinesia | 2 |
| - Nausea | 2 |
| - Unrest | 1 |
| - Visual hallucinations | 1 |
| - Insomina | 1 |
| - Vivid dreams | 1 |
| - Tiredness | 1 |
| - Insomnia | 1 |
| - OFF time increase | 1 |
| - Arthritis in both wrists | 1 |
| - Supraspinatus tendonitis | 1 |
| Patients with at least one AE, N (%) | 11 (33.3) |
| At least possibly related AEs, N | 8 |
| Patients with at least possibly* related to opicapone AEs, N (%) | 7 (21.2) |
| Total SAEs, N | 1 |
| - Arthritis in both wrists | |
| Patients with al least one SAE, N (%) | 1 (3) |
| At least possibly * related to opicapone SAEs, N | 0 |
| Patients with at least possibly related to opicapone SAEs, N (%) | 0 (0) |
| Patients with at least one AE leading to discontinuation, N (%) | 2 (6.1) |
| Patients with at least one possibly* related to opicapone AE leading to discontinuation N (%) | 2 (6.1) |
| Deaths, N (%) | 0 (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos García, D.; Fernández Pajarín, G.; Oropesa-Ruiz, J.M.; Escamilla Sevilla, F.; Rahim López, R.R.A.; Muñoz Enríquez, J.G. Opicapone Improves Global Non-Motor Symptoms Burden in Parkinson’s Disease: An Open-Label Prospective Study. Brain Sci. 2022, 12, 383. https://doi.org/10.3390/brainsci12030383
Santos García D, Fernández Pajarín G, Oropesa-Ruiz JM, Escamilla Sevilla F, Rahim López RRA, Muñoz Enríquez JG. Opicapone Improves Global Non-Motor Symptoms Burden in Parkinson’s Disease: An Open-Label Prospective Study. Brain Sciences. 2022; 12(3):383. https://doi.org/10.3390/brainsci12030383
Chicago/Turabian StyleSantos García, Diego, Gustavo Fernández Pajarín, Juan Manuel Oropesa-Ruiz, Francisco Escamilla Sevilla, Raúl Rashid Abdul Rahim López, and José Guillermo Muñoz Enríquez. 2022. "Opicapone Improves Global Non-Motor Symptoms Burden in Parkinson’s Disease: An Open-Label Prospective Study" Brain Sciences 12, no. 3: 383. https://doi.org/10.3390/brainsci12030383