
Substance Use in the Transgender Population: A Meta-Analysis

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction
2.5. Summary Measures
2.6. Quality Assessment
2.7. Heterogeneity and Publication Bias
2.8. Sensitivity and Subgroup Analysis
3. Results
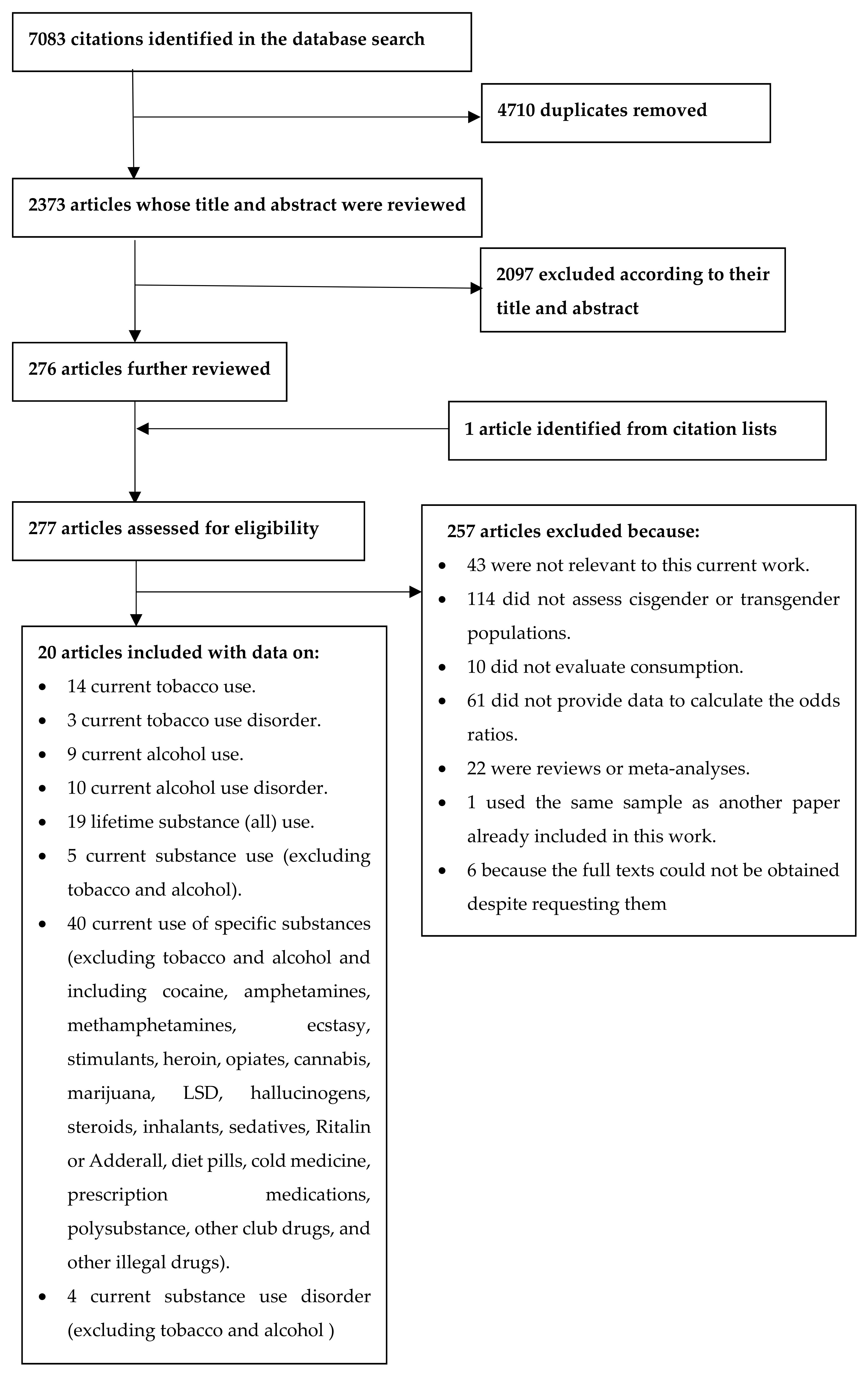
3.1. Studies Included
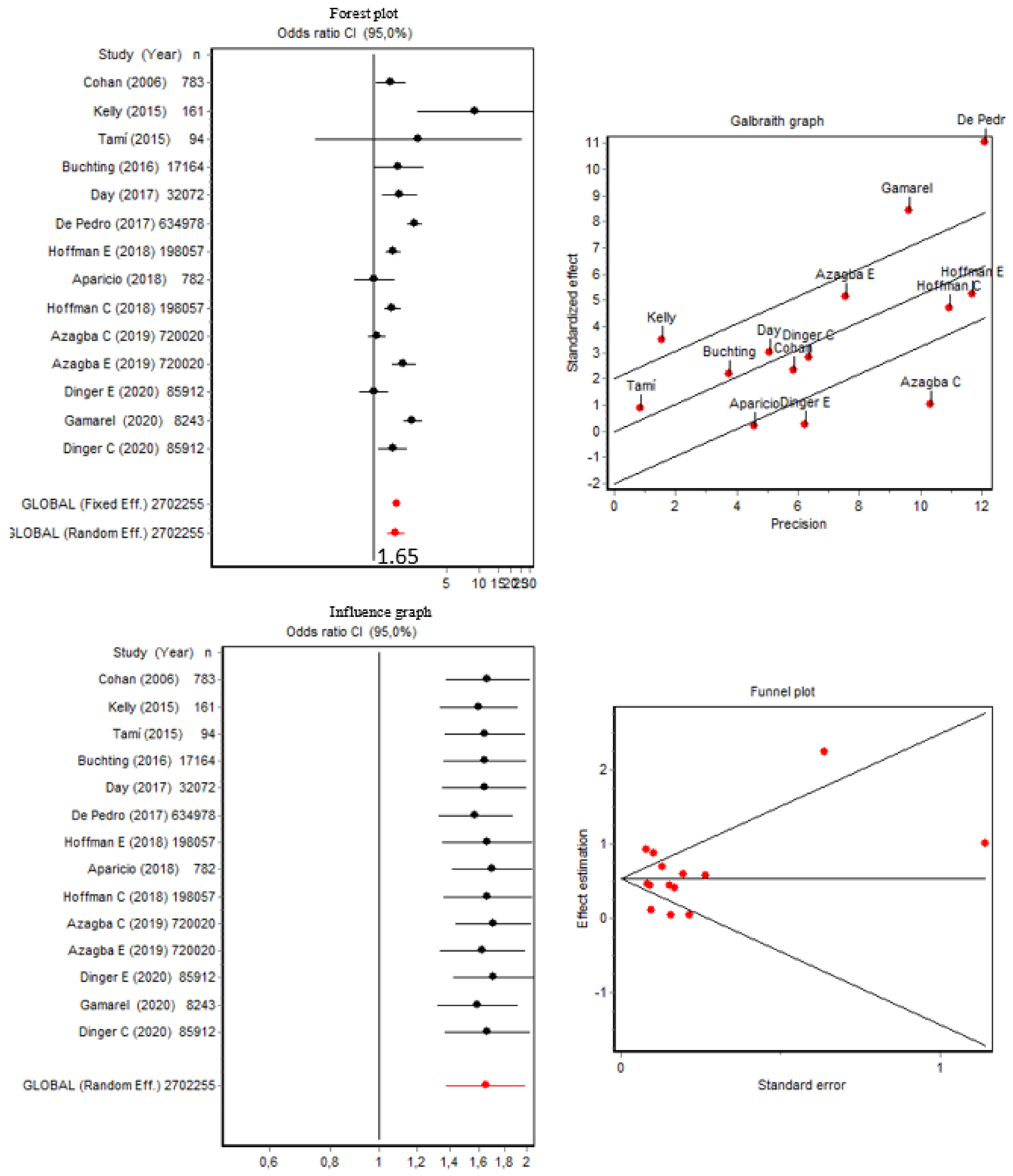
3.2. Current Tobacco Use and Tobacco Use Disorder
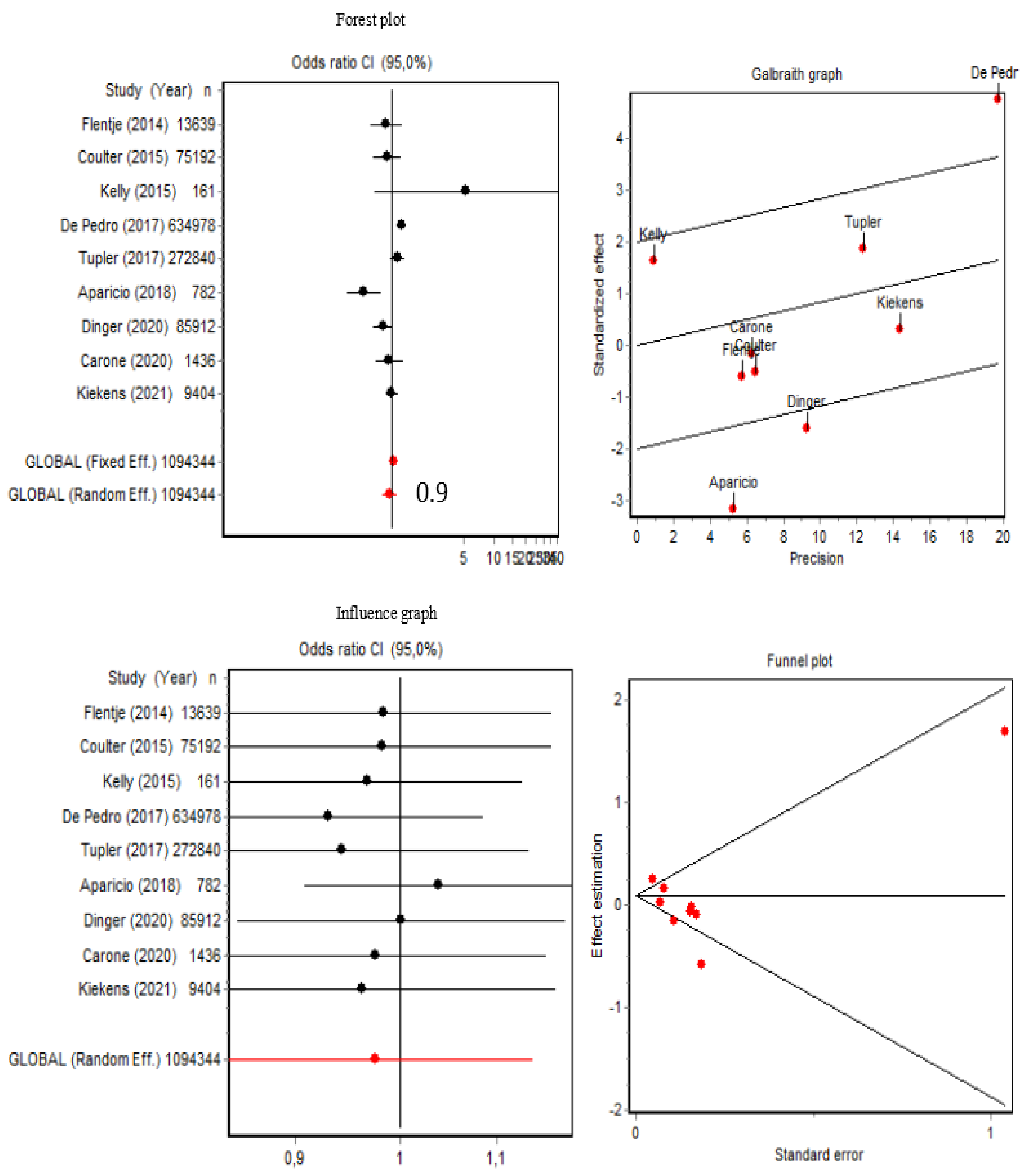
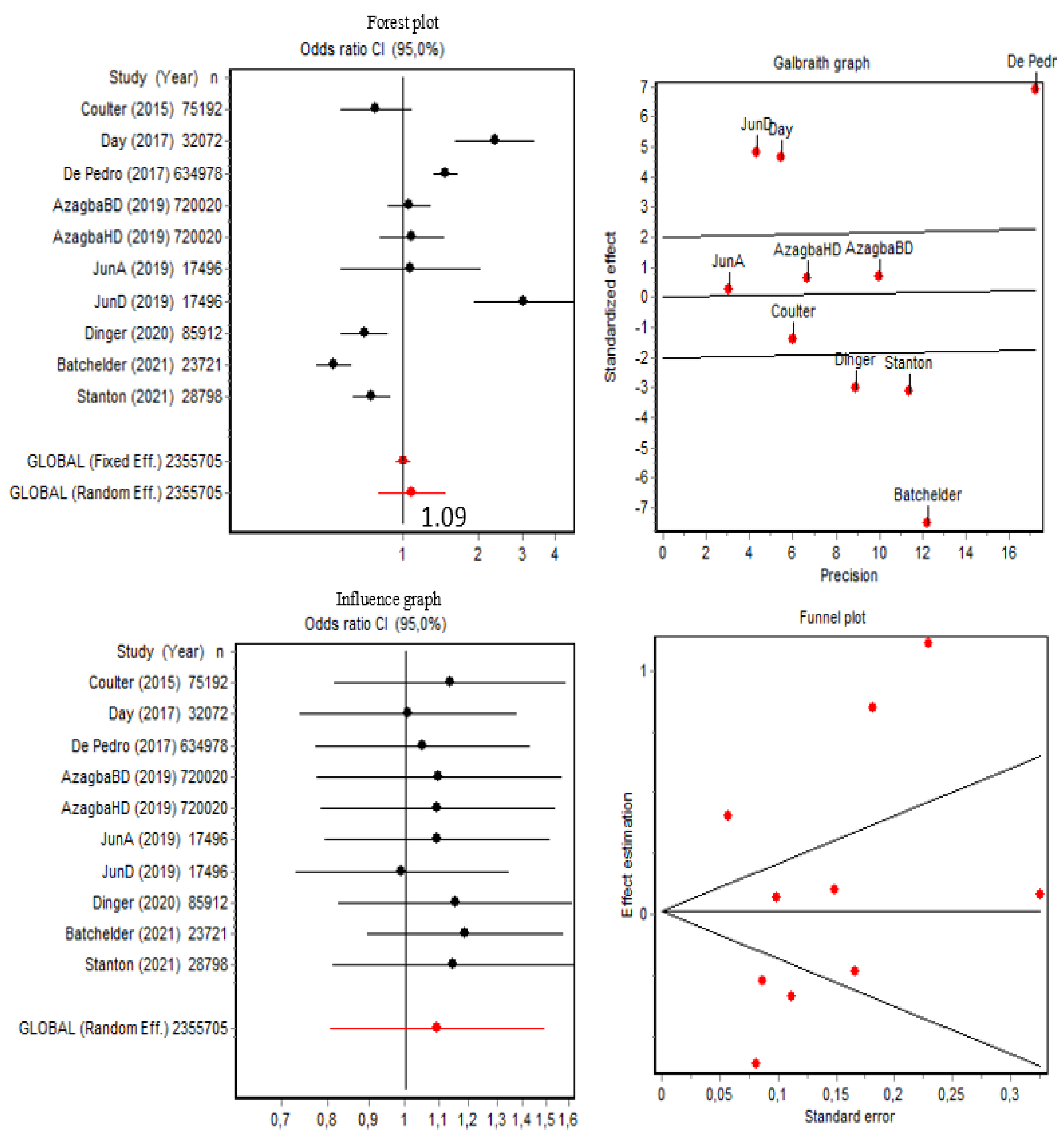
3.3. Current Alcohol Use and Alcohol Use Disorder
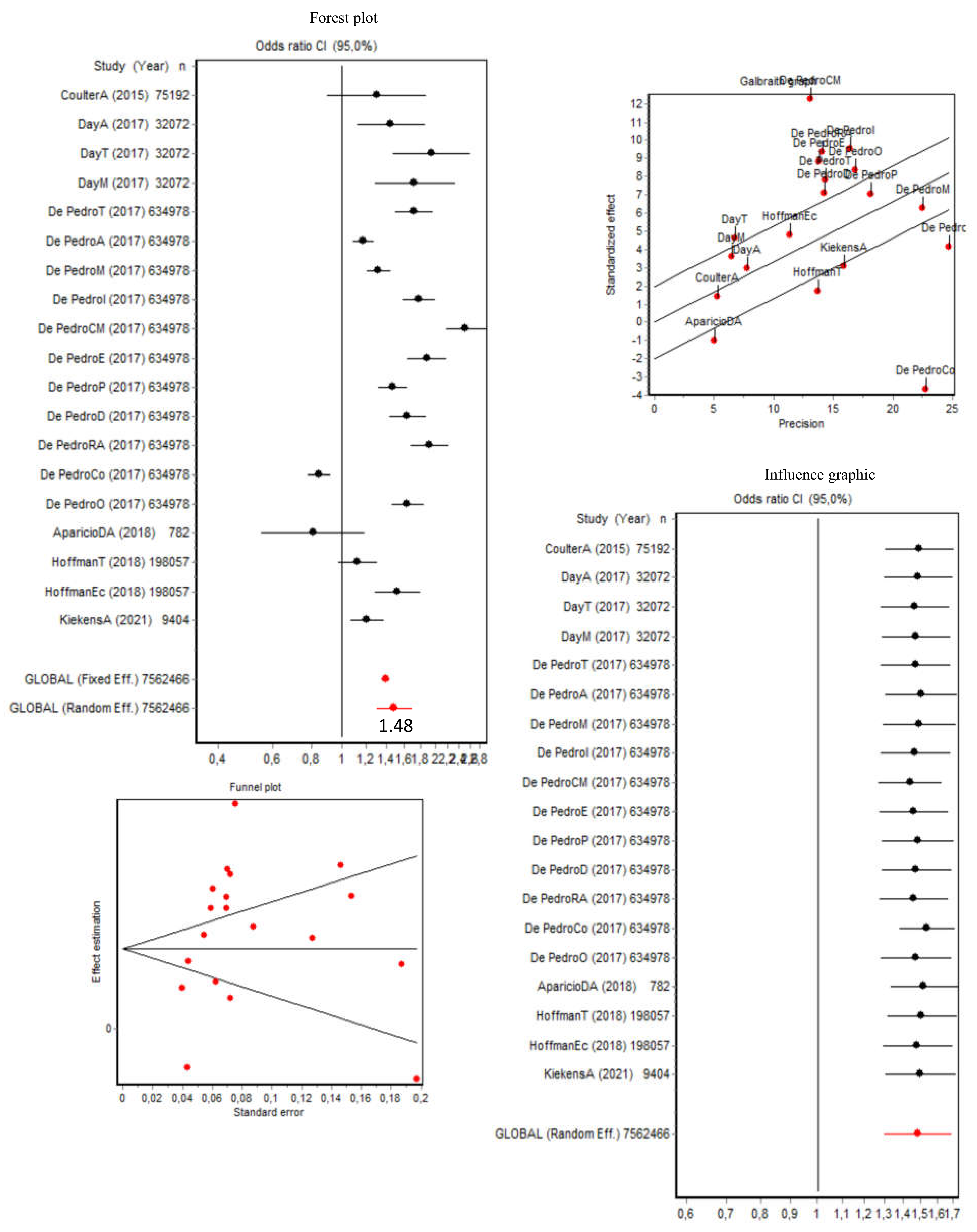
3.4. Lifetime Use of Substances (Including Tobacco, Alcohol, and Other Drugs)
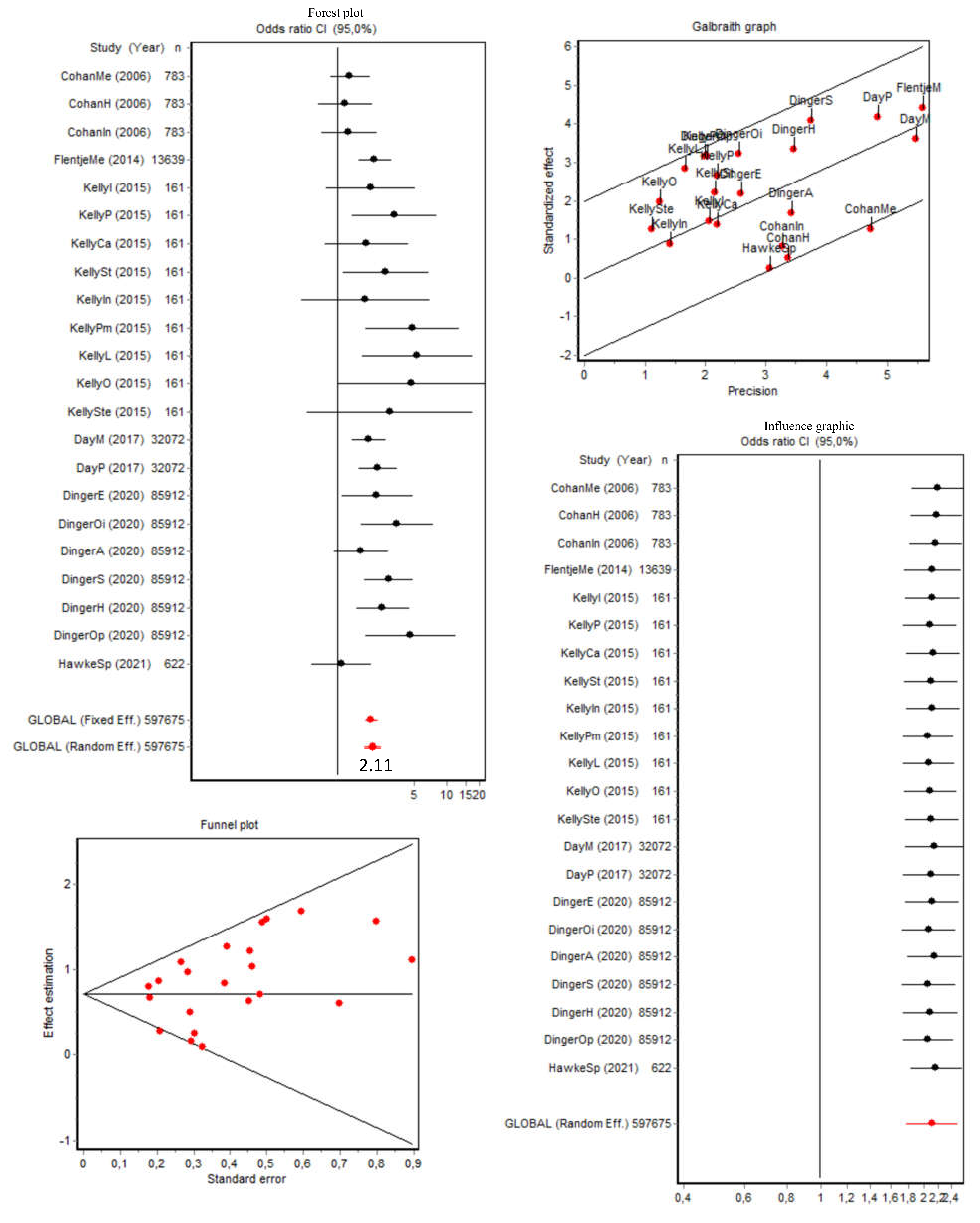
3.5. Current Substance (Excluding Tobacco and Alcohol) Use and Use Disorder
3.6. Summary of the Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coleman, E.; Bockting, W.; Botzer, M.; Cohen-Kettenis, P.; DeCuypere, G.; Feldman, J.; Fraser, L.; Green, J.; Knudson, G.; Meyer, W.J.; et al. The World Professional Association for Transgender Health. Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People. 7th ed, Version 7. Int. J. Transgenderism 2012, 13, 165–232. [Google Scholar] [CrossRef]
- Wålinder, J. Incidence and Sex Ratio of Transsexualism in Sweden. Br. J. Psychiatry. 1971, 119, 195–196. [Google Scholar] [CrossRef] [PubMed]
- Tsoi, W.F. The prevalence of transsexualism in Singapore. Acta Psychiatr. Scand. 1988, 78, 501–504. [Google Scholar] [CrossRef] [PubMed]
- Basterra, V.; Ruiz, R.; Toni, M.; Rebolé, A.; Pérez de Mendiola, Y.; Forga, L. Estudio descriptivo de la transexualidad en Navarra. An. Sist. Sanit. Navar. 2012, 35, 455–460. [Google Scholar] [CrossRef]
- Guzmán-Parra, J.; Sánchez-Álvarez, N.; de Diego-Otero, Y.; Pérez-Costillas, L.; Esteva de Antonio, I.; Navais-Barranco, M.; Castro-Zamudio, S.; Bergero-Miguel, T. Sociodemographic Characteristics and Psychological Adjustment among Transsexuals in Spain. Arch. Sex Behav. 2016, 45, 587–596. [Google Scholar] [CrossRef]
- Gómez Gil, E.; Trilla García, A.; Godás Sieso, T.; Halperin Rabinovich, I.; Puig Domingo, M.; Vidal Hagemeijer, A.; Peri Nogués, J.M. Estimación de la prevalencia, incidencia y razón de sexos del transexualismo en Cataluña según la demanda asistencial. Actas Esp. Psiquiatr. 2006, 34, 295–302. [Google Scholar]
- Peitzmeier, S.M.; Malik, M.; Kattari, S.K.; Marrow, E.; Stephenson, R.; Agénor, M.; Reisner, S.L. Intimate Partner Violence in Transgender Populations: Systematic Review and Meta-analysis of Prevalence and Correlates. Am. J. Public Health 2020, 110, E1–E14. [Google Scholar] [CrossRef]
- Yi, S.; Chann, N.; Chhoun, P.; Tuot, S.; Mun, P.; Brody, C. Social marginalization, gender-based violence, and binge drinking among transgender women in Cambodia. Drug Alcohol Depend. 2020, 207, 107802. [Google Scholar] [CrossRef]
- Chaney, M.P.; Brubaker, M.D. Addiction in LGBTQ Communities: Influences, Treatment, and Prevention. J. LGBT Issues Couns. 2012, 6, 234–236. [Google Scholar] [CrossRef]
- Burgess, D.; Lee, R.; Tran, A.; Van Ryn, M. Effects of perceived discrimination on mental health and mental health services utilization among gay, lesbian, bisexual and transgender persons. J. LGBT Health Res. 2007, 3, 1–14. [Google Scholar] [CrossRef]
- Rodman, K. Transgender People’s Experiences in Substance Abuse Treatment. Ph.D Thesis, California Institute of Integral Studies, San Francisco, CA, USA, 2015. [Google Scholar]
- Day, J.K.; Fish, J.N.; Perez-Brumer, A.; Hatzenbuehler, M.L.; Russell, S.T. Transgender Youth Substance Use Disparities: Results from a Population-Based Sample. J. Adolesc. Health. 2017, 61, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Coulter, R.W.S.; Bersamin, M.; Russell, S.T.; Mair, C. The Effects of Gender- and Sexuality-Based Harassment on Lesbian, Gay, Bisexual, and Transgender Substance Use Disparities. J. Adolesc. Health. 2018, 62, 688–700. [Google Scholar] [CrossRef] [PubMed]
- Stotzer, R.L.; Silverschanz, P.; Wilson, A. Gender identity and social services: Barriers to care. J. Soc. Serv. Res. 2013, 39, 63–77. [Google Scholar] [CrossRef]
- Lindley, L.; Bauerband, L.; Galupo, M.P. Using a Comprehensive Proximal Stress Model to Predict Alcohol Use. Transgend. Health 2021, 6, 164–174. [Google Scholar] [CrossRef]
- Cooper, M.L.; Frone, M.R.; Russell, M.; Mudar, P. Drinking to regulate positive and negative emotions: A motivational model of alcohol use. J. Pers. Soc. Psychol. 1995, 69, 990–1005. [Google Scholar] [CrossRef]
- Miller, L.R.; Grollman, E.A. The Social Costs of Gender Nonconformity for Transgender Adults: Implications for Discrimination and Health. Sociol. Forum 2015, 30, 809–831. [Google Scholar] [CrossRef]
- Reisner, S.L.; Pardo, S.T.; Gamarel, K.E.; Hughto, J.M.W.; Pardee, D.J.; Keo-Meier, C.L. Substance Use to Cope with Stigma in Healthcare among, U.S. Female-to-Male Trans Masculine Adults. LGBT Health 2015, 2, 324. [Google Scholar] [CrossRef] [Green Version]
- Tupler, L.A.; Zapp, D.; DeJong, W.; Ali, M.; O’Rourke, S.; Looney, J.; Swartzwelder, H.S. Alcohol-Related Blackouts, Negative Alcohol-Related Consequences, and Motivations for Drinking Reported by Newly Matriculating Transgender College Students. Alcohol Clin. Exp. Res. 2017, 41, 1012–1023. [Google Scholar] [CrossRef]
- Staples, J.M.; Neilson, E.C.; George, W.H.; Flaherty, B.P.; Davis, K.C. A descriptive analysis of alcohol behaviors across gender subgroups within a sample of transgender adults. Addict. Behav. 2018, 76, 355–362. [Google Scholar] [CrossRef]
- Cochran, B.N.; Peavy, K.M.; Santa, A.F. Differentiating LGBT individuals in substance abuse treatment: Analyses based on sexuality and drug preference. J. LGBT Health Res. 2007, 3, 63–75. [Google Scholar] [CrossRef]
- Peacock, E.; Andrinopoulos, K.; Hembling, J. Binge Drinking among Men Who Have Sex with Men and Transgender Women in San Salvador: Correlates and Sexual Health Implications. J. Urban. Health. 2015, 92, 701–716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connolly, D.; Gilchrist, G. Prevalence and correlates of substance use among transgender adults: A systematic review. Addict. Behav. 2020, 111, 106544. [Google Scholar] [CrossRef] [PubMed]
- Senreich, E. The Substance Abuse Treatment Experiences of a Small Sample of Transgender Clients. The Substance Abuse Treatment Experiences of a Small Sample of Transgender Clients. J. Soc. Work Pract. Addict. 2011, 11, 295–299. [Google Scholar] [CrossRef]
- Wolf, E.C.M.; Dew, B.J. Understanding risk factors contributing to substance use among MTF transgender persons. J. LGBT Issues Couns. 2012, 6, 237–256. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and metaanalyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Metaanalyses. 2019. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 28 December 2021).
- Aparicio-García, M.E.; Díaz-Ramiro Em Rubio-Valdehita, S.; López-Núñez, M.I.; García-Nieto, I. Health and Well-Being of Cisgender, Transgender and Non-Binary Young People. Int. J. Environ. Res. Public Health 2018, 15, 2133. [Google Scholar] [CrossRef] [Green Version]
- Azagba, S.; Latham, K.; Shan, L. Cigarette, smokeless tobacco, and alcohol use among transgender adults in the United States. Int. J. Drug Policy 2019, 73, 163–169. [Google Scholar] [CrossRef]
- Batchelder, A.W.; Stanton, A.M.; Kirakosian, N.; King, D.; Grasso, C.; Potter, J.; Mayer, K.H.; O’Cleirigh, C. Mental Health and Substance Use Diagnoses and Treatment Disparities by Sexual Orientation and Gender in a Community Health Center Sample. LGBT Health. 2021, 8, 290–299. [Google Scholar] [CrossRef]
- Buchting, F.O.; Emory, K.T.; Scout Kim, Y.; Fagan, P.; Vera, L.E.; Emery, S. Transgender Use of Cigarettes, Cigars, and E-Cigarettes in a National Study. Am. J. Prev. Med. 2017, 53, e1–e7. [Google Scholar] [CrossRef]
- Carone, N.; Rothblum, E.D.; Bos, H.M.W.; Gartrell, N.K.; Herman, J.L. Demographics and health outcomes in a U.S. probability sample of transgender parents. J. Fam. Psychol. 2021, 35, 57–68. [Google Scholar] [CrossRef]
- Cohan, D.; Lutnick, A.; Davidson, P.; Cloniger, C.; Herlyn, A.; Breyer, J.; Cobaugh, C.; Wilson, D.; Klausner, J. Sex worker health: San Francisco style. Sex. Transm. Infect. 2006, 82, 418–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coulter, R.W.; Blosnich, J.R.; Bukowski, L.A.; Herrick, A.L.; Siconolfi, D.E.; Stall, R.D. Differences in alcohol use and alcohol-related problems between transgender- and nontransgender-identified young adults. Drug Alcohol Depend. 2015, 154, 251–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Pedro, K.T.; Gilreath, T.D.; Jackson, C.; Esqueda, M.C. Substance Use Among Transgender Students in California Public Middle and High Schools. J. Sch. Health 2017, 87, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Dinger, M.K.; Brittain, D.R.; Patten, L.; Hall, K.C.; Burton, S.; Hydoc, D.S.; Stellino, M.B. Gender Identity and Health-related Outcomes in a National Sample of College Students. Am. J. Health Educ. 2020, 51, 383–394. [Google Scholar] [CrossRef]
- Flentje, A.; Heck, N.C.; Sorensen, J.L. Characteristics of transgender individuals entering substance abuse treatment. Addict. Behav. 2014, 39, 969–975. [Google Scholar] [CrossRef] [Green Version]
- Gamarel, K.E.; Watson, R.J.; Mouzoon, R.; Wheldon, C.W.; Fish, J.N.; Fleischer, N.L. Family Rejection and Cigarette Smoking Among Sexual and Gender Minority Adolescents in the USA. Int. J. Behav. Med. 2020, 27, 179–187. [Google Scholar] [CrossRef]
- Hawke, L.D.; Hayes, E.; Darnay, K.; Henderson, J. Mental health among transgender and gender diverse youth: An exploration of effects during the COVID-19 pandemic. Psychol. Sex. Orientat. Gend. Divers. 2021, 8, 180–187. [Google Scholar] [CrossRef]
- Hoffman, L.; Delahanty, J.; Johnson, S.E.; Zhao, X. Sexual and gender minority cigarette smoking disparities: An analysis of 2016 Behavioral Risk Factor Surveillance System data. Prev. Med. 2018, 113, 109–115. [Google Scholar] [CrossRef]
- Jun, H.J.; Webb-Morgan, M.; Felner, J.K.; Wisdom, J.P.; Haley, S.J.; Austin, S.B.; Corliss, H.L. Sexual orientation and gender identity disparities in substance use disorders during young adulthood in a United States longitudinal cohort. Drug Alcohol Depend. 2019, 205, 107619. [Google Scholar] [CrossRef]
- Kelly, J.; Davis, C.; Schlesinger, C. Substance use by same sex attracted young people: Prevalence, perceptions and homophobia. Drug Alcohol Rev. 2015, 34, 358–365. [Google Scholar] [CrossRef]
- Kiekens, W.J.; Baams, L.; Fish, J.N.; Watson, R.J. Associations of Relationship Experiences, Dating Violence, Sexual Harassment, and Assault With Alcohol Use Among Sexual and Gender Minority Adolescents. J. Interpers. Violence 2021, 1–29. [Google Scholar] [CrossRef] [PubMed]
- Stanton, A.M.; Batchelder, A.W.; Kirakosian, N.; Scholl, J.; King, D.; Grasso, C.; Potter, J.; Mayer, K.H.; O’Cleirigh, C. Differences in mental health symptom severity and care engagement among transgender and gender diverse individuals: Findings from a large community health center. PLoS ONE 2021, 16, e0245872. [Google Scholar] [CrossRef] [PubMed]
- Tamí-Maury, I.; Lin, M.T.; Lapham, H.L.; Hong, J.H.; Cage, C.; Shete, S.; Gritz, E.R. A pilot study to assess tobacco use among sexual minorities in Houston, Texas. Am. J. Addict. 2015, 24, 391–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradford, J.; Reisner, S.L.; Honnold, J.A.; Xavier, J. Experiences of Transgender-Related Discrimination and Implications for Health: Results from the Virginia Transgender Health Initiative Study. Am. J. Public Health 2013, 103, 1820. [Google Scholar] [CrossRef]
- Shires Deirdre, A.; Jaffee Kim, D. Structural Discrimination is Associated with Smoking Status among a National Sample of Transgender Individuals. Nicotine Tob. Res. 2016, 18, 1502–1508. [Google Scholar] [CrossRef]
- Gómez-Gil, E.; Trilla, A.; Salamero, M.; Godás, T.; Valdés, M. Sociodemographic, Clinical, and Psychiatric Characteristics of Transsexuals from Spain. Arch. Sex. Behav. 2009, 38, 378–392. [Google Scholar] [CrossRef]
- Gómez-Gil, E.; Simulionyte, E.; Balcells-Oliveró, M.; Valdés, M.; Salamero, M.; Guillamón, A.; Esteva, I. Patrones de consumo de alcohol, tabaco y drogas ilegales en personas transexuales. Adicciones 2018, 31, 189–195. [Google Scholar] [CrossRef] [Green Version]
- Wheldon, C.W.; Watson, R.J.; Fish, J.N.; Gamarel, K. Cigarette Smoking Among Youth at the Intersection of Sexual Orientation and Gender Identity. LGBT Heal. 2019, 6, 235–241. [Google Scholar] [CrossRef]
- Hughto, J.M.W.; Quinn, E.K.; Dunbar, M.S.; Rose, A.J.; Shireman, T.I.; Jasuja, G.K. Prevalence and Co-occurrence of Alcohol, Nicotine, and Other Substance Use Disorder Diagnoses Among US Transgender and Cisgender Adults. JAMA Netw. Open 2021, 4, e2036512. [Google Scholar] [CrossRef]
- Scheim, A.I.; Bauer, G.R.; Shokoohi, M. Drug use among transgender people in Ontario, Canada: Disparities and associations with social exclusion. Addict. Behav. 2017, 72, 151–158. [Google Scholar] [CrossRef]
- Benotsch, E.G.; Zimmerman, R.S.; Cathers, L.; Pierce, J.; McNulty, S.; Heck, T.; Perrin, P.B.; Snipes, D.J. Non-medical use of prescription drugs and HIV risk behaviour in transgender women in the Mid-Atlantic region of the United States. Int. J. STD AIDS 2016, 27, 776–782. [Google Scholar] [CrossRef] [PubMed]
- Kidd, J.D.; Goetz, T.G.; Shea, E.A.; Bockting, W.O. Prevalence and minority-stress correlates of past 12-month prescription drug misuse in a national sample of transgender and gender nonbinary adults: Results from the U.S. Transgender Survey. Drug Alcohol Depend. 2021, 219, 108474. [Google Scholar] [CrossRef] [PubMed]
- Johns, M.M.; Lowry, R.; Andrzejewski, J.; Barrios, L.C.; Demissie, Z.; McManus, T.; Rasberry, C.N.; Robin, L.; Underwood, J.M. Transgender Identity and Experiences of Violence Victimization, Substance Use, Suicide Risk, and Sexual Risk Behaviors Among High School Students—19 States and Large Urban School Districts, 2017. MMWR Morb. Mortal Wkly. Rep. 2019, 68, 67–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, G.M.; Rapues, J.; Wilson, E.C.; Macias, O.; Packer, T.; Colfax, G.; Raymond, H.F. Alcohol and substance use among transgender women in San Francisco: Prevalence and association with human immunodeficiency virus infection. Drug Alcohol Rev. 2014, 33, 287–295. [Google Scholar] [CrossRef]
- Frost, M.C.; Blosnich, J.R.; Lehavot, K.; Chen, J.A.; Rubinsky, A.D.; Glass, J.E.; Williams, E.C. Disparities in Documented Drug Use Disorders Between Transgender and Cisgender, U.S. Veterans Health Administration Patients. J. Addict. Med. 2021, 15, 334–340. [Google Scholar] [CrossRef]
- Gordon, A.R.; Meyer, I.H. Gender nonconformity as a target of prejudice, discrimination, and violence against LGB individuals. J. LGBT Health Res. 2007, 3, 55–71. [Google Scholar] [CrossRef]
- Reisner, S.L.; White, J.M.; Bradford, J.B.; Mimiaga, M.J. Transgender Health Disparities: Comparing Full Cohort and Nested Matched-Pair Study Designs in a Community Health Center. LGBT Health 2014, 1, 177. [Google Scholar] [CrossRef] [Green Version]
- Reisner, S.L.; Greytak, E.A.; Parsons, J.T.; Ybarra, M.L. Gender Minority Social Stress in Adolescence: Disparities in Adolescent Bullying and Substance Use by Gender Identity. J. Sex. Res. 2015, 52, 243. [Google Scholar] [CrossRef] [Green Version]
- Kosenko, K.; Rintamaki, L.; Raney, S.; Maness, K. Transgender patient perceptions of stigma in health care contexts. Med. Care. 2013, 51, 819–822. [Google Scholar] [CrossRef]
- Hendricks, M.L.; Testa, R.J. A conceptual framework for clinical work with transgender and gender nonconforming clients: An adaptation of the minority stress model. Prof. Psychol Res. Pract. 2012, 43, 460–467. [Google Scholar] [CrossRef]
- Johns, M.M.; Beltran, O.; Armstrong, H.L.; Jayne, P.E.; Barrios, L.C. Protective Factors Among Transgender and Gender Variant Youth: A Systematic Review by Socioecological Level. J. Prim. Prev. 2018, 39, 263–301. [Google Scholar] [CrossRef] [PubMed]
- Felner, J.K.; Wisdom, J.P.; Williams, T.; Katuska, L.; Haley, S.J.; Jun, H.J.; Corliss, H.L. Stress, Coping, and Context: Examining Substance Use Among LGBTQ Young Adults with Probable Substance Use Disorders. Psychiatr Serv. 2020, 71, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Wolford-Clevenger, C.; Flores, L.Y.; Bierma, S.; Cropsey, K.L.; Stuart, G.L. Minority stress and drug use among transgender and gender diverse adults: A daily diary study. Drug Alcohol Depend. 2021, 220, 108–508. [Google Scholar] [CrossRef] [PubMed]
- Katz-Wise, S.L.; Sarda, V.; Bryn Austin, S.; Harris, S.K. Longitudinal effects of gender minority stressors on substance use and related risk and protective factors among gender minority adolescents. PLoS ONE 2021, 16, e0250500. [Google Scholar] [CrossRef]
- Rowe, C.; Santos, G.M.; McFarland, W.; Wilson, E.C. Prevalence and correlates of substance use among trans female youth ages 16-24 years in the San Francisco Bay Area. Drug Alcohol Depend. 2015, 147, 160–166. [Google Scholar] [CrossRef] [Green Version]
- Nuttbrock, L.; Bockting, W.; Rosenblum, A.; Hwahng, S.; Mason, M.; Macri, M.; Becker, J. Gender abuse, depressive symptoms, and substance use among transgender women: A 3-year prospective study. Am. J. Public Health 2014, 104, 2199–2206. [Google Scholar] [CrossRef]
- Budhwani, H.; Hearld, K.R.; Milner, A.N.; McGlaughlin, E.; Charow, R.; Rodriguez-Lauzurique, R.M.; Rosario, S.; Paulino-Ramirez, R. Transgender Women’s Drug Use in the Dominican Republic. Transgender Heal. 2017, 2, 188–194. [Google Scholar] [CrossRef]
- Kcomt, L.; Evans-Polce, R.J.; Boyd, C.J.; McCabe, S.E. Association of transphobic discrimination and alcohol misuse among transgender adults: Results from the U.S. Transgender Survey. Drug Alcohol Depend. 2020, 215, 108223. [Google Scholar] [CrossRef]
- Mintz, S.; Ingram, K.M.; Milliken, A.; Kuehl, T.; Espelage, D.L. Longitudinal Associations Between Sexual Victimization and Substance Misuse Among High School Youth in Colorado. J. Interpers. Violence 2020, 1–24. [Google Scholar]
- Bouman, W.P.; Claes, L.; Brewin, N.; Crawford, J.R.; Millet, N.; Fernandez-Aranda, F.; Arcelus, J. Transgender and anxiety: A comparative study between transgender people and the general population. Int. J. Transgenderism 2017, 18, 16–26. [Google Scholar] [CrossRef]
- Witcomb, G.L.; Bouman, W.P.; Claes, L.; Brewin, N.; Crawford, J.R.; Arcelus, J. Levels of depression in transgender people and its predictors: Results of a large matched control study with transgender people accessing clinical services. J. Affect. Disord 2018, 235, 308–315. [Google Scholar] [CrossRef]
- Carrà, G.; Scioli, R.; Monti, M.C.; Marinoni, A. Severity profiles of substance-abusing patients in Italian community addiction facilities: Influence of psychiatric concurrent disorders. Eur. Addict. Res. 2006, 12, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Scheim, A.I.; Bauer, G.R.; Shokoohi, M. Heavy episodic drinking among transgender persons: Disparities and predictors. Drug Alcohol Depend. 2016, 167, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Sudhinaraset, M.; Wigglesworth, C.; Takeuchi, D.T. Social and Cultural Contexts of Alcohol Use: Influences in a Social-Ecological Framework. Alcohol Res. 2016, 38, 35–45. [Google Scholar] [PubMed]
- Substance Abuse and Mental Health Services Administration. Key Substance Use and Mental Health Indicators in the United States: Results from the 2019 National Survey on Drug Use and Health; HHS Publication No. PEP20-07-01-001, NSDUH Series H-55; Center for Behavioral Health Statistics and Quality; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2020. [Google Scholar]
- Connolly, D.; Davies, E.; Lynskey, M.; Barratt, M.J.; Maier, L.; Ferris, J.; Winstock, A.; Gilchristet, G. Comparing intentions to reduce substance use and willingness to seek help among transgender and cisgender participants from the Global Drug Survey. J. Subst. Abuse Treat. 2020, 112, 86–91. [Google Scholar] [CrossRef]
- Matsuzaka, S. Transgressing gender norms in addiction treatment: Transgender rights to access within gender-segregated facilities. J. Ethn. Subst. Abuse 2018, 17, 420–433. [Google Scholar] [CrossRef]
- Lombardi, E. Substance use treatment experiences of transgender/transsexual men and women. J. LGBT Health Res. 2007, 3, 37–47. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1st Author Year | Country | Population | Age in Years | Sample Size | Substance and Use | NOS Quality |
|---|---|---|---|---|---|---|
| Aparicio-García 2018 | Spain | Contacts of LGBT + associations | 14–25 | 782 | Drugs and alcohol LU, Tobacco CU, Alcohol CU, Drugs CU | 7 |
| Azagba 2019 | USA | General population | >18 | 720,020 | Tobacco CU, UD; Smokeless tobacco CU, UD; Alcohol UD (heavy and binge drinking) | 8 |
| Batchelder 2021 | USA | Community health centre | Mean 31.5 | 23,721 | Alcohol UD, Substance UD | 5 |
| Buchting 2016 | USA | General population | >18 | 17,164 | Tobacco CU | 8 |
| Carone 2020 | USA | General population | >18 | 1436 | Alcohol CU, Drugs CU | 8 |
| Cohan 2006 | USA | Sex workers | 17–76 | 783 | Tobacco CU, Illicit drug CU, Methamphetamines CU, Heroin CU, Cocaine/crack CU, Injection drugs CU | 8 |
| Coulter 2015 | USA | Postsecondary students | 18–29 | 75,192 | Alcohol LU, Alcohol CU, Alcohol UD (heavy drinking) | 8 |
| Day 2017 | USA | Middle and high school students | 10–18 | 32,072 | Alcohol LU, UD (heavy drinking); Tobacco LU, CU; Marijuana LU, CU; Other drugs CU; Polysubstance CU | 8 |
| De Pedro 2017 | USA | Middle and high school students | Not reported | 634,978 | Tobacco LU, CU; Alcohol LU, CU, UD; Marijuana LU, CU; Inhalants LU, CU; Cocaine/Methamphetamine LU; Ecstasy LU; Prescription painkillers LU, CU; Diet pills LU; Ritalin or Adderall LU; Cold Medicine LU; Other drugs LU, CU; 2 or more drugs CU | 8 |
| Dinger 2020 | USA | College and university students | 18–25 | 85,912 | Cigarettes CU; E-cigarettes CU; Alcohol CU, UD (binge drinking); Marijuana CU; Amphetamine CU; Sedative CU; Hallucinogens CU; Opiate CU; Inhalant CU; MDMA (Ecstasy) CU; Other club drugs CU; Other illegal drugs CU | 8 |
| Flentje 2014 | USA | Abuse treatment services clients | Mean 38.31 | 13,639 | Alcohol CU, Cocaine CU, Heroin CU, Methamphetamine CU, Marijuana CU, Other drugs CU | 8 |
| Gamarel 2020 | USA | Sexual and gender minorities | 13–17 | 8243 | Tobacco CU | 7 |
| Hawke 2021 | Canada | Clinical and nonclinical | 14–28 | 622 | Substance CU (pre-COVID and intra-COVID) | 6 |
| Hoffman 2018 | USA | Noninstitutionalised population | >18 | 198,057 | Cigarettes LU, CU; E-cigarettes LU; CU; Nicotine UD (dependence) | 8 |
| Jun 2019 | USA | General population | 20–35 | 253,033 | Nicotine UD (dependence), Alcohol UD (abuse and dependence), Drug UD (abuse and dependence) | 8 |
| Kelly 2015 | Australia | LGBT festival goers | 13–24 | 161 | Alcohol CU, Tobacco CU, Any illicit drug CU, Poly-drug CU, Cannabis CU, Stimulants CU, Inhalants CU, Prescription medications CU, LSD CU, Opiates CU, Steroids CU | 5 |
| Kiekens 2021 | USA | Sexual and gender minorities | 13–17 | 9404 | Alcohol CU, Alcohol LU | 7 |
| Stanton 2021 | USA | Community health centre specialising in sexual and gender minorities | >18 | 28,798 | Alcohol UD, Substance UD | 6 |
| Tamí-Maury 2015 | USA | LGBT individuals participating in the Pride Parade and Festival | Mean 30 | 94 | Tobacco CU | 5 |
| Tupler 2017 | USA | College students | >17 | 272,840 | Alcohol CU | 7 |
| DATA | N1 | OR1 | 95% IC1 | N2 | OR2 | 95% IC2 |
|---|---|---|---|---|---|---|
| Current tobacco use | 14 | 1.65 * | 1.37, 1.98 | 9 | 1.58 * | 1.44, 1.73 |
| Current tobacco use disorder | 3 | 1.52 | 0.94, 2.45 | 2 | 1.29 | 0.79, 2.11 |
| Current alcohol use | 9 | 0.97 | 0.83, 1.14 | 6 | 1.03 | 0.93, 1.15 |
| Current alcohol use disorder | 10 | 1.09 | 0.80, 1.49 | 4 | 1.01 | 0.69, 1.28 |
| Lifetime substance (all) use | 19 | 1.48 * | 1.30, 1.68 | 7 | 1.38 * | 1.28, 1.49 |
| Current substance use (excluding tobacco and alcohol) | 5 | 1.12 | 0.58, 2.15 | 3 | 0.98 | 0.70, 1.37 |
| Current use of specific substances (excluding tobacco and alcohol) | 40 | 1.79 * | 1.54, 2.59 | 22 | 2.11 * | 1.77, 2.51 |
| Current substance use disorder (excluding tobacco and alcohol) | 4 | 1.53 | 0.91, 2.59 | 3 | 1.06 | 0.80, 1.40 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cotaina, M.; Peraire, M.; Boscá, M.; Echeverria, I.; Benito, A.; Haro, G. Substance Use in the Transgender Population: A Meta-Analysis. Brain Sci. 2022, 12, 366. https://doi.org/10.3390/brainsci12030366
Cotaina M, Peraire M, Boscá M, Echeverria I, Benito A, Haro G. Substance Use in the Transgender Population: A Meta-Analysis. Brain Sciences. 2022; 12(3):366. https://doi.org/10.3390/brainsci12030366
Chicago/Turabian StyleCotaina, Miriam, Marc Peraire, Mireia Boscá, Iván Echeverria, Ana Benito, and Gonzalo Haro. 2022. "Substance Use in the Transgender Population: A Meta-Analysis" Brain Sciences 12, no. 3: 366. https://doi.org/10.3390/brainsci12030366