
Orofacial Muscle Strength across the Dysarthrias

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Clinical Motor Speech Assessment
2.3. Orofacial Strength Measures
2.4. Data Analysis
3. Results
3.1. Missing Data
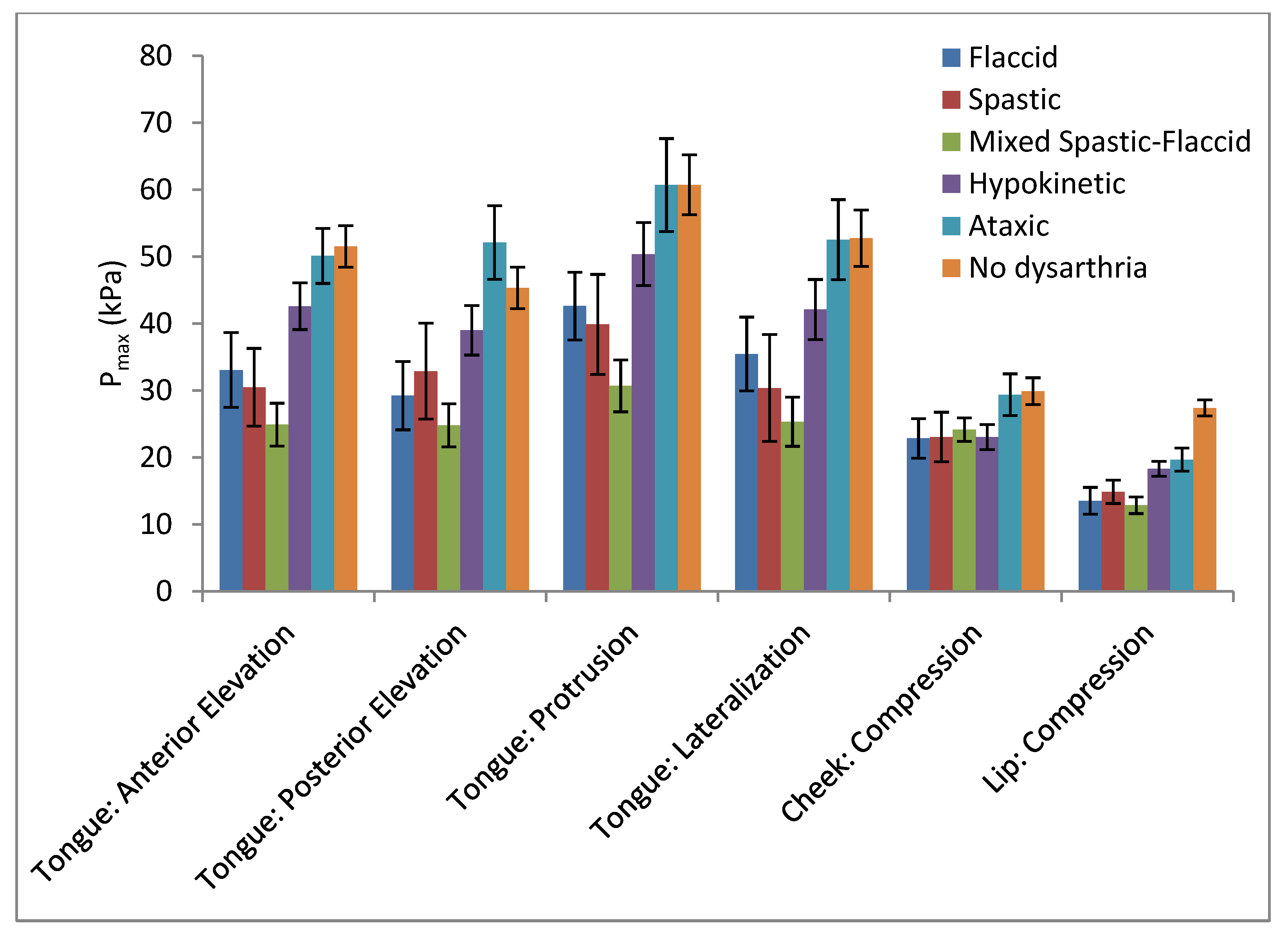
3.2. Group and Task Comparisons
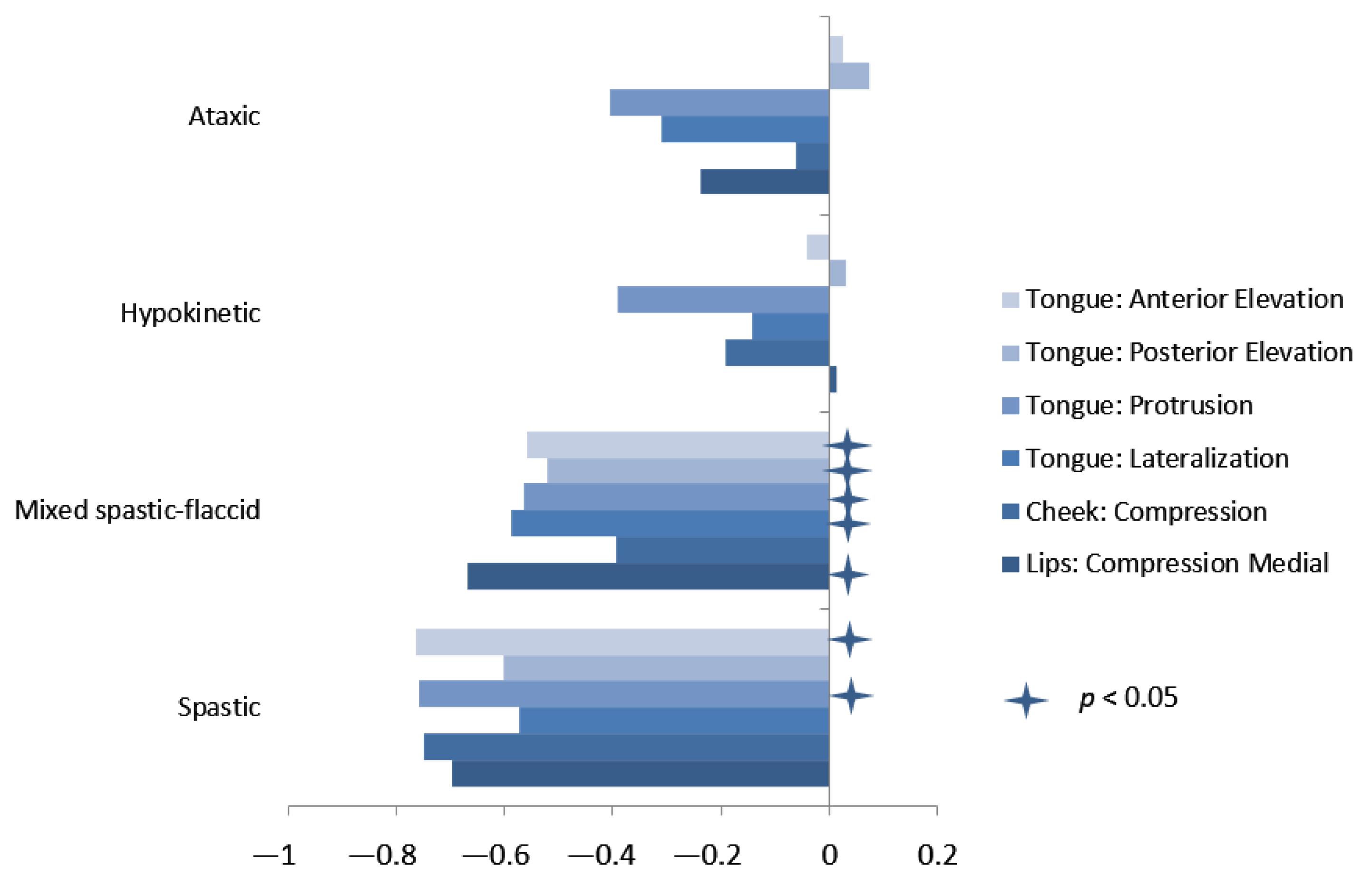
3.3. Relationship of Orofacial Strength to Dysarthria Severity
4. Discussion
4.1. Orofacial Strength in Speakers with and without Dysarthria
4.2. Orofacial Strength across Dysarthria Types
4.3. Relationship of Severity of Weakness to Severity of Dysarthria
4.4. Study Limitations
4.5. Clinical Implications
4.6. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Disclaimers
References
- Darley, F.L.; Aronson, A.E.; Brown, J.R. Clusters of Deviant Speech Dimensions in the Dysarthrias. J. Speech Hear. Res. 1969, 12, 462–496. [Google Scholar] [CrossRef] [PubMed]
- Duffy, J.R. Motor Speech Disorders: Substrates, Differential Diagnosis, and Management, 4th ed.; Elsevier: St. Louis, MO, USA, 2020. [Google Scholar]
- Kent, R.D.; Kent, J.F.; Duffy, J.; Weismer, G. The dysarthrias: Speech-voice profiles, related dysfunctions, and neuropathology. J. Med. Speech-Lang. Pathol. 1998, 6, 165–211. [Google Scholar]
- Peacher, W.G. The etiology and differential diagnosis of dysarthria. J Speech Hear. Disord. 1950, 15, 252–265. [Google Scholar] [CrossRef] [PubMed]
- De Paul, R.; Brooks, B.R. Multiple orofacial indices in amyotrophic lateral sclerosis. J. Speech Hear. Res. 1993, 36, 1158–1167. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, J.P.; Aronson, A.E.; Mulder, D.W. Tongue force in normals and in dysarthric patients with amyotrophic lateral sclerosis. J. Speech Hear. Res. 1980, 23, 828–837. [Google Scholar] [CrossRef]
- Dworkin, J.P.; Aronson, A.E. Tongue strength and alternate motion rates in normal and dysarthric subjects. J. Commun. Disord. 1986, 19, 115–132. [Google Scholar] [CrossRef]
- Solomon, N.P.; Lorell, D.M.; Robin, D.A.; Rodnitzky, R.L.; Luschei, E.S. Tongue strength and endurance in mild to moderate Parkinson’s disease. J. Med. Speech-Lang. Pathol. 1995, 3, 15–26. [Google Scholar]
- Solomon, N.P.; Robin, D.A.; Luschei, E.S. Strength, endurance, and stability of the tongue and hand in Parkinson disease. J. Speech Lang. Hear. Res. 2000, 43, 256–267. [Google Scholar] [CrossRef]
- Thompson, E.C.; Murdoch, B.E.; Stokes, P.D. Tongue function in subjects with upper motor neuron type dysarthria following cerebrovascular accident. J. Med. Speech-Lang. Pathol. 1995, 3, 27–40. [Google Scholar]
- Thompson, E.C.; Stokes, P.D.; Murdoch, B.E. Lip function in subjects with upper motor neuron type dysarthria following cerebrovascular accidents. Eur. J. Disord. Commun. 1995, 30, 451–466. [Google Scholar] [CrossRef]
- Neel, A.T.; Palmer, P.M.; Sprouls, G.; Morrison, L. Muscle weakness and speech in oculopharyngeal muscular dystrophy. J. Speech Lang. Hear. Res. 2015, 58, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mul, K.; Berggren, K.N.; Sills, M.Y.; McCalley, A.; van Engelen, B.G.; Johnson, N.E.; Statland, J.M. Effects of weakness of orofacial muscles on swallowing and communication in FSHD. Neurology 2019, 92, e957–e963. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.M.; Hughes, J.; Hayes, K.C.; Wolfe, D.L. Reliability of labial closure force measurements in normal subjects and patients with CNS disorders. J. Speech Hear. Res. 1992, 35, 252–258. [Google Scholar] [CrossRef]
- Langmore, S.; Lehman, M.E. Physiologic deficits in the orofacial system underlying dysarthria in amyotrophic lateral sclerosis. J. Speech Hear. Res. 1994, 37, 28–37. [Google Scholar] [CrossRef]
- Jones, H.N.; Ma, K.D.C.; Asrani, P.; Sloane, R.; Kishnani, P.S. Quantitative assessment of lingual strength in late-onset Pompe disease. Muscle Nerve 2015, 51, 731–735. [Google Scholar] [CrossRef] [PubMed]
- O’Day, C.; Frank, E.; Montgomery, A.; Nichols, M.; McDade, H. Repeated tongue and hand strength measurements in normal adults and individuals with Parkinson’s disease. Int. J. Orofac. Myol. Myofunctional Ther. 2005, 31, 15–25. [Google Scholar] [CrossRef]
- De Paul, R.; Abbs, J.H.; Caligiuri, M.; Gracco, V.L.; Brooks, B.R. Hypoglossal, trigeminal, and facial motoneuron involvement in amyotrophic lateral sclerosis. Neurology 1988, 38, 281–283. [Google Scholar] [CrossRef]
- Hartelius, L.; Lillvik, M. Lip and tongue function differently affected in individuals with multiple sclerosis. Folia Phoniatr Logop 2003, 55, 1–9. [Google Scholar] [CrossRef]
- Weeks, K.; Dzielak, D.; Hamadain, E.; Bailey, J. Examining the relationship between stroke and labial strength. Contemp. Issues Commun. Sci. Disord. 2013, 40, 160–169. [Google Scholar] [CrossRef]
- Searl, J.; Knollhoff, S.; Barohn, R.J. Lingual-Alveolar Contact Pressure During Speech in Amyotrophic Lateral Sclerosis: Preliminary Findings. J. Speech Lang. Hear. Res. 2017, 60, 810–825. [Google Scholar] [CrossRef] [Green Version]
- Solomon, N.P.; Makashay, M.J.; Helou, L.B.; Clark, H.M. Neurogenic Orofacial Weakness and Speech in Adults With Dysarthria. Am. J. Speech Lang. Pathol. 2017, 26, 951–960. [Google Scholar] [CrossRef] [PubMed]
- Jones, H.N.; Hobson-Webb, L.D.; Kuchibhatla, M.; Crisp, K.D.; Whyte-Rayson, A.; Batten, M.T.; Zwelling, P.J.; Kishnani, P.S. Tongue weakness and atrophy differentiates late-onset Pompe disease from other forms of acquired/hereditary myopathy. Mol. Genet. Metab. 2021, 133, 261–268. [Google Scholar] [CrossRef]
- Neel, A.T.; Boyd, E.C.; Corral, M.E.; Sanchez, D.L. Randomized variable practice appears to be effective in the acquisition and generalization of speech sounds in childhood apraxia of speech. Evid.-Based Commun. Assess. Interv. 2015, 9, 57–60. [Google Scholar] [CrossRef]
- Adams, V.; Mathisen, B.; Baines, S.; Lazarus, C.; Callister, R. A systematic review and meta-analysis of measurements of tongue and hand strength and endurance using the Iowa Oral Performance Instrument (IOPI). Dysphagia 2013, 28, 350–369. [Google Scholar] [CrossRef]
- Darley, F.L.; Aronson, A.E.; Brown, J.R. Differential diagnostic patterns of dysarthria. J. Speech Hear. Res. 1969, 12, 246–269. [Google Scholar] [CrossRef] [PubMed]
- ClarkNancy, H.M.; Solomon, N.P. Age and sex differences in orofacial strength. Dysphagia 2012, 27, 2–9. [Google Scholar] [CrossRef] [Green Version]
- Dietsch, A.M.; Solomon, N.P.; Sharkey, L.A.; Duffy, J.R.; Strand, E.A.; Clark, H.M. Perceptual and instrumental assessments of orofacial muscle tone in dysarthric and normal speakers. J. Rehabil. Res. Dev. 2014, 51, 1127–1142. [Google Scholar] [CrossRef]
- Solomon, N.P.; Clark, H.M. The effect of an anti-slip surface on objective measures of tongue strength in healthy adults. Int. J. Orofac. Myol. Myofunctional Ther. 2020, 46, 13–21. [Google Scholar] [CrossRef]
- Clark, H.M.; Duffy, J.R.; Whitwell, J.L.; Ahlskog, J.E.; Sorenson, E.J.; Josephs, K.A. Clinical and imaging characterization of progressive spastic dysarthria. Eur. J. Neurol. 2014, 21, 368–376. [Google Scholar] [CrossRef] [Green Version]
- Mulligan, M.; Carpenter, J.; Riddel, J.; Delaney, M.K.; Badger, G.; Krusinski, P.; Tandan, R. Intelligibility and the acoustic characteristics of speech in amyotrophic lateral sclerosis (ALS). J. Speech Hear. Res. 1994, 37, 496–503. [Google Scholar] [CrossRef]
- Ramig, L.O.; Gould, W.J. Speech characteristics in Parkinson’s Disease. Neuorologic Consult. 1986, 4, 1–8. [Google Scholar]
- Spencer, K.A.; France, A.A. Perceptual ratings of subgroups of ataxic dysarthria. Int. J. Lang. Commun. Disord. 2016, 51, 430–441. [Google Scholar] [CrossRef]
- Clark, H.M.; O’Brien, K.; Calleja, A.; Corrie, S.N. Effects of directional exercise on lingual strength. J. Speech Lang. Hear. Res. 2009, 52, 1034–1047. [Google Scholar] [CrossRef]
- Robin, D.A.; Somodi, L.B.; Luschei, E.S. Measurement of tongue strength and endurance in normal and articulation disordered subjects. In Dysarthria and Apraxia of Speech: Perspectives on Management; Moore, C., Yorkston, K., Beukelman, D., Eds.; Paul H. Brooks Publishers: Baltimore, MD, USA, 1991. [Google Scholar]
- Hedges, L.V. Distribution theory for Glass’s estimator of effect size and related estimators. J. Educ. Stat. 1981, 6, 107–128. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Theodoros, D.G.; Murdoch, B.E.; Stokes, P. A physiological analysis of articulatory dysfunction in dysarthric speakers following severe closed-head injury. Brain Inj. 1995, 9, 237–254. [Google Scholar] [CrossRef] [PubMed]
- Pitts, L.L.; Cox, A.; Morales, S.; Tiffany, H. A Systematic Review and Meta-analysis of Iowa Oral Performance Instrument Measures in Persons with Parkinson’s Disease Compared to Healthy Adults. Dysphagia 2022, 37, 99–115. [Google Scholar] [CrossRef] [PubMed]
- Chu, S.Y.; Barlow, S.M.; Lee, J. Face-referenced measurement of perioral stiffness and speech kinematics in Parkinson’s disease. J. Speech Lang. Hear. Res. 2015, 58, 201–212. [Google Scholar] [CrossRef] [Green Version]
- Cano-De-La-Cuerda, R.; Pérez-De-Heredia, M.; Miangolarra-Page, J.C.; Muñoz-Hellín, E.; Fernández-De-Las-Peñas, C. Is there muscular weakness in Parkinson’s disease? Am. J. Phys. Med. Rehabil. 2010, 89, 70–76. [Google Scholar] [CrossRef]
- Gilman, S. A mechanism underlying cerebellar hypotonia. Trans. Am. Neurol. Assoc. 1968, 93, 213–215. [Google Scholar]
- Corfield, D.R.; Murphy, K.; Josephs, O.; Fink, G.R.; Frackowiak, R.S.J.; Guz, A.; Adams, L.; Turner, R. Cortical and subcortical control of tongue movement in humans: A functional neuroimaging study using fMRI. J. Appl. Physiol. 1999, 86, 1468–1477. [Google Scholar] [CrossRef]
- Rödel, R.M.W.; Laskawi, R.; Markus, H. Tongue representation in the lateral cortical motor region of the human brain as assessed by transcranial magnetic stimulation. Ann. Otol. Rhinol. Laryngol. 2003, 112, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, R.J.; Napadow, V.; Gaige, T.A.; Wedeen, V.J. Anatomical basis of lingual hydrostatic deformation. J. Exp. Biol. 2007, 210 Pt 23, 4069–4082. [Google Scholar] [CrossRef] [Green Version]
- Kier, W.M.; Smith, K.K. Tongues, Tentacles and Trunks—The Biomechanics of Movement in Muscular-Hydrostats. Zool. J. Linn. Soc. 1985, 83, 307–324. [Google Scholar] [CrossRef]
- Robin, D.A.; Goel, A.; Somodi, L.B.; Luschei, E.S. Tongue strength and endurance: Relation to highly skilled movements. J. Speech Hear. Res. 1992, 35, 1239–1245. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, J.P. Tongue strength measurement in patients with amyotrophic lateral sclerosis: Qualitative vs. quantitative procedures. Arch. Phys. Med. Rehabil. 1980, 61, 422–424. [Google Scholar]
- Clark, H.M.; Duffy, J.; Strand, E.; Whitwell, J.L.; Josephs, K. Motor Speech Disorders Accompanying RS and SL Variants of Progressive Supanuclear Palsy. Stem- Spraak- Taalpathologie 2017, 22, 100. [Google Scholar]
- Utianski, R.L.; Duffy, J.R.; Clark, H.M.; Strand, E.A.; Botha, H.; Schwarz, C.G.; Machulda, M.M.; Senjem, M.L.; Spychalla, A.J.; Jack, C.R.; et al. Prosodic and phonetic subtypes of primary progressive apraxia of speech. Brain Lang. 2018, 184, 54–65. [Google Scholar] [CrossRef]
- Barkmeier-Kraemer, J.M.; Clark, H.M. Speech-Language Pathology Evaluation and Management of Hyperkinetic Disorders Affecting Speech and Swallowing Function. Tremor Other Hyperkinet Mov. 2017, 7, 489. [Google Scholar] [CrossRef]
- Adams, V.; Mathisen, B.; Baines, S.; Lazarus, C.; Callister, R. Reliability of Measurements of Tongue and Hand Strength and Endurance Using the Iowa Oral Performance Instrument with Healthy Adults. Dysphagia 2013, 29, 83–95. [Google Scholar] [CrossRef]
- Rong, P.; Green, J.R. Predicting Speech Intelligibility Based on Spatial Tongue-Jaw Coupling in Persons with Amyotrophic Lateral Sclerosis: The Impact of Tongue Weakness and Jaw Adaptation. J. Speech Lang. Hear. Res. 2019, 62, 3085–3103. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dysarthria Type | N | Sex (F:M) | Mean Age (SD) | Medical Diagnoses (N) | Mean Time Post-Onset (Months) |
|---|---|---|---|---|---|
| Flaccid | 13 | 5:8 | 64.4 (22.8) | ALS (6) Myasthenia gravis (1) Myopathy (1) Congenital neuromuscular disorder (2) Neoplasm (3) | 27.2 |
| Spastic | 8 | 4:4 | 64.9 (8.23) | ALS (6) Multiple sclerosis (1) Parkinson plus (1) | 25.0 |
| Mixed Spastic–flaccid | 26 | 13:13 | 56.7 (12.4) | ALS (26) | 38.9 |
| Hypokinetic | 19 | 2:17 | 64.3 (9.8) | Parkinson disease (14) Parkinson plus (2) Stroke (1) Unknown (2) | 38.4 |
| Ataxic | 13 | 5:8 | 54.07 (13.6) | Cerebellar disease (8) Parkinson plus (2) Multiple sclerosis (1) Other/Unknown (2) | 29.6 |
| Combined Groups | 79 | 29:50 | 58.8 (14.3) Range 18–83 | 37.3 | |
| Healthy Controls | 33 | 2:31 | 59.8 (19.8) Range 25–89 | n/a |
| Dysarthria Type | Features | |
|---|---|---|
| Flaccid | Normal or slow rate Hypernasality Breathiness | Short phrases Articulatory imprecision |
| Spastic | Slow rate Strained vocal quality Monopitch | Monoloudness Articulatory imprecision Slow and regular AMRs |
| Mixed Spastic–Flaccid | Slow rate Strained vocal quality Vocal flutter Monopitch | Monoloudness Hypernasality Articulatory imprecision Slow and regular AMRs |
| Hypokinetic | Rapid rate and/or short rushes of speech Reduced loudness Monopitch | Monoloudness Articulatory imprecision Rapid and blurred AMRs |
| Ataxic | Slow or normal rate Excess and equal stress Irregular articulatory breakdowns | Telescoping of syllables Irregular AMRs |
| Flaccid | Spastic | Mixed Spastic–Flaccid | Hypokinetic | Ataxic | Controls (No Dysarthria) | |
|---|---|---|---|---|---|---|
| Tongue: Anterior Elevation | ||||||
| # of Missing Data Points | ||||||
| Mean | 33.1 B | 30.5 B | 24.9 B,C | 42.6 | 50.1 A,B | 51.5 A |
| Standard Deviation | (20.3) | (16.4) | (16.4) | (15.4) | (14.7) | (17.6) |
| Hedges’ g | 1.0 | 1.2 | 1.55 | 0.53 | 0.08 | |
| Tongue: Posterior Elevation | ||||||
| # of Missing Data Points | 1 | 1 | 1 | 1 | ||
| Mean | 29.2 | 32.9 | 24.8 B | 39.0 | 52.1 A | 45.3 A |
| Standard Deviation | (18.5) | (19.0) | (15.7) | (16.1) | (19.3) | (18.0) |
| Hedges’ g | 0.89 | 0.69 | 1.21 | 0.36 | 0.4 | |
| Tongue: Protrusion | ||||||
| # of Missing Data Points | 1 | 1 | ||||
| Mean | 42.6 | 39.9 | 30.7 B | 50.4 | 60.7 A | 60.7 A |
| Standard Deviation | (18.2) | (21.2) | (19.3) | (20.1) | (25.1) | (25.7) |
| Hedges’ g | 0.76 | 0.84 | 1.30 | 0.43 | 0.00 | |
| Tongue: Lateralization | ||||||
| # of Missing Data Points | 2 | |||||
| Mean | 35.5 | 30.4 | 25.3 B | 42.1 | 52.5 A | 52.8 A |
| Standard Deviation | (19.9) | (22.6) | (18.7) | (19.6) | (21.6) | (23.4) |
| Hedges’ g | 0.77 | 0.96 | 1.04 | 0.48 | 0.01 | |
| Cheek: Compression | ||||||
| # of Missing Data Points | 2 | 2 | 2 | |||
| Mean | 22.8 | 23.1 | 24.2 | 23.0 | 29.4 | 29.9 |
| Standard Deviation | (10.7) | (10.4) | (8.7) | (7.9) | (11.2) | (11.3) |
| Hedges’ g | 0.63 | 0.62 | 0.56 | 0.67 | 0.04 | |
| Lip: Compression | ||||||
| # of Missing Data Points | 1 | |||||
| Mean | 13.5 B | 14.8 B | 12.8 B | 18.3 B | 19.7 A,B | 27.4 A |
| Standard Deviation | (7.2) | (4.9) | (6.3) | (4.9) | (6.0) | (6.9) |
| Hedges’ g | 1.98 | 1.89 | 2.19 | 1.45 | 1.15 |
| Tongue: Anterior Elevation | Tongue: Posterior Elevation | Tongue: Protrusion | Tongue: Lateralization | Cheek: Compression | Lips: Compression | |
|---|---|---|---|---|---|---|
| Tongue: Anterior Elevation | 0.9042 | 0.7844 | 0.8448 | 0.5702 | 0.4805 | |
| Tongue: Posterior Elevation | 0.8058 | 0.8626 | 0.5535 | 0.4004 | ||
| Tongue: Protrusion | 0.8874 | 0.6244 | 0.4964 | |||
| Tongue: Lateralization | 0.5573 | 0.4964 | ||||
| Cheek: Compression | 0.5288 | |||||
| Dysarthria Severity | −0.3238 | −0.2708 | −0.4474 | −0.3900 | −0.2458 | −0.3321 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clark, H.M.; Duffy, J.R.; Strand, E.A.; Hanley, H.; Solomon, N.P. Orofacial Muscle Strength across the Dysarthrias. Brain Sci. 2022, 12, 365. https://doi.org/10.3390/brainsci12030365
Clark HM, Duffy JR, Strand EA, Hanley H, Solomon NP. Orofacial Muscle Strength across the Dysarthrias. Brain Sciences. 2022; 12(3):365. https://doi.org/10.3390/brainsci12030365
Chicago/Turabian StyleClark, Heather M., Joseph R. Duffy, Edythe A. Strand, Holly Hanley, and Nancy Pearl Solomon. 2022. "Orofacial Muscle Strength across the Dysarthrias" Brain Sciences 12, no. 3: 365. https://doi.org/10.3390/brainsci12030365