
Switching and Combining Device-Aided Therapies in Advanced Parkinson’s Disease: A Double Centre Retrospective Study

 , and
, and
Abstract
:1. Introduction
2. Methods
3. Results
3.1. Reasons for Switching between DATs
3.2. Reasons for Combining DATs
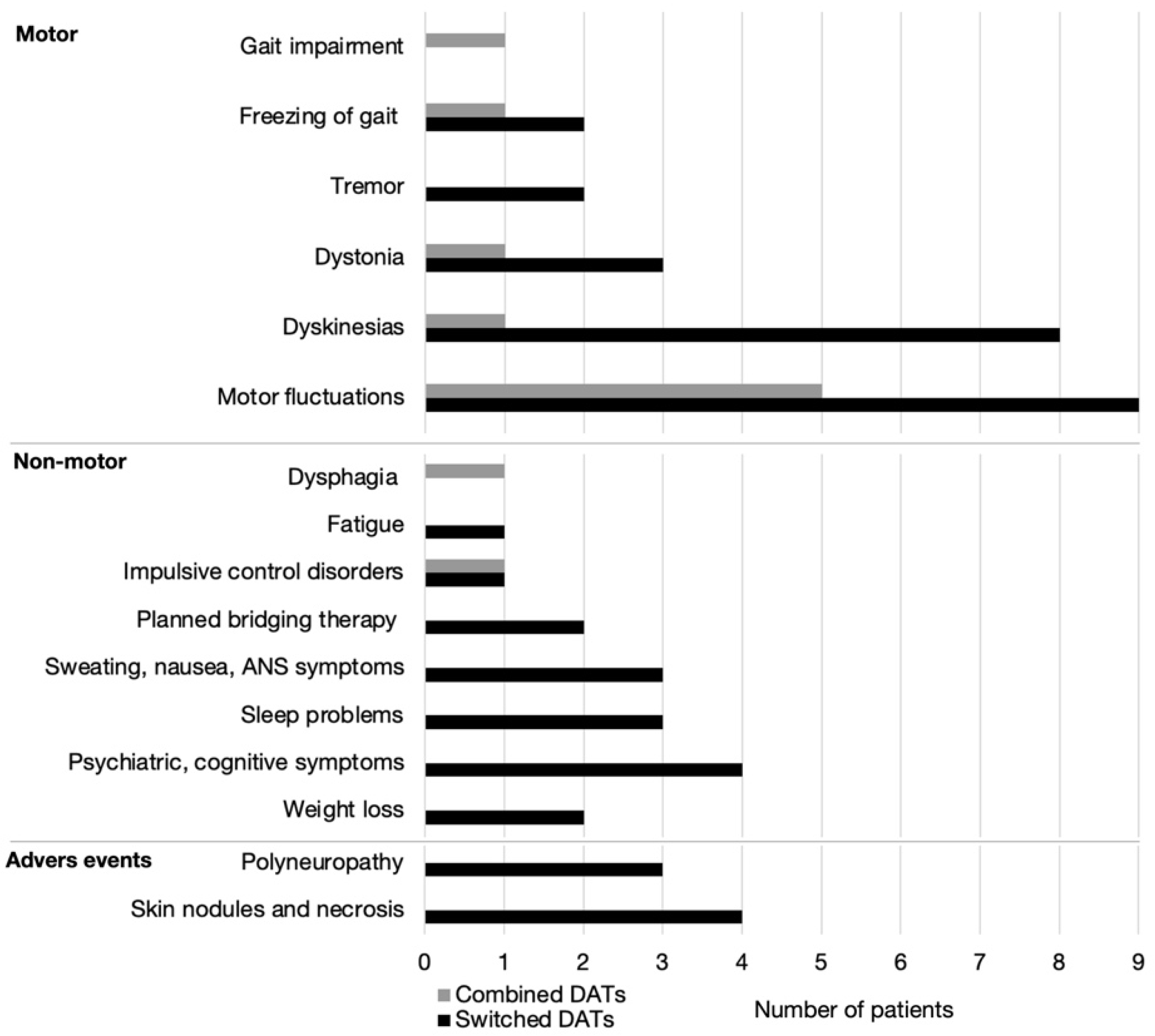
3.3. Motor vs. Non-Motor Reasons for Switching and Combining DATs
4. Discussion
4.1. Switching between DATs
4.2. Combining DATs
5. Limitations of the Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lees, A.J.; Hardy, J.; Revesz, T. Parkinson’s disease. Lancet 2009, 373, 2055–2066. [Google Scholar] [CrossRef]
- Antonini, A.; Moro, E.; Godeiro, C.; Reichmann, H. Medical and surgical management of advanced Parkinson’s disease. Mov. Disord. 2018, 33, 900–908. [Google Scholar] [CrossRef]
- Dafsari, H.S.; Martinez-Martin, P.; Rizos, A.; Trost, M.; Ghilardi, M.G.D.S.; Reddy, P.; Sauerbier, A.; Petry-Schmelzer, J.N.; Kramberger, M.; Borgemeester, R.W.K.; et al. EuroInf 2: Subthalamic stimulation, apomorphine, and levodopa infusion in Parkinson’s disease. Mov. Disord. 2019, 34, 353–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Martin, P.; Reddy, P.; Katzenschlager, R.; Antonini, A.; Todorova, A.; Odin, P.; Henriksen, T.; Martin, A.; Calandrella, D.; Rizos, A.; et al. EuroInf: AMulticenter Comparative Observational Study of Apomorphine and Levodopa Infusion in Parkinson’s Disease. Mov. Disord. 2014, 30, 510–516. [Google Scholar] [CrossRef]
- Volkmann, J.; Albanese, A.; Antonini, A.; Chaudhuri, K.R.; Clarke, C.E.; de Bie, R.M.A.; Deuschl, G.; Eggert, K.; Houeto, J.-L.; Kulisevsky, J.; et al. Selecting deep brain stimulation or infusion therapies in advanced Parkinson’s disease: An evidence-based review. J. Neurol. 2013, 260, 2701–2714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, N.; Murgai, A.; Naranian, T.; Jog, M.; Fasano, A. Levodopa-carbidopa intestinal gel therapy after deep brain stimulation. Mov. Disord. 2018, 33, 334–335. [Google Scholar] [CrossRef] [PubMed]
- Guy, W. ECDEU Assessment Manual for Psychopharmacology; U.S. Department of Health, Education, and Welfare Public Health Service, Alcohol, Drug Abuse, and Mental Health Administration, National Institute of Mental Health, Psychopharmacology Research Branch, Division of Extramural Research Programs: Rockville, MD, USA, 1976. [Google Scholar]
- Winge, K.; Werdelin, L.M.; Nielsen, K.K.; Stimpel, H. Effects of dopaminergic treatment on bladder function in Parkinson’s disease. Neurourol. Urodynamics 2004, 23, 689–696. [Google Scholar] [CrossRef]
- Aranda, B.; Cramer, P. Effects of apomorphine and L-dopa on the parkinsonian bladder. Neurourol. Urodynamics 1993, 12, 203–209. [Google Scholar] [CrossRef]
- Fitzmaurice, H.; Fowler, C.J.; Rickards, D.; Kirby, R.S.; Quinn, N.P.; Marsden, C.D.; Milroy, E.J.G.; Turner-Warwick, R.T. Micturition Disturbance in Parkinson’s Disease. Br. J. Urol. 1985, 57, 652–656. [Google Scholar] [CrossRef]
- Bhidayasiri, R.; Phokaewvarangkul, O.; Boonpang, K.; Boonmongkol, T.; Thongchuem, Y.; Kantachadvanich, N.; Ruiz, P.J.G. Long-term Apomorphine Infusion Users Versus Short-term Users: An International Dual-center Analysis of the Reasons for Discontinuing Therapy. Clin. Neuropharmacol. 2019, 42, 172–178. [Google Scholar] [CrossRef]
- Freire-Alvarez, E.; Kurča, E.; Manzanares, L.L.; Pekkonen, E.; Spanaki, C.; Vanni, P.; Liu, Y.; Sánchez-Soliño, O.; Barbato, L.M. Levodopa-Carbidopa Intestinal Gel Reduces Dyskinesia in Parkinson’s Disease in a Randomized Trial. Mov. Disord. 2021, 36, 2615–2623. [Google Scholar] [CrossRef] [PubMed]
- Van Poppelen, D.; Tromp, A.; de Bie, R.; Dijk, J. Combined and Sequential Treatment with Deep Brain Stimulation and Continuous Intrajejunal Levodopa Infusion for Parkinson’s Disease. J. Pers. Med. 2021, 11, 547. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Pajarín, G.; Sesar, Á.; Ares, B.; Jiménez-Martín, I.; Gelabert, M.; Arán-Echabe, E.; Relova, J.L.; Castro, A. Continuous Subcutaneous Apomorphine Infusion before Subthalamic Deep Brain Stimulation: A Prospective, Comparative Study in 20 Patients. Mov. Disord. Clin. Pr. 2021, 8, 1216–1224. [Google Scholar] [CrossRef]
- Sage, J.I.; McHale, D.M.; Sonsalla, P.; Vitagliano, D.; Heikkila, R.E. Continuous levodopa infusions to treat complex dystonia in Parkinson’s disease. Neurol. 1989, 39, 888. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, P.J.G.; Ignacio, Á.S.; Pensado, B.A.; García, A.C.; Frech, F.A.; López, M.Á.; González, J.A.; Octavio, J.B.; Hernández, J.A.B.; Garriga, M.C.; et al. Efficacy of long-term continuous subcutaneous apomorphine infusion in advanced Parkinson’s disease with motor fluctuations: A multicenter study. Mov. Disord. 2008, 23, 1130–1136. [Google Scholar] [CrossRef]
- Sesar, Á.; Fernández-Pajarín, G.; Ares, B.; Rivas, M.T.; Castro, A. Continuous subcutaneous apomorphine infusion in advanced Parkinson’s disease: 10-year experience with 230 patients. J. Neurol. 2017, 264, 946–954. [Google Scholar] [CrossRef]
- Sensi, M.; Cossu, G.; Mancini, F.; Pilleri, M.; Zibetti, M.; Modugno, N.; Quatrale, R.; Tamma, F.; Antonini, A.; Aguggia, M.; et al. Which patients discontinue? Issues on Levodopa/carbidopa intestinal gel treatment: Italian multicentre survey of 905 patients with long-term follow-up. Park. Relat. Disord. 2017, 38, 90–92. [Google Scholar] [CrossRef]
- Jick, S.S.; Oleske, D.M.; Persson, R.; Zamudio, J.; Facheris, M.F. Epidemiology of skin event rates among users of pumps for the subcutaneous administration of drugs for chronic conditions. Curr. Med Res. Opin. 2021, 37, 1563–1571. [Google Scholar] [CrossRef]
- Limousin, P.; Foltynie, T. Long-term outcomes of deep brain stimulation in Parkinson disease. Nat. Rev. Neurol. 2019, 15, 234–242. [Google Scholar] [CrossRef] [Green Version]
- Klostermann, F.; Jugel, C.; Marzinzik, F. Jejunal levodopa infusion in long-term DBS patients with Parkinson’s disease. Mov. Disord. 2011, 26, 2298–2299. [Google Scholar] [CrossRef]
- Boura, I.; Haliasos, N.; GiannopoulouΙ, I.-A.; Karabetsos, D.; Spanaki, C. Combining Device-Aided Therapies in Parkinson’s Disease: A Case Series and a Literature Review. Mov. Disord. Clin. Pr. 2021, 8, 750–757. [Google Scholar] [CrossRef]
- Elkouzi, A.; Ramirez-Zamora, A.; Zeilman, P.; Barabas, M.; Eisinger, R.; Malaty, I.; Okun, M.S.; Almeida, L. Rescue levodopa-carbidopa intestinal gel (LCIG) therapy in Parkinson’s disease patients with suboptimal response to deep brain stimulation. Ann. Clin. Transl. Neurol. 2019, 6, 1989–1995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regidor, I.; Benita, V.; Pedro, M.D.; Álamo, D.; Ley, L.; Castrillo, J.C.M. Duodenal Levodopa Infusion for Long-Term Deep Brain Stimulation–Refractory Symptoms in Advanced Parkinson Disease. Clin. Neuropharmacol. 2017, 40, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Mann, H.B.; Whitney, D.R. On a Test of Whether one of Two Random Variables is Stochastically Larger than the Other. Ann. Math. Stat. 1947, 18, 50–60. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Switched (n = 24) | Combined (n = 6) | |
|---|---|---|
| Gender (F:M) | 10:14 | 2:4 |
| Age at PD onset | 49 (29–66) | 55 (46–69) |
| PD duration at 1st DAT | 10 (7–28) | 7 (3–11) |
| Age at 1st DAT | 60 (38–74) | 62 (57–75) |
| Duration of 1st DAT | 1.75 (0.08–18) | 5 (3–10) |
| Age at 2nd DAT | 66 (39–77) | 68 (64–79) |
| Duration of 2nd DAT | 3 (0.08–9) | 3 (0.08–5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Georgiev, D.; Delalić, S.; Zupančič Križnar, N.; Socher, A.; Gurevich, T.; Trošt, M. Switching and Combining Device-Aided Therapies in Advanced Parkinson’s Disease: A Double Centre Retrospective Study. Brain Sci. 2022, 12, 343. https://doi.org/10.3390/brainsci12030343
Georgiev D, Delalić S, Zupančič Križnar N, Socher A, Gurevich T, Trošt M. Switching and Combining Device-Aided Therapies in Advanced Parkinson’s Disease: A Double Centre Retrospective Study. Brain Sciences. 2022; 12(3):343. https://doi.org/10.3390/brainsci12030343
Chicago/Turabian StyleGeorgiev, Dejan, Sentilija Delalić, Nina Zupančič Križnar, Achinoam Socher, Tanya Gurevich, and Maja Trošt. 2022. "Switching and Combining Device-Aided Therapies in Advanced Parkinson’s Disease: A Double Centre Retrospective Study" Brain Sciences 12, no. 3: 343. https://doi.org/10.3390/brainsci12030343