
Examining Association of Personality Characteristics and Neuropsychiatric Symptoms in Post-COVID Syndrome

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Statistical Analysis
3. Results
3.1. Comparison between Patients with Post-COVID Syndrome and Controls
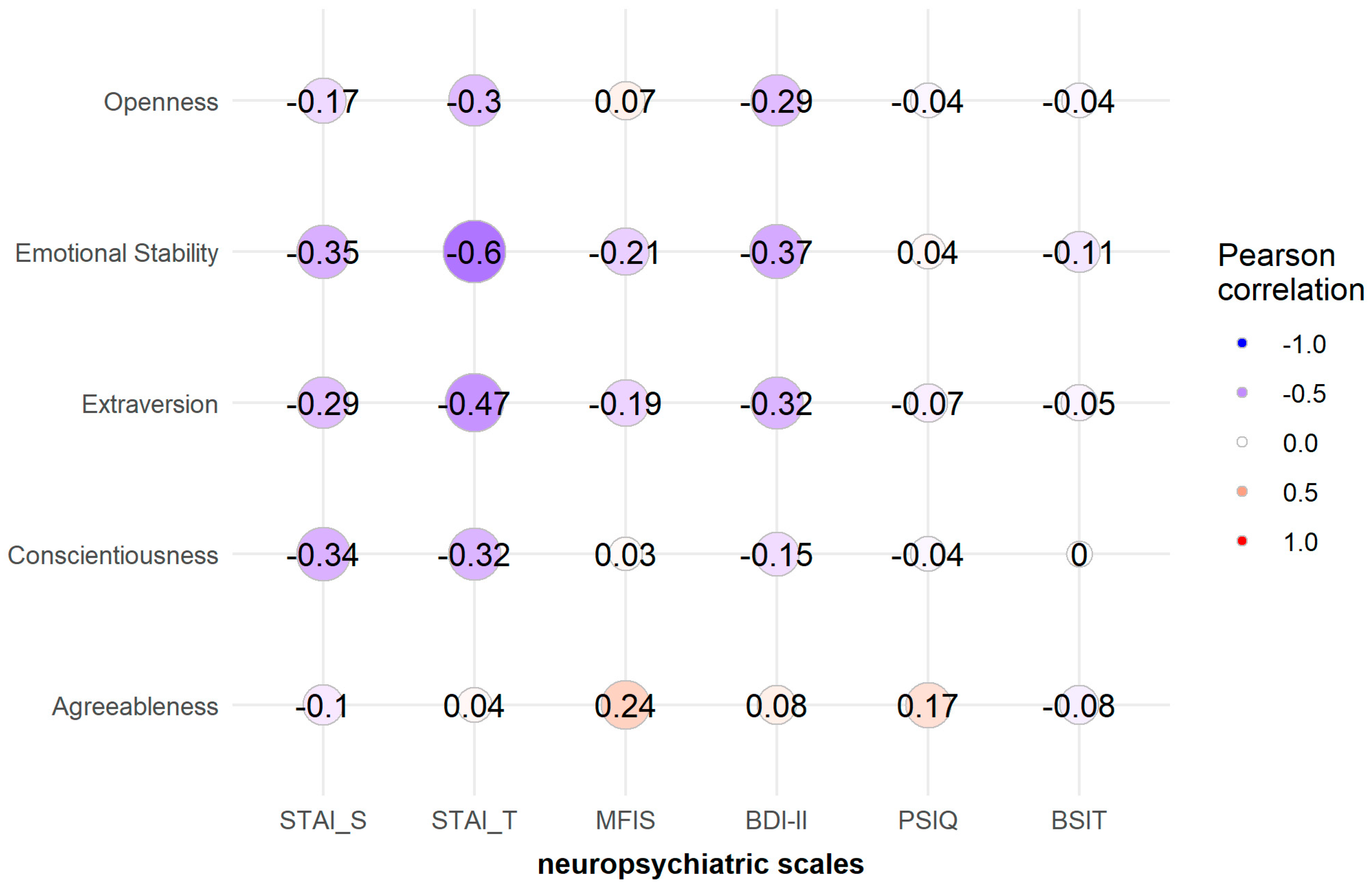
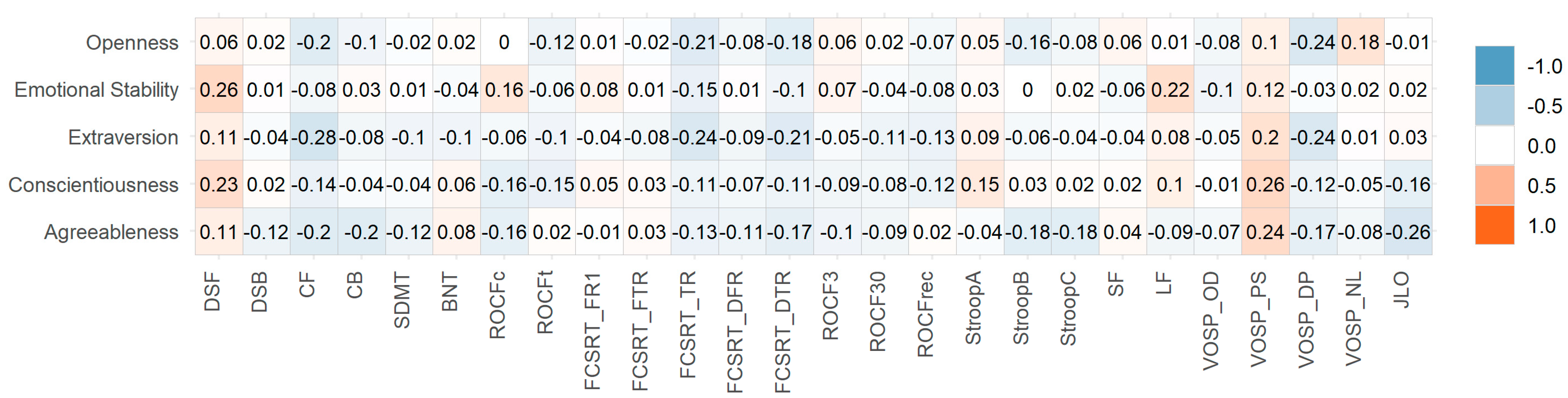
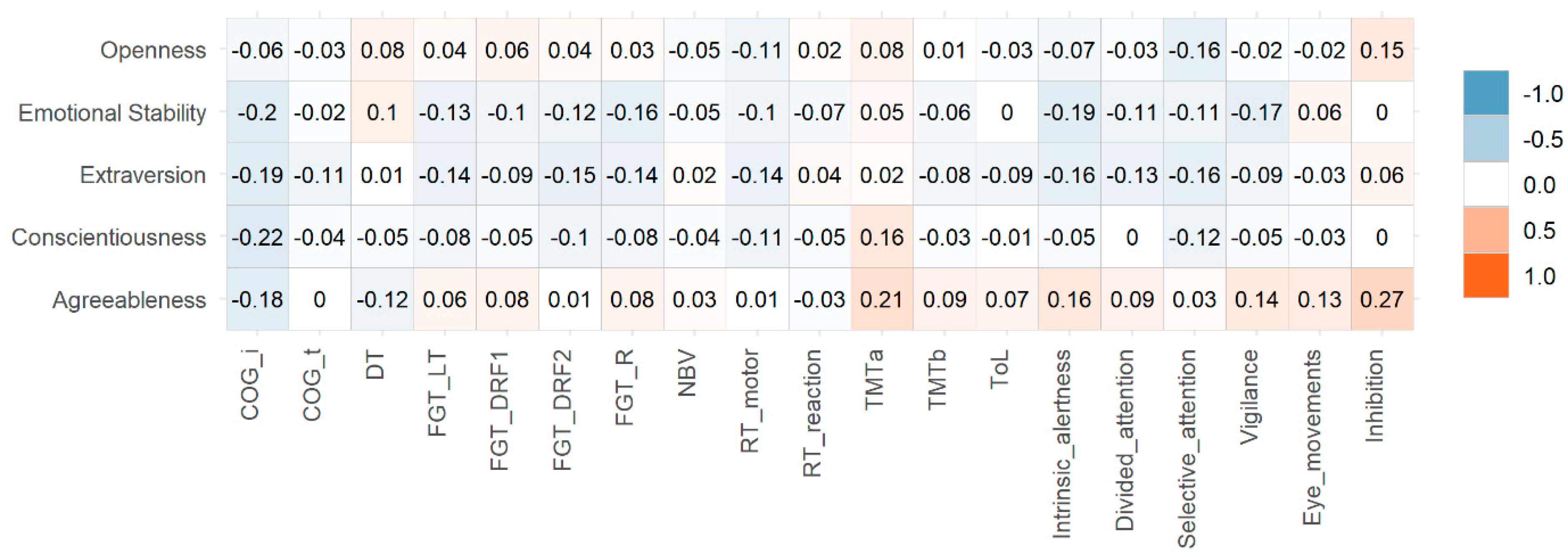
3.2. Correlation Analysis
3.3. Personality-Related Predictors of Depression and Anxiety
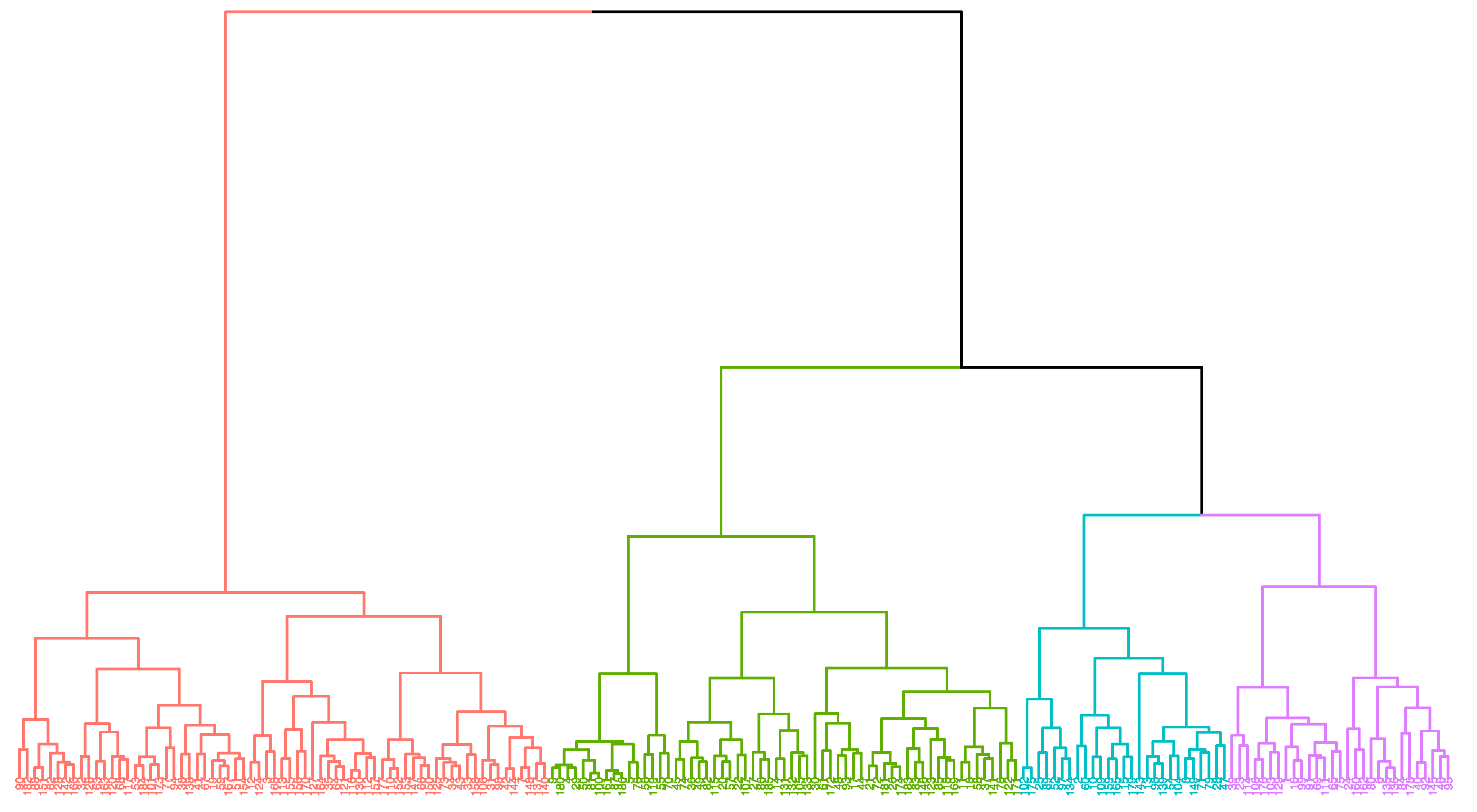
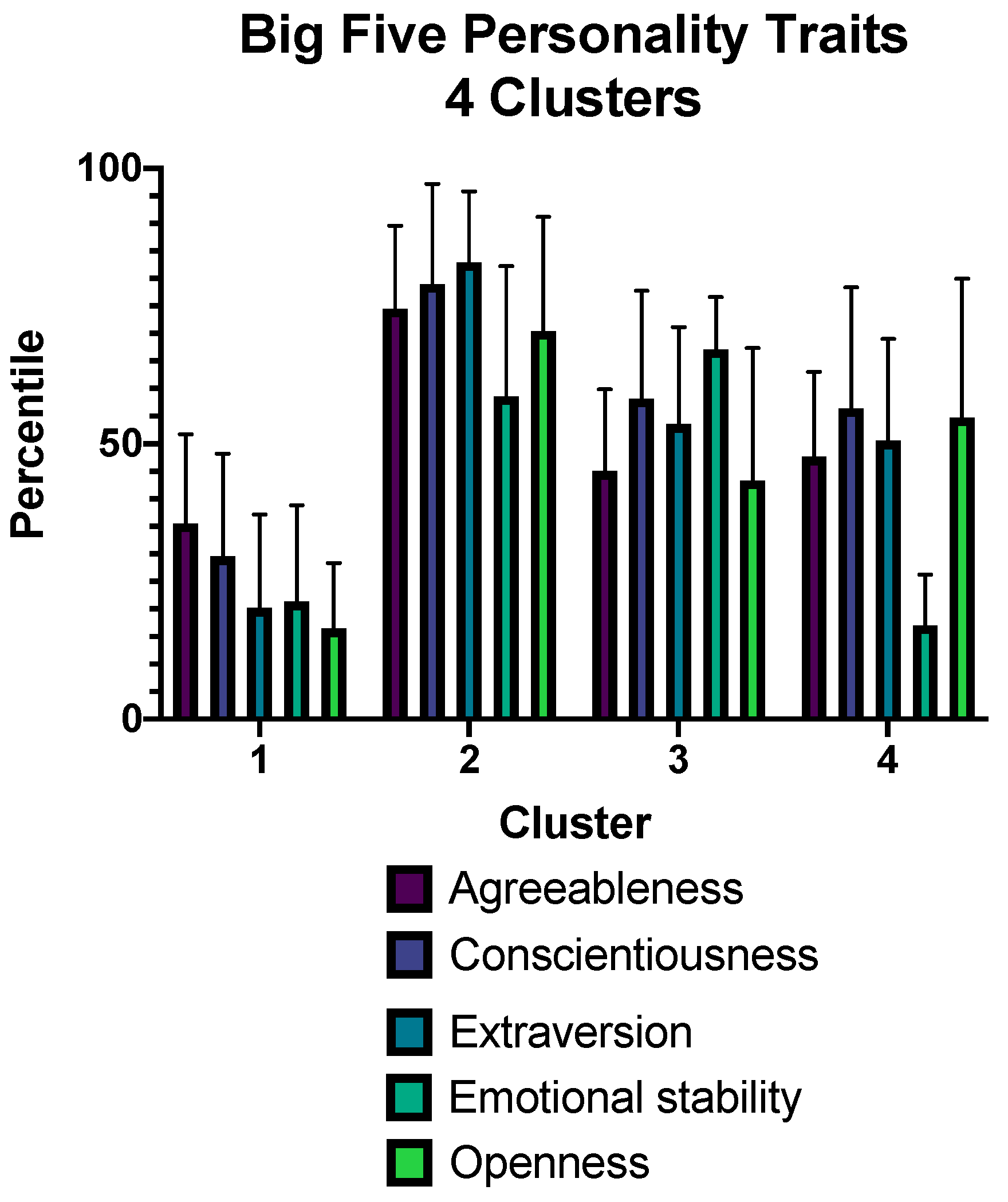
3.4. Cluster Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus, 6 October 2021. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (accessed on 8 February 2022).
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef] [PubMed]
- Premraj, L.; Kannapadi, N.V.; Briggs, J.; Seal, S.M.; Battaglini, D.; Fanning, J.; Suen, J.; Robba, C.; Fraser, J.; Cho, S.M. Mid and long-term neurological and neuropsychiatric manifestations of post-COVID-19 syndrome: A meta-analysis. J. Neurol. Sci. 2022, 434, 120162. [Google Scholar] [CrossRef] [PubMed]
- Maltezou, H.C.; Pavli, A.; Tsakris, A. Post-COVID syndrome: An insight on its pathogenesis. Vaccines 2021, 9, 497. [Google Scholar] [CrossRef]
- Apple, A.C.; Oddi, A.; Peluso, M.J.; Asken, B.; Henrich, T.J.; Kelly, H.J.; Pleasure, S.J.; Deeks, S.G.; Allen, I.E.; Martin, J.N.; et al. Risk factors and abnormal cerebrospinal fluid associate with cognitive symptoms after mild COVID-19. Ann. Clin. Transl. Neurol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Spudich, S.; Nath, A. Nervous system consequences of COVID-19. Science 2022, 375, 267–269. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Pinedo, U.; Matías-Guiu, J.; Sanclemente-Alaman, I.; Moreno-Jiménez, L.; Montero-Escribano, P.; Matias-Guiu, J.A. SARS-CoV-2 as a potential trigger of neurodegenerative diseases. Mov. Disord. 2020, 35, 1104–1105. [Google Scholar] [CrossRef] [PubMed]
- Matias-Guiu, J.A.; Delgado-Alonso, C.; Yus, M.; Polidura, C.; Gómez-Ruiz, N.; Valles-Salgado, M.; Ortega-Madueño, I.; Cabrera-Martín, M.N.; Matías-Guiu, J. “Brain fog” by COVID-19 or Alzheimer’s disease? A case report. Front. Psychol. 2021, 12, 724022. [Google Scholar] [CrossRef] [PubMed]
- Ka, L.; Elliott, R.; Ware, K.; Juhasz, G.; Lje, B. Associations between facets and aspects of Big Five Personality and affective disorders: A systematic review and best evidence synthesis. J. Affect. Disord. 2021, 288, 175–188. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, L.F.; Pianowski, G.; Gonçalves, A.P. Personality differences and COVID-19: Are extroversion and conscientiousness personality traits associated with engagement with containment measures? Trends Psychatry Psychother. 2020, 42, 179–184. [Google Scholar] [CrossRef]
- Airaksinen, J.; Komulainen, K.; Jokela, M.; Gluschkoff, K. Big Five personality traits and COVID-19 precautionary behaviors among older adults in Europe. Aging Health Res. 2021, 1, 100038. [Google Scholar] [CrossRef]
- Nikcevik, A.V.; Marino, C.; Kolubinski, D.C.; Leach, D.; Spada, M.M. Modelling the contribution of the Big Five Personality traits, health anxiety, and COVID-19 psychological distress to generalized anxiety and depressive symptoms during the COVID-19 pandemic. J. Affect. Disord. 2021, 279, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Proto, E.; Zhang, A. COVID-19 and mental health of individuals with different personalities. Proc. Natl. Acad. Sci. USA 2021, 118, e2109282118. [Google Scholar] [CrossRef]
- Gori, A.; Topino, E.; Palazzeschi, L.; Di Fabio, A. Which personality traits can mitigate the impact of the pandemic? Assessment of the relationship between personality traits and traumatic events in the COVID-19 pandemic as mediated by defense mechanisms. PLoS ONE 2021, 16, e0251984. [Google Scholar] [CrossRef]
- Naylor, B.; Boag, S.; Gustin, S.M. New evidence for a pain personality? A critical review of the last 120 years of pain and personality. Scand. J. Pain 2017, 17, 58–67. [Google Scholar] [CrossRef]
- García-Fontanals, A.; Portell, M.; García-Blanco, S.; Poca-Dias, V.; García-Fructuoso, F.; López-Ruiz, M.; Gutiérrez-Rosado, T.; Gomà-I-Freixanet, M.; Deus, J. Vulnerability to psychopathology and dimensions of personality in patients with fibromyalgia. Clin. J. Pain 2017, 33, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, M.E.; Weber, K.; Courvoisier, D.S.; Genevay, S. Big Five Personality traits and disabling chronic low pain: Association with fear-avoidance, anxious and depressive moods. J. Pain Res. 2020, 13, 745–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinberg, S.I.; Negash, S.; Sammel, M.D.; Bogner, H.; Harel, B.T.; Livney, M.G.; McCoubrey, H.; Wolk, D.A.; Kling, M.A.; Arnold, S.E. Subjective memory complaints, cognitive performance, and psychological factors in healthy older adults. Am. J. Alzheimer’s Dis. Other Dement. 2013, 28, 776–783. [Google Scholar] [CrossRef] [PubMed]
- Bell, T.; Hill, N.; Stavrinos, D. Personality determinants of subjective executive function in older adults. Aging Ment. Health 2020, 24, 1935–1944. [Google Scholar] [CrossRef]
- Fazeli, P.L.; Cheatwood, J.D.; Hopkins, C.; Vance, D.E.; Shirey, M.R.; Azuero, A.; Crowe, M. Association between personality and cognitive performance in middle-aged and older adults with human immunodeficiency virus (HIV). Appl. Neuropsychol. Adult 2021. [Google Scholar] [CrossRef]
- Penedo, F.J.; Gonzalez, J.S.; Dahn, J.R.; Antoni, M.; Malow, R.; Costa, P.; Schneiderman, N. Personality, quality of life and HAART adherence among men and women living with HIV/AIDS. J. Psychosom. Res. 2003, 54, 271–278. [Google Scholar] [CrossRef]
- Rzeszutek, M.; Gruszczynska, E. Consistency of health-related quality of life among people with HIV: Latent profile analysis. Health Qual. Life Outcomes 2018, 101, 16. [Google Scholar]
- O’Cleirigh, C.; Ironson, G.; Weiss, A.; Costa, P.T., Jr. Conscientiousness predicts disease progression (CD4 number and viral load) in people living with HIV. Health Psychol. 2007, 26, 473–480. [Google Scholar] [CrossRef]
- Castellvi, P.; Navinés, R.; Gutiérrez, F.; Jiménez, D.; Márquez, C.; Subirà, S.; Solà, R.; Martín-Santos, R. Pegylated interferón and ribavirin-induced depression in chronic hepatitis C: Role of personality. J. Clin. Psychiatry 2009, 70, 817–828. [Google Scholar] [CrossRef]
- Beck, A.; Steer, R.; Brown, G. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait. Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Kos, D.; Kerckhofs, E.; Carrea, I.; Verza, R.; Ramos, M.; Jansa, J. Evaluation of the Modified Fatigue Impact Scale in four different European countries. Mult. Scler. J. 2005, 11, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Alonso, C.; Valles-Salgado, M.; Delgado-Álvarez, A.; Yus, M.; Gómez-Ruiz, N.; Jorquera, M.; Polidura, C.; Gil, M.J.; Marcos, A.; Matías-Guiu, J.; et al. Cognitive dysfunction associated with COVID-19: A comprehensive neuropsychological study. Res. Sq. 2021. preprint. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Ward, J.H., Jr. Hierarchical grouping to optimize an objective function. J. Am. Stat. Assoc. 1963, 58, 234–244. [Google Scholar] [CrossRef]
- Chaumont, H.; Meppiel, E.; Roze, E.; Tressières, B.; de Broucker, T.; Lannuzel, A. Long-term outcomes after NeuroCOVID: A 6-month follow-up study on 60 patients. Rev. Neurol. 2022, 178, 137–143. [Google Scholar] [CrossRef]
- Krishan, K.; Miller, A.K.; Reiter, K.; Bonner-Jackson, A. Neurocognitive profiles in patients with persisting cognitive symptoms associated with COVID-19. Arch. Clin. Neuropsychol 2022. [Google Scholar] [CrossRef] [PubMed]
- Terracciano, A.; Stephan, Y.; Luchetti, M.; Albanese, E.; Sutin, A.R. Personality traits and risk of cognitive impairment and dementia. J. Psychiatr. Res. 2017, 89, 22–27. [Google Scholar] [CrossRef]
- Bessi, V.; Mazzeo, S.; Padiglioni, S.; Piccini, C.; Nacmias, B.; Sorbi, S.; Bracco, L. From subjective cognitive decline to Alzheimer’s disease: The predictive role of neuropsychological assessment, personality traits, and cognitive reserve. A 7-year follow-up study. J. Alzheimer’s Dis. 2018, 63, 1523–1535. [Google Scholar] [CrossRef]
- Rouch, I.; Padovan, C.; Pongan, E.; Boublay, N.; Laurent, B.; Dorey, J.M.; Krolak-Salmon, P. Personality traits are related to selective cognitive impairment in early Alzheimer’s disease. J. Alzheimer’s Dis. 2019, 71, 1153–1162. [Google Scholar] [CrossRef]
- Ayers, E.; Gulley, E.; Verghese, J. The effect of personality traits on risk of incident pre-dementia syndromes. J. Am. Geriatr. Soc. 2020, 68, 1554–1559. [Google Scholar] [CrossRef]
- Gerlach, M.; Farb, B.; Revelle, W.; Nunes Amaral, L.A. A robust data-driven approach identifies four personality types across four large data sets. Nature Hum. Behav. 2018, 2, 734–742. [Google Scholar] [CrossRef]
- Roberts, B.W.; DelVecchio, W.F. The rank-order consistency of personality traits from childhood to old age: A quantitative review of longitudinal studies. Psychol. Bull. 2000, 126, 3–25. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Post-COVID Syndrome | |
|---|---|
| Age | 50.39 ± 11.26 |
| Sex (women) | 66 (71.0%) |
| Years of schooling | 14.38 ± 3.64 |
| BDI-II | 14.03 ± 8.48 |
| STAI-S | 40.86 ± 11.57 |
| STAI-T | 48.18 ± 10.52 |
| MFIS | 52.96 ± 15.14 |
| PSQI | 9.96 ± 4.74 |
| BSIT | 8.92 ± 2.50 |
| Post-COVID Syndrome | Healthy Controls | t (p Value) | |
|---|---|---|---|
| Agreeableness | 47.94 ± 22.47 | 55.66 ± 22.40 | 2.34 (0.020) |
| Conscientiousness | 50.33 ± 29.05 | 58.38 ± 26.82 | 1.96 (0.051) |
| Extraversion | 45.04 ± 30.79 | 56.38 ± 29.78 | 2.55 (0.012) |
| Emotional stability | 34.15 ± 27.00 | 45.24 ± 27.00 | 2.79 (0.006) |
| Openness | 40.02 ± 31.45 | 48.62 ± 28.09 | 1.96 (0.051) |
| Post-COVID Syndrome | Healthy Controls | t (p Value) | ||
|---|---|---|---|---|
| Agreeableness | Willingness to trust | 39.94 ± 27.26 | 48.10 ± 29.01 | 1.97 (0.050) |
| Genuineness | 54.58 ± 26.27 | 60.10 ± 26.52 | 1.42 (0.156) | |
| Helpfulness | 65.03 ± 27.38 | 74.15 ± 23.25 | 2.44 (0.015) | |
| Obligingness | 61.39 ± 28.49 | 67.72 ± 23.97 | 1.64 (0.103) | |
| Modesty | 33.34 ± 22.02 | 41.54 ± 23.39 | 2.45 (0.015) | |
| Good-naturedness | 57.10 ± 27.88 | 65.14 ± 26.19 | 2.02 (0.044) | |
| Conscientiousness | Competence | 46.17 ± 26.45 | 55.60 ± 25.27 | 2.48 (0.014) |
| Love of order | 31.43 ± 26.12 | 41.11 ± 30.96 | 2.30 (0.022) | |
| Sense of duty | 55.72 ± 24.87 | 61.59 ± 23.84 | 1.64 (0.102) | |
| Ambition | 53.65 ± 26.94 | 59.26 ± 24.36 | 1.49 (0.138) | |
| Discipline | 50.71 ± 29.46 | 58.40 ± 25.90 | 1.80 (0.060) | |
| Caution | 74.33 ± 22.96 | 76.53 ± 22.54 | 0.65 (0.512) | |
| Extraversion | Friendliness | 55.56 ± 25.94 | 64.11 ± 25.42 | 2.26 (0.024) |
| Sociableness | 60.52 ± 28.97 | 71.48 ± 26.25 | 2.70 (0.007) | |
| Assertiveness | 38.22 ± 25.25 | 43.11 ± 25.57 | 1.31 (0.191) | |
| Dynamism | 57.48 ± 32.21 | 66.08 ± 28.84 | 1.91 (0.057) | |
| Adventurousness | 24.29 ± 24.71 | 26.74 ± 23.12 | 0.69 (0.486) | |
| Cheerfulness | 45.69 ± 34.00 | 58.38 ± 32.65 | 2.59 (0.010) | |
| Emotional stability | Careefreeness | 26.29 ± 25.42 | 29.43 ± 25.79 | 0.83 (0.404) |
| Equanimity | 28.61 ± 22.21 | 39.13 ± 24.05 | 3.09 (0.002) | |
| Positive mood | 32.70 ± 29.71 | 45.60 ± 29.52 | 2.97 (0.003) | |
| Social confidence | 37.52 ± 27.06 | 46.18 ± 28.28 | 2.13 (0.034) | |
| Self-control | 46.81 ± 23.67 | 57.09 ± 25.50 | 2.84 (0.005) | |
| Emotional robustness | 26.85 ± 25.63 | 35.05 ± 26.30 | 2.15 (0.033) | |
| Openness | Openness to imagination | 45.83 ± 32.17 | 54.41 ± 28.24 | 1.93 (0.055) |
| Openness to aesthetics | 25.80 ± 20.72 | 27.87 ± 21.18 | 0.675 (0.500) | |
| Openness to feelings | 62.63 ± 31.14 | 65.43 ± 29.38 | 0.630 (0.530) | |
| Openness to actions | 35.13 ± 31.07 | 44.54 ± 29.18 | 2.12 (0.035) | |
| Openness to ideas | 54.33 ± 34.68 | 65.73 ± 29.79 | 2.40 (0.017) | |
| Openness to values | 38.16 ± 24.32 | 44.88 ± 25.37 | 1.84 (0.067) |
| R2 | Variables (Transformed) | Beta Coefficient | SE | t | 95% CI | p Value | Importance |
|---|---|---|---|---|---|---|---|
| BDI-II (depression) | |||||||
| 0.363 | Intercept | 10.557 | 2.601 | 4.059 | 5.384, 15.731 | <0.001 | - |
| Openness to ideas | −0.16 | 0.042 | −3.86 | <0.001 | 0.32 | ||
| Obligingness | 0.089 | 0.031 | 2.881 | 0.027, 0.150 | 0.05 | 0.178 | |
| Dynamism | −0.078 | 0.030 | −2.627 | −0.137, −0.019 | 0.010 | 0.148 | |
| Openness to feelings | 0.078 | 0.036 | 2.132 | 0.005, 0.150 | 0.036 | 0.098 | |
| STAI-S (anxiety) | |||||||
| 0.410 | Intercept | 38.042 | 3.496 | 10.881 | 31.083, 45.001 | <0.001 | - |
| Openness to actions | −0.222 | 0.063 | −3.515 | −0.347, −0.096 | 0.001 | 0.153 | |
| Caution | −0.209 | 0.060 | −3.494 | −0.328, −0.090 | 0.001 | 0.151 | |
| Love of order | 0.144 | 0.050 | 2.886 | 0.045, 0.243 | 0.005 | 0.103 | |
| Competence | −0.232 | 0.082 | −2.846 | −0.395, −0.070 | 0.006 | 0.100 | |
| Cheerfulness | −0.108 | 0.042 | −2.568 | −0.192, −0.024 | 0.012 | 0.082 | |
| Social confidence | 0.185 | 0.072 | 2.562 | 0.041, 0.328 | 0.012 | 0.081 | |
| Adventurousness | 0.196 | 0.078 | 2.497 | 0.040, 0.352 | 0.015 | 0.077 | |
| Discipline | 0.136 | 0.058 | 2.335 | 0.020, 0.252 | 0.022 | 0.068 | |
| Assertiveness | −0.122 | 0.059 | −2.073 | −0.239, −0.005 | 0.041 | 0.053 | |
| Openness to aesthetics | 0.131 | 0.064 | 2.030 | 0.003, 0.259 | 0.046 | 0.051 | |
| Cluster 1 | Cluster 2 | Cluster 3 | Cluster 4 | F (p Value) | |
|---|---|---|---|---|---|
| Number of patients with COVID-19/number of controls | 43/25 | 23/39 | 13/14 | 14/15 | 8.96 * (0.030) |
| Age | 53.74 ± 9.57 | 47.43 ± 10.88 | 52.83 ± 13.40 | 43.64 ± 11.46 | 4.02 (0.010) c |
| Sex (women) | 29 (67.4%) | 17 (73.9%) | 8 (61.5%) | 12 (85.7%) | 2.57 * (0.461) |
| BDI-II | 16.72 ± 8.77 | 10.30 ± 6.69 | 9.67 ± 7.79 | 15.77 ± 7.60 | 4.66 (0.005) a,b |
| STAI-S | 24.51 ± 11.11 | 13.39 ± 8.78 | 19.00 ± 12.71 | 23.50 ± 10.71 | 5.74 (0.001) a,d |
| STAI-T | 32.65 ± 8.28 | 22.70 ± 9.33 | 19.58 ± 12.09 | 30.86 ± 9.32 | 9.88 (<0.001) a,b,c,e |
| MFIS | 55.07 ± 13.14 | 48.35 ± 17.29 | 50.67 ± 18.47 | 56.23 ± 13.42 | 1.29 (0.281) |
| PSQI | 10.07 ± 4.93 | 9.82 ± 4.87 | 8.45 ± 4.52 | 11.00 ± 4.26 | 0.59 (0.617) |
| BSIT | 8.98 ± 2.45 | 9.17 ± 2.05 | 8.75 ± 3.30 | 8.50 ± 2.79 | 0.229 (0.876) |
| SDMT | 43.21 ± 15.31 | 41.17 ± 11.09 | 42.75 ± 11.45 | 47.29 ± 11.47 | 0.616 (0.606) |
| BNT | 51.86 ± 5.61 | 50.65 ± 6.28 | 50.92 ± 7.63 | 53.07 ± 3.68 | 0.579 (0.630) |
| FGT-LT | 53.74 ± 9.57 | 47.43 ± 10.88 | 51.77 ± 13.39 | 43.64 ± 11.46 | 0.338 (0.798) |
| ROCF-c | 33.18± 3.20 | 32.13 ± 3.52 | 32.83 ± 2.40 | 32.07 ± 5.70 | 0.576 (0.632) |
| JLO | 20.65 ± 7.19 | 19.78 ± 5.14 | 21.67 ± 5.29 | 19.57 ± 7.34 | 0.314 (0.815) |
| NBV | 8.90 ± 13.66 | 7.93 ± 7.91 | 9.10 ± 11.90 | 9.25 ± 11.45 | 0.035 (0.991) |
| TMT-B | 49.22 ± 36.56 | 44.22 ± 18.22 | 49.04 ± 26.27 | 37.31 ± 8.40 | 0.560 (0.643) |
| ToL | 13.23 ± 3.77 | 13.25 ± 2.14 | 10.70 ± 2.00 | 13.16 ± 3.99 | 1.650 (0.185) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delgado-Alonso, C.; Valles-Salgado, M.; Delgado-Álvarez, A.; Gómez-Ruiz, N.; Yus, M.; Polidura, C.; Pérez-Izquierdo, C.; Marcos, A.; Gil, M.J.; Matías-Guiu, J.; et al. Examining Association of Personality Characteristics and Neuropsychiatric Symptoms in Post-COVID Syndrome. Brain Sci. 2022, 12, 265. https://doi.org/10.3390/brainsci12020265
Delgado-Alonso C, Valles-Salgado M, Delgado-Álvarez A, Gómez-Ruiz N, Yus M, Polidura C, Pérez-Izquierdo C, Marcos A, Gil MJ, Matías-Guiu J, et al. Examining Association of Personality Characteristics and Neuropsychiatric Symptoms in Post-COVID Syndrome. Brain Sciences. 2022; 12(2):265. https://doi.org/10.3390/brainsci12020265
Chicago/Turabian StyleDelgado-Alonso, Cristina, María Valles-Salgado, Alfonso Delgado-Álvarez, Natividad Gómez-Ruiz, Miguel Yus, Carmen Polidura, Carlos Pérez-Izquierdo, Alberto Marcos, María José Gil, Jorge Matías-Guiu, and et al. 2022. "Examining Association of Personality Characteristics and Neuropsychiatric Symptoms in Post-COVID Syndrome" Brain Sciences 12, no. 2: 265. https://doi.org/10.3390/brainsci12020265