

Facial Emotion Recognition Deficit in Children with Moderate/Severe Obstructive Sleep Apnea


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
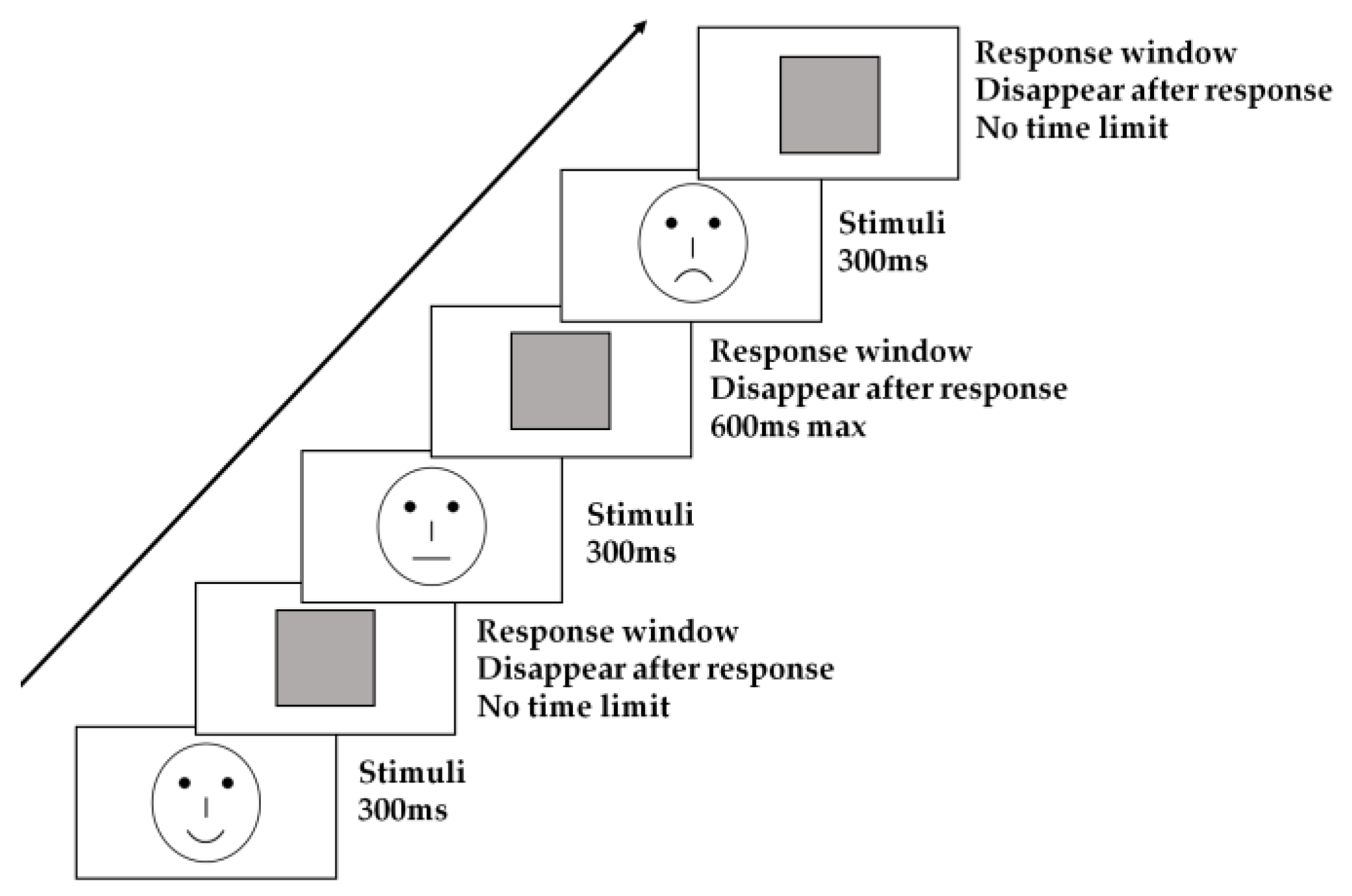
2.2. Procedure
2.3. Overnight Polysomnography (PSG)
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics and PSG Characteristics
3.2. Behavioral Performance
3.3. Correlations Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AASM | American Academy of Sleep Medicine |
| ACC | accuracy rate |
| ADHD | attention deficit and hyperactivity disorder |
| AHI | apnea-hypopnea index |
| ArI | arousal index |
| BMI | body mass index |
| MAOSA | moderate/severe obstructive sleep apnea |
| OAHI | obstructive apnea-hypopnea index |
| OSA | obstructive sleep apnea |
| PCA | positive classification advantage |
| PS | primary snoring |
| PSG | polysomnography |
| RT | reaction time |
| SaO2 | arterial oxygen |
| SD | standard deviation |
| SDB | sleep-disordered breathing |
| SDQ | strengths and difficulties questionnaire |
| SE | standard error |
| TST | total sleep time |
References
- Guo, Y.; Pan, Z.; Gao, F.; Wang, Q.; Pan, S.; Xu, S.; Hui, Y.; Li, L.; Qian, J. Characteristics and risk factors of children with sleep-disordered breathing in Wuxi, China. BMC Pediatr. 2020, 20, 310. [Google Scholar] [CrossRef] [PubMed]
- Operto, F.F.; Precenzano, F.; Bitetti, I.; Lanzara, V.; Fontana, M.L.; Pastorino, G.M.G.; Carotenuto, M.; Pisani, F.; Polito, A.N.; Smirni, D.; et al. Emotional Intelligence in Children with Severe Sleep-Related Breathing Disorders. Behav. Neurol. 2019, 2019, 6530539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kheirandish-Gozal, L.; Yoder, K.; Kulkarni, R.; Gozal, D.; Decety, J. Preliminary functional MRI neural correlates of executive functioning and empathy in children with obstructive sleep apnea. Sleep 2014, 37, 587–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelayo, R.; Sivan, Y. Increased behavioral morbidity in school-aged children with sleep-disordered breathing. Pediatrics 2005, 116, 797–798. [Google Scholar] [CrossRef]
- Dollion, N.; Grandgeorge, M.; Saint-Amour, D.; Hosein Poitras Loewen, A.; Francois, N.; Fontaine, N.M.G.; Champagne, N.; Plusquellec, P. Emotion Facial Processing in Children With Autism Spectrum Disorder: A Pilot Study of the Impact of Service Dogs. Front. Psychol. 2022, 13, 869452. [Google Scholar] [CrossRef]
- Kyle, S.D.; Beattie, L.; Spiegelhalder, K.; Rogers, Z.; Espie, C.A. Altered emotion perception in insomnia disorder. Sleep 2014, 37, 775–783. [Google Scholar] [CrossRef]
- Leppanen, J.M.; Hietanen, J.K. Positive facial expressions are recognized faster than negative facial expressions, but why? Psychol. Res. 2004, 69, 22–29. [Google Scholar] [CrossRef]
- Liu, X.; Liao, Y.; Zhou, L.; Sun, G.; Li, M.; Zhao, L. Mapping the time course of the positive classification advantage: An ERP study. Cogn. Affect. Behav. Neurosci. 2013, 13, 491–500. [Google Scholar] [CrossRef]
- Guo, J.; Ma, Y.; Liu, Z.; Wang, F.; Hou, X.; Chen, J.; Hong, Y.; Xu, S.; Liu, X. Performance of facial expression classification tasks in patients with obstructive sleep apnea. J. Clin. Sleep Med. 2020, 16, 523–530. [Google Scholar] [CrossRef]
- Lee, V.V.; Schembri, R.; Jordan, A.S.; Jackson, M.L. The independent effects of sleep deprivation and sleep fragmentation on processing of emotional information. Behav. Brain Res. 2022, 424, 113802. [Google Scholar] [CrossRef]
- Collin, L.; Bindra, J.; Raju, M.; Gillberg, C.; Minnis, H. Facial emotion recognition in child psychiatry: A systematic review. Res. Dev. Disabil. 2013, 34, 1505–1520. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.; Chen, S.; Zhao, L.; Miao, D. Categorization of emotional faces in schizophrenia patients: An ERP study. Neurosci. Lett. 2019, 713, 134493. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Liu, X.; Zhao, L. Categorization of Emotional Faces in Insomnia Disorder. Front. Neurol. 2020, 11, 569. [Google Scholar] [CrossRef] [PubMed]
- Operto, F.F.; Pastorino, G.M.G.; Stellato, M.; Morcaldi, L.; Vetri, L.; Carotenuto, M.; Viggiano, A.; Coppola, G. Facial Emotion Recognition in Children and Adolescents with Specific Learning Disorder. Brain Sci. 2020, 10, 473. [Google Scholar] [CrossRef]
- Aspan, N.; Bozsik, C.; Gadoros, J.; Nagy, P.; Inantsy-Pap, J.; Vida, P.; Halasz, J. Emotion recognition pattern in adolescent boys with attention-deficit/hyperactivity disorder. BioMed Res. Int. 2014, 2014, 761340. [Google Scholar] [CrossRef] [Green Version]
- Xin, W.; Yu, R.; Zhao, L. Event-related-potential based evidence of cognitive dysfunction of processing emotional faces in major depressive disorder patients. Neurosci. Lett. 2021, 742, 135545. [Google Scholar] [CrossRef]
- Tempesta, D.; Couyoumdjian, A.; Curcio, G.; Moroni, F.; Marzano, C.; de Gennaro, L.; Ferrara, M. Lack of sleep affects the evaluation of emotional stimuli. Brain Res. Bull. 2010, 82, 104–108. [Google Scholar] [CrossRef]
- Franzen, P.L.; Buysse, D.J.; Dahl, R.E.; Thompson, W.; Siegle, G.J. Sleep deprivation alters pupillary reactivity to emotional stimuli in healthy young adults. Biol. Psychol. 2009, 80, 300–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Helm, E.; Gujar, N.; Walker, M.P. Sleep deprivation impairs the accurate recognition of human emotions. Sleep 2010, 33, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Killgore, W.D.S.; Balkin, T.J.; Yarnell, A.M.; Capaldi, V.F., II. Sleep deprivation impairs recognition of specific emotions. Neurobiol. Sleep Circadian Rhythm. 2017, 3, 10–16. [Google Scholar] [CrossRef]
- Menzies, B.; Teng, A.; Burns, M.; Lah, S. Neurocognitive outcomes of children with sleep disordered breathing: A systematic review with meta-analysis. Sleep Med. Rev. 2022, 63, 101629. [Google Scholar] [CrossRef] [PubMed]
- Soffer-Dudek, N.; Sadeh, A.; Dahl, R.E.; Rosenblat-Stein, S. Poor sleep quality predicts deficient emotion information processing over time in early adolescence. Sleep 2011, 34, 1499–1508. [Google Scholar] [CrossRef] [PubMed]
- Cronlein, T.; Langguth, B.; Eichhammer, P.; Busch, V. Impaired Recognition of Facially Expressed Emotions in Different Groups of Patients with Sleep Disorders. PLoS ONE 2016, 11, e0152754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mei, L.; Li, X.; Zhou, G.; Ji, T.; Chen, J.; Xu, Z.; Peng, Y.; Liu, Y.; Li, H.; Zhang, J.; et al. Effects of obstructive sleep apnoea severity on neurocognitive and brain white matter alterations in children according to sex: A tract-based spatial statistics study. Sleep Med. 2021, 82, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Macey, P.M.; Cross, R.L.; Woo, M.A.; Yan-Go, F.L.; Harper, R.M. Neural alterations associated with anxiety symptoms in obstructive sleep apnea syndrome. Depress. Anxiety 2009, 26, 480–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawrence, K.; Campbell, R.; Skuse, D. Age, gender, and puberty influence the development of facial emotion recognition. Front. Psychol. 2015, 6, 761. [Google Scholar] [CrossRef] [Green Version]
- Gregory, A.M.; Sadeh, A. Sleep, emotional and behavioral difficulties in children and adolescents. Sleep Med. Rev. 2012, 16, 129–136. [Google Scholar] [CrossRef] [Green Version]
- Walker, M.P.; van der Helm, E. Overnight therapy? The role of sleep in emotional brain processing. Psychol. Bull. 2009, 135, 731–748. [Google Scholar] [CrossRef] [Green Version]
- Holding, B.C.; Laukka, P.; Fischer, H.; Banziger, T.; Axelsson, J.; Sundelin, T. Multimodal Emotion Recognition Is Resilient to Insufficient Sleep: Results From Cross-Sectional and Experimental Studies. Sleep 2017, 40, zsx145. [Google Scholar] [CrossRef] [Green Version]
- Romero-Rebollar, C.; Garcia-Gomez, L.; Baez-Yanez, M.G.; Gutierrez-Aguilar, R.; Pacheco-Lopez, G. Adiposity affects emotional information processing. Front. Psychol. 2022, 13, 879065. [Google Scholar] [CrossRef]
- Vaioli, G.; Scarpina, F. Facial Emotion Recognition in Obesity and in Fibromyalgia: A Systematic Review. NeuroSci 2021, 2, 25. [Google Scholar] [CrossRef]
- Cooper, S.; Hobson, C.W.; van Goozen, S.H. Facial emotion recognition in children with externalising behaviours: A systematic review. Clin. Child Psychol. Psychiatry 2020, 25, 1068–1085. [Google Scholar] [CrossRef]
- Goodman, R. The Strengths and Difficulties Questionnaire: A research note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Paine, A.L.; van Goozen, S.H.M.; Burley, D.T.; Anthony, R.; Shelton, K.H. Facial emotion recognition in adopted children. Eur. Child Adolesc. Psychiatry 2021, 1–13. [Google Scholar] [CrossRef]
- Staff, A.I.; Luman, M.; van der Oord, S.; Bergwerff, C.E.; van den Hoofdakker, B.J.; Oosterlaan, J. Facial emotion recognition impairment predicts social and emotional problems in children with (subthreshold) ADHD. Eur. Child Adolesc. Psychiatry 2022, 31, 715–727. [Google Scholar] [CrossRef]
- Hunnikin, L.M.; Wells, A.E.; Ash, D.P.; van Goozen, S.H.M. The nature and extent of emotion recognition and empathy impairments in children showing disruptive behaviour referred into a crime prevention programme. Eur. Child Adolesc. Psychiatry 2020, 29, 363–371. [Google Scholar] [CrossRef] [Green Version]
- Burley, D.T.; Hobson, C.W.; Adegboye, D.; Shelton, K.H.; van Goozen, S.H.M. Negative parental emotional environment increases the association between childhood behavioral problems and impaired recognition of negative facial expressions. Dev. Psychopathol. 2022, 34, 936–945. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Kou, J.; Coghill, D. The validity, reliability and normative scores of the parent, teacher and self report versions of the Strengths and Difficulties Questionnaire in China. Child Adolesc. Psychiatry Ment. Health 2008, 2, 8. [Google Scholar] [CrossRef] [Green Version]
- Kou, J.; Du, Y.; Xia, L. Reliability and validity of “children strengths and difficulties questionnaire” in Shanghai norm. Shanghai Arch. Psychiatry 2005, 17, 25–28. [Google Scholar]
- Xu, Q.; Yang, Y.; Wang, P.; Sun, G.; Zhao, L. Gender differences in preattentive processing of facial expressions: An ERP study. Brain Topogr. 2013, 26, 488–500. [Google Scholar] [CrossRef]
- MacDonald, P.M.; Kirkpatrick, S.W.; Sullivan, L.A. Schematic drawings of facial expressions for emotion recognition and interpretation by preschool-aged children. Genet. Soc. Gen. Psychol. Monogr. 1996, 122, 373–388. [Google Scholar]
- Wright, C.I.; Martis, B.; Shin, L.M.; Fischer, H.; Rauch, S.L. Enhanced amygdala responses to emotional versus neutral schematic facial expressions. Neuroreport 2002, 13, 785–790. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Sleep Medicine. The International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2014. [Google Scholar]
- Working group of Chinese Guideline for the Diagnosis and Treatment of Childhood OSA; Subspecialty Group of Pediatrics, Society of Otorhinolaryngology Head and Neck Surgery, Chinese Medical Association; Subspecialty Group of Respiratory Diseases, Society of Pediatrics, Chinese Medical Association; Society of Pediatric Surgery, Chinese Medical Association; Editorial Board of Chinese Journal of Otorhinolaryngology Head and Neck Surgery; Ni, X. Chinese guideline for the diagnosis and treatment of childhood obstructive sleep apnea (2020). Pediatr. Investig. 2021, 5, 167–187. [Google Scholar] [CrossRef]
- Hunter, S.J.; Gozal, D.; Smith, D.L.; Philby, M.F.; Kaylegian, J.; Kheirandish-Gozal, L. Effect of Sleep-disordered Breathing Severity on Cognitive Performance Measures in a Large Community Cohort of Young School-aged Children. Am. J. Respir. Crit. Care Med. 2016, 194, 739–747. [Google Scholar] [CrossRef] [Green Version]
- Horne, R.S.; Yang, J.S.; Walter, L.M.; Richardson, H.L.; O’Driscoll, D.M.; Foster, A.M.; Wong, S.; Ng, M.L.; Bashir, F.; Patterson, R.; et al. Nocturnal dipping is preserved in children with sleep disordered breathing regardless of its severity. Pediatr. Pulmonol. 2013, 48, 1127–1134. [Google Scholar] [CrossRef]
- Yang, J.S.; Nicholas, C.L.; Nixon, G.M.; Davey, M.J.; Anderson, V.; Walker, A.M.; Trinder, J.A.; Horne, R.S. Determining sleep quality in children with sleep disordered breathing: EEG spectral analysis compared with conventional polysomnography. Sleep 2010, 33, 1165–1172. [Google Scholar] [CrossRef] [Green Version]
- Beattie, L. How does sleep affect the perception of facial emotion? Sleep 2018, 41, zsy030. [Google Scholar] [CrossRef] [Green Version]
- Chang, F.; Klumpp, H. Sleep quality and emotion recognition in individuals with and without internalizing psychopathologies. J. Behav. Ther. Exp. Psychiatry 2022, 75, 101719. [Google Scholar] [CrossRef]
- Zsido, A.N.; Arato, N.; Ihasz, V.; Basler, J.; Budai, T.; Inhof, O.; Schacht, A.; Labadi, B.; Coelho, C.M. ‘Finding an emotional face’revisited: Differences in own-age bias and the happiness superiority effect in children and young adults. Front. Psychol. 2021, 12, 764. [Google Scholar] [CrossRef]
- Zhao, J.; Meng, Q.; An, L.; Wang, Y. An event-related potential comparison of facial expression processing between cartoon and real faces. PLoS ONE 2019, 14, e0198868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, J.; Liu, M.; Yao, S.; Yan, Y.; Ding, H.; Yan, T.; Zhao, L.; Xu, G. Classification of Emotional Expressions Is Affected by Inversion: Behavioral and Electrophysiological Evidence. Front. Behav. Neurosci. 2017, 11, 21. [Google Scholar] [CrossRef] [Green Version]
- Calvo, M.G.; Nummenmaa, L. Detection of emotional faces: Salient physical features guide effective visual search. J. Exp. Psychol. Gen. 2008, 137, 471–494. [Google Scholar] [CrossRef]
- Horne, R.S.C.; Ong, C.; Weichard, A.; Nixon, G.M.; Davey, M.J. Are there gender differences in the severity and consequences of sleep disordered in children? Sleep Med. 2020, 67, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Borges, J.G.; Ginani, G.E.; Hachul, H.; Cintra, F.D.; Tufik, S.; Pompeia, S. Executive functioning in obstructive sleep apnea syndrome patients without comorbidities: Focus on the fractionation of executive functions. J. Clin. Exp. Neuropsychol. 2013, 35, 1094–1107. [Google Scholar] [CrossRef]
- Itier, R.J.; Taylor, M.J. Face recognition memory and configural processing: A developmental ERP study using upright, inverted, and contrast-reversed faces. J. Cogn. Neurosci. 2004, 16, 487–502. [Google Scholar] [CrossRef]
- Alsubie, H.S.; BaHammam, A.S. Obstructive Sleep Apnoea: Children are not little Adults. Paediatr. Respir. Rev. 2017, 21, 72–79. [Google Scholar] [CrossRef]
- De Almondes, K.M.; Junior, F.; Leonardo, M.E.M.; Alves, N.T. Facial Emotion Recognition and Executive Functions in Insomnia Disorder: An Exploratory Study. Front. Psychol. 2020, 11, 502. [Google Scholar] [CrossRef]
- Hayes, G.S.; McLennan, S.N.; Henry, J.D.; Phillips, L.H.; Terrett, G.; Rendell, P.G.; Pelly, R.M.; Labuschagne, I. Task characteristics influence facial emotion recognition age-effects: A meta-analytic review. Psychol. Aging 2020, 35, 295–315. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Control | PS | Mild OSA | MSOSA | p Value |
|---|---|---|---|---|---|
| n = 20 | n = 51 | n = 39 | n = 26 | ||
| Gender (%) | 13M/7F | 34M/17F | 27M/12F | 17M/9F | 0.974 |
| Age (years) | 8.5 ± 1.8 | 8.4 ± 1.8 | 8.3 ± 1.7 | 8.6 ± 1.9 | 0.964 |
| BMI (kg/m2) | 17.5 ± 3.1 a | 17.5 ± 3.3 b | 17.8 ± 4.1 c | 20.8 ± 6.4 | 0.008 |
| BMI z-score | 0.92 ± 1.95 | 0.69 ± 1.19 | 0.85 ± 1.52 | 1.43 ± 1.75 | 0.225 |
| OAHI (events/hour) | 0.4 ± 0.3 a | 0.4 ± 0.2 b | 2.3 ± 1.0 c | 21.4 ± 36.1 | <0.001 |
| TST | 436.7 ± 61.2 | 430.9 ± 57.1 | 419.7 ± 58.6 | 414.8 ± 63.2 | 0.508 |
| ArI (events/hour) | 5.6 ± 1.6 a | 5.8 ± 1.9 b | 6.8 ± 2.4 c | 16.0 ± 13.4 | <0.001 |
| SpO2 nadir (%) | 92.8 ± 1.8 d | 93.2 ± 2.7 e | 91.6 ± 2.8 f | 87.4 ± 8.9 | <0.001 |
| Time with SpO2 < 90% | 0.00 ± 0.00 | 0.00 ± 0.00 | 0.01 ± 0.02 | 2.08 ± 9.13 | 0.129 |
| SDQ | |||||
| Emotional symptoms | 2.1 ± 2.0 | 2.4 ± 2.2 | 2.6 ± 2.4 | 2.8 ± 1.8 | 0.707 |
| Conduct problems | 1.2 ± 1.0 | 1.5 ± 1.4 | 1.5 ± 1.3 | 1.4 ± 0.7 | 0.778 |
| Hyperactivity | 2.8 ± 2.2 | 4.1 ± 2.5 | 4.0 ± 1.9 | 4.2 ± 1.9 | 0.106 |
| Peer problems | 1.7 ± 1.2 | 2.4 ± 1.6 | 2.4 ± 1.7 | 2.4 ± 1.4 | 0.292 |
| Prosocial behaviors | 8.4 ± 1.4 | 8.1 ± 2.0 | 7.9 ± 1.6 | 8.0 ± 1.6 | 0.796 |
| Control | PS | Mild OSA | MSOSA | |
|---|---|---|---|---|
| RTHappy (ms) | 505.23 ± 43.65 | 533.30 ± 27.33 | 554.59 ± 31.26 | 544.70 ± 38.28 |
| RTSad (ms) | 543.66 ± 47.52 | 602.17 ± 29.76 | 597.17 ± 34.03 | 568.23 ± 41.68 |
| ACCHappy (%) | 93.26 ± 1.14 | 93.19 ± 0.71 | 91.84 ± 0.81 | 93.11 ± 1.00 |
| ACCSad (%) | 93.13 ± 1.10 | 93.19 ± 0.65 | 91.95 ± 0.75 | 93.00 ± 0.92 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, F.-J.; Chen, Q.-W.; Wu, Y.; Xie, X.; Xu, Z.; Ni, X. Facial Emotion Recognition Deficit in Children with Moderate/Severe Obstructive Sleep Apnea. Brain Sci. 2022, 12, 1688. https://doi.org/10.3390/brainsci12121688
Zhao F-J, Chen Q-W, Wu Y, Xie X, Xu Z, Ni X. Facial Emotion Recognition Deficit in Children with Moderate/Severe Obstructive Sleep Apnea. Brain Sciences. 2022; 12(12):1688. https://doi.org/10.3390/brainsci12121688
Chicago/Turabian StyleZhao, Fu-Jun, Qing-Wei Chen, Yunxiao Wu, Xiaohong Xie, Zhifei Xu, and Xin Ni. 2022. "Facial Emotion Recognition Deficit in Children with Moderate/Severe Obstructive Sleep Apnea" Brain Sciences 12, no. 12: 1688. https://doi.org/10.3390/brainsci12121688