
Assessment of Executive and Cognitive Functions in Children with Restless Sleep Disorder: A Pilot Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Instruments
2.3. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hosker, D.K.; Elkins, R.M.; Potter, M.P. Promoting Mental Health and Wellness in Youth through Physical Activity, Nutrition, and Sleep. Child Adolesc. Psychiatr. Clin. N. Am. 2019, 28, 171–193. [Google Scholar] [CrossRef] [PubMed]
- Paruthi, S.; Brooks, L.J.; D’Ambrosio, C.; Hall, W.A.; Kotagal, S.; Lloyd, R.M.; Malow, B.A.; Maski, K.; Nichols, C.; Quan, S.F.; et al. Recommended Amount of Sleep for Pediatric Populations: A Consensus Statement of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2016, 12, 785–786. [Google Scholar] [CrossRef] [PubMed]
- Owens, J.A.; Weiss, M.R. Insufficient sleep in adolescents: Causes and consequences. Minerva Pediatr. 2017, 69, 326–336. [Google Scholar] [CrossRef] [PubMed]
- Sateia, M.J. International classification of sleep disorders-third edition: Highlights and modifications. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Ramos, A.R.; Tarraf, W.; Rundek, T.; Redline, S.; Wohlgemuth, W.K.; Loredo, J.S.; Sacco, R.L.; Lee, D.J.; Arens, R.; Lazalde, P.; et al. Obstructive sleep apnea and neurocognitive function in a Hispanic/Latino population. Neurology 2015, 84, 391–398. [Google Scholar] [CrossRef]
- Bucks, R.S.; Olaithe, M.; Eastwood, P. Neurocognitive function in obstructive sleep apnoea: A meta-review. Respirology 2013, 18, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Mouthon, A.L.; Huber, R. Methods in pediatric sleep research and sleep medicine. Neuropediatrics 2015, 46, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Owens, J.A.; Mindell, J.A. Pediatric sleep medicine: Priorities for research, patient care, policy and education. J. Clin. Sleep Med. 2006, 2, 77–88. [Google Scholar] [CrossRef]
- DelRosso, L.M.; Picchietti, D.L.; Spruyt, K.; Bruni, O.; Garcia-Borreguero, D.; Kotagal, S.; Owens, J.A.; Simakajornboon, N.; Ferri, R.; International Restless Legs Syndrome Study Group. Restless sleep in children: A systematic review. Sleep Med. Rev. 2021, 56, 101406. [Google Scholar] [CrossRef]
- Kothare, S.V.; Kaleyias, J. The clinical and laboratory assessment of the sleepy child. Semin. Pediatric Neurol. 2008, 15, 61–69. [Google Scholar] [CrossRef] [PubMed]
- DelRosso, L.M.; Jackson, C.V.; Trotter, K.; Bruni, O.; Ferri, R. Video-polysomnographic characterization of sleep movements in children with restless sleep disorder. Sleep 2019, 42, zsy269. [Google Scholar] [CrossRef] [PubMed]
- DelRosso, L.M.; Bruni, O.; Ferri, R. Restless sleep disorder in children: A pilot study on a tentative new diagnostic category. Sleep 2018, 41, zsy102. [Google Scholar] [CrossRef] [PubMed]
- DelRosso, L.M.; Mogavero, M.P.; Ferri, R. Restless sleep disorder, restless legs syndrome, and periodic limb movement disorder-Sleep in motion! Pediatr. Pulmonol. 2022, 57, 1879–1886. [Google Scholar] [CrossRef] [PubMed]
- DelRosso, L.M.; Ferri, R. The prevalence of restless sleep disorder among a clinical sample of children and adolescents referred to a sleep centre. J. Sleep Res. 2019, 28, e12870. [Google Scholar] [CrossRef]
- DelRosso, L.M.; Hartmann, S.; Baumert, M.; Bruni, O.; Ruth, C.; Ferri, R. Non-REM sleep instability in children with restless sleep disorder. Sleep Med. 2020, 75, 276–281. [Google Scholar] [CrossRef]
- DelRosso, L.M.; Bruni, O.; Ferri, R. Heart rate variability during sleep in children and adolescents with restless sleep disorder: A comparison with restless legs syndrome and normal controls. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2020, 16, 1883–1890. [Google Scholar] [CrossRef] [PubMed]
- DelRosso, L.M.; Picchietti, D.L.; Ferri, R. Comparison between oral ferrous sulfate and intravenous ferric carboxymaltose in children with restless sleep disorder. Sleep 2021, 44, zsaa155. [Google Scholar] [CrossRef] [PubMed]
- Johannsdottir, K.R.; Ferretti, D.; Arnadottir, B.S.; Jonsdottir, M.K. Objective Measures of Cognitive Performance in Sleep Disorder Research. Sleep Med. Clin. 2021, 16, 575–593. [Google Scholar] [CrossRef]
- Macchitella, L.; Romano, D.L.; Marinelli, C.V.; Toraldo, D.M.; Arigliani, M.; De Benedetto, M.; Angelelli, P. Neuropsychological and socio-cognitive deficits in patients with obstructive sleep apnea. J. Clin. Exp. Neuropsychol. 2021, 43, 514–533. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, F.I.; Bosco, P.; Drago, V.; Prestianni, G.; Lanuzza, B.; Iero, I.; Tripodi, M.; Spada, R.S.; Toscano, G.; Caraci, F.; et al. The APOE epsilon4 allele increases the risk of impaired spatial working memory in obstructive sleep apnea. Sleep Med. 2008, 9, 831–839. [Google Scholar] [CrossRef] [PubMed]
- da Silva Gusmao Cardoso, T.; Pompeia, S.; Miranda, M.C. Cognitive and behavioral effects of obstructive sleep apnea syndrome in children: A systematic literature review. Sleep Med. 2018, 46, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [PubMed]
- Cristofori, I.; Cohen-Zimerman, S.; Grafman, J. Executive functions. Handb. Clin. Neurol. 2019, 163, 197–219. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Luo, H.; Liu, H.; Hou, J.; Feng, Y.; Chen, J.; Xing, L.; Ren, X. Related biomarkers of neurocognitive impairment in children with obstructive sleep apnea. Int. J. Pediatr. Otorhinolaryngol. 2019, 116, 38–42. [Google Scholar] [CrossRef]
- Krysta, K.; Bratek, A.; Zawada, K.; Stepanczak, R. Cognitive deficits in adults with obstructive sleep apnea compared to children and adolescents. J. Neural. Transm. 2017, 124, 187–201. [Google Scholar] [CrossRef]
- Joyce, A.; Elphick, H.; Farquhar, M.; Gringras, P.; Evans, H.; Bucks, R.S.; Kreppner, J.; Kingshott, R.; Martin, J.; Reynolds, J.; et al. Obstructive Sleep Apnoea Contributes to Executive Function Impairment in Young Children with Down Syndrome. Behav. Sleep Med. 2020, 18, 611–621. [Google Scholar] [CrossRef]
- DelRosso, L.M.; Ferri, R.; Allen, R.P.; Bruni, O.; Garcia-Borreguero, D.; Kotagal, S.; Owens, J.A.; Peirano, P.; Simakajornboon, N.; Picchietti, D.L.; et al. Consensus diagnostic criteria for a newly defined pediatric sleep disorder: Restless sleep disorder (RSD). Sleep Med. 2020, 75, 335–340. [Google Scholar] [CrossRef]
- Berry, R.B.; Brooks, R.; Gamaldo, C.; Harding, S.M.; Lloyd, R.M.; Quan, S.F.; Troester, M.T.; Vaughn, B.V. AASM Scoring Manual Version 2.6; American Academy of Sleep Medicine: Darien, IL, USA, 2019. [Google Scholar]
- Ferri, R.; DelRosso, L.M.; Provini, F.; Stefani, A.; Walters, A.S.; Picchietti, D.L. Scoring of large muscle group movements during sleep: An International Restless Legs Syndrome Study Group position statement. Sleep 2021, 44, zsab092. [Google Scholar] [CrossRef]
- Akshoomoff, N.; Newman, E.; Thompson, W.K.; McCabe, C.; Bloss, C.S.; Chang, L.; Amaral, D.G.; Casey, B.J.; Ernst, T.M.; Frazier, J.A.; et al. The NIH Toolbox Cognition Battery: Results from a large normative developmental sample (PING). Neuropsychology 2014, 28, 1–10. [Google Scholar] [CrossRef]
- Zelazo, P.D. The Dimensional Change Card Sort (DCCS): A method of assessing executive function in children. Nat. Protoc. 2006, 1, 297–301. [Google Scholar] [CrossRef]
- Bauer, P.J.; Dikmen, S.S.; Heaton, R.K.; Mungas, D.; Slotkin, J.; Beaumont, J.L. III. NIH Toolbox Cognition Battery (CB): Measuring episodic memory. Monogr. Soc. Res. Child. Dev. 2013, 78, 34–48. [Google Scholar] [CrossRef] [PubMed]
- Isaiah, A.; Ernst, T.; Cloak, C.C.; Clark, D.B.; Chang, L. Association Between Habitual Snoring and Cognitive Performance Among a Large Sample of Preadolescent Children. JAMA Otolaryngol. Head Neck Surg. 2021, 147, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Solomon, M.; Gordon, A.; Iosif, A.M.; Geddert, R.; Krug, M.K.; Mundy, P.; Hessl, D. Using the NIH Toolbox to Assess Cognition in Adolescents and Young Adults with Autism Spectrum Disorders. Autism. Res. 2021, 14, 500–511. [Google Scholar] [CrossRef] [PubMed]
- Haigh, S.M.; Walsh, J.A.; Mazefsky, C.A.; Minshew, N.J.; Eack, S.M. Processing Speed is Impaired in Adults with Autism Spectrum Disorder, and Relates to Social Communication Abilities. J. Autism. Dev. Disord. 2018, 48, 2653–2662. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, C.; Soleimani, M.; Carroll, A.; Hodlevskyy, O. Neuropsychological functioning in children with Tourette syndrome (TS). J. Can. Acad. Child. Adolesc. Psychiatry 2009, 18, 307–315. [Google Scholar]
- Chervin, R.D.; Ruzicka, D.L.; Giordani, B.J.; Weatherly, R.A.; Dillon, J.E.; Hodges, E.K.; Marcus, C.L.; Guire, K.E. Sleep-disordered breathing, behavior, and cognition in children before and after adenotonsillectomy. Pediatrics 2006, 117, e769–e778. [Google Scholar] [CrossRef]
- Brodeur, D.A.; Pond, M. The development of selective attention in children with attention deficit hyperactivity disorder. J. Abnorm. Child. Psychol. 2001, 29, 229–239. [Google Scholar] [CrossRef]
- Posner, M.I.; Driver, J. The neurobiology of selective attention. Curr. Opin. Neurobiol. 1992, 2, 165–169. [Google Scholar] [CrossRef]
- Corbetta, M.; Miezin, F.M.; Shulman, G.L.; Petersen, S.E. Selective attention modulates extrastriate visual regions in humans during visual feature discrimination and recognition. Ciba Found. Symp. 1991, 163, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Muto, V.; Shaffii-le Bourdiec, A.; Matarazzo, L.; Foret, A.; Mascetti, L.; Jaspar, M.; Vandewalle, G.; Phillips, C.; Degueldre, C.; Balteau, E.; et al. Influence of acute sleep loss on the neural correlates of alerting, orientating and executive attention components. J. Sleep Res. 2012, 21, 648–658. [Google Scholar] [CrossRef] [PubMed]
- Fisk, A.S.; Tam, S.K.E.; Brown, L.A.; Vyazovskiy, V.V.; Bannerman, D.M.; Peirson, S.N. Light and Cognition: Roles for Circadian Rhythms, Sleep, and Arousal. Front. Neurol. 2018, 9, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Short, M.A.; Gradisar, M.; Lack, L.C.; Wright, H.R. The impact of sleep on adolescent depressed mood, alertness and academic performance. J. Adolesc. 2013, 36, 1025–1033. [Google Scholar] [CrossRef] [PubMed]
- Killgore, W.D. Effects of sleep deprivation on cognition. Prog. Brain Res. 2010, 185, 105–129. [Google Scholar] [CrossRef] [PubMed]
- Durmer, J.S.; Dinges, D.F. Neurocognitive consequences of sleep deprivation. Semin. Neurol. 2005, 25, 117–129. [Google Scholar] [CrossRef]
- Knight, F.L.C.; Dimitriou, D. Poor Sleep Has Negative Implications for Children with and without ADHD, but in Different Ways. Behav. Sleep Med. 2019, 17, 423–436. [Google Scholar] [CrossRef] [PubMed]
- Ferri, R.; Huber, R.; Arico, D.; Drago, V.; Rundo, F.; Ghilardi, M.F.; Massimini, M.; Tononi, G. The slow-wave components of the cyclic alternating pattern (CAP) have a role in sleep-related learning processes. Neurosci. Lett. 2008, 432, 228–231. [Google Scholar] [CrossRef] [PubMed]
- Ferri, R.; Drago, V.; Arico, D.; Bruni, O.; Remington, R.D.; Stamatakis, K.; Punjabi, N.M. The effects of experimental sleep fragmentation on cognitive processing. Sleep Med. 2010, 11, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Arico, D.; Drago, V.; Foster, P.S.; Heilman, K.M.; Williamson, J.; Ferri, R. Effects of NREM sleep instability on cognitive processing. Sleep Med. 2010, 11, 791–798. [Google Scholar] [CrossRef]
- Fulda, S.; Beitinger, M.E.; Reppermund, S.; Winkelmann, J.; Wetter, T.C. Short-term attention and verbal fluency is decreased in restless legs syndrome patients. Mov. Disord. Off. J. Mov. Disord. Soc. 2010, 25, 2641–2648. [Google Scholar] [CrossRef]
- Pearson, V.E.; Allen, R.P.; Dean, T.; Gamaldo, C.E.; Lesage, S.R.; Earley, C.J. Cognitive deficits associated with restless legs syndrome (RLS). Sleep Med. 2006, 7, 25–30. [Google Scholar] [CrossRef]
- Driver-Dunckley, E.; Connor, D.; Hentz, J.; Sabbagh, M.; Silverberg, N.; Hernandez, J.; Vedders, L.; Evidente, V.G.; Shill, H.; Caviness, J.; et al. No evidence for cognitive dysfunction or depression in patients with mild restless legs syndrome. Mov. Disord. Off. J. Mov. Disord. Soc. 2009, 24, 1840–1842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blair, C. Educating executive function. Wiley Interdiscip. Rev. Cogn. Sci. 2017, 8, e1403. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
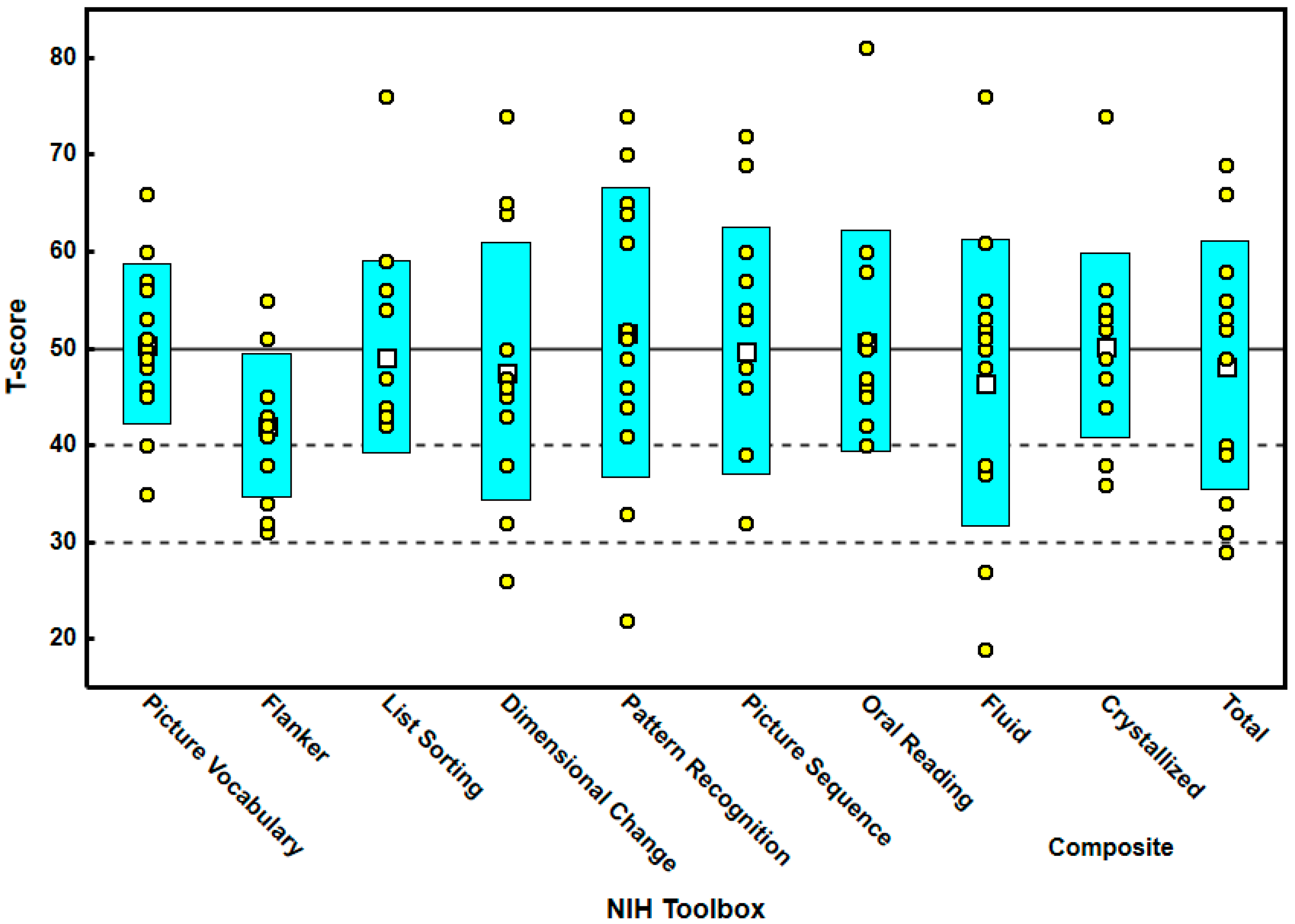
| Min | Max | Mean | S.D. | |
|---|---|---|---|---|
| Picture vocabulary | 32 | 66 | 50.23 | 8.757 |
| Flanker | 31 | 55 | 42.08 | 7.331 |
| List sorting | 42 | 76 | 48.77 | 9.808 |
| Dimensional change | 26 | 74 | 47.92 | 13.131 |
| Pattern recognition | 22 | 74 | 51.85 | 14.781 |
| Picture sequence | 31 | 72 | 49.92 | 12.939 |
| Oral reading | 40 | 81 | 50.85 | 11.371 |
| Composite fluid | 19 | 76 | 46.46 | 14.858 |
| Composite crystallized | 36 | 74 | 50.31 | 9.517 |
| Composite cognitive | 29 | 69 | 48.23 | 12.788 |
| T-Score ≤ 50 | T-Score > 50 | Chi-Squared | p = | Effect Size φ | |
|---|---|---|---|---|---|
| Picture vocabulary | 7 | 6 | 0.07 | 0.791 | 0.019 |
| Flanker | 10 | 3 | 3.35 | 0.067 | 0.929 |
| List sorting | 9 | 4 | 1.71 | 0.191 | 0.474 |
| Dimensional change | 10 | 3 | 3.35 | 0.067 | 0.929 |
| Pattern recognition | 6 | 7 | 0.07 | 0.791 | 0.019 |
| Picture sequence | 7 | 6 | 0.07 | 0.791 | 0.019 |
| Oral reading | 8 | 5 | 0.61 | 0.435 | 0.169 |
| Composite fluid | 7 | 6 | 0.07 | 0.791 | 0.019 |
| Composite crystallized | 6 | 7 | 0.07 | 0.791 | 0.019 |
| Composite cognitive | 6 | 7 | 0.07 | 0.791 | 0.019 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
DelRosso, L.M.; Vega-Flores, G.; Ferri, R.; Mogavero, M.P.; Diamond, A. Assessment of Executive and Cognitive Functions in Children with Restless Sleep Disorder: A Pilot Study. Brain Sci. 2022, 12, 1289. https://doi.org/10.3390/brainsci12101289
DelRosso LM, Vega-Flores G, Ferri R, Mogavero MP, Diamond A. Assessment of Executive and Cognitive Functions in Children with Restless Sleep Disorder: A Pilot Study. Brain Sciences. 2022; 12(10):1289. https://doi.org/10.3390/brainsci12101289
Chicago/Turabian StyleDelRosso, Lourdes M., German Vega-Flores, Raffaele Ferri, Maria P. Mogavero, and Adele Diamond. 2022. "Assessment of Executive and Cognitive Functions in Children with Restless Sleep Disorder: A Pilot Study" Brain Sciences 12, no. 10: 1289. https://doi.org/10.3390/brainsci12101289