
A Qualitative Assessment among Personnel Working in Community-Led Development Program Settings Regarding Sexualized Substance Use

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
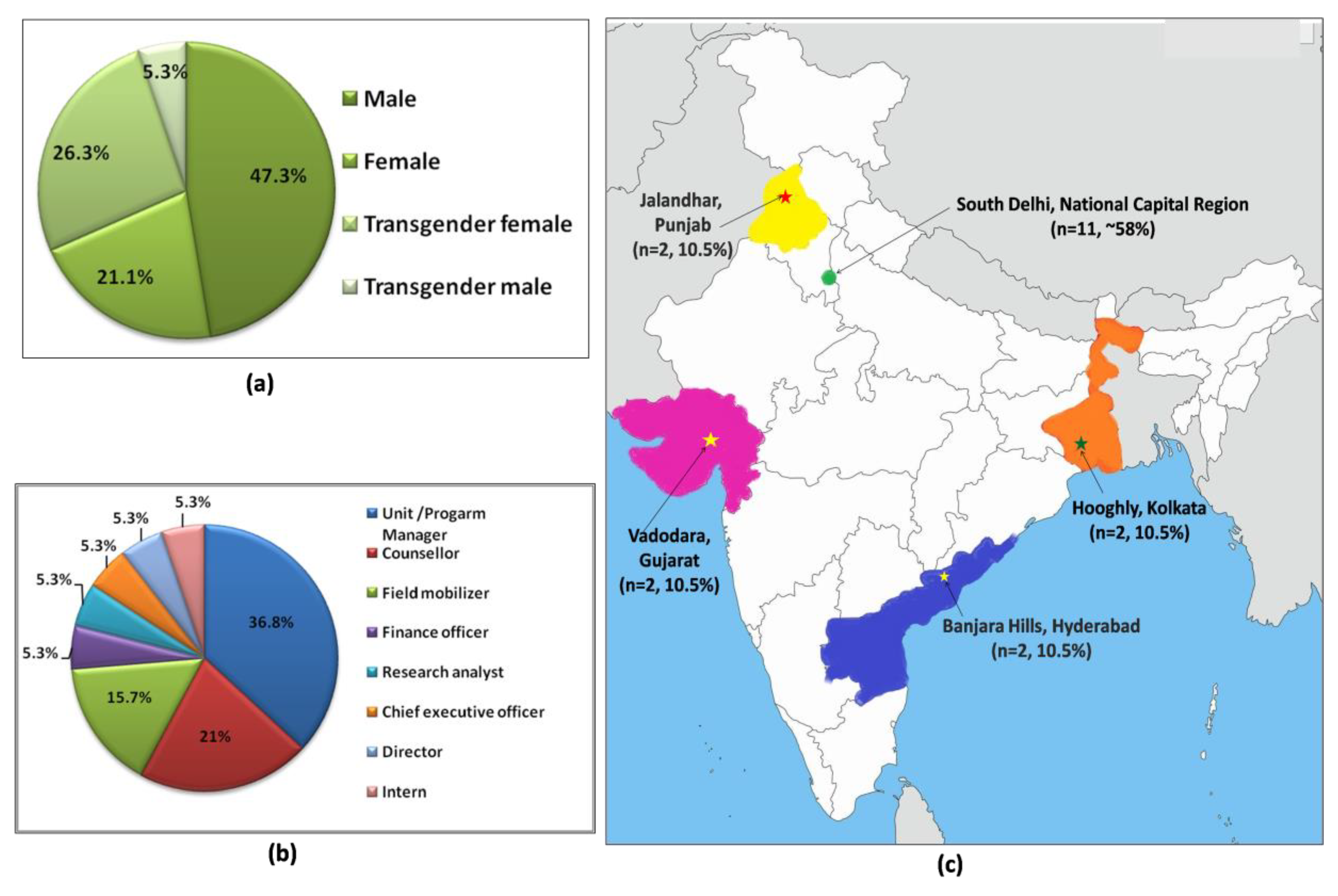
2.1. Study Site
2.2. Study Design and Gaining Access to the Study Subjects
2.3. Participants and Eligibility Criteria
2.4. Data Collection Tool
2.5. Data Analysis
3. Results
3.1. Participant Demographics
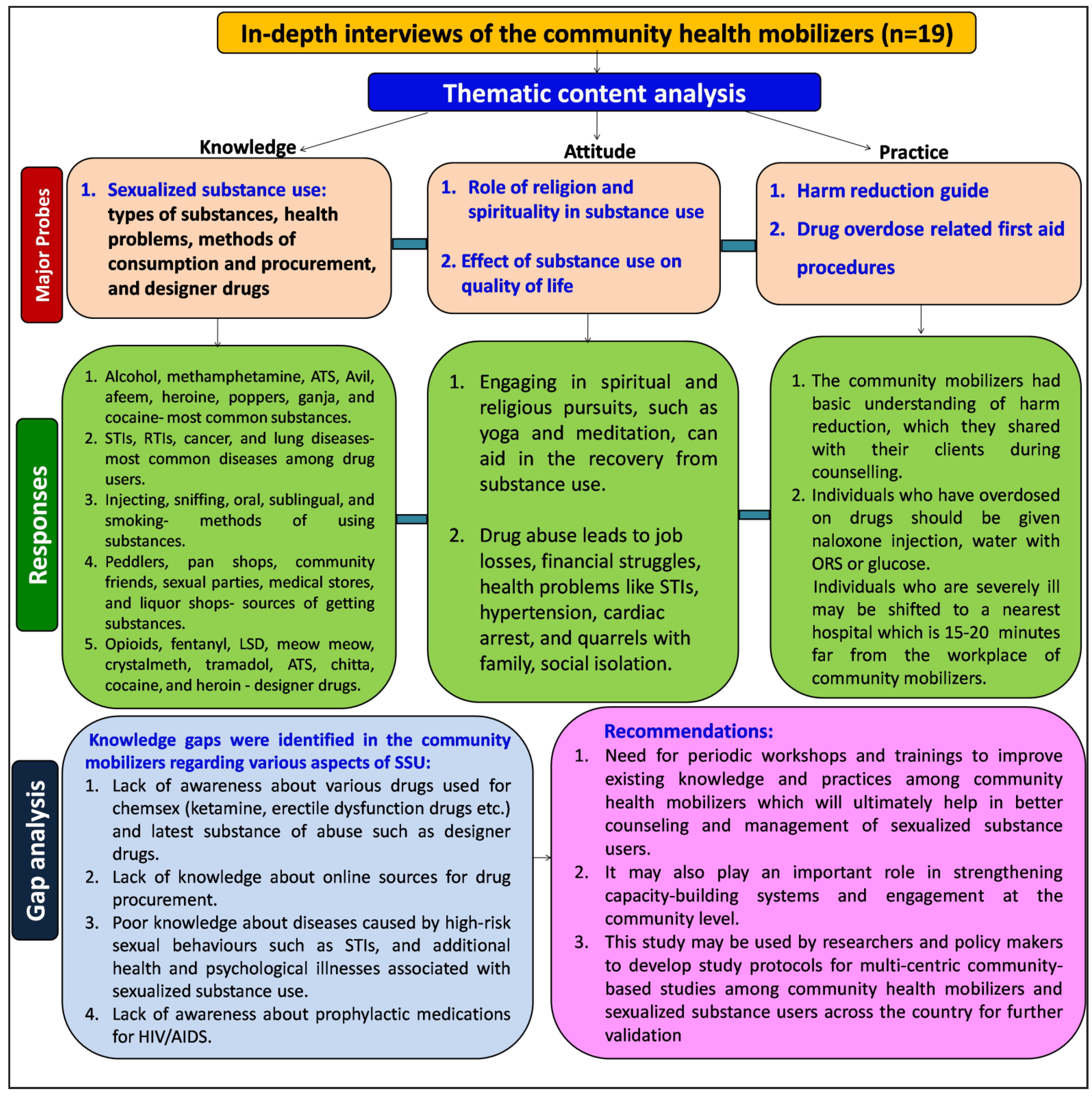
3.2. Thematic Content Analysis
3.2.1. Participants’ Response to Knowledge-Assessment Probes
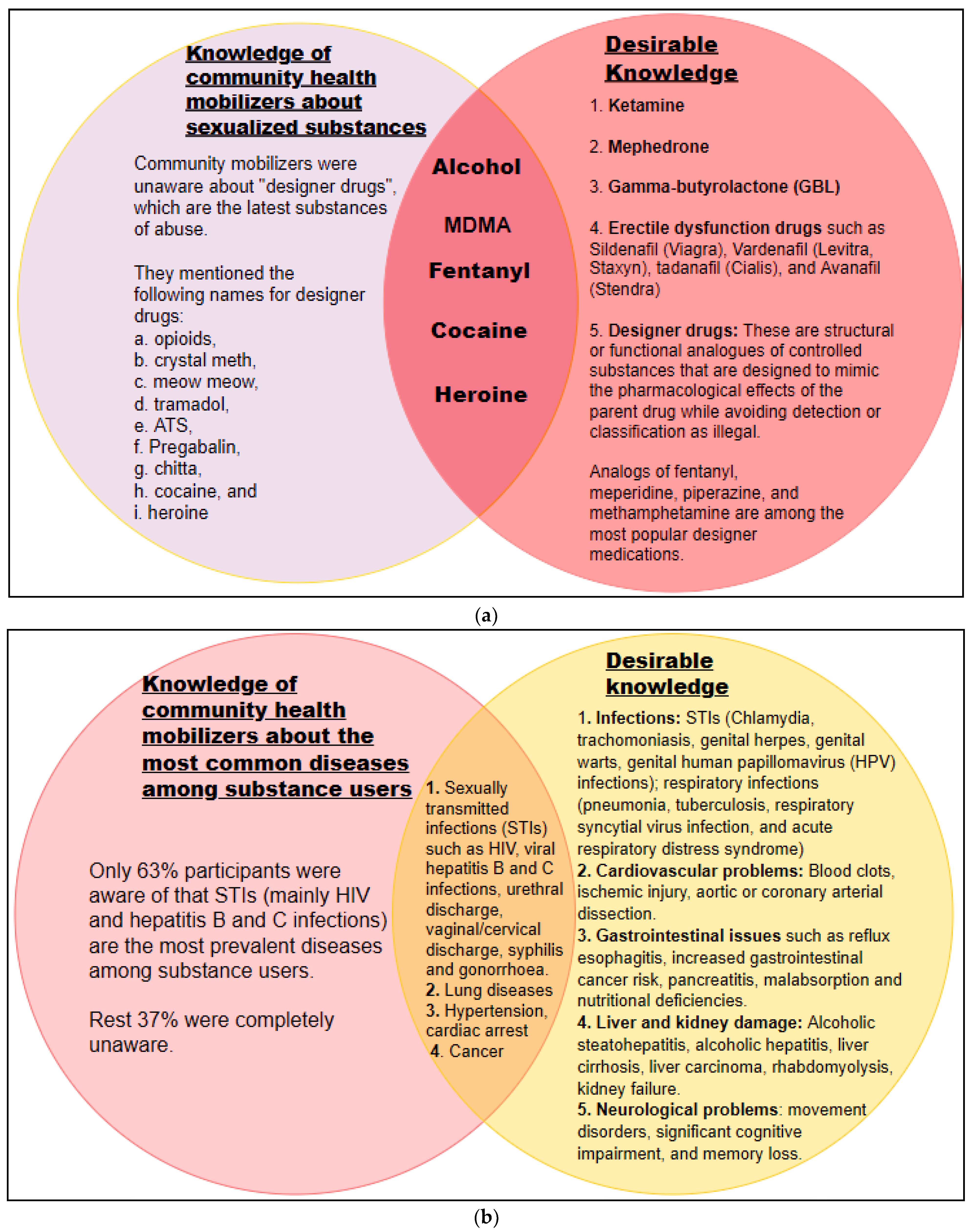
Sexualized Substance Use
Prophylaxis
Drug Overdose Related Complications
Relapse to Addiction
“People suffer from withdrawal syndrome after quitting drugs and so start abusing drugs again”—Bharat (CBO3)
“Stress, peer pressure, and sex pleasure are some of the major triggers for relapse”—Vicky (CBO2)
“Relationship, problems in family, office pressure, bullying in college, mind distraction are some of the reasons people start taking drugs again”—Shaurya (CBO4)
Work Challenges
“Legal barriers not faced till date…. but dealt with structural stigma, people stigma, social stigma, and self-stigma”—Sunil (CBO1)
“Sometimes police says that we are involved in substance sale”—Piku (CBO14)
“People usually start taking drugs out of curiosity, for enhancing sexual pleasure…. some people do drugs for countering their inhibition, to overcome their guilt feeling, some people do it just for fun”—Bharat (CBO3)
“Common reasons which I have heard for doing drugs are to overcome depression after breakup …...People with high ambition take drugs to relieve stress and workload”—Barkha (CBO17)
“First reason, people feel good after taking drugs, next they want to reduce their anxiety, and depression…. but it’s vice versa, like people who take drugs become prone to anxiety and depression because they lose their jobs, and their personal lives get jeopardized…. Genetics, and environment also contribute for drug abuse like peer group, hang out places etc”—Sunil (CBO1)
“The reasons which I have heard from my clients are that…they lack confidence for doing sex with same sex…there is lack of confidence for standing on road for sexwork…some people take substance because they have entered to sex orgy parties”—Piku (CBO14)
Work Experience
3.2.2. Participants’ Response to Attitude-Assessment Probes
Role of Religion and Spirituality
“Yes, most of the users go to quacks or ojhas (person who practice black magic)”—Ujjwal (CBO9)
“If we can start meditation through spirituality, this will help to cope up from substance…some people go for meditation…some people start using if they get connected to religious group like religious akhada”—Piku (CBO14)
“Sometimes it is possible but not always…. depends on client mental status”—Mayur (CBO6)
“Many religion and spirituality things play a role in Punjab”—Bobby (CBO15)
Effect of Substance Use on Quality of Life
“Due to substance use, most of the time he/she lose job, they don’t feel seriousness about his/her lives…usually they lead their life very messy and most of time they don’t use condoms while engaging in sex work”—Sunil (CBO1)
3.2.3. Participants’ Response to Practice-Assessment Probes
Harm Reduction
First-Aid for Drug Overdose
“In the event of a drug overdose, we first provide ABC therapy, second we call an ambulance, if we have naloxone injection then we give 2 mL dose to the patient and take him to the nearest hospital”—Bobby (CBO15)
“We take the drug overdosed patients to the nearest government set up which is almost 20 min from our organization”—Bharat (CBO3)
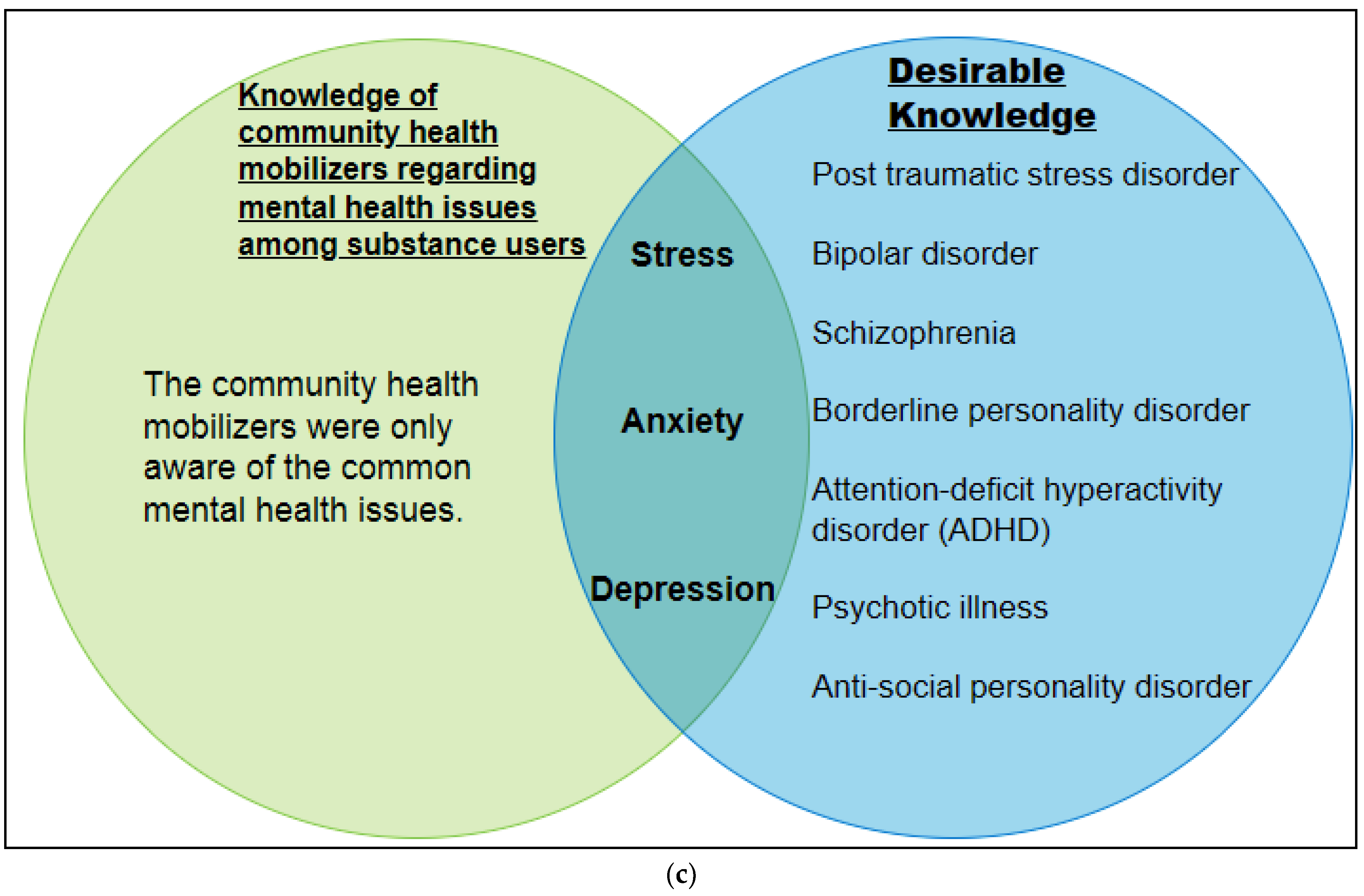
3.3. Gap Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tomkins, A.; George, R.; Kliner, M. Sexualised drug taking among men who have sex with men: A systematic review. Perspect. Public Health 2019, 139, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Chou, L.W.; Chang, K.M.; Puspitasari, I. Drug Abuse Research Trend Investigation with Text Mining. Comput. Math. Methods Med. 2020, 2020, 1030815. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar] [CrossRef]
- Compton, W.M.; Jones, C.M. Substance Use among Men Who Have Sex with Men. N. Engl. J. Med. 2021, 385, 352–356. [Google Scholar] [CrossRef]
- Wenz, B.; the DRUCK Study group; Nielsen, S.; Gassowski, M.; Santos-Hövener, C.; Cai, W.; Ross, R.S.; Bock, C.-T.; Ratsch, B.-A.; Kücherer, C.; et al. High variability of HIV and HCV seroprevalence and risk behaviours among people who inject drugs: Results from a cross-sectional study using respondent-driven sampling in eight German cities (2011–14). BMC Public Health 2016, 16, 927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chettiar, J.; Shannon, K.; Wood, E.; Zhang, R.; Kerr, T. Survival sex work involvement among street-involved youth who use drugs in a Canadian setting. J. Public Health 2010, 32, 322–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luethi, D.; Liechti, M.E. Designer drugs: Mechanism of action and adverse effects [published correction appears in Arch Toxicol. Arch. Toxicol. 2020, 94, 1085–1133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Substance Abuse and Mental Health Services Administration (SAMHSA). National Survey of Substance Abuse Treatment Services (N-SSATS): 2013. Data on Substance Abuse Treatment Facilities; No. (SMA) 14-489, BHSIS Series S-73; HHS Publication: Rockville, MD, USA, 2014. [Google Scholar]
- Hoyumpa, A.M. Mechanisms of vitamin deficiencies in alcoholism. Alcohol. Clin. Exp. Res. 1986, 10, 573–581. [Google Scholar] [CrossRef] [PubMed]
- NIDA. Drug Use and Viral Infections (HIV, Hepatitis) Drug Facts. National Institute on Drug Abuse Website. Available online: https://nida.nih.gov/publications/drugfacts/drug-use-viral-infections-hiv-hepatitis (accessed on 30 October 2022).
- Centers for Disease Control and Prevention (CDC). HIV and Injection Drug Use. 2017. Available online: https://www.cdc.gov/hiv/risk/idu.html (accessed on 8 February 2018).
- Degenhardt, L.; A Whiteford, H.; Ferrari, A.J.; Baxter, A.J.; Charlson, F.J.; Hall, W.D.; Freedman, G.; Burstein, R.; Johns, N.; E Engell, R.; et al. Global burden of disease attributable to illicit drug use and dependence: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 382, 1564–1574. [Google Scholar] [CrossRef]
- Volkow, N.D.; Baler, R.D.; Normand, J.L. The unrealized potential of addiction science in curbing the HIV epidemic. Curr. HIV Res. 2011, 9, 393–395. [Google Scholar] [CrossRef]
- Dash, S.; Balasubramaniam, M.; Villalta, F.; Dash, C.; Pandhare, J. Impact of cocaine abuse on HIV pathogenesis. Front. Microbiol. 2015, 6, 1111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, A.N.C.; Tross, S.; Caslyn, D.A. Substance Use Disorders and HIV/AIDS Prevention and Treatment Intervention: Research and Practice Considerations. Soc. Work Public Health 2013, 28, 333–348. [Google Scholar] [CrossRef]
- González-Baeza, A.; Dolengevich-Segal, H.; Valero, I.P.; Cabello, A.; Téllez, M.J.; Sanz, J.; Pérez-Latorre, L.; Bernardino, J.I.; Troya, J.; De La Fuente, S.; et al. Sexualized Drug Use (Chemsex) Is Associated with High-Risk Sexual Behaviors and Sexually Transmitted Infections in HIV-Positive Men Who Have Sex with Men: Data from the U-SEX GESIDA 9416 Study. AIDS Patient Care STDS 2018, 32, 112–118. [Google Scholar] [CrossRef]
- Reback, C.J.; Fletcher, J.B. HIV prevalence, substance use, and sexual risk behaviors among transgender women recruited through outreach. AIDS Behav. 2014, 18, 1359–1367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Amico, E.J.; Rodriguez, A.; Dunbar, M.S.; Firth, C.L.; Tucker, J.S.; Seelam, R.; Pedersen, E.R.; Davis, J.P. Sources of cannabis among young adults and associations with cannabis-related outcomes. Int. J. Drug Policy 2020, 86, 102971. [Google Scholar] [CrossRef] [PubMed]
- McCabe, S.E.; Veliz, P.; Wilens, T.E.; West, B.T.; Schepis, T.; Ford, J.; Pomykacz, C.; Boyd, C. Sources of Nonmedical Prescription Drug Misuse Among US High School Seniors: Differences in Motives and Substance Use Behaviors. J. Am. Acad. Child Adolesc. Psychiatry 2019, 58, 681–691. [Google Scholar] [CrossRef] [PubMed]
- Grau-López, L.; Roncero, C.; Daigre, C.; Gonzalvo, B.; Bachiller, D.; Rodriguez-Cintas, L.; Egido, Á.; Casas, M. Factores de riesgo de recaída en pacientes drogodependientes tras desintoxicación hospitalaria (Riskfactorsfor relapse in drug-dependent patients after hospital detoxification). Adicciones 2012, 24, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Manini, A.F.; Nelson, L.S.; Stimmel, B.; Vlahov, D.; Hoffman, R.S. Incidence of adverse cardiovascular events in adults following drug overdose. Acad. Emerg. Med. 2012, 19, 843–849. [Google Scholar] [CrossRef] [Green Version]
- Campleman, S.L.; Brent, J.; Pizon, A.F.; Shulman, J.; Wax, P.; Manini, A.F. Toxicology Investigators’ Consortium (ToxIC). Drug-specific risk of severe QT prolongation following acute drug overdose. Clin. Toxicol. 2020, 58, 1326–1334. [Google Scholar] [CrossRef]
- Jones, A.L.; Rankin, J.A.; Then, K.L. Drug Overdose, Loss of Consciousness, and Compartment Syndrome: A Life-Threatening Combination. J. Emerg. Nurs. 2020, 46, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Muller, A.E.; Skurtveit, S.; Clausen, T. Many correlates of poor quality of life among substance users entering treatment are not addiction specific. Health Qual. Life Outcomes 2016, 14, 39. [Google Scholar] [CrossRef] [Green Version]
- Laudet, A.B. The case for considering quality of life in addiction research and clinical practice. Addict. Sci. Clin. Pr. 2011, 6, 44–55. [Google Scholar]
- Frisch, M.B.; Cornell, J.; Villanueva, M.; Retzlaff, P.J. Clinical validation of the Quality-of-Life Inventory. A measure of life satisfaction for use in treatment planning and outcome assessment. Psychol. Assess. 1992, 4, 92–101. [Google Scholar] [CrossRef]
- Foster, J.H.; Powell, J.E.; Marshall, E.J.; Peters, T.J. Quality of Life in alcohol-dependent subjects—A review. Qual. Life Res. 1999, 8, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Hawk, M.; Coulter, R.W.S.; Egan, J.E.; Fisk, S.; Friedman, M.R.; Tula, M.; Kinsky, S. Harm reduction principles for healthcare settings. Harm Reduct. J. 2017, 14, 70. [Google Scholar] [CrossRef] [Green Version]
- Walley, A.Y.; Xuan, Z.; Hackman, H.H.; Quinn, E.; Doe-Simkins, M.; Sorensen-Alawad, A.; Ruiz, S.; Ozonoff, A. Opioid overdose rates and implementation of overdose education and nasal naloxone distribution in Massachusetts: Interrupted time series analysis. BMJ 2013, 346, f174. [Google Scholar] [CrossRef] [Green Version]
- Krieger, M.; Goedel, W.; Buxton, J.A.; Lysyshyn, M.; Bernstein, E.; Sherman, S.G.; Rich, J.D.; Hadland, S.E.; Green, T.C.; Marshall, B.D. Use of rapid fentanyl test strips among young adults who use drugs. Int. J. Drug Policy 2018, 61, 52–58. [Google Scholar] [CrossRef]
- Covington, S. Working with substance abusing mothers: A trauma-informed, gender-responsive approach. Source 2007, 16, 1–11. [Google Scholar]
- Ducharme, L.J.; Mello, H.L.; Roman, P.M.; Knudsen, H.K.; Johnson, A.J. Service delivery in substance abuse treatment: Reexamining “comprehensive” care. J. Behav. Health Serv. Res. 2007, 34, 121–136. [Google Scholar] [CrossRef] [Green Version]
- McNulty, T.; Oser, C.; Johnson, J.A.; Knudsen, H.; Roman, P. Counselor turnover in substance abuse treatment centers: An organizational-level analysis. Sociol. Inq. 2007, 77, 166–193. [Google Scholar] [CrossRef]
- Shoptaw, S.; Stein, J.A.; Rawson, R.A. Burnout in substance abuse counselors: Impact of environment, attitudes, and clients with HIV. J. Subst. Abus. Treat. 2000, 19, 117–126. [Google Scholar] [CrossRef]
- Donnadieu-Rigole, H.; Peyrière, H.; Benyamina, A.; Karila, L. Complications Related to Sexualized Drug Use: What Can We Learn from Literature? Front. Neurosci. 2020, 14, 548704. [Google Scholar] [CrossRef]
- Coppola, M.; Mondola, R. Synthetic cathinones: Chemistry, pharmacology, and toxicology of a new class of designer drugs of abuse marketed as “bath salts” or “plant food”. Toxicol. Lett. 2012, 211, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Petit, A.; Karila, L.; Sananes, M.; Lejoyeux, M. La méphédrone: Une nouvelle drogue de synthèse Mephedrone: A new syntheticdrug. Presse Méd. 2013, 42, 1310–1316. [Google Scholar] [CrossRef] [PubMed]
- Grov, C.; Breslow, A.S.; Newcomb, M.E.; Rosenberger, J.G.; Bauermeister, J.A. Gay and bisexual men’s use of the Internet: Research from the 1990s through 2013. J. Sex Res. 2014, 51, 390–409. [Google Scholar] [CrossRef]
- Lewnard, J.A.; Berrang-Ford, L. Internet-based partner selection and risk for unprotected anal intercourse in sexual encounters among men who have sex with men: A meta-analysis of observational studies. Sex. Transm. Infect. 2014, 90, 290–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitfield, D.L.; Kattari, S.K.; Walls, N.E.; Al-Tayyib, A. Grindr, Scruff, and on the Hunt: Predictors of Condomless Anal Sex, Internet Use, and Mobile Application Use Among Men Who Have Sex with Men. Am. J. Men’s Health 2017, 11, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Heinsbroek, E.; Glass, R.; Edmundson, C.; Hope, V.; Desai, M. Patterns of injecting and non-injecting drug use by sexual behaviour in people who inject drugs attending services in England, Wales and Northern Ireland, 2013–2016. Int. J. Drug Policy 2018, 55, 215–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spiller, H.A.; Ryan, M.L.; Weston, R.G.; Jansen, J. Clinical experience with and analytical confirmation of “bath salts” and “legal highs” (synthetic cathinones) in the United States. Clin. Toxicol. 2011, 49, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Pereira, F.R.; McMaster, M.T.B.; Schellekens, A.; Polderman, N.; De Vries, Y.D.A.T.; Brink, W.V.D.; van Wingen, G. Effects of Recreational GHB Use and Multiple GHB-Induced Comas on Brain Structure and Impulsivity. Front. Psychiatry 2020, 11, 166. [Google Scholar] [CrossRef] [Green Version]
- Morgan, C.J.; Curran, H.V. Independent Scientific Committee on Drugs. Ketamine use: A review. Addiction 2012, 107, 27–38. [Google Scholar] [CrossRef]
- Elliott, T.; Sanders, E.J.; Doherty, M.; Ndung′U, T.; Cohen, M.; Patel, P.; Cairns, G.; E Rutstein, S.; Ananworanich, J.; Brown, C.; et al. Challenges of HIV diagnosis and management in the context of pre-exposure prophylaxis (PrEP), post-exposure prophylaxis (PEP), test and start and acute HIV infection: A scoping review. J. Int. AIDS Soc. 2019, 22, e25419. [Google Scholar] [CrossRef] [PubMed]
- Elliott, T.; Sanders, E.J.; Doherty, M.; Ndung′U, T.; Cohen, M.; Patel, P.; Cairns, G.; E Rutstein, S.; Ananworanich, J.; Brown, C.; et al. Structural competency: Curriculum for medical students, residents, and interprofessional teams on the structural factors that produce health disparities. MedEdPORTAL 2020, 16, 10888. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Domains | Enquiries | Probes |
|---|---|---|
| Sexualized substance use | What do you know about SSU? | Types of substances, recent substances of abuse such as designer drugs, methods of consumption and procurement, diseases, and infections |
| Prophylaxis | What do you know about prophylaxis for HIV/STI? | Pre-exposure prophylaxis (PrEP) and post-exposure prophylaxis (PEP) |
| Drug overdose related complications and first-aid procedures | How do you manage in case of drug overdose? | Symptoms of drug overdose, harm reduction, possible ways of getting services |
| Relapse to addiction | What do you know about relapse after deaddiction? | Rates of relapse, possible triggers |
| Work challenges | Would you like to share the problems you have faced while working with substance users? | Stigma, discrimination, legal challenges |
| Work experience | Would you like to share your various experiences working with substance users? | Age group, relationship with family members, role of religion and spirituality, effect on quality of life |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marik, B.; Mahajan, N.; Sarkar, R.; Mitra, R.; Dua, R.; Aggarwal, S. A Qualitative Assessment among Personnel Working in Community-Led Development Program Settings Regarding Sexualized Substance Use. Brain Sci. 2022, 12, 1590. https://doi.org/10.3390/brainsci12111590
Marik B, Mahajan N, Sarkar R, Mitra R, Dua R, Aggarwal S. A Qualitative Assessment among Personnel Working in Community-Led Development Program Settings Regarding Sexualized Substance Use. Brain Sciences. 2022; 12(11):1590. https://doi.org/10.3390/brainsci12111590
Chicago/Turabian StyleMarik, Binata, Nupur Mahajan, Rohit Sarkar, Rochana Mitra, Rajiv Dua, and Sumit Aggarwal. 2022. "A Qualitative Assessment among Personnel Working in Community-Led Development Program Settings Regarding Sexualized Substance Use" Brain Sciences 12, no. 11: 1590. https://doi.org/10.3390/brainsci12111590