
Differentiation of Motor Speech Disorders through the Seven Deviance Scores from MonPaGe-2.0.s

Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Assessment of Speech Dimensions
2.2.1. Intelligibility
2.2.2. Articulation
2.2.3. Maximum Phonation Time (MPT)
2.2.4. Voice
2.2.5. Prosodic Contrast
2.2.6. Speech Rate
2.2.7. Diadochokinetic Rate
2.3. Measures of Impaired Speech (Deviance Scores)
2.4. Automatic Classification
3. Results
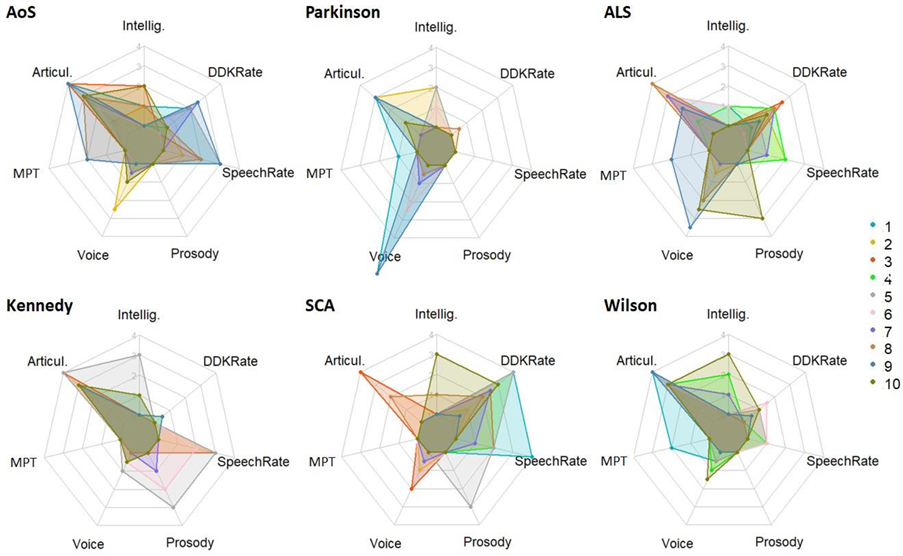
3.1. Description of Speech Profiles Per Group
3.2. Two-Class Automatic Classification
3.3. Feature Importance for all Considered Two-Class Classifications
4. Discussion
4.1. Success and Failures to Classify Subtypes of MSD
4.2. Relative Contribution of the Seven DevS
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Code, C. Models, Theories and Heuristics in Apraxia of Speech. Clin. Linguist. Phon. 1998, 12, 47–65. [Google Scholar] [CrossRef]
- Darley, F.L.; Aronson, A.E.; Brown, J.R. Motor Speech Disorders; WB Saunders Company: Philadelphia, PA, USA, 1975. [Google Scholar]
- Van Der Merwe, A. New Perspectives on Speech Motor Planning and Programming in the Context of the Four- Level Model and Its Implications for Understanding the Pathophysiology Underlying Apraxia of Speech and Other Motor Speech Disorders. Aphasiology 2021, 35, 397–423. [Google Scholar] [CrossRef]
- Ziegler, W. Modelling the Architecture of Phonetic Plans: Evidence from Apraxia of Speech. Lang. Cogn. Process. 2009, 24, 631–661. [Google Scholar] [CrossRef]
- Miller, H.E.; Guenther, F.H. Modelling Speech Motor Programming and Apraxia of Speech in the DIVA/GODIVA Neurocomputational Framework. Aphasiology 2021, 35, 424–441. [Google Scholar] [CrossRef] [PubMed]
- Darley, F.L.; Aronson, A.E.; Brown, J.R. Clusters of Deviant Speech Dimensions in the Dysarthrias. J. Speech Hear. Res. 1969, 12, 462–496. [Google Scholar] [CrossRef] [PubMed]
- Darley, F.L.; Aronson, A.E.; Brown, J.R. Differential Diagnostic Patterns of Dysarthria. J. Speech Hear. Res. 1969, 12, 246–269. [Google Scholar] [CrossRef]
- Duffy, J.R. Motor Speech Disorders E-Book: Substrates, Differential Diagnosis, and Management; Elsevier Health Sciences: Amsterdam, The Netherlands, 2019. [Google Scholar]
- McNeil, M.R. Clinical Management of Sensorimotor Speech Disorders; Thieme: New York, NY, USA, 2009. [Google Scholar]
- Molloy, J.; Jagoe, C. Use of Diverse Diagnostic Criteria for Acquired Apraxia of Speech: A Scoping Review. Int. J. Lang. Commun. Disord. 2019, 54, 875–893. [Google Scholar] [CrossRef]
- Bunton, K.; Kent, R.D.; Duffy, J.R.; Rosenbek, J.C.; Kent, J.F. Listener Agreement for Auditory-Perceptual Ratings of Dysarthria. J. Speech Lang. Hear. Res. 2007, 50, 1481–1495. [Google Scholar] [CrossRef]
- Kent, R.D. Hearing and Believing: Some Limits to the Auditory-Perceptual Assessment of Speech and Voice Disorders. Am. J. Speech Lang. Pathol. 1996, 5, 7–23. [Google Scholar] [CrossRef] [Green Version]
- Fonville, S.; Worp, H.B.; Maat, P.; Aldenhoven, M.; Algra, A.; Gijn, J. Accuracy and Inter-Observer Variation in the Classification of Dysarthria from Speech Recordings. J. Neurol. 2008, 255, 1545–1548. [Google Scholar] [CrossRef]
- Van der Graaff, M.; Kuiper, T.; Zwinderman, A.; Van de Warrenburg, B.; Poels, P.; Offeringa, A.; Van der Kooi, A.; Speelman, H.; De Visser, M. Clinical Identification of Dysarthria Types among Neurologists, Residents in Neurology and Speech Therapists. Eur. Neurol. 2009, 61, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Zyski, B.J.; Weisiger, B.E. Identification of Dysarthria Types Based on Perceptual Analysis. J. Commun. Disord. 1987, 20, 367–378. [Google Scholar] [CrossRef]
- Pernon, M.; Assal, F.; Kodrasi, I.; Laganaro, M. Perceptual Classification of Motor Speech Disorders: The Role of Severity, Speech Task, and Listener’s Expertise. J. Speech Lang. Hear. Res. 2022, 65, 2727–2747. [Google Scholar] [CrossRef] [PubMed]
- Kent, R.D.; Weismer, G.; Kent, J.F.; Vorperian, H.K.; Duffy, J.R. Acoustic Studies of Dysarthric Speech: Methods, Progress, and Potential. J. Commun. Disord. 1999, 32, 141–186. [Google Scholar] [CrossRef]
- Papakyritsis, I. Acoustic Phonetics for the Speech Clinician. In Manual of Clinical Phonetics; Routledge: Oxfordshire, UK, 2021; pp. 16–26. [Google Scholar]
- Fougeron, C.; Delvaux, V.; Menard, L.; Laganaro, M. The MonPaGe_HA Database for the Documentation of Spoken French throughout Adulthood. In Proceedings of the Eleventh International Conference on Language Resources and Évaluation (LREC 2018), Myazaki, Japan, 7–12 May 2018. [Google Scholar]
- Laganaro, M.; Fougeron, C.; Pernon, M.; Levêque, N.; Borel, S.; Fournet, M.; Catalano Chiuvé, S.; Lopez, U.; Trouville, R.; Ménard, L.; et al. Sensitivity and Specificity of an Acoustic- and Perceptual-Based Tool for Assessing Motor Speech Disorders in French: The MonPaGe-Screening Protocol. Clin. Linguist. Phon. 2021, 35, 1060–1075. [Google Scholar] [CrossRef]
- Rusz, J.; Cmejla, R.; Tykalova, T.; Ruzickova, H.; Klempir, J.; Majerova, V.; Picmausova, J.; Roth, J.; Ruzicka, E. Imprecise Vowel Articulation as a Potential Early Marker of Parkinson’s Disease: Effect of Speaking Task. J. Acoust. Soc. Am. 2013, 134, 2171–2181. [Google Scholar] [CrossRef] [Green Version]
- Little, M.; McSharry, P.; Hunter, E.; Spielman, J.; Ramig, L. Suitability of Dysphonia Measurements for Telemonitoring of Parkinson’s Disease. Nat. Preced. 2008, 1, 1. [Google Scholar] [CrossRef]
- Sztahó, D.; Kiss, G.; Vicsi, K. Estimating the Severity of Parkinson’s Disease from Speech Using Linear Regression and Database Partitioning. In Proceedings of the Sixteenth Annual Conference of the International Speech Communication Association, Dresden, Germany, 6–10 September 2015. [Google Scholar]
- Wang, J.; Kothalkar, P.V.; Cao, B.; Heitzman, D. Towards Automatic Detection of Amyotrophic Lateral Sclerosis from Speech Acoustic and Articulatory Samples. In Proceedings of the Interspeech, San Francisco, CA, USA, 8–12 September 2016; pp. 1195–1199. [Google Scholar]
- Hemmerling, D.; Orozco-Arroyave, J.R.; Skalski, A.; Gajda, J.; Nöth, E. Automatic Detection of Parkinson’s Disease Based on Modulated Vowels. In Proceedings of the Interspeech, San Francisco, CA, USA, 8–12 September 2016; pp. 1190–1194. [Google Scholar]
- Kodrasi, I.; Bourlard, H. Spectro-Temporal Sparsity Characterization for Dysarthric Speech Detection. IEEE/ACM Trans. Audio Speech Lang. Process. 2020, 28, 1210–1222. [Google Scholar] [CrossRef]
- Kodrasi, I.; Bourlard, H. Statistical Modeling of Speech Spectral Coefficients in Patients with Parkinson’s Disease. In Proceedings of the Speech Communication, 13th ITG-Symposium, Oldenburg, Germany, 10–12 October 2018; pp. 1–5. [Google Scholar]
- Janbakhshi, P.; Kodrasi, I.; Bourlard, H. Subspace-Based Learning for Automatic Dysarthric Speech Detection. IEEE Signal Process. Lett. 2020, 28, 96–100. [Google Scholar] [CrossRef]
- Kodrasi, I.; Pernon, M.; Laganaro, M.; Bourlard, H. Automatic Discrimination of Apraxia of Speech and Dysarthria Using a Minimalistic Set of Handcrafted Features. In Proceedings of the INTERSPEECH, Shanghai, China, 25–29 October 2020; pp. 4991–4995. [Google Scholar]
- Kodrasi, I.; Pernon, M.; Laganaro, M.; Bourlard, H. Automatic and Perceptual Discrimination between Dysarthria, Apraxia of Speech, and Neurotypical Speech. In Proceedings of the ICASSP 2021-2021 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Toronto, ON, Canada, 6–11 June 2021; pp. 7308–7312. [Google Scholar]
- Lansford, K.L.; Liss, J.M. Vowel Acoustics in Dysarthria: Speech Disorder Diagnosis and Classification. J. Speech Lang. Hear. Res. 2014, 57, 57–67. [Google Scholar] [CrossRef]
- Liss, J.M.; LeGendre, S.; Lotto, A.J. Discriminating Dysarthria Type from Envelope Modulation Spectra. J. Speech Lang. Hear. Res. 2010, 53, 1246–1255. [Google Scholar] [CrossRef] [Green Version]
- Illa, A.; Patel, D.; Yamini, B.; Shivashankar, N.; Veeramani, P.-K.; Polavarapui, K.; Nashi, S.; Nalini, A.; Ghosh, P.K. Comparison of Speech Tasks for Automatic Classification of Patients with Amyotrophic Lateral Sclerosis and Healthy Subjects. In Proceedings of the 2018 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Calgary, AB, Canada, 15–20 April 2018; pp. 6014–6018. [Google Scholar]
- Auzou, P.; Rolland-Monnoury, V. BECD: Batterie d’évaluation Clinique de La Dysarthrie; Ortho Edition: Isbergues, France, 2006. [Google Scholar]
- Boersma, P. Praat: Doing Phonetics by Computer [Computer Program]. 2011. Available online: http://www.praat.org/ (accessed on 15 March 2021).
- Ziegler, W. Task-Related Factors in Oral Motor Control: Speech and Oral Diadochokinesis in Dysarthria and Apraxia of Speech. Brain Lang. 2002, 80, 556–575. [Google Scholar] [CrossRef] [PubMed]
- Webb, G.I.; Fürnkranz, J.; Fürnkranz, J.; Fürnkranz, J.; Hinton, G.; Sammut, C.; Sander, J.; Vlachos, M.; Teh, Y.W.; Yang, Y.; et al. Decision Tree. In Encyclopedia of Machine Learning; Sammut, C., Webb, G.I., Eds.; Springer: Boston, MA, USA, 2011; pp. 263–267. [Google Scholar] [CrossRef]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-Learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Schalling, E.; Hartelius, L. Speech in Spinocerebellar Ataxia. Brain Lang. 2013, 127, 317–322. [Google Scholar] [CrossRef]
- Schalling, E.; Hammarberg, B.; Hartelius, L. Perceptual and Acoustic Analysis of Speech in Individuals with Spinocerebellar Ataxia (SCA). Logop. Phoniatr. Vocology 2007, 32, 31–46. [Google Scholar] [CrossRef]
- Sidtis, J.J.; Ahn, J.S.; Gomez, C.; Sidtis, D. Speech Characteristics Associated with Three Genotypes of Ataxia. J. Commun. Disord. 2011, 44, 478–492. [Google Scholar] [CrossRef] [Green Version]
- Atsuta, N. Natural History of Spinal and Bulbar Muscular Atrophy (SBMA): A Study of 223 Japanese Patients. Brain 2006, 129, 1446–1455. [Google Scholar] [CrossRef] [Green Version]
- Lévêque, N.; Slis, A.; Lancia, L.; Bruneteau, G.; Fougeron, C. Acoustic Change Over Time in Spastic and/or Flaccid Dysarthria in Motor Neuron Diseases. J. Speech Lang. Hear. Res. 2022, 65, 1767–1783. [Google Scholar] [CrossRef]
- Tanaka, S.; Banno, H.; Katsuno, M.; Suzuki, K.; Suga, N.; Hashizume, A.; Mano, T.; Araki, A.; Watanabe, H.; Adachi, H.; et al. Distinct Acoustic Features in Spinal and Bulbar Muscular Atrophy Patients with Laryngospasm. J. Neurol. Sci. 2014, 337, 193–200. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, S.; Hashizume, A.; Hijikata, Y.; Yamada, S.; Ito, D.; Nakayama, A.; Kurita, K.; Yogo, H.; Banno, H.; Suzuki, K.; et al. Nasometric Scores in Spinal and Bulbar Muscular Atrophy-Effects of Palatal Lift Prosthesis on Dysarthria and Dysphagia. J. Neurol. Sci. 2019, 407, 116503. [Google Scholar] [CrossRef]
- Mano, T.; Katsuno, M.; Banno, H.; Suzuki, K.; Suga, N.; Hashizume, A.; Araki, A.; Watanabe, H.; Tanaka, S.; Yamamoto, M.; et al. Tongue Pressure as a Novel Biomarker of Spinal and Bulbar Muscular Atrophy. Neurology 2014, 82, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Pernon, M.; Trocello, J.-M.; Vaissière, J.; Cousin, C.; Chevaillier, G.; Rémy, P.; Kidri-Osmani, K.; Fougeron, C.; Woimant, F. Le débit de parole du patient wilsonien dysarthrique peut-il être amélioré en condition de double tâche ? Rev. Neurol. 2013, 169, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Allison, K.M.; Cordella, C.; Iuzzini-Seigel, J.; Green, J.R. Differential Diagnosis of Apraxia of Speech in Children and Adults: A Scoping Review. J. Speech Lang. Hear. Res. 2020, 63, 2952–2994. [Google Scholar] [CrossRef]
- Ziegler, W.; Schölderle, T.; Brendel, B.; Amsellem, J.; Staiger, A. Higher-Faster-Farther: Maximum Performance Tests in the Assessment of Neurogenic Speech Impairment. Folia Phoniatr. Logop. 2019, 71, 261–274. [Google Scholar] [CrossRef] [PubMed]
- Speyer, R.; Bogaardt, H.C.A.; Passos, V.L.; Roodenburg, N.P.H.D.; Zumach, A.; Heijnen, M.A.M.; Baijens, L.W.J.; Fleskens, S.J.H.M.; Brunings, J.W. Maximum Phonation Time: Variability and Reliability. J. Voice 2010, 24, 281–284. [Google Scholar] [CrossRef]
- Maslan, J.; Leng, X.; Rees, C.; Blalock, D.; Butler, S.G. Maximum Phonation Time in Healthy Older Adults. J. Voice 2011, 25, 709–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goy, H.; Fernandes, D.N.; Pichora-Fuller, M.K.; van Lieshout, P. Normative Voice Data for Younger and Older Adults. J. Voice 2013, 27, 545–555. [Google Scholar] [CrossRef]
- Kent, R.D. Nonspeech Oral Movements and Oral Motor Disorders: A Narrative Review. Am. J. Speech Lang. Pathol. 2015, 24, 763–789. [Google Scholar] [CrossRef]
- Ziegler, W. Speech Motor Control Is Task-Specific: Evidence from Dysarthria and Apraxia of Speech. Aphasiology 2003, 17, 3–36. [Google Scholar] [CrossRef]
- Lancheros, M.; Pernon, M.; Laganaro, M. Is There a Continuum between Speech and Other Oromotor Tasks? Evidence from Motor Speech Disorders. Aphasiology 2022, 1–20. [Google Scholar] [CrossRef]
- Karlsson, F.; Hartelius, L. How Well Does Diadochokinetic Task Performance Predict Articulatory Imprecision? Differentiating Individuals with Parkinson’s Disease from Control Subjects. Folia Phoniatr. Logop. 2019, 71, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Skodda, S.; Grönheit, W.; Lukas, C.; Bellenberg, B.; von Hein, S.M.; Hoffmann, R.; Saft, C. Two Different Phenomena in Basic Motor Speech Performance in Premanifest Huntington Disease. Neurology 2016, 86, 1329–1335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.-T.; Kent, R.D.; Duffy, J.R.; Thomas, J.E. Analysis of Diadochokinesis in Ataxic Dysarthria Using the Motor Speech Profile ProgramTM. Folia Phoniatr. Logop. 2009, 61, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deger, K.; Ziegler, W. Speech Motor Programming in Apraxia of Speech. J. Phon. 2002, 30, 321–335. [Google Scholar] [CrossRef]
- Staiger, A.; Schölderle, T.; Brendel, B.; Ziegler, W. Dissociating Oral Motor Capabilities: Evidence from Patients with Movement Disorders. Neuropsychologia 2017, 95, 40–53. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, W.; Aichert, I. How Much Is a Word? Predicting Ease of Articulation Planning from Apraxic Speech Error Patterns. Cortex 2015, 69, 24–39. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, W.; Aichert, I.; Staiger, A. When Words Don׳t Come Easily: A Latent Trait Analysis of Impaired Speech Motor Planning in Patients with Apraxia of Speech. J. Phon. 2017, 64, 145–155. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Clinical group | Sex (F-M) | Age (range) | CPSS (range) |
|---|---|---|---|
| Post-stroke apraxia of speech (AoS) | 6-4 | 52.5 (24–72) | 8.5 (4–14) |
| Hypokinetic dysarthria in Parkinson Disease (PD) | 2-8 | 74.5 (55–93) | 7.2 (4–11) |
| Mixed dysarthria in amyotrophic lateral sclerosis (ALS) | 3-7 | 61.5 (45–75) | 8.6 (6–14) |
| Flaccid dysarthria in Kennedy disease | 0-10 | 68.7(49–85) | 7.7 (5–13) |
| Ataxic dysarthria in spinocerebellar ataxia (SCA) | 7-3 | 50.4 (27–67) | 7.8 (6–12) |
| Mixed dysarthria in Wilson disease | 1-9 | 35.5 (26–49) | 9.2 (5–14) |
| C1 | |||||||
|---|---|---|---|---|---|---|---|
| AoS | Parkinson | ALS | Kennedy | Wilson | SCA | ||
| C2 | AoS | - | 75 (90/60) | 80 (80/80) | 70 (70/70) | 75 (100/50) | 95 (100/90) |
| Parkinson | 75 (60/90) | - | 80 (90/70) | 90 (90/90) | 95 (100/90) | 90 (90/90) | |
| ALS | 80 (80/80) | 80 (70/90) | - | 100 (100/100) | 75 (90/60) | 70 (80/60) | |
| Kennedy | 70 (70/70) | 90 (90/90) | 100 (100/100) | - | 75 (50/100) | 90 (80/100) | |
| Wilson | 75 (50/100) | 95 (90/100) | 75 (60/90) | 75 (100/50) | - | 90 (80/100) | |
| SCA | 95 (90/100) | 90 (90/90) | 70 (60/80) | 90 (100/80) | 90 (100/80) | - | |
| Mean ± SD | 79.0 ± 8.6 (70.0 ± 14.1 / 88.0 ± 14.1) | 86.0 ± 7.3 (86.0 ± 8.0 / 86.0 ± 13.6) | 81.0 ± 10.2 (78.0 ± 16.0 / 84.0 ± 10.2) | 85.0 ± 11.0 (92.0 ± 11.7 / 78.0 ± 17.2) | 82.0 ± 8.7 (88.0 ± 19.4 / 76.0 ± 18.5) | 87.0 ± 8.7 (86.0 ± 8.0 / 88.0 ± 4.7) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fougeron, C.; Kodrasi, I.; Laganaro, M. Differentiation of Motor Speech Disorders through the Seven Deviance Scores from MonPaGe-2.0.s. Brain Sci. 2022, 12, 1471. https://doi.org/10.3390/brainsci12111471
Fougeron C, Kodrasi I, Laganaro M. Differentiation of Motor Speech Disorders through the Seven Deviance Scores from MonPaGe-2.0.s. Brain Sciences. 2022; 12(11):1471. https://doi.org/10.3390/brainsci12111471
Chicago/Turabian StyleFougeron, Cécile, Ina Kodrasi, and Marina Laganaro. 2022. "Differentiation of Motor Speech Disorders through the Seven Deviance Scores from MonPaGe-2.0.s" Brain Sciences 12, no. 11: 1471. https://doi.org/10.3390/brainsci12111471