3.1. Parameter Distributions
Table 4 presents an overview of the distributions of BoDyS raw and standard scores in the control participants and the patients. Recall that all variables were normalized for age and sex. Significant influences of age were present in the respiration (RSP) and the voice stability raw scores (VOS), a significant influence of sex was present in voice quality (VOQ).
There was overlap between the PAT and the CTRL participants on all scales, but completely unremarkable profiles were rare in the patients. The most severe impairments were observed in articulation (ART), prosodic modulation (MOD), articulation rate (TEM), and respiration (RSP). Student’s t-tests revealed significant differences between the two groups in all parameters.
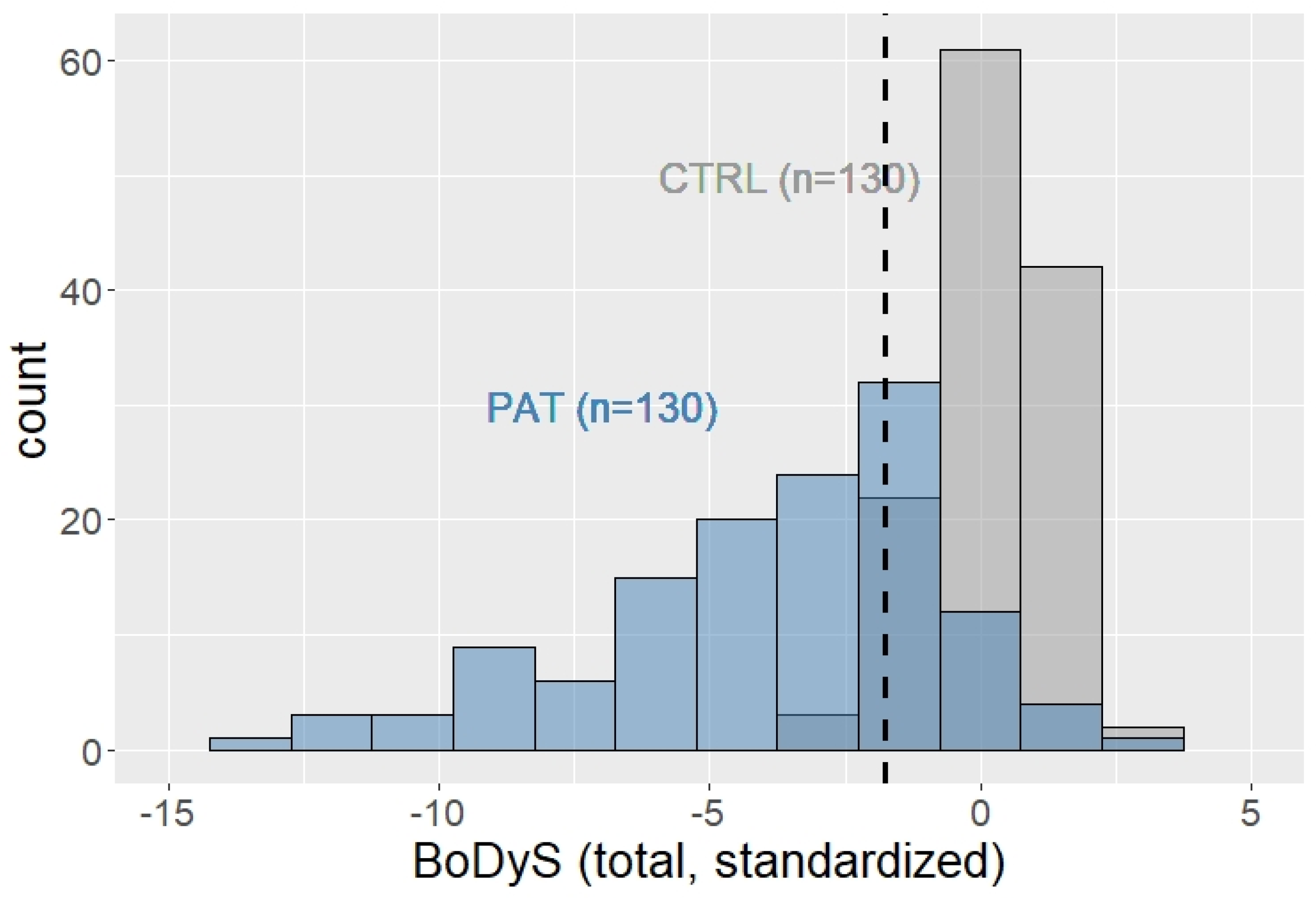
Figure A2 in
Appendix A plots the distributions of standardized BoDyS total scores in both groups (see also
Table 4, bottom row), illustrating that the distribution in the patient group was strongly left-skewed, that is, the vast majority of the neurologic patients (94%) ranged clearly below the median of the CTRL group. Overall, 91/130 (70%) had BoDyS total scores below the 5th percentile of the controls, and 79/130 patients (61%) were below the 1% cutoff, suggesting that between 60 and 70% of the patients most likely had dysarthria.
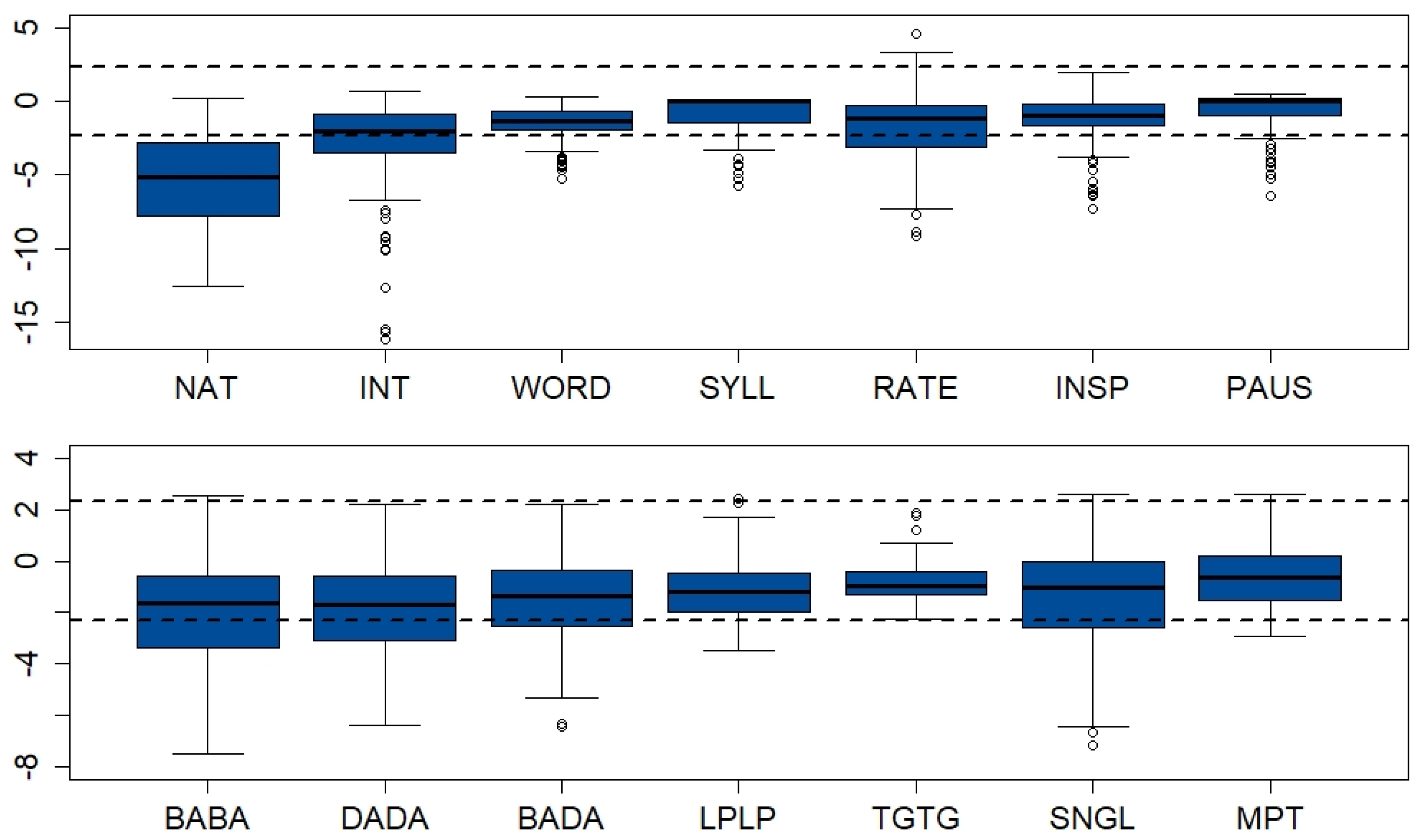
Figure 1 depicts the distributions of the specific speech- (top panel) and nonspeech parameters (bottom panel) in the patient sample. Standard scores are plotted for all parameters, with the dashed horizontal lines delineating the 1–99% range of the control data.
Table A7 in
Appendix C documents the raw and ƶ-scores corresponding to
Figure 1. Student’s
t-tests revealed significant group differences in all parameters.
Notably, in the patients, most of the standardized speech parameters covered a much wider range than the nonspeech parameters, which was due to the narrower distributions of speech parameters in the neurotypical participants (
Figure 1). The clearest separation between the CTRL and PAT groups resulted in the naturalness ratings, whereas for other variables, considerable overlap was found, for example, in the perceived accuracy of segmental articulation in isolated words and syllables and in speech pauses, as well as in repetitive lip (LPLP) and tongue movement rates (TGTG) and in maximum phonation times (MPT).
3.2. Factor Structure and Dimensionality of the Assessment Parameters
To explore how the speech and nonspeech parameters interacted and thereby to cross-validate nonspeech by speech measures, we applied Exploratory Graph Analysis (EGA; R-function boot EGA [
76]) to fit the standardized scores of all diagnostic variables across the patient group. A graphical LASSO model was computed using the walktrap algorithm with 1000 bootstrap iterations. The “Leading Eigenvalue” (LE) algorithm was applied to the Spearman correlation matrix. For details regarding this method see [
53].
The EGA model converged to a 5-factor solution in 100% of the bootstrap iterations, demonstrating a high dimension stability.
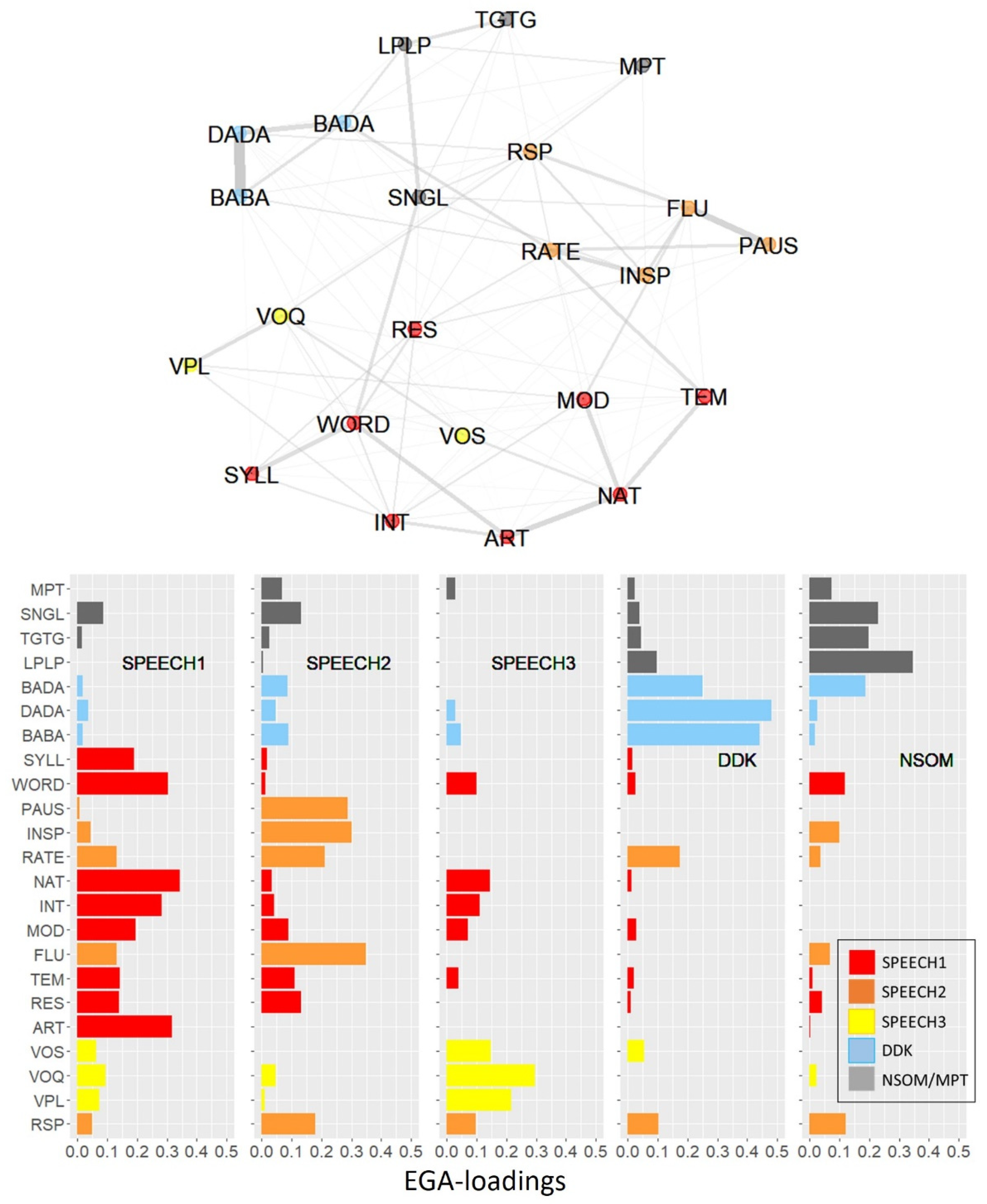
Figure 2 (top) plots the graphical solution and illustrates how the diagnostic variables were allocated to the five dimensions. The nodes represent the diagnostic variables; edges represent the strengths of the connections between variables (essentially partial correlations). The bottom panel of
Figure 2 displays the EGA loadings of each dimension on each variable, with high loadings indicating a strong association with the respective factor.
Dimension 1 (red nodes/bars in
Figure 2) comprised the BoDyS resonance, articulation, articulation rate, and prosodic modulation scales (RES, ART, TEM, MOD), as well as segmental accuracy in word- and syllable production (WORD, SYLL), together with intelligibility and naturalness (INT, NAT). Particularly strong bindings connected naturalness with ART, TEM, and MOD as well as the BoDyS articulation scale (ART) with the two syllable- and word-based articulation parameters (WORD, SYLL) and with intelligibility (INT). As all indicators of dimension 1 were speech parameters, this dimension will be referred to as SPEECH 1.
Dimension 2 (orange nodes/bars in
Figure 2) comprised parameters related with speech fluency, that is, the BoDyS fluency scale (FLU) and the acoustic measures of speech pauses and articulation rate (PAUS, INSP, RATE), as well as BoDyS respiration parameter (RSP). Low RSP scores are usually associated with increased speech breathing, which in turn has an impact on fluency [
77]. Particularly strong connections were held between perceived fluency (FLU) and speech pauses (PAUS) and between inspiration pauses (INSP) and articulation rate (RATE). As all indicators of dimension 2 were speech parameters, it will henceforth be referred to as SPEECH 2.
Dimension 3 (yellow nodes/bars in
Figure 2) comprised the three voice scales of the BoDyS and will be referred to as SPEECH 3.
Dimension 4 (blue nodes/bars in
Figure 2) comprised the three DDK
syl rate variables BABA, DADA, and BADA, with a strong binding between BABA and DADA. Note that this dimension had very low loadings on all speech parameters except RATE.
Dimension 5 (grey nodes/bars in
Figure 2) comprised the three nonspeech oral motor tasks, that is, the alternating lip and tongue movement rates (LPLP, TGTG) and the single nonspeech oral motor accuracy measure (SNGL), together with maximum phonation time (MPT). This dimension will be referred to as NSOM/MPT. Its loadings on the speech parameters were low. Note that MPT had low or zero loadings from all five dimensions, indicating an outsider role of this measure within the set of diagnostic parameters examined here.
A notably strong binding between dimensions was found between perceived articulation rate (TEM; SPEECH 1) and articulation rate measured in the acoustic signal (RATE, SPEECH 2). Note that the three SPEECH dimensions had very low or even zero loadings on the DDKsyl and the NSOM/MPT parameters.
To validate the EGA model, a confirmatory factor analysis (CFA) with Maximum Likelihood estimation was performed, including the five EGA dimensions as factors and their corresponding parameters as indicators. The metric of the five latent variables was determined by fixing their variances to 1.0. The model was overidentified with 220 degrees of freedom. Admittedly, with 23 indicators and a sample size of 130, this analysis can only be seen as orienting, as it bears the risk of overfitting. The CFA model fitted the data with acceptable overall fit statistics: The root mean square error of approximation (RMSEA) was 0.08, which suggests adequate fit, and comparative fit indices of CFI = 0.90 and TLI = 0.88 were indicative of acceptable model fit (cf. [
75]. The correlations between the five dimensions ranged between r = 0.37 (SPEECH3 vs. NSOM/MPT) and r = 0.81 (SPEECH2 vs. DDK). The complete correlation matrix is plotted in
Table A8 of
Appendix D. Inspection of the CFA loadings revealed an area of strain in the NSOM factor with a loading of only 0.35 on maximum phonation time (MPT), which underscores the outsider role of this parameter and explains why the model fit was only moderate.
3.3. Effectors, Domain–General Functions or Tasks?
As mentioned in the introduction, one of the reasons why nonspeech tasks are so common in dysarthria assessment is that they can be designed for high effector-specificity [
15]. Another hypothesis was that nonspeech tasks can be designed to test specific functional goals on which they overlap with speech [
16]. The EGA model of
Figure 2 is inconsistent with the effector-specificity assumption insofar as the lip- and tongue-related DDK-parameters were not assigned to separate lip and tongue dimensions, respectively, but were grouped by task, that is, syllable DDK (BABA, DADA) and single-articulator DDK (LPLP, TGTG). Furthermore, the result that two parameters reflecting fundamentally different functional goals, that is, maximum repetition rate (LPLP, TGTG) and single movement accuracy (SNGL) were allocated to the same factor NSOM/MPT, whereas the maximum repetition parameters with their overlapping functional goals were split into two separate factors, that is, NSOM/MPT and DDK
syl, is inconsistent with the function-specificity assumption.
Because the analysis presented in the previous section did not consider this aspect systematically enough, potential evidence for effector- or function-specificity may have gone unnoticed. In particular, the EGA model was not specified for effector-specific speech- and single-articulator tasks. To refine the model for suitable testing of the three competing assumptions, that is, effector-, function- or task-specificity, the speech parameters describing the accuracy of segmental articulation in words and syllables (WORD, SYLL) was re-analyzed by splitting the materials into items involving lip vs. anterior tongue movements, that is, labial vs. coronal consonants (see
Appendix B,
Table A4 and
Table A5). Furthermore, the nonspeech parameter characterizing the accuracy of single articulator movements (parameter SNGL) was split into items addressing the motility of the lips and the tongue separately (
Appendix B,
Table A6). Together with the two-syllable repetition parameters BABA vs. DADA and the two repetitive lip and tongue movement tasks LPLP vs. TGTG, this design comprised four effector-specific speech parameters, that is, WORD.LP/SYLL.LP and WORD.TG/SYLL.TG for the accuracy of labial and alveolar consonant articulation, respectively, and six effector-specific nonspeech parameters. The latter were split into two parameters characterizing the accuracy of non-repetitive single articulator movements, referred to as LP and TG, two parameters characterizing the maximum speed of repetitive single articulator movements (LPLP and TGTG), and two maximum repetition rate parameters for the lips and the tongue blade (BABA, DADA). This selection of diagnostic parameters allowed us to analyze, along with effector-specificity (labial vs. lingual), also the function-specificity of speech and nonspeech parameters, that is, whether they test the involved functional goals, accuracy vs. speed, across the speech and the nonspeech domains. The parameter set was further expanded by the effector-unspecific intelligibility parameter INT. In an effector-specific diagnostic model, we expected that INT would be excluded from the lip and tongue dimensions. In a function-specific model, it would be assigned to the accuracy- rather than the speed dimension and in a task-specific model, it would go together with the WORD- and SYLL-parameters.
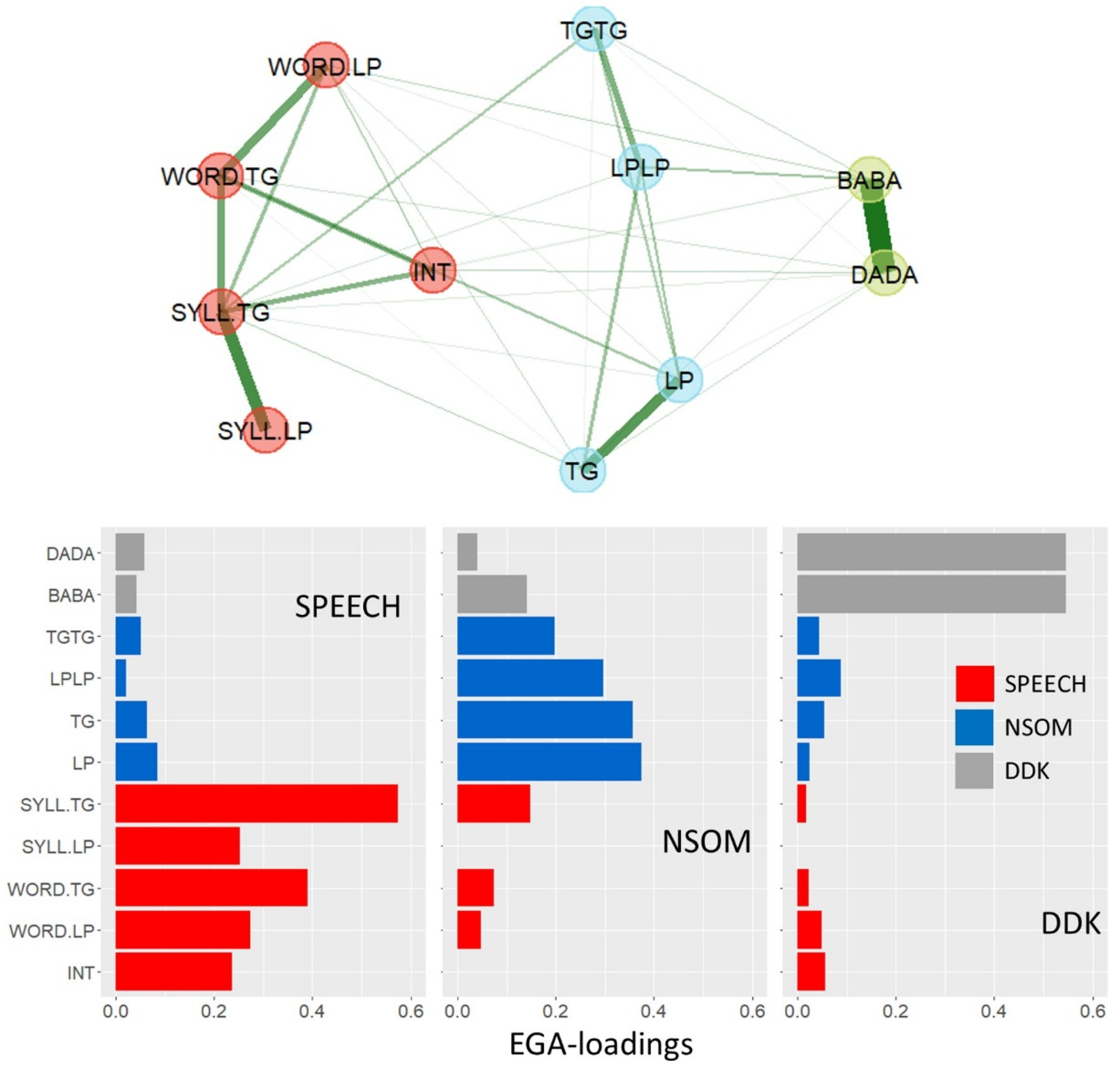
Figure 3 depicts an EGA-model of these parameters over the patient sample (
n = 130), with the graphical solution (top) and the EGA loadings (bottom). The model converged to a 3-dimensional solution with no variation of dimensionality across 1000 bootstrap iterations, indicating high dimensional stability of the solution.
A first dimension, termed SPEECH, encompassed the four parameters representing accuracy of consonant articulation together with intelligibility, that is, exclusively speech-related parameters. A second dimension aggregated the repetitive and non-repetitive single articulator parameters (NSOM), and a third dimension combined the two-syllable DDK parameters. Thus, the three factors respected neither effector- nor function boundaries: the lip and tongue-related parameters were all conflated within dimensions, the parameters targeting speed goals were split between the NSOM and the DDKsyl dimensions, and the parameters targeting spatial accuracy were split between the SPEECH and the NSOM dimensions. In all dimensions, strong bindings were found between the lip- and tongue-specific variables within parameter types, suggesting that it was the characteristics of the task rather than the particular effector which made parameters structurally similar.
To validate the exploratory model, a confirmatory factor analysis (CFA) was performed with the three EGA-dimensions as factors and their corresponding parameters as indicators. Given the inclusion of only 11 indicators with a sample size of 130, the risk of overfitting was lower with this smaller measurement model [
75]. The model fitted the data exceptionally well (RMSEA = 0.02, CFI = 0.99, TLI = 0.99; cf.
Section 2.3). For the intercorrelation matrix of the three factors see
Table A9 of
Appendix D.
To further test the assumptions of effector-, function-, and task-specificity against each other, a simplified, orthogonal design based on one pair of effector-specific variables per parameter type was included, and intelligibility was dropped from the parameter list (see
Table 5). As for the effector hypothesis, a confirmatory factor analysis was designed using a two-factor measurement model in which the four lip-related variables were modeled to load onto a LIP factor, and the four tongue-related variables onto a TONGUE factor. The two latent variables were permitted to be correlated, based on the assumption that external variables may exert third-variable influences on both factors. The fit indices of this model indicated an extremely poor fit, with CFI and TLI coefficients substantially below 0.90 and an RMSEA coefficient far above 0.10 (
Table 5). Therefore, the effector-model was abandoned (for goodness-of-fit criteria cf.
Section 2.3).
A further two-factor measurement model with domain-general functions as latent variables was designed, in which the two speech and the two single, non-repetitive articulator variables were modeled to load onto an ACCURACY factor and the four maximum repetition rate parameters onto a SPEED factor. Again, the two factors were permitted to be correlated. The fit indices of this model also indicated a poor fit, with CFI and TLI coefficients clearly below 0.90 and an RMSEA coefficient clearly above 0.10 (
Table 5), leading to the rejection of the model based on domain–general functions.
In a third CFA model, the task hypothesis was tested again for the more selective parameter ensemble of
Table 5. The model was designed for three latent variables, that is, SPEECH, NSOM, and DDK
syl, with diagnostic parameters assigned as indicators as shown in
Table 5. The comparative fit indices of this model, CFI and TLI, were both clearly above 0.95, and the RMSEA was 0.08, indicating a fully adequate model fit.
As a result, the hypothesis of task-specificity was maintained, whereas the two alternative models of effector- and function-specificity were abandoned.


 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}




