
Multi-Perspective Feature Extraction and Fusion Based on Deep Latent Space for Diagnosis of Alzheimer’s Diseases
 , ,
, ,
Abstract
:
1. Introduction
2. Materials
3. Methods
3.1. Latent Space Representation Network
3.1.1. Stage 1: Deep Latent Space Representation Learning
- rs-fMRI pre-processing: The first task is to normalize the ROIs for each subject, and for a BOLD time series t with N ROIs. We obtained the following Equation (1):, are the mean and variance of the corresponding series, respectively.
- Construction of the dFC: To describe the dynamic changes in brain regions and construct the dFC, we divided the time series of ROIs obtained by rs-fMRI into M overlapping sliding windows. The sliding window size and step size in this paper are based on previous work [13,21,23,26], with a window size of 30 timepoints (90 volumes for a total of 270 s) and a step size of two steps (6 s) to construct M overlapping subsequences ; for any , we have , and M is 54 in this paper. According to the PCC, for each overlapping subsequence of N ROIs, M dFCs are constructed, and we have Equation (2), as follows:In the above Equation (2), ,; then, denote the i-th and j-th ROI segments in each overlapping subsequence, and , and , correspond to the mean and variance of the i-th and j-th segments of that ROI sequence, respectively.
- Learning of the dFC using a deep autoencoder to obtain the latent space representation: We constructed M dFCs, and since the dFC obtained by PCC is a diagonal matrix, the redundant feature information is removed, the upper triangular part of each diagonal matrix is taken out, and the dimensionality of the features is reduced from to . For each subject, we have features, and these are used as the input and label of the autoencoder in stage 1.
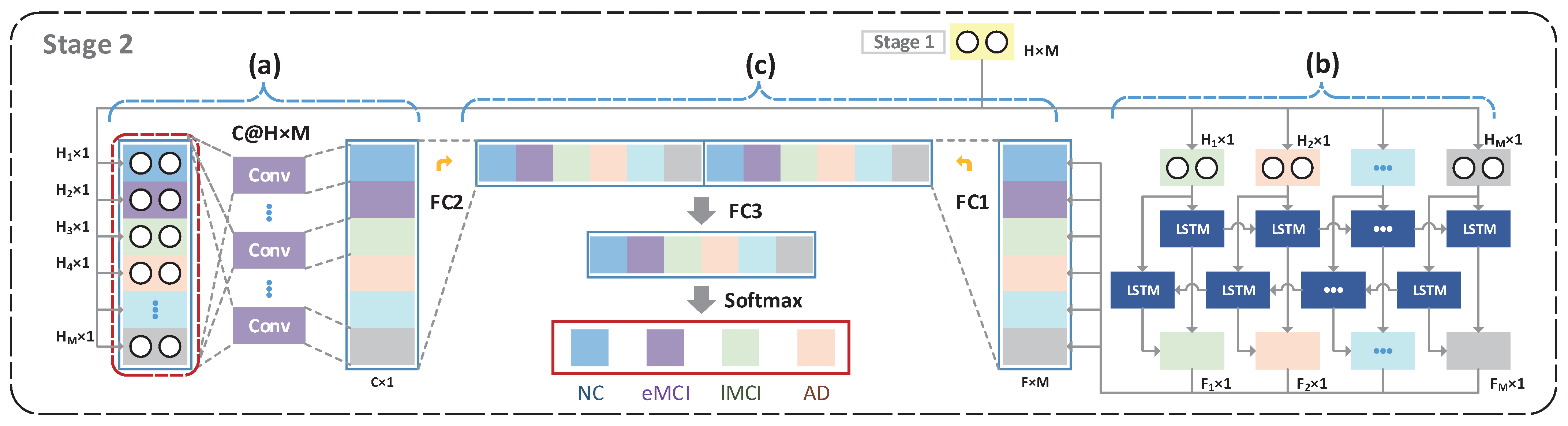
3.1.2. Stage 2: Multi-Perspective Latent Space Representation Learning and Fusion
- Convolutional neural networks for the global perspective (Global CNN, GCNN): In order to parse the global contextual information latent in brain regions, we designed a global-perspective-based convolutional neural network to extract global contextual information in the latent space representation. Specifically, for each subject, we set the size of the kernel to . That is, we globally parsed the dynamic features of the brain regions at each moment in time from a global perspective, which can also be interpreted as extracting contextual information as the brain completes high-level tasks, enabling the understanding of multiple complex brain-context-related activity information through multiple convolutional kernels. However, since the latent space representation belongs to the high-level feature representation in the dFC, a convolutional neural network employing a global perspective at this stage could discover global contextual information from the high-level features. The multi-kernel convolutioncan be thought of as understanding the brain’s high-level tasks and extracting the contextual feature information needed to perform these high-level tasks.
- BiLSTM for the local perspective: In order to parse the local spatial and temporal dynamics of brain regions, we used a BiLSTM to parse the temporal dimension, to parse the features in both directions from the temporal dimension, to obtain the spatial feature variations, and to gradually filter the features at multiple levels from the spatial dimension to finally obtain dynamic high-level information at the spatial and temporal levels. At this stage, it can be understood that the BiLSTM network gradually understands the high-level information of the brain according to the temporal variation, and then abstractly understands the relationship between the dynamic variations in brain regions and disease in different patients.
- Multi-perspective feature fusion network (FusionNet): We combined the global contextual feature information (global features, GF) of the high-level task with the spatial and temporal dynamic variation features (dynamic features, DF), and compressed and downscaled the two models to perform multi-level deep feature fusion. As shown in Equation (4), we stacked the feature information from GF and TF and fed this into FusionNet for feature dimensionality reduction and compression, and finally used the softmax layer for feature classification.
4. Results
4.1. Methods for Comparison
- ROIs + SVM: A simple method for processing BOLD signals, which directly stacks full-length BOLD signals () from N brain regions, trains the intensity of BOLD as an SVM and predicts brain disease.
- sFC + SVM: Most traditional research methods involve the construction of sFCs from full-length BOLD information based on the PCC, stacking the sFCs in a reduced dimension and feeding them to SVMs for training.
- dFC + BiLSTM: In recent studies, the dFC is usually constructed according to a set sliding window, and the upper triangular features of the dFC symmetrical matrix are extracted and input to the BiLSTM model. The BiLSTM learns relevant information about brain regions in both directions and the association between diseases and brain region FC, and finally achieves brain disease diagnosis. Specifically, the upper triangular features are stacked into , the hidden layer features of the BiLSTM are set to H, and features of the same subject are used as the model input.
- dFC + GCNN: As a component of our study, the direct use of GCNN can extract high-level features in the global context of brain regions in the dFC. Specifically, we use M dFCs from each subject as input to the global convolutional layer, and the output features are classified via softmax.
- dFC + AE + GCNN (LSRNet-G): This method removes the BiLSTM compared to the proposed method to evaluate the BiLSTM’s contribution to the model. Specifically, we use the compressed global high-level contextual features for brain disease classification after learning the global perspective of the GCNN’s representation of the latent space of the autoencoder.
- dFC + AE + BiLSTM (LSRNet-B): This method removes the GCNN and directly uses the BiLSTM to extract the latent space representation for brain region classification. The M output latent space representations are fed into the BiLSTM one at a time, according to the temporal order for extracting dynamic variations in brain regions. Finally, we perform feature stacking and dimensionality reductions on the last layer of the BiLSTM output for brain disease diagnosis classification.
4.2. Feature Analysis
4.3. Comparison with Other Methods
5. Discussion
Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bondi, M.W.; Edmonds, E.C.; Salmon, D.P. Alzheimer’s disease: Past, present, and future. J. Int. Neuropsychol. Soc. 2017, 23, 818–831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosyreva, A.M.; Sentyabreva, A.V.; Tsvetkov, I.S.; Makarova, O.V. Alzheimer’s Disease and Inflammaging. Brain Sci. 2022, 12, 1237. [Google Scholar] [CrossRef]
- Yiannopoulou, K.G.; Papageorgiou, S.G. Current and future treatments in Alzheimer disease: An update. J. Cent. Nerv. Syst. Dis. 2020, 12, 1179573520907397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, K.; Jie, B.; Dong, P.; Ding, X.; Bian, W.; Liu, M. Convolutional Recurrent Neural Network for Dynamic Functional MRI Analysis and Brain Disease Identification. Front. Neurosci. 2022, 1050. [Google Scholar] [CrossRef]
- Dubois, B.; Feldman, H.H.; Jacova, C.; Cummings, J.L.; DeKosky, S.T.; Barberger-Gateau, P.; Delacourte, A.; Frisoni, G.; Fox, N.C.; Galasko, D. Revising the definition of Alzheimer’s disease: A new lexicon. Lancet Neurol. 2010, 9, 1118–1127. [Google Scholar] [CrossRef]
- Jiao, Z.; Chen, S.; Shi, H.; Xu, J. Multi-modal feature selection with feature correlation and feature structure fusion for MCI and AD classification. Brain Sci. 2022, 12, 80. [Google Scholar] [CrossRef] [PubMed]
- Bai, F.; Zhang, Z.; Watson, D.R.; Yu, H.; Shi, Y.; Yuan, Y.; Zang, Y.; Zhu, C.; Qian, Y. Abnormal functional connectivity of hippocampus during episodic memory retrieval processing network in amnestic mild cognitive impairment. Biol. Psychiatry 2009, 65, 951–958. [Google Scholar] [CrossRef]
- Meir-Hasson, Y.; Kinreich, S.; Podlipsky, I.; Hendler, T.; Intrator, N. An EEG finger-print of fMRI deep regional activation. Neuroimage 2014, 102, 128–141. [Google Scholar] [CrossRef] [PubMed]
- Mao, Z.; Su, Y.; Xu, G.; Wang, X.; Huang, Y.; Yue, W.; Sun, L.; Xiong, N. Spatio-temporal deep learning method for adhd fmri classification. Inf. Sci. 2019, 499, 1–11. [Google Scholar] [CrossRef]
- Qiao, J.; Lv, Y.; Cao, C.; Wang, Z.; Li, A. Multivariate deep learning classification of Alzheimer’s disease based on hierarchical partner matching independent component analysis. Front. Aging Neurosci. 2018, 10, 417. [Google Scholar] [CrossRef]
- Van Den Heuvel, M.P.; Pol, H.E.H. Exploring the brain network: A review on resting-state fMRI functional connectivity. Eur. Neuropsychopharmacol. 2010, 20, 519–534. [Google Scholar] [CrossRef] [PubMed]
- Feng, C.; Jie, B.; Ding, X.; Zhang, D.; Liu, M. Constructing high-order dynamic functional connectivity networks from resting-state fMRI for brain dementia identification. In Proceedings of the International Workshop on Machine Learning in Medical Imaging, Lima, Peru, 4 October 2020; pp. 303–311. [Google Scholar]
- Wang, M.; Lian, C.; Yao, D.; Zhang, D.; Liu, M.; Shen, D. Spatial-temporal dependency modeling and network hub detection for functional MRI analysis via convolutional-recurrent network. IEEE Trans. Biomed. Eng. 2019, 67, 2241–2252. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Xiao, Z.; Wu, J. Functional connectivity-based classification of autism and control using SVM-RFECV on rs-fMRI data. Phys. Medica 2019, 65, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Sporns, O. The human connectome: A complex network. Ann. N. Y. Acad. Sci. 2011, 1224, 109–125. [Google Scholar] [CrossRef]
- Wang, M.; Zhang, D.; Huang, J.; Yap, P.-T.; Shen, D.; Liu, M. Identifying autism spectrum disorder with multi-site fMRI via low-rank domain adaptation. IEEE Trans. Med. Imaging 2019, 39, 644–655. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Small, M. Complex network from pseudoperiodic time series: Topology versus dynamics. Phys. Rev. Lett. 2006, 96, 238701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lacasa, L.; Luque, B.; Ballesteros, F.; Luque, J.; Nuno, J.C. From time series to complex networks: The visibility graph. Proc. Natl. Acad. Sci. USA 2008, 105, 4972–4975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Cheng, W.; Liu, Z.; Zhang, K.; Lei, X.; Yao, Y.; Becker, B.; Liu, Y.; Kendrick, K.M.; Lu, G. Neural, electrophysiological and anatomical basis of brain-network variability and its characteristic changes in mental disorders. Brain 2016, 139, 2307–2321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, E.A.; Damaraju, E.; Plis, S.M.; Erhardt, E.B.; Eichele, T.; Calhoun, V.D. Tracking whole-brain connectivity dynamics in the resting state. Cereb. Cortex 2014, 24, 663–676. [Google Scholar] [CrossRef] [PubMed]
- Jie, B.; Liu, M.; Lian, C.; Shi, F.; Shen, D. Designing weighted correlation kernels in convolutional neural networks for functional connectivity based brain disease diagnosis. Med. Image Anal. 2020, 63, 101709. [Google Scholar] [CrossRef]
- Azevedo, T.; Campbell, A.; Romero-Garcia, R.; Passamonti, L.; Bethlehem, R.A.; Liò, P.; Toschi, N. A deep graph neural network architecture for modelling spatio-temporal dynamics in resting-state functional MRI data. Med Image Anal. 2022, 79, 102471. [Google Scholar] [CrossRef]
- Yan, W.; Zhang, H.; Sui, J.; Shen, D. Deep chronnectome learning via full bidirectional long short-term memory networks for MCI diagnosis. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Granada, Spain, 16–20 September 2018; pp. 249–257. [Google Scholar]
- Jack, C.R., Jr.; Bernstein, M.A.; Fox, N.C.; Thompson, P.; Alexander, G.; Harvey, D.; Borowski, B.; Britson, P.J.; Whitwell, J.L.; Ward, C. The Alzheimer’s disease neuroimaging initiative (ADNI): MRI methods. J. Magn. Reson. Imaging Off. J. Int. Soc. Magn. Reson. Med. 2008, 27, 685–691. [Google Scholar] [CrossRef] [Green Version]
- Petersen, R.C.; Aisen, P.; Beckett, L.A.; Donohue, M.; Gamst, A.; Harvey, D.J.; Jack, C.; Jagust, W.; Shaw, L.; Toga, A. Alzheimer’s disease neuroimaging initiative (ADNI): Clinical characterization. Neurology 2010, 74, 201–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jie, B.; Liu, M.; Shen, D. Integration of temporal and spatial properties of dynamic connectivity networks for automatic diagnosis of brain disease. Med. Image Anal. 2018, 47, 81–94. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.; Jie, B.; Dong, P.; Ding, X.; Bian, W.; Liu, M. Extracting Sequential Features from Dynamic Connectivity Network with rs-fMRI Data for AD Classification. In Proceedings of the International Workshop on Machine Learning in Medical Imaging, Strasbourg, France, 27 September 2021; pp. 664–673. [Google Scholar]
- Bi, X.-a.; Shu, Q.; Sun, Q.; Xu, Q. Random support vector machine cluster analysis of resting-state fMRI in Alzheimer’s disease. PLoS ONE 2018, 13, e0194479. [Google Scholar] [CrossRef] [Green Version]
- Kam, T.-E.; Zhang, H.; Jiao, Z.; Shen, D. Deep learning of static and dynamic brain functional networks for early MCI detection. IEEE Trans. Med Imaging 2019, 39, 478–487. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Wang, J.; Zhang, C.; Luo, Z.; Luo, X.; Xiao, L.; Shi, J. Uncertainty modeling for multi center autism spectrum disorder classification using takagi-sugeno-kang fuzzy systems. IEEE Trans. Cogn. Dev. Syst. 2021, 14, 21764540. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | NC vs. eMCI (%) | NC vs. AD (%) | ||||
|---|---|---|---|---|---|---|
| ROIs + SVM | ||||||
| sFC + SVM | ||||||
| dFC + BiLSTM | ||||||
| dFC + GCNN | ||||||
| LSRNet-G | ||||||
| LSRNet-B | ||||||
| LSRNet | ||||||
| Method | eMCI vs. lMCI (%) | lMCI vs. AD (%) | ||||
|---|---|---|---|---|---|---|
| ACC | ACC | ACC | ACC | ACC | ||
| ROIs + SVM | ||||||
| sFC + SVM | ||||||
| dFC + BiLSTM | ||||||
| dFC + GCNN | ||||||
| LSRNet-G | ||||||
| LSRNet-B | ||||||
| LSRNet | ||||||
| Method | NC vs. eMCI vs. lMCI vs. AD (%) | ||||
|---|---|---|---|---|---|
| ROIs + SVM | |||||
| sFC + SVM | |||||
| dFC + BiLSTM | |||||
| dFC + GCNN | |||||
| LSRNet-G | |||||
| LSRNet-B | |||||
| LSRNet | |||||
| Target | Authors | Method | Modality | Dataset | Accuracy (%) |
|---|---|---|---|---|---|
| NC/eMCI | Jie et al. [21] | Wck-CNN | rs-fMRI | 48 NC, 50 eMCI | 84.6 |
| Lin et al. [27] | LSTM | rs-fMRI | 48 NC, 50 eMCI | 84.5 | |
| Our | LSRNet | rs-fMRI | 48 NC, 50 eMCI | 84.6 | |
| NC/AD | Jie et al. [21] | Wck-CNN | rs-fMRI | 48 NC, 31 AD | 88.0 |
| Wang et al. [13] | STNet | rs-fMRI | 48 NC, 31 AD | 90.3 | |
| Lin et al. [27] | LSTM | rs-fMRI | 48 NC, 31 AD | 92.8 | |
| Bi et al. [28] | PCC + SVM | rs-fMRI | 36 NC, 25AD | 94.4 | |
| Our | LSRNet | rs-fMRI | 48 NC, 31 AD | 95.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, L.; Hu, Z.; Li, R.; Lu, X.; Li, Z.; Zhang, X.; Xu, S. Multi-Perspective Feature Extraction and Fusion Based on Deep Latent Space for Diagnosis of Alzheimer’s Diseases. Brain Sci. 2022, 12, 1348. https://doi.org/10.3390/brainsci12101348
Gao L, Hu Z, Li R, Lu X, Li Z, Zhang X, Xu S. Multi-Perspective Feature Extraction and Fusion Based on Deep Latent Space for Diagnosis of Alzheimer’s Diseases. Brain Sciences. 2022; 12(10):1348. https://doi.org/10.3390/brainsci12101348
Chicago/Turabian StyleGao, Libin, Zhongyi Hu, Rui Li, Xingjin Lu, Zuoyong Li, Xiabin Zhang, and Shiwei Xu. 2022. "Multi-Perspective Feature Extraction and Fusion Based on Deep Latent Space for Diagnosis of Alzheimer’s Diseases" Brain Sciences 12, no. 10: 1348. https://doi.org/10.3390/brainsci12101348