
Postoperative Hematoma Expansion in Patients Undergoing Decompressive Hemicraniectomy for Spontaneous Intracerebral Hemorrhage
 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Exclusion Criteria
2.3. Neuroimaging
2.4. Hypertension Management
2.5. Statistics
3. Results
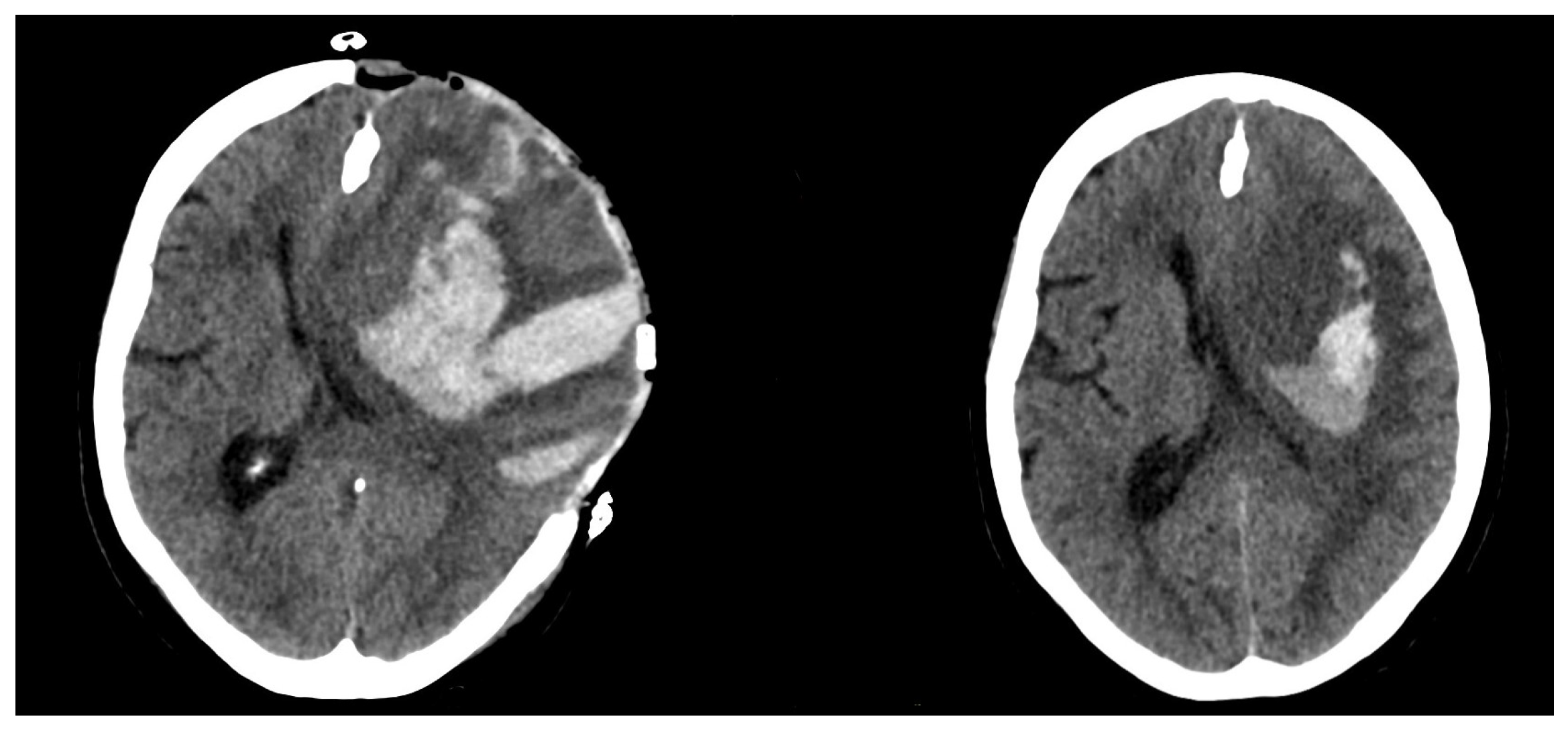
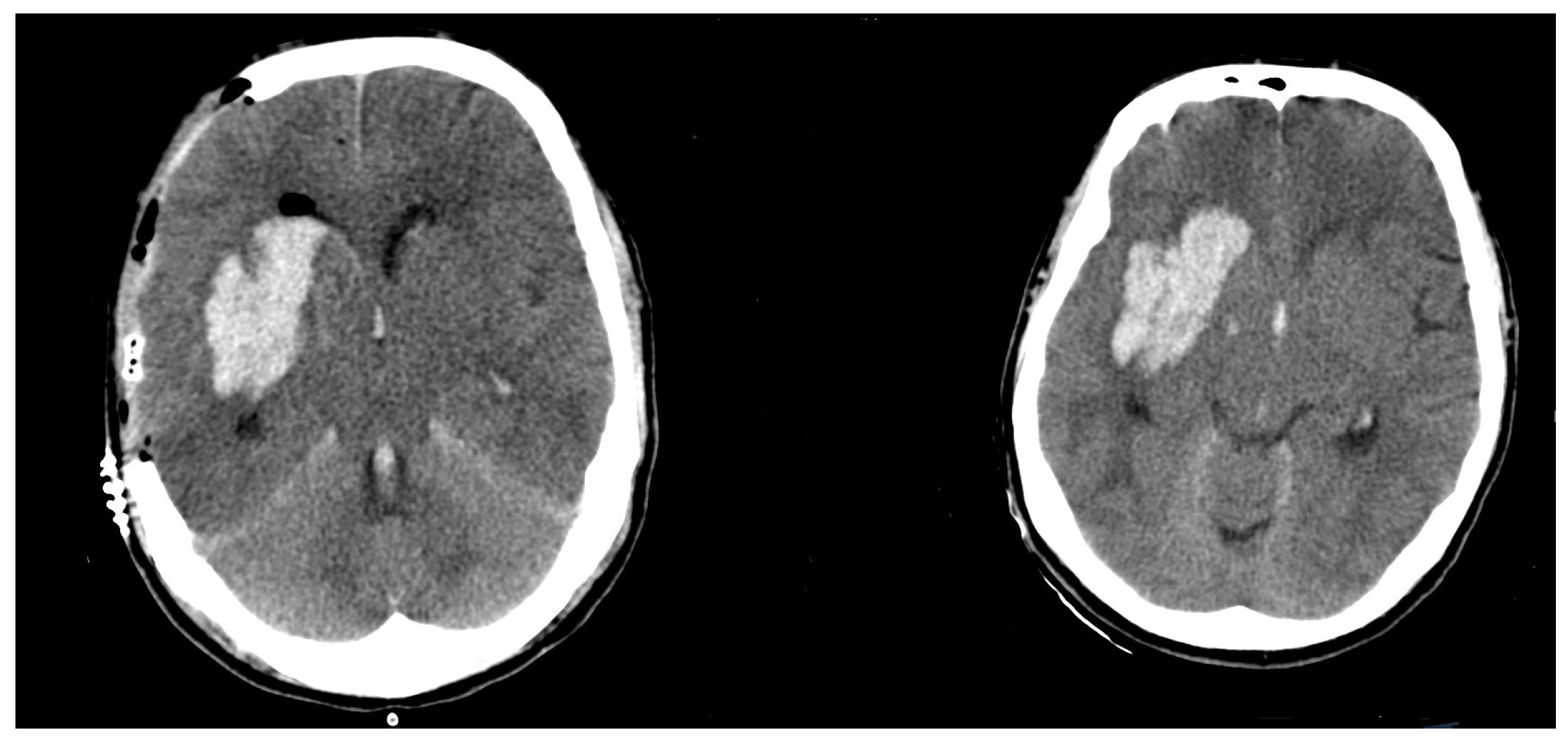
3.1. Preoperative/Postoperative Size Differences
3.2. Anticoagulant/Antiplatelet Medication (AC/AP)
3.3. Age
3.4. Blood Particles
3.5. Coagulation Parameters
3.6. Comorbidities
3.7. Mid-line Shift and DC Size
3.8. Outcome According to Modified Rankin Scale (mRS) 6 Months Postoperatively
3.9. Multivariate Analysis of Univariate Significant Risk Factors
3.10. AC/AP Medication as an Outcome and Mortality Predictor
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Demchuk, A.M.; Dowlatshahi, D.; Rodriguez-Luna, D.; Molina, C.A.; Blas, Y.S.; Dzialowski, I.; Kobayashi, A.; Boulanger, J.M.; Lum, C.; Gubitz, G.; et al. Prediction of haematoma growth and outcome in patients with intracerebral haemorrhage using the CT-angiography spot sign (PREDICT): A prospective observational study. Lancet Neurol. 2012, 11, 307–314. [Google Scholar] [CrossRef]
- Zheng, H.; Chen, C.; Zhang, J.; Hu, Z. Mechanism and Therapy of Brain Edema after Intracerebral Hemorrhage. Cerebrovasc. Dis. 2016, 42, 155–169. [Google Scholar] [CrossRef] [PubMed]
- Hemphill, J.C., III; Greenberg, S.M.; Anderson, C.S.; Becker, K.; Bendok, B.R.; Cushman, M.; Fung, G.L.; Goldstein, J.N.; Macdonald, R.L.; Mitchell, P.H.; et al. American Heart Association Stroke Council; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2015, 46, 2032–2060. [Google Scholar] [PubMed]
- Hadjiathanasiou, A.; Schuss, P.; Ilic, I.; Borger, V.; Vatter, H.; Güresir, E. Decompressive craniectomy for intracerebral haematoma: The influence of additional haematoma evacuation. Neurosurg. Rev. 2018, 41, 649–654. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, S.; Wada, K.; Nagatani, K.; Otani, N.; Mori, K. Decompressive hemicraniectomy for spontaneous intracerebral hemorrhage. Neurosurg. Focus 2013, 34, E5. [Google Scholar] [CrossRef]
- Fung, C.; Murek, M.; Z’Graggen, W.J.; Krähenbühl, A.K.; Gautschi, O.P.; Schucht, P.; Gralla, J.; Schaller, K.; Arnold, M.; Fischer, U.; et al. Decompressive hemicraniectomy in patients with supratentorial intracerebral hemorrhage. Neurosurg. Focus 2012, 43, 3207–3211. [Google Scholar] [CrossRef]
- Gopalakrishnan, M.S.; Shanbhag, N.C.; Shukla, D.P.; Konar, S.K.; Bhat, D.I.; Devi, B.I. Complications of Decompressive Craniectomy. Front. Neurol. 2018, 9, 977. [Google Scholar] [CrossRef]
- Brott, T.; Broderick, J.; Kothari, R.; Barsan, W.; Tomsick, T.; Sauerbeck, L.; Spilker, J.; Duldner, J.; Khoury, J. Early hemorrhage growth in patients with intracerebral hemorrhage. Stroke 1997, 28, 1–5. [Google Scholar] [CrossRef]
- Balami, J.S.; Buchan, A.M. Complications of intracerebral haemorrhage. Lancet Neurol. 2012, 11, 101–118. [Google Scholar] [CrossRef]
- Vahedi, K.; Vicaut, E.; Mateo, J.; Kurtz, A.; Orabi, M.; Guichard, J.P.; Boutron, C.; Couvreur, G.; Rouanet, F.; Touzé, E.; et al. Sequential-design, multicenter, randomized, controlled trial of early decompressive craniectomy in malignant middle cerebral artery infarction (DECIMAL Trial). Stroke 2007, 38, 2506–2517. [Google Scholar] [CrossRef] [Green Version]
- Morgenstern, L.B.; Hemphill, J.C., III; Anderson, C.; Becker, K.; Broderick, J.P.; Connolly, E.S., Jr.; Greenberg, S.M.; Huang, J.N.; Macdonald, R.L.; Messé, S.R.; et al. American Heart Association Stroke Council and Council on Cardiovascular Nursing. Guidelines for the management of spontaneous intracerebral hemorrhage: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2010, 41, 2108–2129. [Google Scholar] [CrossRef] [PubMed]
- Forsting, M.; Reith, W.; Schäbitz, W.R.; Heiland, S.; von Kummer, R.; Hacke, W.; Sartor, K. Decompressive craniectomy for cerebral infarction: An experimental study in rats. Stroke 1995, 26, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Doerfler, A.; Forsting, M.; Reith, W.; Staff, C.; Heiland, S.; Schäbitz, W.R.; von Kummer, R.; Hacke, W.; Sartor, K. Decompressive craniectomy in a rat model of “malignant” cerebral hemispheric stroke: Experimental support for an aggressive therapeutic approach. J. Neurosurg. 1996, 85, 853–859. [Google Scholar] [CrossRef] [PubMed]
- Hofmeijer, J.; Kappelle, L.J.; Algra, A.; Amelink, G.J.; van Gijn, J.; van der Worp, H.B. Surgical decompression for space-occupying cerebral infarction (the Hemicraniectomy After Middle Cerebral Artery infarction with Life-threatening Edema Trial [HAMLET]): A multicentre, open, randomised trial. Lancet Neurol. 2009, 8, 326–333. [Google Scholar] [CrossRef]
- Vychopen, M.; Schneider, M.; Borger, V.; Schuss, P.; Behning, C.; Vatter, H.; Güresir, E. Complete hemispheric exposure vs. superior sagittal sinus sparing craniectomy: Incidence of shear-bleeding and shunt-dependency. Eur. J. Trauma Emerg. Surg. 2021, 48, 2449–2457. [Google Scholar] [CrossRef]
- Güresir, E.; Vatter, H.; Schuss, P.; Oszvald, A.; Raabe, A.; Seifert, V.; Beck, J. Rapid closure technique in decompressive craniectomy. J. Neurosurg. 2011, 114, 954–960. [Google Scholar] [CrossRef]
- Wach, J.; Hamed, M.; Schuss, P.; Güresir, E.; Herrlinger, U.; Vatter, H.; Schneider, M. Impact of initial midline shift in glioblastoma on survival. Neurosurg. Rev. 2021, 44, 1401–1409. [Google Scholar] [CrossRef]
- Boulouis, G.; Morotti, A.; Brouwers, H.B.; Charidimou, A.; Jessel, M.J.; Auriel, E.; Pontes-Neto, O.; Ayres, A.; Vashkevich, A.; Schwab, K.M.; et al. Association between Hypodensities Detected by Computed Tomography and Hematoma Expansion in Patients with Intracerebral Hemorrhage. JAMA Neurol. 2016, 73, 961–968. [Google Scholar] [CrossRef]
- Ho, M.-Y.; Tseng, W.-L.; Xiao, F. Estimation of the Craniectomy Surface Area by Using Postoperative Images. Int. J. Biomed. Imaging 2018, 2018, 5237693. [Google Scholar] [CrossRef]
- Li, Z.; You, M.; Long, C.; Bi, R.; Xu, H.; He, Q.; Hu, B. Hematoma Expansion in Intracerebral Hemorrhage: An Update on Prediction and Treatment. Front. Neurol. 2020, 11, 702. [Google Scholar] [CrossRef]
- Alcusky, M.; McManus, D.D.; Hume, A.L.; Fisher, M.; Tjia, J.; Lapane, K.L. Changes in Anticoagulant Utilization among United States Nursing Home Residents with Atrial Fibrillation from 2011 to 2016. J. Am. Heart Assoc. 2019, 8, e012023. [Google Scholar] [CrossRef]
- Campitelli, M.A.; Bronskill, S.E.; Huang, A.; Maclagan, L.C.; Atzema, C.L.; Hogan, D.B.; Lapane, K.L.; Harris, D.A.; Maxwell, C.J. Trends in Anticoagulant Use at Nursing Home Admission and Variation by Frailty and Chronic Kidney Disease among Older Adults with Atrial Fibrillation. Drugs Aging. 2021, 38, 611–623. [Google Scholar] [CrossRef] [PubMed]
- Mengel, A.; Stefanou, M.I.; Hadaschik, K.A.; Wolf, M.; Stadler, V.; Poli, K.; Lindig, T.; Ernemann, U.; Grimm, F.; Tatagiba, M.; et al. Early Administration of Desmopressin and Platelet Transfusion for Reducing Hematoma Expansion in Patients with Acute Antiplatelet Therapy Associated Intracerebral Hemorrhage. Crit. Care Med. 2020, 48, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- Mayer, S.A.; Brun, N.C.; Begtrup, K.; Broderick, J.; Davis, S.; Diringer, M.N.; Skolnick, B.E.; Steiner, T. Recombinant Activated Factor VII Intracerebral Hemorrhage Trial Investigators. Recombinant activated factor VII for acute intracerebral hemorrhage. N. Engl. J. Med. 2005, 352, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Frontera, J.A.; Lewin, J.J., III; Rabinstein, A.A.; Aisiku, I.P.; Alexandrov, A.W.; Cook, A.M.; del Zoppo, G.J.; Kumar, M.A.; Peerschke, E.I.; Stiefel, M.F.; et al. Guideline for Reversal of Antithrombotics in Intracranial Hemorrhage: A Statement for Healthcare Professionals from the Neurocritical Care Society and Society of Critical Care Medicine. Neurocrit. Care 2016, 24, 6–46. [Google Scholar] [CrossRef] [PubMed]
- Sacks, D.; Baxter, B.; Campbell, B.C.; Carpenter, J.S.; Cognard, C.; Dippel, D.; Eesa, M.; Fischer, U.; Hausegger, K.; Hirsch, J.A. Multisociety Consensus Quality Improvement Revised Consensus Statement for Endovascular Therapy of Acute Ischemic Stroke. Int. J. Stroke 2018, 13, 612–632. [Google Scholar] [CrossRef]
- Song, L.; Sandset, E.C.; Arima, H.; Heeley, E.; Delcourt, C.; Chen, G.; Yang, J.; Wu, G.; Wang, X.; Lavados, P.M.; et al. Early blood pressure lowering in patients with intracerebral haemorrhage and prior use of antithrombotic agents: Pooled analysis of the INTERACT studies. J. Neurol. Neurosurg. Psychiatry 2016, 87, 1330–1335. [Google Scholar] [CrossRef]
- Nasi, D.; Di Somma, L.; Gladi, M.; Moriconi, E.; Scerrati, M.; Iacoangeli, M.; Dobran, M. New or Blossoming Hemorrhagic Contusions after Decompressive Craniectomy in Traumatic Brain Injury: Analysis of Risk Factors. Front. Neurol. 2019, 9, 1186. [Google Scholar] [CrossRef]
- Flint, A.C.; Manley, G.T.; Gean, A.D.; Hemphill, J.C., III; Rosenthal, G. Post-operative expansion of hemorrhagic contusions after unilateral decompressive hemicraniectomy in severe traumatic brain injury. J. Neurotrauma 2008, 25, 503–512. [Google Scholar] [CrossRef]
- Qiu, W.; Guo, C.; Shen, H.; Chen, K.; Wen, L.; Huang, H.; Ding, M.; Sun, L.; Jiang, Q.; Wang, W. Effects of unilateral decompressive craniectomy on patients with unilateral acute post-traumatic brain swelling after severe traumatic brain injury. J. Neurotrauma 2008, 13, R185. [Google Scholar] [CrossRef] [Green Version]
- Jiang, J.Y.; Xu, W.; Li, W.P.; Xu, W.H.; Zhang, J.; Bao, Y.H.; Ying, Y.H.; Luo, Q.Z. Efficacy of standard trauma craniectomy for refractory intracranial hypertension with severe traumatic brain injury: A multicenter, prospective, randomized controlled study. J. Neurotrauma 2005, 22, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Cepeda, S.; Castaño-León, A.M.; Munarriz, P.M.; Paredes, I.; Panero, I.; Eiriz, C.; Gómez, P.A.; Lagares, A. Effect of decompressive craniectomy in the postoperative expansion of traumatic intracerebral hemorrhage: A propensity score-based analysis. J. Neurosurg. 2019, 132, 1623–1635. [Google Scholar] [CrossRef]
- Rodriguez-Luna, D.; Piñeiro, S.; Rubiera, M.; Ribo, M.; Coscojuela, P.; Pagola, J.; Flores, A.; Muchada, M.; Ibarra, B.; Meler, P.; et al. Impact of blood pressure changes and course on hematoma growth in acute intracerebral hemorrhage. Eur. J. Neurol. 2013, 20, 1277–1283. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| ICH Expansion < 6 cm3 (No Expansion) n = 16 | ICH Expansion >= 6 cm3 (Expansion) n = 38 | p Value | |
|---|---|---|---|
| ICH size preoperativ | 87.1 ± 40.8 cm3 | 59.72 ± 27.4 cm3 | n.s. |
| size difference | 65.1 ± 47.9 cm3 | −0.5 ± 4.19 cm3 | p < 0.0001 |
| Midline shift preop. | 11.7 ± 5.8 mm | 10.3 ± 5.5 mm | n.s. |
| Midline shift postop. | 6.9 ± 4.8 mm | 5.8 ± 5.4 mm | n.s. |
| AC/AP Medication (%) | 15/16 (93.75%) | 5/38 (13.15%) | p < 0.00001 |
| DC Size | 218.7 ± 50.2 cm2 | 204.4 ± 44.92 cm2 | n.s. |
| Intraoperative blood loss | 980 ± 804 mL | 784 ± 520 mL | n.s. |
| mRS positive | 0/16 (0%) | 10/38 (26.3%) | p < 0.0001 |
| 30-day mortality | 15/16 (93.75%) | 11/38 (28.9%) | p < 0.0001 |
| Age (years) | 66.7 ± 16.2 | 54.4 ± 12.4 | p = 0.0193 |
| Laboratory results | |||
| Platelets | 219.2 ± 83 | 194.0 ± 88 | n.s. |
| Hematocrit (%) | 34.1 ± 5.4 | 38.1 ± 4.8 | p = 0.0095 |
| Hemoglobin (g/dL) | 11.5 ± 1.6 | 13.13 ± 1.8 | p = 0.0028 |
| Pathological creatinine /Chronic kid-ney failure | 2/16 | 3/38 | n.s. |
| Tranexamic Acid + FFP + Prothrom-bin substitution | 14/16 | 12/38 | n.s. |
| Pathological Quick | 6/16 | 10/38 | n.s. |
| Single factor analysis | |||
| Antitrombin <85% | 7/16 | 19/38 | n.s. |
| F I < (ref. 180–355 mg/dL) | 1/16 | 6/38 | n.s. |
| F II < (ref. 83–145%) | 7/16 | 6/38 | n.s. |
| F V < (ref. 75–152%) | 4/16 | 7/38 | n.s. |
| F VII < (ref. 74–158%) | 5/16 | 10/38 | n.s. |
| F VIII < (ref. 67–220%) | 0/38 | 0/38 | n.s. |
| F X < (ref. 80–140%) | 2/16 | 14/38 | n.s. |
| PFA Test positive | 8/16 | 15/38 | n.s. |
| Hypertension | 12/16 | 30/38 | n.s. 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vychopen, M.; Wach, J.; Lampmann, T.; Asoglu, H.; Borger, V.; Hamed, M.; Vatter, H.; Güresir, E. Postoperative Hematoma Expansion in Patients Undergoing Decompressive Hemicraniectomy for Spontaneous Intracerebral Hemorrhage. Brain Sci. 2022, 12, 1298. https://doi.org/10.3390/brainsci12101298
Vychopen M, Wach J, Lampmann T, Asoglu H, Borger V, Hamed M, Vatter H, Güresir E. Postoperative Hematoma Expansion in Patients Undergoing Decompressive Hemicraniectomy for Spontaneous Intracerebral Hemorrhage. Brain Sciences. 2022; 12(10):1298. https://doi.org/10.3390/brainsci12101298
Chicago/Turabian StyleVychopen, Martin, Johannes Wach, Tim Lampmann, Harun Asoglu, Valeri Borger, Motaz Hamed, Hartmut Vatter, and Erdem Güresir. 2022. "Postoperative Hematoma Expansion in Patients Undergoing Decompressive Hemicraniectomy for Spontaneous Intracerebral Hemorrhage" Brain Sciences 12, no. 10: 1298. https://doi.org/10.3390/brainsci12101298