
(Dys)Prosody in Parkinson’s Disease: Effects of Medication and Disease Duration on Intonation and Prosodic Phrasing

 , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
1.1. Prosody: Structure and Meaning
- (1)
- a. A Maria vem. Mary is coming.b. A Maria vem? Is Mary coming?c. A Maria VEM. Mary is coming (not leaving).
- (2)
- a. A Maria bebeu o vinho. Mary drank the wine.b. A Maria, bebeu o vinho. As for Mary, she drank the wine.
- (3)
- a. (A Maria vem) b. (A Maria vem) c. (A Maria VEM)H + L* L% H + L* LH% H* + L L%
- (4)
- a. (A Maria bebeu o vinho) b. (A Maria) (bebeu o vinho)H + L* L% L* + H H% H + L* L%
1.2. Prosody in Parkinson’s Disease
1.3. Dopaminergic Treatment, Disease Duration, and Prosody
1.4. The Present Study
2. Materials and Methods
2.1. Participants and Assessments
2.2. Materials and Procedure
- (5)
- Topic phrase: (Às alunas) (os amigos ofereceram rosas)To-the students the friends gave roses
- (6)
- Parenthetical phrase: (O Álvaro) (antes de partir) (falou com os amigos)Álvaro before leaving talked to his friends
- (7)
- Enumeration: (Gosto de maçã) (banana) (uvas) (laranja) (e tangerina)(I) like apple banana grape orange and tangerine
- (8)
- Related sentences: (O músico compôs uma cantiga) (Ela inspirou-o)The musician wrote a song She inspired him
- (9)
- Context: Quer que a Marina venha para que o jantar possa ser servido. Chame-a.You want Marina to come so that dinner can be served. So you call her.Target: Marina!
2.3. Prosodic Analysis
2.3.1. Intonation: Sentence Type and Pragmatic Meaning
2.3.2. Prosodic Phrasing
2.4. Statistical Analysis
3. Results
3.1. Intonation Results
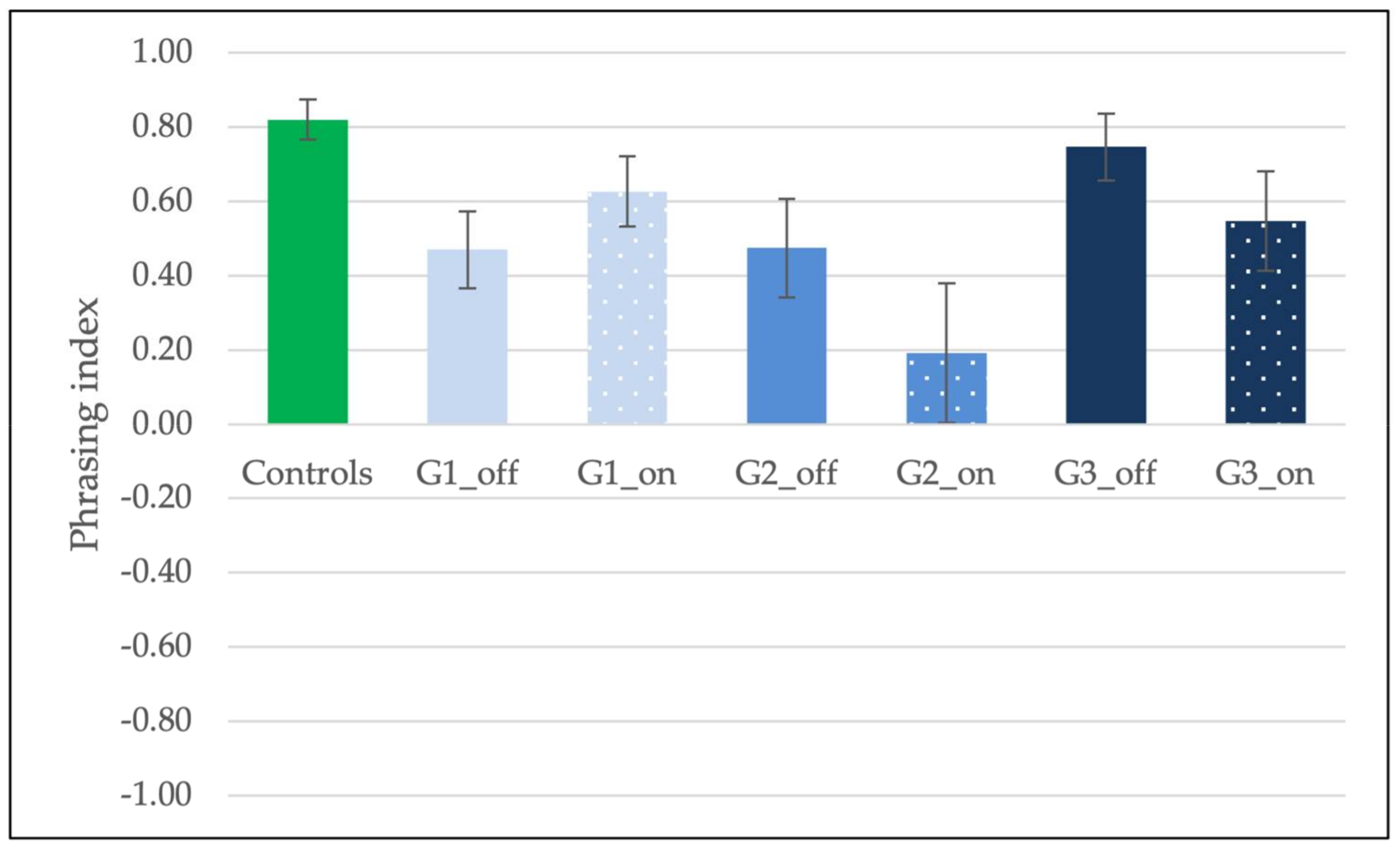
3.2. Prosodic Phrasing Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Set 1
- A loura cantava uma melodia maravilhosa de Espanha.‘The blond girl was singing a wonderful melody from Spain.’
- (C: O senhor/A senhora saiu de casa e viu a rua molhada. Então, perguntou se choveu:) Choveu?‘(C: You went outside and saw that the floor was wet. You then asked whether it had rained.) Did it rain?’
- (C: A Maria está do outro lado da rua e não sabe se vai conseguir chamá-la:) Maria!‘(C: Maria is across the street and you do not know whether you will be able to call her:) Maria!’
- (C: O seu filho, que sempre viveu na costa, regressou de uma longa estadia no interior da Alemanha. Apesar de ele estar muito ocupado, o senhor/a senhora tem um pedido que pensa ser do seu agrado:) Anda ver o mar.‘(C: Your son, who has always lived on the coast, has returned from a long stay in the interior of Germany. Although he is very busy, you have a request that you think he will appreciate:) Come to see the sea.’
- A descida das taxas de juro foi muito elogiada.‘The lowering of interest rates was highly praised.’
- (C: Não faço ideia do que aconteceu.) Ela foi ver a Marina?‘(C: I have no idea about what happened.) Did she go to see Marina?’
- O novo presidente será eleito em Outubro.‘The new president is going to be elected in October.’
- O Álvaro, antes de partir, falou com os amigos.‘Álvaro, before leaving, spoke to his friends.’
- (C: Está a falar com a Júlia sobre os vossos amigos que vão viver para outra cidade. Tem a certeza de que vão para Lisboa, mas a sua amiga pensa que vão para Évora. Diga-lhe que não, que vão para Lisboa.) Eles não vão morar para Évora. Vão para LISBOA!‘(C: You are talking with Júlia about your friends, who will move to another city. You know for sure that they are moving to Lisbon, but your Júlia thinks that they are moving to Évora. Tell her that they are moving to Lisbon.) They are not moving to Évora. They are moving to LISBON!’
- (C: Diga de que frutas gosta mais.) Gosto de maçã, banana, uvas, laranja e tangerina.‘(C: Indicate your favorite fruits.) I love apple, banana, grapes, orange, and tangerine.’
- (C: Gostaria de saber o que se passou.) Os rapazes compraram lâminas?‘(C: I would like to know what happened.) Did the boys buy blades?’
- Espera sentada. A Maria vai demorar.‘Wait seated. Maria will take long.’
- (C: Um amigo do seu filho esqueceu-se do telemóvel em sua casa. Ele acabou de sair e o senhor/a senhora tenta ainda ir a tempo:) Valdemar!‘(C: Your son’s friend has forgotten his mobile at your place. He has just left and you try to make sure you still reach him:) Valdemar!’
- Os artistas foram sempre atraídos pelas cidades.‘The artists were always attracted to the cities.’
- (C: A sua amiga diz que a Maria e o Manuel se separaram, mas você tem a certeza de que eles se casaram. E diz à sua amiga:) Afinal, a Maria e o Manuel não se separaram. Eles CASARAM!‘(C: Your friend is saying that Maria and Manuel got divorced, but you know for sure that they got married. Tell it to your friend:) After all, Maria and Manuel did not get divorced. They GOT MARRIED!’
- Às alunas, os amigos ofereceram rosas.‘To the students, their friends have offered roses.’
- Um quadro de grande valor foi leiloado ontem.‘A valuable painting was auctioned yesterday.’
- Vi, após o tiro, uma pessoa a fugir.‘I saw, after the shooting, someone running away.’
- As alunas estrangeiras nos Açores, até onde sabemos, aceitaram vir.‘The foreigner students in Azores, as far as we know, accepted to come.’
- A inflação subiu cerca de cinco pontos no ano passado.‘The inflation increased five points last year.’
Appendix A.2. Set 2
- A descida das taxas de juro foi muito elogiada.‘The lowering of interest rates was highly praised.’
- Às alunas, os amigos ofereceram rosas.‘To the students, their friends have offered roses.’
- (C: Está a falar com a Maria sobre os vossos amigos que foram viver para outro sítio. Tem a certeza de que mudaram para Lisboa, mas a Maria pensa que mudaram para o Sul. Diga-lhe que não, que mudaram para Lisboa.) Eles não mudaram para o Sul. Mudaram para LISBOA!‘(C: You are talking with Maria about your friends, who have moved to another place. You know for sure that they have moved to Lisbon, but your Maria thinks that they have moved to the South. Tell her that they have moved to Lisbon.) They did not move to the South. They have moved to LISBON!’
- (C: O senhor/A senhora saiu de casa e viu a rua molhada. Então, perguntou se choveu:) Choveu?‘(C: You went outside and you saw that the floor was wet. You then ask whether it rained.) Did it rain?’
- O Álvaro, após o conflito, abandonou a sala.‘Álvaro, after the conflict, left the room.’
- (C: Quer que a Marina venha para que o jantar possa ser servido. Chame-a:) Marina!!‘(C: You want Marina to come so that the dinner can be served. Call her:) Marina!!’
- A inflação subiu cerca de cinco pontos no ano passado.‘The inflation increased five points last year.’
- (C: O seu filho agarrou o jornal que o senhor/a senhora ainda não leu. Tem receio de que ele o rasgue e tenta convencê-lo a devolver o jornal:) Dá-me o jornal.‘(C: Your child grasped the newspaper which you haven’t read yet. You are afraid he destroys it, so you try to convince the child to give it back to you:) Give me the newspaper.’
- O novo presidente será eleito em Outubro.‘The new president is going to be elected in October.’
- (C: Não faço ideia do que aconteceu.) Ela foi ver a Maria?‘(C: I have no idea about what happened.) Did she go to see Maria?’
- As alunas estrangeiras em Chaves, até onde sabemos, adoram comer.‘The foreigner students in Chaves, as far as we know, love to eat.’
- Um quadro de grande valor foi leiloado ontem.‘A valuable painting was auctioned yesterday.’
- (C: O João não o/a viu e o senhor/a senhora precisava mesmo de falar com ele. Está a tentar chamá-lo:) João!‘(C: João did not see you and you really need to talk to him. You are trying to reach his attention:) João!
- Vi, atrás do bandido, um grupo de crianças.‘I saw, chasing a robber, a group of children.’
- (C: A sua amiga diz que os donos do restaurante da sua rua se separaram, mas você tem a certeza de que eles se casaram. E diz à sua amiga:) Os donos do restaurante não se separaram. Eles CASARAM!‘(C: Your friend is saying that the owners of the restaurant in her street got divorced, but you know for sure that they got married. Tell that to your friend:) The owners of the restaurant did not get divorced. They GOT MARRIED!’
- A loura cantava uma melodia maravilhosa de Espanha.‘The blond girl was singing a wonderful melody from Spain.’
- (C: Gostaria de saber o que se passou.) Os rapazes compraram lâminas?‘(C: I would like to know what happened.) Did the boys buy blades?’
- O músico compôs uma cantiga. Ela inspirou-o.‘The musician has written a song. She inspired him.’
- Os artistas foram sempre atraídos pelas cidades.‘The artists were always attracted to the cities.’
- (C: Diga que frutas comprou no mercado:) Comprei laranja, banana, limão, tangerina e cenoura.‘(C: Indicate the fruits you have bought in the market:) I have bought orange, banana, lemon, tangerine, and carrot.’
References
- Gussenhoven, C. Intonation. In The Cambridge Handbook of Phonology; Lacy, P., Ed.; Cambridge University Press: Cambridge, UK, 2007; pp. 253–280. [Google Scholar]
- Ladd, D.R. Intonational Phonology, 2nd ed.; Cambridge University Press: Cambridge, UK, 2008. [Google Scholar]
- Boutsen, F.; Dvorak, J. Prosody and Motor Speech Disorders: A Retrospective Review of a Merger That Is Imminent. Lingua 2017, 199, 50–59. [Google Scholar] [CrossRef]
- Duffy, J. Motor Speech Disorders: Substrates, Differential Diagnosis, and Management, Fourth; Elsevier: Maryland Heights, MO, USA, 2019. [Google Scholar]
- Halliday, M.A.K. Notes on Transitivity and Theme in English: Part 2. J. Linguist. 1967, 3, 199–244. [Google Scholar] [CrossRef]
- Nespor, M.; Vogel, I. Prosodic Phonology: With a New Foreword, Studies in Generative Grammar; Mouton de Gruyter: Berlin, Germany, 2007. [Google Scholar]
- Gussenhoven, C. The Phonology of Tone and Intonation; Cambridge University Press: Cambridge, UK, 2004. [Google Scholar]
- Jun, S.-A. Prosodic Typology: The Phonology of Intonation and Phrasing; Oxford University Press: Oxford, UK, 2005. [Google Scholar] [CrossRef]
- Jun, S.-A. Prosodic Typology II: The Phonology of Intonation and Phrasing; Oxford University Press: Oxford, UK, 2014. [Google Scholar]
- Frota, S.; Prieto, P. Intonation in Romance; Oxford University Press: Oxford, UK, 2015. [Google Scholar] [CrossRef] [Green Version]
- Gussenhoven, C.; Chen, A. The Oxford Handbook of Language Prosody, Oxford Handbooks; Oxford University Press: Oxford, UK, 2020. [Google Scholar]
- Frota, S. The Intonational Phonology of European Portuguese. In Prosodic Typology II: The Phonology of Intonation and Phrasing; Jun, S.-A., Ed.; Oxford University Press: Oxford, UK, 2014; pp. 6–42. [Google Scholar] [CrossRef] [Green Version]
- Frota, S.; Oliveira, P.; Cruz, M.; Vigário, M. P-ToBI: Tools for the Transcription of Portuguese Prosody; Laboratório de Fonética: Lisboa, Portugal, 2015; ISBN 978-989-95713-9-6; Available online: http://labfon.letras.ulisboa.pt/InAPoP/P-ToBI/ (accessed on 19 August 2021).
- Frota, S. Prosody and Focus in European Portuguese: Phonological Phrasing and Intonation; Routledge: London, UK, 2000. [Google Scholar]
- Meireles, J.; Massano, J. Cognitive Impairment and Dementia in Parkinson’s Disease: Clinical Features, Diagnosis, and Management. Front. Neurol. 2012, 3, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartel, W.P.; Van Laar, V.S.; Burton, E.A. Parkinson’s Disease. In Behavioral and Neural Genetics of Zebrafish; Gerlai, R.T., Ed.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 377–412. [Google Scholar] [CrossRef]
- Tysnes, O.-B.; Storstein, A. Epidemiology of Parkinson’s Disease. J. Neural Transm. 2017, 124, 901–905. [Google Scholar] [CrossRef] [PubMed]
- Balestrino, R.; Schapira, A.H.V. Parkinson Disease. Eur. J. Neurol. 2020, 27, 27–42. [Google Scholar] [CrossRef] [PubMed]
- Sapir, S. Multiple Factors Are Involved in the Dysarthria Associated with Parkinson’s Disease: A Review With Implications for Clinical Practice and Research. J. Speech Lang. Hear. Res. 2014, 57, 1330–1343. [Google Scholar] [CrossRef]
- Hlavnička, J.; Tykalová, T.; Čmejla, R.; Klempíř, J.; Růžička, E.; Rusz, J. Dysprosody Differentiate Between Parkinson’s Disease, Progressive Supranuclear Palsy, and Multiple System Atrophy. In Proceedings of the Interspeech 2017, Stockholm, Sweden, 20–24 August 2017; pp. 1844–1848. [Google Scholar] [CrossRef] [Green Version]
- Tjaden, K. Speech and Swallowing in Parkinson’s Disease. Top. Geriatr. Rehabil. 2008, 24, 115–126. [Google Scholar] [CrossRef]
- Harris, R.; Leenders, K.L.; de Jong, B.M. Speech Dysprosody but No Music ‘Dysprosody’ in Parkinson’s Disease. Brain Lang. 2016, 163, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Brabenec, L.; Mekyska, J.; Galaz, Z.; Rektorova, I. Speech Disorders in Parkinson’s Disease: Early Diagnostics and Effects of Medication and Brain Stimulation. J. Neural Transm. 2017, 124, 303–334. [Google Scholar] [CrossRef]
- Godino-Llorente, J.I.; Shattuck-Hufnagel, S.; Choi, J.Y.; Moro-Velázquez, L.; Gómez-García, J.A. Towards the Identification of Idiopathic Parkinson’s Disease from the Speech. New Articulatory Kinetic Biomarkers. PLoS ONE 2017, 12, e0189583. [Google Scholar] [CrossRef] [Green Version]
- Pell, M.; Cheang, H.; Leonard, C. The Impact of Parkinson’s Disease on Vocal-Prosodic Communication from the Perspective of Listeners. Brain Lang. 2006, 97, 123–134. [Google Scholar] [CrossRef] [PubMed]
- Jones, H.N. Prosody in Parkinson’s Disease. Perspect. Neurophysiol. Neurogenic Speech Lang. Disord. 2009, 19, 77–82. [Google Scholar] [CrossRef]
- Cardoso, R.; Guimarães, I.; Santos, H.; Loureiro, R.; Domingos, J.; Abreu, D.; Gonçalves, N.; Pinto, S.; Ferreira, J.J. Psychosocial Impact of Parkinson’s Disease-Associated Dysarthria: Cross-Cultural Adaptation and Validation of the Dysarthria Impact Profile into European Portuguese: EP: DIP Validation for PD. Geriatr. Gerontol. Int. 2018, 18, 767–774. [Google Scholar] [CrossRef]
- Darley, F.L.; Aronson, A.E.; Brown, J.R. Motor Speech Disorders; Saunders: Philadelphia, PA, USA, 1975. [Google Scholar]
- Martens, H.; Van Nuffelen, G.; Cras, P.; Pickut, B.; De Letter, M.; De Bodt, M. Assessment of Prosodic Communicative Efficiency in Parkinson’s Disease As Judged by Professional Listeners. Park. Dis. 2011, 2011, 129310. [Google Scholar] [CrossRef] [Green Version]
- Schulz, G.; Halpern, A.; Spielman, J.; Ramig, L.; Panzer, I.; Sharpley, A.; Freeman, K. Single Word Intelligibility of Individuals with Parkinson’s Disease in Noise: Pre-Specified Secondary Outcome Variables from a Randomized Control Trial (RCT) Comparing Two Intensive Speech Treatments (LSVT LOUD vs. LSVT ARTIC). Brain Sci. 2021, 11, 857. [Google Scholar] [CrossRef]
- Boutsen, F.; Park, E.; Dvorak, J.; Cid, C. Prosodic Improvement in Persons with Parkinson Disease Receiving SPEAK OUT!® Voice Therapy. Folia Phoniatr. Logop. 2018, 70, 51–58. [Google Scholar] [CrossRef]
- Cheang, H.S.; Pell, M.D. An Acoustic Investigation of Parkinsonian Speech in Linguistic and Emotional Contexts. J. Neurolinguistics 2007, 20, 221–241. [Google Scholar] [CrossRef]
- Skodda, S.; Rinsche, H.; Schlegel, U. Progression of Dysprosody in Parkinson’s Disease over Time-A Longitudinal Study. Mov. Disord. 2009, 24, 716–722. [Google Scholar] [CrossRef]
- Skodda, S.; Grönheit, W.; Schlegel, U. Intonation and Speech Rate in Parkinson’s Disease: General and Dynamic Aspects and Responsiveness to Levodopa Admission. J. Voice 2011, 25, e199–e205. [Google Scholar] [CrossRef]
- Tykalova, T.; Rusz, J.; Cmejla, R.; Ruzickova, H.; Ruzicka, E. Acoustic Investigation of Stress Patterns in Parkinson’s Disease. J. Voice 2014, 28, 129.e1–129.e8. [Google Scholar] [CrossRef]
- Thies, T.; Mücke, D.; Lowit, A.; Kalbe, E.; Steffen, J.; Barbe, M.T. Prominence Marking in Parkinsonian Speech and Its Correlation with Motor Performance and Cognitive Abilities. Neuropsychologia 2020, 137, 107306. [Google Scholar] [CrossRef]
- Thies, T.; Mücke, D.; Dano, R.; Barbe, M.T. Levodopa-Based Changes on Vocalic Speech Movements during Prosodic Prominence Marking. Brain Sci. 2021, 11, 594. [Google Scholar] [CrossRef]
- Ma, J.K.-Y.; Whitehill, T.L.; So, S.Y.-S. Intonation Contrast in Cantonese Speakers with Hypokinetic Dysarthria Associated with Parkinson’s Disease. J. Speech Lang. Hear. Res. 2010, 53, 836–849. [Google Scholar] [CrossRef]
- Skodda, S.; Visser, W.; Schlegel, U. Short- and Long-Term Dopaminergic Effects on Dysarthria in Early Parkinson’s Disease. J. Neural Transm. 2010, 117, 197–205. [Google Scholar] [CrossRef]
- Skodda, S.; Grönheit, W.; Mancinelli, N.; Schlegel, U. Progression of Voice and Speech Impairment in the Course of Parkinson’s Disease: A Longitudinal Study. Park. Dis. 2013, 2013, 389195. [Google Scholar] [CrossRef]
- Gili Fivela, B.; Sallustio, V.; Pede, S.; Patrocinio, D. Phonetic Complexity, Speech Accuracy and Intelligibility Assessment of Italian Dysarthric Speech. In Proceedings of the Interspeech 2021, Brno, Czech Republic, 30 August–3 September 2021. [Google Scholar]
- Mennen, I.; Schaeffler, F.; Watt, N.; Miller, N. An Autosegmental-Metrical Investigation of Intonation in People with Parkinson’s Disease. Asia Pac. J. Speech Lang. Hear. 2008, 11, 205–219. [Google Scholar] [CrossRef]
- Lowit, A.; Kuschmann, A. Characterizing Intonation Deficit in Motor Speech Disorders: An Autosegmental–Metrical Analysis of Spontaneous Speech in Hypokinetic Dysarthria, Ataxic Dysarthria, and Foreign Accent Syndrome. J. Speech Lang. Hear. Res. 2012, 55, 1472–1484. [Google Scholar] [CrossRef]
- Lloyd, A.J. Comprehension of Prosody in Parkinson’s Disease. Cortex 1999, 35, 389–402. [Google Scholar] [CrossRef]
- Pell, M.D.; Leonard, C.L. Processing Emotional Tone from Speech in Parkinson’s Disease: A Role for the Basal Ganglia. Cogn. Affect. Behav. Neurosci. 2003, 3, 275–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dara, C.; Monetta, L.; Pell, M.D. Vocal Emotion Processing in Parkinson’s Disease: Reduced Sensitivity to Negative Emotions. Brain Res. 2008, 1188, 100–111. [Google Scholar] [CrossRef]
- Albuquerque, L.; Martins, M.; Coelho, M.; Guedes, L.; Ferreira, J.J.; Rosa, M.; Martins, I.P. Advanced Parkinson Disease Patients Have Impairment in Prosody Processing. J. Clin. Exp. Neuropsychol. 2016, 38, 208–216. [Google Scholar] [CrossRef]
- Martens, H.; Van Nuffelen, G.; Wouters, K.; De Bodt, M. Reception of Communicative Functions of Prosody in Hypokinetic Dysarthria Due to Parkinson’s Disease. J. Park. Dis. 2016, 6, 219–229. [Google Scholar] [CrossRef]
- Basirat, A.; Schwartz, J.-L.; Moreau, C. Word Segmentation Based on Prosody in Parkinson’s Disease. Clin. Linguist. Phon. 2021, 35, 534–541. [Google Scholar] [CrossRef]
- Armstrong, M.J.; Okun, M.S. Diagnosis and Treatment of Parkinson Disease: A Review. JAMA 2020, 323, 548. [Google Scholar] [CrossRef] [PubMed]
- Boucherie, D.M.; Duarte, G.S.; Machado, T.; Faustino, P.R.; Sampaio, C.; Rascol, O.; Ferreira, J.J. Parkinson’s Disease Drug Development Since 1999: A Story of Repurposing and Relative Success. J. Park. Dis. 2021, 11, 421–429. [Google Scholar] [CrossRef]
- Pinto, S.; Ozsancak, C.; Tripoliti, E.; Thobois, S.; Limousin-Dowsey, P.; Auzou, P. Treatments for Dysarthria in Parkinson’s Disease. Lancet Neurol. 2004, 3, 547–556. [Google Scholar] [CrossRef]
- Elfmarková, N.; Gajdoš, M.; Mračková, M.; Mekyska, J.; Mikl, M.; Rektorová, I. Impact of Parkinson’s Disease and Levodopa on Resting State Functional Connectivity Related to Speech Prosody Control. Parkinsonism Relat. Disord. 2016, 22, S52–S55. [Google Scholar] [CrossRef] [PubMed]
- Pinho, P.; Monteiro, L.; de Soares, P.M.F.; Tourinho, L.; Melo, A.; Nóbrega, A.C. Impact of Levodopa Treatment in the Voice Pattern of Parkinson’s Disease Patients: A Systematic Review and Meta-Analysis. CoDAS 2018, 30, e20170200. [Google Scholar] [CrossRef] [PubMed]
- De Azevedo, L.L.; da Reis, C.A.C.; de Souza, I.S.; Cardoso, F.E.C. Prosody and Levodopa in Parkinsons Disease. Arq. Neuropsiquiatr. 2013, 71, 835–840. [Google Scholar] [CrossRef] [Green Version]
- Cameron, D.J.; Pickett, K.A.; Earhart, G.M.; Grahn, J.A. The Effect of Dopaminergic Medication on Beat-Based Auditory Timing in Parkinson’s Disease. Front. Neurol. 2016, 7, 19. [Google Scholar] [CrossRef] [Green Version]
- Pinto, S.; Cardoso, R.; Sadat, J.; Guimarães, I.; Mercier, C.; Santos, H.; Atkinson-Clement, C.; Carvalho, J.; Welby, P.; Oliveira, P.; et al. Dysarthria in Individuals with Parkinson’s Disease: A Protocol for a Binational, Cross-Sectional, Case-Controlled Study in French and European Portuguese (FraLusoPark). BMJ Open 2016, 6, e012885. [Google Scholar] [CrossRef]
- Rusz, J.; Tykalová, T.; Klempíř, J.; Čmejla, R.; Růžička, E. Effects of Dopaminergic Replacement Therapy on Motor Speech Disorders in Parkinson’s Disease: Longitudinal Follow-up Study on Previously Untreated Patients. J. Neural Transm. 2016, 123, 379–387. [Google Scholar] [CrossRef]
- Weiner, W.J. Motor Fluctuations in Parkinson’s Disease. Rev. Neurol. Dis. 2006, 3, 101–108. [Google Scholar]
- Bowen, L.K.; Hands, G.L.; Pradhan, S.; Stepp, C.E. Effects of Parkinson’s Disease on Fundamental Frequency Variability in Running Speech. J. Med. Speech Lang. Pathol. 2013, 21, 235–244. [Google Scholar] [PubMed]
- Gibb, W.R.; Lees, A.J. The Relevance of the Lewy Body to the Pathogenesis of Idiopathic Parkinson’s Disease. J. Neurol. Neurosurg. Amp. Psychiatry 1988, 51, 745. [Google Scholar] [CrossRef] [Green Version]
- Frota, S.; Cruz, M. Interactive Atlas of the Prosody of Portuguese Webplatform, 2012–2015. ISLRN 596-167-619-923-0. Available online: http://labfon.letras.ulisboa.pt/InAPoP/index.html (accessed on 19 August 2021).
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Busner, J.; Targum, S.D. The Clinical Global Impressions Scale: Applying a Research Tool in Clinical Practice. Psychiatry Edgmont Townsh. 2007, 4, 28–37. [Google Scholar]
- Cardoso, R.; Guimarães, I.; Santos, H.; Loureiro, R.; Domingos, J.; de Abreu, D.; Gonçalves, N.; Pinto, S.; Ferreira, J. Frenchay Dysarthria Assessment (FDA-2) in Parkinson’s Disease: Cross-Cultural Adaptation and Psychometric Properties of the European Portuguese Version. J. Neurol. 2017, 264, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Movement Disorder Society Task Force on Rating Scales for Parkinson’s Disease. The Unified Parkinson’s Disease Rating Scale (UPDRS): Status and Recommendations. Mov. Disord. 2003, 18, 738–750. [Google Scholar] [CrossRef]
- Tomlinson, C.L.; Stowe, R.; Patel, S.; Rick, C.; Gray, R.; Clarke, C.E. Systematic Review of Levodopa Dose Equivalency Reporting in Parkinson’s Disease: Systematic Review of LED Reporting in PD. Mov. Disord. 2010, 25, 2649–2653. [Google Scholar] [CrossRef] [PubMed]
- Schade, S.; Mollenhauer, B.; Trenkwalder, C. Levodopa Equivalent Dose Conversion Factors: An Updated Proposal Including Opicapone and Safinamide. Mov. Disord. Clin. Pract. 2020, 7, 343–345. [Google Scholar] [CrossRef]
- Frota, S.; Cruz, M.; Fernandes, S.; Collischonn, G.; Fonseca, A.; Serra, C.; Oliveira, P.; Vigário, M. Intonational Variation in Portuguese: European and Brazilian Varieties. In Intonation in Romance; Frota, S., Prieto, P., Eds.; Oxford University Press: Oxfrod, UK, 2015; pp. 235–283. [Google Scholar]
- Boersma, P.; Weenink, D. Praat-Doing Phonetics by Computer. 1992–2021. Available online: www.fon.hum.uva.nl/praat/ (accessed on 19 August 2021).
- Frota, S. Surface and Structure: Transcribing Intonation within and across Languages. Lab. Phonol. 2016, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Frota, S.; Vigário, M. Syntax–Phonology Interface. In Oxford Research Encyclopedia of Linguistics; Aronoff, M., Ed.; Oxford University Press: Oxford, UK, 2018. [Google Scholar] [CrossRef]
- Sammler, D.; Grosbras, M.-H.; Anwander, A.; Bestelmeyer, P.E.G.; Belin, P. Dorsal and Ventral Pathways for Prosody. Curr. Biol. 2015, 25, 3079–3085. [Google Scholar] [CrossRef] [Green Version]
- Sammler, D.; Cunitz, K.; Gierhan, S.M.E.; Anwander, A.; Adermann, J.; Meixensberger, J.; Friederici, A.D. White Matter Pathways for Prosodic Structure Building: A Case Study. Brain Lang. 2018, 183, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Rusz, J.; Hlavnička, J.; Novotný, M.; Tykalová, T.; Pelletier, A.; Montplaisir, J.; Gagnon, J.; Dušek, P.; Galbiati, A.; Marelli, S.; et al. Speech Biomarkers in Rapid Eye Movement Sleep Behavior Disorder and Parkinson Disease. Ann. Neurol. 2021, 90, 62–75. [Google Scholar] [CrossRef] [PubMed]
- Frota, S. The Prosody of Focus: A Case-Study with Cross-Linguistic Implications. In Proceedings of the Speech Prosody 2002, Aix en Provence, France, 11–13 April 2002. [Google Scholar]
- Maskikit-Essed, R.; Gussenhoven, C. No Stress, No Pitch Accent, No Prosodic Focus: The Case of Ambonese Malay. Phonology 2016, 33, 353–389. [Google Scholar] [CrossRef]
- Pinto, S.; Chan, A.; Guimarães, I.; Rothe-Neves, R.; Sadat, J. A Cross-Linguistic Perspective to the Study of Dysarthria in Parkinson’s Disease. J. Phon. 2017, 64, 156–167. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | Healthy Controls | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| ID | Gender | Age | Disease Duration (Years) | MDS-UPDRS III (OFF) | MDS-UPDRS III (ON) | LED | ID | Gender | Age |
| PD01 | M | 65 | 3 | 21 | 19 | 100 | C01 | F | 74 |
| PD02 | F | 58 | 1 | 35 | 30 | --- * | C02 | M | 59 |
| PD03 | F | 59 | 3 | 29 | 23 | 370 | C03 | F | 51 |
| PD04 | M | 59 | 3 | 32 | 29 | 150 | C04 | F | 74 |
| PD05 | F | 71 | 1 | 23 | 16 | 80 | C05 | M | 73 |
| PD06 | F | 80 | 2 | 46 | 36 | 100 | C06 | F | 63 |
| PD07 | F | 52 | 2 | 29 | 23 | 260 | C07 | M | 64 |
| PD08 | F | 70 | <1 | 43 | 43 | --- * | C08 | F | 59 |
| PD09 | M | 82 | 3 | 70 | 65 | 125 | C09 | F | 68 |
| PD10 | M | 67 | 1 | 37 | 30 | 100 | C10 | F | 50 |
| PD11 | F | 40 | 5 | 38 | 19 | 500 | C11 | M | 62 |
| PD12 | F | 64 | 4 | 18 | 11 | 420 | C12 | F | 43 |
| PD13 | M | 72 | 4 | 34 | 22 | 100 | C13 | M | 65 |
| PD14 | M | 72 | 5 | 48 | 37 | 290 | C14 | M | 62 |
| PD15 | F | 60 | 4 | 64 | 43 | --- * | C15 | M | 66 |
| PD16 | M | 73 | 7 | 26 | 22 | --- * | C16 | M | 54 |
| PD17 | F | 54 | 8 | 29 | 24 | 300 | C17 | F | 44 |
| PD18 | F | 41 | 6 | 43 | 15 | 360 | C18 | F | 63 |
| PD19 | F | 56 | 7 | 27 | 24 | 100 | C19 | M | 52 |
| PD20 | M | 48 | 8 | 48 | 38 | 416 | C20 | M | 54 |
| PD21 | M | 79 | 15 | 75 | 43 | 200 | |||
| PD22 | M | 70 | 16 | 60 | 40 | 200 | |||
| PD23 | F | 65 | 10 | 30 | 21 | 240 | |||
| PD24 | F | 74 | 23 | 26 | 27 | --- * | |||
| PD25 | M | 53 | 15 | 56 | 49 | 570 | |||
| PD26 | F | 61 | 13 | 38 | 19 | 100 | |||
| PD27 | M | 63 | 13 | 64 | 43 | 460 | |||
| PD28 | M | 52 | 15 | 35 | 27 | 626 | |||
| PD29 | M | 73 | 16 | 28 | 29 | 530 | |||
| PD30 | M | 73 | 14 | 34 | 28 | 200 | |||
| Mean | --- | 63.4 | 7.6 | 39.5 | 29.8 | 275.9 | --- | --- | 60.0 |
| SD | --- | (10.9) | (6.0) | (15.1) | (11.8) | (170.3) | --- | --- | (9.2) |
| Labels | Realization | Context/Meaning/Usage |
|---|---|---|
| H+L* L% |  | Broad focus statements |
| H*+L L% |  | Contrastive focus |
| H*+L L% |  | Imperative sentences (commands) |
| L*+H L% | ||
| H+L* LH% |  | Interrogative sentences (yes–no questions) |
| L+H* !H% |  | Calling sentences (first call) |
| Deviance | Broad Focus Statement | Contrastive Focus | Command | Yes–No Question | Calling |
|---|---|---|---|---|---|
| D1 (non-deviant) | H+L* L% | H*+L L% | H*+L L%/L*+H L% | Falling–rising | L+H* !H% |
| D2 (less deviant) | L* L% | ¡H+H* L% | --- | All–rising | --- |
| D3 (more deviant) | --- | H+L* L% | L* L% | Rising–falling | L+H* L% |
| D4 (highly deviant) | --- | H* !H% | --- | All–falling | H*+L !H%/L*+H H% |
| Deviance | Position | Equation |
|---|---|---|
| D1 | 1 to 0.5 | 0.5 + D*0.5/100 |
| D2 | 0.5 to 0 | 0.5 − D*0.5/100 |
| D3 | 0 to −0.5 | 0 + D* − 0.5/100 |
| D4 | −0.5 to −1 | −0.5 + D* − 0.5/100 |
| Patients | |||
|---|---|---|---|
| Group | Gender | Age | Disease Duration (Years) |
| G1 | 6F/4M | 66.30 (9.73) | 1.95 (1.01) |
| G2 | 6F/4M | 58.00 (12.43) | 5.80 (1.62) |
| G3 | 3F/7M | 66.30 (9.10) | 15.00 (3.33) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frota, S.; Cruz, M.; Cardoso, R.; Guimarães, I.; Ferreira, J.J.; Pinto, S.; Vigário, M. (Dys)Prosody in Parkinson’s Disease: Effects of Medication and Disease Duration on Intonation and Prosodic Phrasing. Brain Sci. 2021, 11, 1100. https://doi.org/10.3390/brainsci11081100
Frota S, Cruz M, Cardoso R, Guimarães I, Ferreira JJ, Pinto S, Vigário M. (Dys)Prosody in Parkinson’s Disease: Effects of Medication and Disease Duration on Intonation and Prosodic Phrasing. Brain Sciences. 2021; 11(8):1100. https://doi.org/10.3390/brainsci11081100
Chicago/Turabian StyleFrota, Sónia, Marisa Cruz, Rita Cardoso, Isabel Guimarães, Joaquim J. Ferreira, Serge Pinto, and Marina Vigário. 2021. "(Dys)Prosody in Parkinson’s Disease: Effects of Medication and Disease Duration on Intonation and Prosodic Phrasing" Brain Sciences 11, no. 8: 1100. https://doi.org/10.3390/brainsci11081100