
Electrophysiological Studies of Cognitive Reappraisal Success and Failure in aMCI


Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment, Inclusion Criteria, and Participants
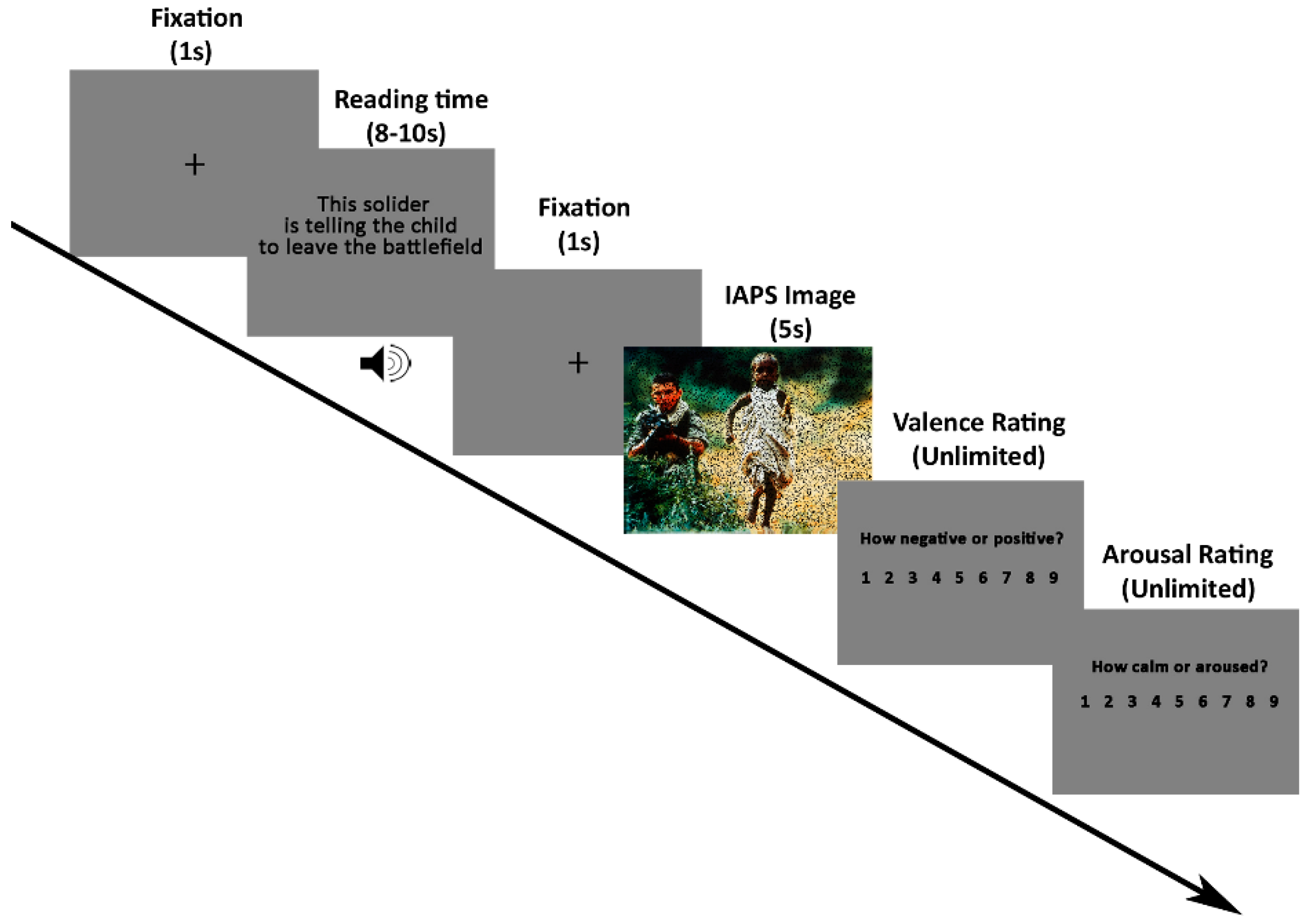
2.2. Stimuli and Procedure
2.3. Behavioral Criteria for Grouping
2.4. EEG Recording and Data Preprocessing
2.5. Statistical Analyses
2.5.1. Behavioral Data
2.5.2. Event-Related Spectral Perturbation Analyses
2.5.3. LPP Analyses
3. Results
3.1. MMSE Scores
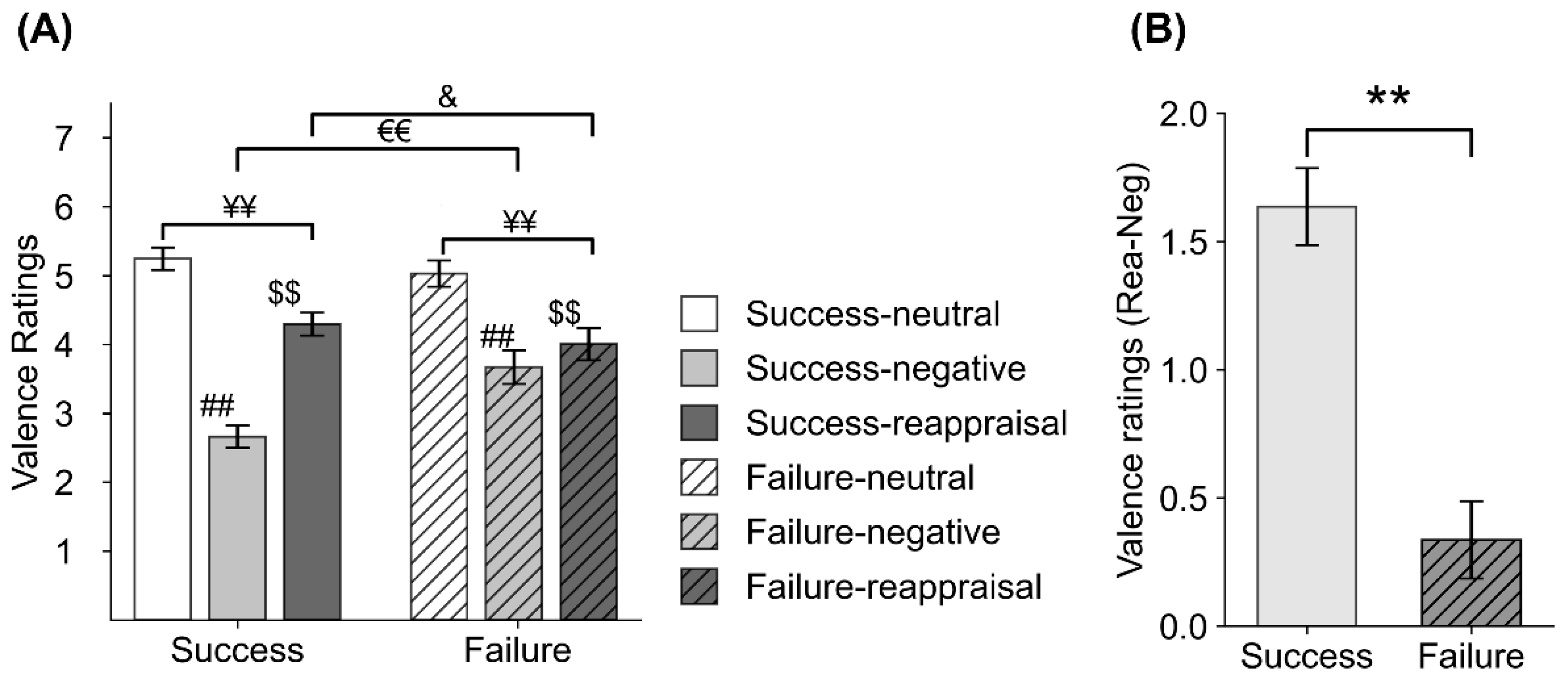
3.2. Behavioral Data
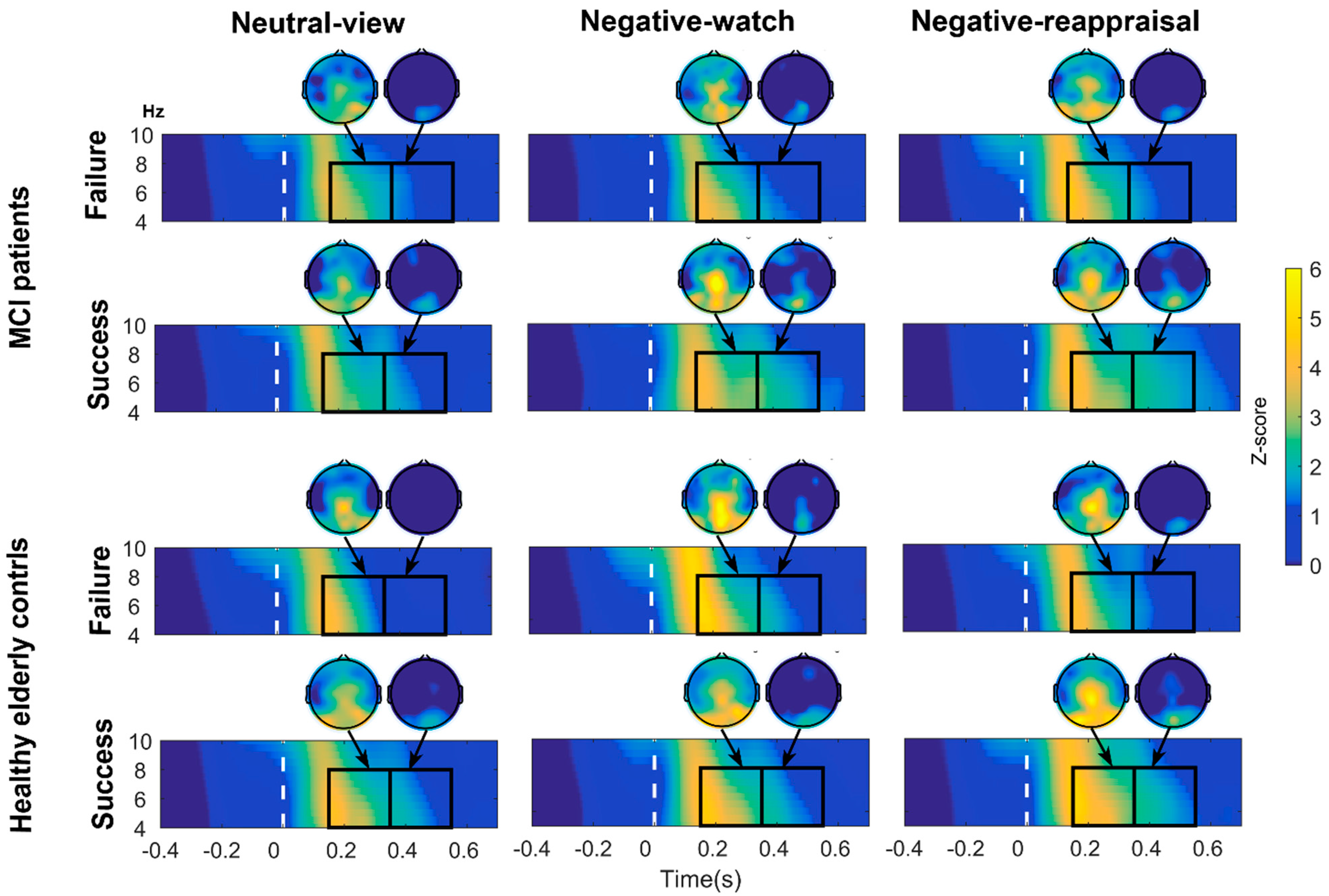
3.3. Regional ERSP for the Theta Band
- In the MCI group, follow-up ANOVAs (within-subjects factor: Condition) were performed separately in the MCI-Success and MCI-Failure groups. A significant effect of condition was found for MCI-Success subjects (F(2,40) = 4.841, p = 0.013, η2p = 0.195), indicating that theta power was stronger in the Neg and Rea conditions than in the Neut condition (p = 0.012 and p = 0.055, respectively). Independent t-tests conducted in each condition revealed that in the Neg and Rea conditions, MCI-Success subjects showed stronger theta power than MCI-Failure subjects (t = −2.074, p = 0.044 and t = −2.362, p = 0.023, respectively).
- In the HEC group, follow-up ANOVAs (within-subjects factor: Condition) were performed separately in the HEC-Success and HEC-Failure groups. A significant effect of condition was found for HEC-Failure subjects (F(2,50) = 8.543, p = 0.001, η2p = 0.255), suggesting that theta power was stronger in the Neg and Rea conditions than in the Neut condition (p = 0.004 and p = 0.018, respectively). Independent t-tests performed in each condition revealed that HEC-Success subjects showed stronger theta spectral power than HEC-Failure subjects in the Neut and Rea conditions (t = −4.073, p < 0.001 and t = −2.921, p = 0.005, respectively).
3.4. LPP Data Results
3.4.1. Window 1 (450–1200 ms)
- In MCI subjects, ANOVAs (within-subjects factor: Condition) were conducted separately in the MCI-Success and MCI-Failure groups. We found a condition effect in both the MCI-Success group (F(2,44) = 9.41, p < 0.001, η2p = 0.3) and MCI-Failure group (F(2,40) = 25.531, ε = 0.773, p < 0.001, η2p = 0.561). The LPP of MCI-Success subjects was more positive in the Neg and Rea condition than in the Neut condition (p < 0.001, respectively), while the LPP of MCI-Failure subjects was more positive in the Neg condition than in the Neut (p = 0.001) and Rea (p = 0.016) condition.
- The ANOVA test in the success group revealed a condition effect in the HEC-success group (F(2,90) = 33.421, p < 0.001, η2p = 0.426), indicating that the LPP evoked by Neg stimuli was significantly larger than the LPP evoked by Rea and Neut stimuli (p = 0.003 and p < 0.001, respectively) and that the LPP elicited by Rea stimuli was significantly larger than the LPP elicited by Neut stimuli (p = 0.001). The condition effect in the MCI-Success group was described in the previous paragraph. Independent t-tests indicated that the LPP for Neut stimuli was larger in the HEC-Success group than in the MCI-Success group (t = −2.213, p = 0.030).
3.4.2. Window 2 (1200–3500 ms)
- As for MCI, ANOVA tests (within-subjects factor: Condition) were conducted separately in the MCI-Success and MCI-Failure groups. A significant effect of condition was found for MCI-Success subjects (F(2,40) = 16.049, ε = 0.768, p < 0.001, η2p = 0.445), indicating that the LPP to Rea stimuli were significantly larger than to Neut (p < 0.001) and Neg stimuli (p = 0.045), and the LPP to Neg stimuli were more positive than to Neut stimuli (p = 0.008).
- As for HEC, ANOVA tests were performed separately for HEC-Success and HEC-Failure subjects. We found a condition effect in the HEC-Success group (F(2,90) = 10.28, p < 0.001, η2p = 0.186), suggesting that the LPP was more positive to Neg stimuli than to Neut stimuli (p < 0.001). Independent t-tests indicated that subjects in the HEC-Success group showed a larger LPP for Neg pictures relative to subjects in the HEC-Failure group (t = −3.232, p = 0.002).
- In the success group, independent t-tests were performed in each condition. The results revealed that subjects in the HEC-Success group showed a larger LPP for Neg and Neut stimuli than subjects in the MCI-Failure group (t = −2.691, p = 0.009; t = −3.164, p = 0.002, respectively).
3.4.3. Window 3 (3500–5000 ms)
3.4.4. The LPP Difference (Rea–Neg)
3.5. Partial Correlation Analyses Results
4. Discussion
4.1. Suppressed Negative Feelings on Negative Images in Both the MCI-Failure and HEC-Failure Groups
4.2. Theta Oscillations Differed between Groups at the Early Perception Stage
4.3. Enhanced LPP for Reappraisal of Negative Pictures in the MCI-Success Group Represents a Compensatory Effort
4.4. Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lu, Y.; Liu, C.; Yu, D.; Fawkes, S.; Ma, J.; Zhang, M.; Li, C. Prevalence of mild cognitive impairment in community-dwelling Chinese populations aged over 55 years: A meta-analysis and systematic review. BMC Geriatr. 2021, 21, 10. [Google Scholar] [CrossRef] [PubMed]
- Yaffe, K.; Petersen, R.C.; Lindquist, K.; Kramer, J.; Miller, B. Subtype of mild cognitive impairment and progression to dementia and death. Dement. Geriatr. Cogn. Disord. 2006, 22, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Doody, R.; Kurz, A.; Mohs, R.C.; Morris, J.C.; Rabins, P.V.; Ritchie, K.; Rossor, M.; Thal, L.; Winblad, B. Current concepts in mild cognitive impairment. Arch. Neurol. 2001, 58, 1985–1992. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Roberts, R.O.; Knopman, D.S.; Boeve, B.F.; Geda, Y.E.; Ivnik, R.J.; Smith, G.E.; Jack, C.R. Mild cognitive impairment: Ten years later. Arch. Neurol. 2009, 66, 1447–1455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Gálvez, A.; Jarén-Galán, M.; Garrido-Fernández, J.; Calvo, M.V.; Visioli, F.; Fontecha, J. Activities, bioavailability, and metabolism of lipids from structural membranes and oils: Promising research on mild cognitive impairment. Pharmacol. Res. 2018, 134, 299–304. [Google Scholar] [CrossRef]
- Peters, M.E.; Rosenberg, P.B.; Steinberg, M.; Tschanz, J.T.; Norton, M.C.; Welsh-Bohmer, K.A.; Hayden, K.M.; Breitner, J.C.S.; Lyketsos, C.G. Prevalence of neuropsychiatric symptoms in CIND and its subtypes: The cache county study. Am. J. Geriatr. Psychiatry 2012, 20, 416–424. [Google Scholar] [CrossRef] [Green Version]
- Ma, L. Depression, Anxiety, and Apathy in Mild Cognitive Impairment: Current Perspectives. Front. Aging Neurosci. 2020, 12, 9. [Google Scholar] [CrossRef] [Green Version]
- Cerejeira, J.; Lagarto, L.; Mukaetova-Ladinska, E.B. Behavioral and psychological symptoms of dementia. Front. Neurol. 2012, 3, 73. [Google Scholar] [CrossRef] [Green Version]
- Palmer, K.; Berger, A.K.; Monastero, R.; Winblad, B.; Bäckman, L.; Fratiglioni, L. Predictors of progression from mild cognitive impairment to Alzheimer disease. Neurology 2007, 68, 1596–1602. [Google Scholar] [CrossRef] [Green Version]
- Mroczek, D.K. Age and emotion in adulthood. Curr. Dir. Psychol. Sci. 2001, 10, 87–90. [Google Scholar] [CrossRef]
- Knight, M.; Seymour, T.L.; Gaunt, J.T.; Baker, C.; Nesmith, K.; Mather, M. Aging and Goal-Directed Emotional Attention: Distraction Reverses Emotional Biases. Emotion 2007, 7, 705–714. [Google Scholar] [CrossRef] [Green Version]
- Brose, A.; De Roover, K.; Ceulemans, E.; Kuppens, P. Older Adults’ Affective Experiences Across 100 Days Are Less Variable and Less Complex Than Younger Adults’. Psychol. Aging 2015, 30, 194–208. [Google Scholar] [CrossRef] [Green Version]
- Nashiro, K.; Sakaki, M.; Mather, M. Age differences in brain activity during emotion processing: Reflections of age-related decline or increased emotion regulation? Gerontology 2012, 58, 156–163. [Google Scholar] [CrossRef] [Green Version]
- Sasse, L.K.; Gamer, M.; Büchel, C.; Brassen, S. Selective control of attention supports the positivity effect in aging. PLoS ONE 2014, 9, e104180. [Google Scholar] [CrossRef]
- Klein-Koerkamp, Y.; Baciu, M.; Hot, P. Preserved and impaired emotional memory in Alzheimer’s disease. Front. Psychol. 2012, 3, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waring, J.D.; Dimsdale-zucker, H.R.; Flannery, S.; Kensinger, E.A. Effects of Mild Cognitive Impairment on Emotional Scene Memory. Neuropsychologia 2017, 96, 240–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meltzer, E.P. Emotion Regulation in Relation to Cognitive Functioning in the Preclinical Stages of Dementia. Ph.D. Thesis, City University of New York, New York, NY, USA, 2016. [Google Scholar]
- Boehme, S.; Biehl, S.C.; Mühlberger, A. Effects of differential strategies of emotion regulation. Brain Sci. 2019, 9, 225. [Google Scholar] [CrossRef] [Green Version]
- Hermann, A.; Kress, L.; Stark, R. Neural correlates of immediate and prolonged effects of cognitive reappraisal and distraction on emotional experience. Brain Imaging Behav. 2017, 11, 1227–1237. [Google Scholar] [CrossRef] [Green Version]
- Richards, J.M.; Gross, J.J. Emotion regulation and memory: The cognitive costs of keeping one’s cool. J. Personal. Soc. Psychol. 2000, 79, 410–424. [Google Scholar] [CrossRef]
- Ferreira, S.; Pêgo, J.M.; Morgado, P. A Systematic Review of Behavioral, Physiological, and Neurobiological Cognitive Regulation Alterations in Obsessive-Compulsive Disorder. Brain Sci. 2020, 10, 797. [Google Scholar] [CrossRef]
- Gross, J.J. Emotion regulation: Affective, cognitive, and social consequences. Psychophysiology 2002, 39, 281–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morawetz, C.; Bode, S.; Derntl, B.; Heekeren, H.R. The effect of strategies, goals and stimulus material on the neural mechanisms of emotion regulation: A meta-analysis of fMRI studies. Neurosci. Biobehav. Rev. 2017, 72, 111–128. [Google Scholar] [CrossRef]
- Ochsner, K.N.; Silvers, J.A.; Buhle, J.T. Functional imaging studies of emotion regulation: A synthetic review and evolving model of the cognitive control of emotion. Ann. N. Y. Acad. Sci. 2012, 1251, E1–E24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morawetz, C.; Riedel, M.C.; Salo, T.; Berboth, S.; Eickhoff, S.B.; Laird, A.R.; Kohn, N. Multiple large-scale neural networks underlying emotion regulation. Neurosci. Biobehav. Rev. 2020, 116, 382–395. [Google Scholar] [CrossRef]
- Nejati, V.; Majdi, R.; Salehinejad, M.A.; Nitsche, M.A. The role of dorsolateral and ventromedial prefrontal cortex in the processing of emotional dimensions. Sci. Rep. 2021, 11, 1971. [Google Scholar] [CrossRef]
- Guarino, A.; Forte, G.; Giovannoli, J.; Casagrande, M. Executive functions in the elderly with mild cognitive impairment: A systematic review on motor and cognitive inhibition, conflict control and cognitive flexibility. Aging Ment. Health 2020, 24, 1028–1045. [Google Scholar] [CrossRef]
- Berger, N.; Richards, A.; Davelaar, E.J. When Emotions Matter: Focusing on Emotion Improves Working Memory Updating in Older Adults. Front. Psychol. 2017, 8, 1565. [Google Scholar] [CrossRef] [Green Version]
- Lohani, M.; Isaacowitz, D.M. Age differences in managing response to sadness elicitors using attentional deployment, positive reappraisal and suppression. Cogn. Emot. 2014, 28, 678–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Opitz, P.C.; Rauch, L.C.; Terry, D.P.; Urry, H.L. Prefrontal mediation of age differences in cognitive reappraisal. Neurobiol. Aging 2012, 33, 645–655. [Google Scholar] [CrossRef]
- Lewis, M.D. Bridging emotion theory and neurobiology through dynamic systems modeling. Behav. Brain Sci. 2005, 28, 169–194. [Google Scholar] [CrossRef]
- Başar, E.; Güntekin, B.; Öniz, A. Principles of oscillatory brain dynamics and a treatise of recognition of faces and facial expressions. In Event-Related Dynamics of Brain Oscillations; Neuper, C., Klimesch, W., Eds.; Progress in Brain Research; Elsevier: Amsterdam, The Netherlands, 2006; Volume 159, pp. 43–62. [Google Scholar]
- Zhang, W.; Li, X.; Liu, X.; Duan, X.; Wang, D.; Shen, J. Distraction reduces theta synchronization in emotion regulation during adolescence. Neurosci. Lett. 2013, 550, 81–86. [Google Scholar] [CrossRef]
- von Stein, A.; Sarnthein, J. Different frequencies for different scales of cortical integration: From local gamma to long range alpha/theta synchronization. Int. J. Psychophysiol. 2000, 38, 301–313. [Google Scholar] [CrossRef]
- Varela, F.; Lachaux, J.P.; Rodriguez, E.; Martinerie, J. The brainweb: Phase synchronization and large-scale integration. Nat. Rev. Neurosci. 2001, 2, 229–239. [Google Scholar] [CrossRef]
- Uusberg, A.; Thiruchselvam, R.; Gross, J.J. Using distraction to regulate emotion: Insights from EEG theta dynamics. Int. J. Psychophysiol. 2014, 91, 254–260. [Google Scholar] [CrossRef]
- Knyazev, G.G.; Slobodskoj-Plusnin, J.Y.; Bocharov, A.V. Event-related delta and theta synchronization during explicit and implicit emotion processing. Neuroscience 2009, 164, 1588–1600. [Google Scholar] [CrossRef] [PubMed]
- Knyazev, G.G.; Slobodskoj-plusnin, J.Y.; Bocharov, A.V. Gender Differences in Implicit and Explicit Processing of Emotional Facial Expressions as Revealed by Event-Related Theta Synchronization. Emotion 2010, 10, 678–687. [Google Scholar] [CrossRef] [PubMed]
- Hajcak, G.; Macnamara, A.; Olvet, D.M. Event-related potentials, emotion, and emotion regulation: An integrative review. Dev. Neuropsychol. 2010, 35, 129–155. [Google Scholar] [CrossRef] [PubMed]
- Bernat, E.M.; Cadwallader, M.; Seo, D.; Vizueta, N.; Patrick, C.J. Effects of instructed emotion regulation on valence, arousal, and attentional measures of affective processing. Dev. Neuropsychol. 2011, 36, 493–518. [Google Scholar] [CrossRef] [PubMed]
- Thiruchselvam, R.; Blechert, J.; Sheppes, G.; Rydstrom, A.; Gross, J.J. The temporal dynamics of emotion regulation: An EEG study of distraction and reappraisal. Biol. Psychol. 2011, 87, 84–92. [Google Scholar] [CrossRef]
- Baker, J.C.; Williams, J.K.; Witvliet, C.V.O.; Hill, P.C. Positive reappraisals after an offense: Event-related potentials and emotional effects of benefit-finding and compassion. J. Posit. Psychol. 2017, 12, 373–384. [Google Scholar] [CrossRef]
- Parvaz, M.A.; MacNamara, A.; Goldstein, R.Z.; Hajcak, G. Event-related induced frontal alpha as a marker of lateral prefrontal cortex activation during cognitive reappraisal. Cogn. Affect. Behav. Neurosci. 2012, 12, 730–740. [Google Scholar] [CrossRef] [Green Version]
- MacNamara, A.; Foti, D.; Hajcak, G. Tell Me About It: Neural Activity Elicited by Emotional Pictures and Preceding Descriptions. Emotion 2009, 9, 531–543. [Google Scholar] [CrossRef] [Green Version]
- Foti, D.; Hajcak, G. Deconstructing reappraisal: Descriptions preceding arousing pictures modulate the subsequent neural response. J. Cogn. Neurosci. 2008, 20, 977–988. [Google Scholar] [CrossRef]
- Hajcak, G.; Nieuwenhuis, S. Reappraisal modulates the electrocortical response to unpleasant pictures. Cogn. Affect. Behav. Neurosci. 2006, 6, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Baur, R.; Conzelmann, A.; Wieser, M.J.; Pauli, P. Spontaneous emotion regulation: Differential effects on evoked brain potentials and facial muscle activity. Int. J. Psychophysiol. 2015, 96, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Langeslag, S.J.E.; van Strien, J.W. Comparable modulation of the late positive potential by emotion regulation in younger and older adults. J. Psychophysiol. 2010, 24, 186–197. [Google Scholar] [CrossRef]
- Langeslag, S.J.E.; Surti, K. The effect of arousal on regulation of negative emotions using cognitive reappraisal: An ERP study. Int. J. Psychophysiol. 2017, 118, 18–26. [Google Scholar] [CrossRef]
- Cao, D.; Li, Y.; Niznikiewicz, M.A. Neural characteristics of cognitive reappraisal success and failure: An ERP study. Brain Behav. 2020, 10, e01584. [Google Scholar] [CrossRef]
- Morris, J.C. The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology 1993, 43, 2412–2414. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Hamilton, M.A.X. The assessment of anxiety states by rating. Br. J. Med. Psychol. 1959, 32, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56. [Google Scholar] [CrossRef] [Green Version]
- Bondi, M.W.; Edmonds, E.C.; Jak, A.J.; Clark, L.R.; Delano-Wood, L.; McDonald, C.R.; Nation, D.A.; Libon, D.J.; Au, R.; Galasko, D.; et al. Neuropsychological Criteria for Mild Cognitive Impairment Improves Diagnostic Precision, Biomarker Associations, and Progression Rates. J. Alzheimer’s Dis. 2014, 42, 275–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradley, M.M.; Lang, P.J. Measuring emotion: The self-assessment manikin and the semantic differential. J. Behav. Ther. Exp. Psychiatry 1994, 25, 49–59. [Google Scholar] [CrossRef]
- Lang, P.J.; Bradley, M.M.; Cuthbert, B.N. International affective picture system (IAPS): Technical manual and affective ratings. NIMH Cent. Study Emot. Atten. 1997, 1, 39–58. [Google Scholar]
- Delorme, A.; Makeig, S. EEGLAB: An open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J. Neurosci. Methods 2004, 134, 9–21. [Google Scholar] [CrossRef] [Green Version]
- Hyvärinen, A.; Oja, E. Independent component analysis: Algorithms and applications. Neural Netw. 2000, 13, 411–430. [Google Scholar] [CrossRef] [Green Version]
- Yao, D. A method to standardize a reference of scalp EEG. Physiol. Meas. 2001, 22, 693–711. [Google Scholar] [CrossRef] [PubMed]
- Qi, S. The Temporal Dynamics of Directed Reappraisal in High-Trait-Anxious Individuals. Emotion 2016, 16, 886–896. [Google Scholar] [CrossRef]
- Schupp, H.T.; Flaisch, T.; Stockburger, J.; Junghöfer, M. Chapter 2 Emotion and attention: Event-related brain potential studies. Prog. Brain Res. 2006, 156, 31–51. [Google Scholar] [CrossRef] [Green Version]
- Gao, C.; Wedell, D.H.; Green, J.J.; Jia, X.; Mao, X.; Guo, C.; Shinkareva, S.V. Temporal dynamics of audiovisual affective processing. Biol. Psychol. 2018, 139, 59–72. [Google Scholar] [CrossRef]
- Deweese, M.M.; Codispoti, M.; Robinson, J.D.; Cinciripini, P.M.; Versace, F. Cigarette cues capture attention of smokers and never-smokers, but for different reasons. Drug Alcohol Depend. 2018, 185, 50–57. [Google Scholar] [CrossRef] [PubMed]
- O’Hare, A.J.; Atchley, R.A.; Young, K.M. Valence and arousal influence the late positive potential during central and lateralized presentation of images. Laterality 2017, 22, 541–559. [Google Scholar] [CrossRef]
- Langeslag, S.J.E.; Van Strien, J.W. Up-regulation of emotional responses to reward-predicting stimuli: An ERP study. Biol. Psychol. 2013, 94, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Che, X.; Luo, X.; Tong, D.; Fitzgibbon, B.M.; Yang, J. Habitual suppression relates to difficulty in regulating emotion with cognitive reappraisal. Biol. Psychol. 2015, 112, 20–26. [Google Scholar] [CrossRef]
- Gross, J.J.; Jazaieri, H. Emotion, emotion regulation, and psychopathology: An affective science perspective. Clin. Psychol. Sci. 2014, 2, 387–401. [Google Scholar] [CrossRef]
- Bekkedal, M.Y.V.; Rossi, J.; Panksepp, J. Human brain EEG indices of emotions: Delineating responses to affective vocalizations by measuring frontal theta event-related synchronization. Neurosci. Biobehav. Rev. 2011, 35, 1959–1970. [Google Scholar] [CrossRef]
- Knyazev, G.G. Motivation, emotion, and their inhibitory control mirrored in brain oscillations. Neurosci. Biobehav. Rev. 2007, 31, 377–395. [Google Scholar] [CrossRef] [PubMed]
- Gardener, E.K.T.; Carr, A.R.; MacGregor, A.; Felmingham, K.L. Sex differences and emotion regulation: An event-related potential study. PLoS ONE 2020, 8, e73475. [Google Scholar] [CrossRef] [Green Version]
- Cai, A.; Lou, Y.; Long, Q.; Yuan, J.; Frederickson, J.J. The Sex Differences in Regulating Unpleasant Emotion by Expressive Suppression: Extraversion Matters. Front. Psychol. 2016, 7, 1011. [Google Scholar] [CrossRef] [Green Version]
- Rohr, L.; Rahman, R.A. Emotional language production: Time course, behavioral and electrophysiological correlates. Neuropsychologia 2018, 117, 241–252. [Google Scholar] [CrossRef] [PubMed]
- Mallorquí-Bagué, N.; Lozano-Madrid, M.; Testa, G.; Vintró-Alcaraz, C.; Sánchez, I.; Riesco, N.; César Perales, J.; Francisco Navas, J.; Martínez-Zalacaín, I.; Megías, A.; et al. Clinical and Neurophysiological Correlates of Emotion and Food Craving Regulation in Patients with Anorexia Nervosa. J. Clin. Med. 2020, 9, 960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lian, H.; Cao, D.; Li, Y. Electroencephalogram characteristics under successful cognitive reappraisal in emotion regulation. Sheng Wu Yi Xue Gong Cheng Xue Za Zhi J. Biomed. Eng. Shengwu Yixue Gongchengxue Zazhi 2020, 37, 579–586. [Google Scholar]
- Shigeto, H.; Ishiguro, J.; Nittono, H. Effects of visual stimulus complexity on event-related brain potentials and viewing duration in a free-viewing task. Neurosci. Lett. 2011, 497, 85–89. [Google Scholar] [CrossRef]
- Schindler, S.; Kissler, J. Selective visual attention to emotional words: Early parallel frontal and visual activations followed by interactive effects in visual cortex. Hum. Brain Mapp. 2016, 37, 3575–3587. [Google Scholar] [CrossRef]
- Rushworth, M.F.S.; Passingham, R.E.; Nobre, A.C. Components of attentional set-switching. Exp. Psychol. 2005, 52, 83–98. [Google Scholar] [CrossRef]
- Macnamara, A.; Jackson, T.B.; Fitzgerald, J.M.; Hajcak, G.; Phan, L. Working Memory Load and Negative Picture Processing: Neural and Behavioral Associations With Panic, Social Anxiety, and Positive Affect. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2019, 4, 151–159. [Google Scholar] [CrossRef]
- Herring, D.R.; Allen, J.J.B.; Güereca, Y.M.; Crites, S.L. An intra-individual approach for detecting evaluation with event-related potentials. Int. J. Psychophysiol. 2019, 141, 65–75. [Google Scholar] [CrossRef]
- Granholm, E.L.; Panizzon, M.S.; Elman, J.A.; Jak, A.J.; Hauger, R.L.; Bondi, M.W.; Lyons, M.J.; Franz, C.E.; Kremen, W.S. Pupillary Responses as a Biomarker of Early Risk for Alzheimer’s Disease. J. Alzheimer’s Dis. 2017, 56, 1419–1428. [Google Scholar] [CrossRef] [Green Version]
- Sweeney-reed, C.M.; Riddell, P.M.; Ellis, J.A.; Freeman, J.E.; Nasuto, S.J. Neural Correlates of True and False Memory in Mild Cognitive Impairment. PLoS ONE 2012, 7, e48357. [Google Scholar] [CrossRef] [Green Version]
- McRae, K.; Ciesielski, B.; Gross, J.J. Unpacking cognitive reappraisal: Goals, tactics, and outcomes. Emotion 2012, 12, 250–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, W.; Li, Y.; Cao, D. The effectiveness of emotion cognitive reappraisal as measured by self-reported response and its link to EEG alpha asymmetry. Behav. Brain Res. 2021, 400, 113042. [Google Scholar] [CrossRef] [PubMed]
- Cao, D. Brain Activity of Cognitive Reappraisal by TMS-EEG Co-Registration. Ph.D. Thesis, Shanghai University, Shanghai, China, 2019. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MCI (n = 44) | HEC (n = 72) | Group Effect | Cognition Effect | Group*Cognition Effect | |||
|---|---|---|---|---|---|---|---|
| Failure (n = 23) | Success (n = 21) | Failure (n = 26) | Success (n = 46) | ||||
| Age (years) | 68 (8) | 71 (9) | 68 (7) | 70 (6) | F = 1.790 p = 0.184 | F = 0.109 p = 0.742 | F = 0.135 p = 0.714 |
| Gender (M/F) | 9/14 | 8/13 | 14/12 | 23/23 | = 0.943 p = 1.000 | = 1.785 p = 0.182 | = 1.889 p = 0.596 |
| Education (years) | 10 (3) | 10 (4) | 11 (3) | 12 (3) | F = 0.245 p = 0.622 | F = 2.509 p = 0.116 | F = 1.396 p = 0.240 |
| MMSE | 24.3 (2.3) | 25.4 (2.3) | 27.0 (1.8) | 27.7 (1.4) | F = 6.215 p = 0.014 * | F = 48.148 p < 0.001 * | F = 0.215 p = 0.644 |
| HAMA | 7.5 (3.4) | 8.1 (3) | 6.7 (2.7) | 6.9 (4.4) | F = 0.336 p = 0.564 | F = 1.970 p = 0.163 | F = 1.679 p = 0.724 |
| HAMD | 5.2 (3.0) | 5.1 (3.2) | 4.5 (3.0) | 4.8 (3.9) | F = 0.050 p = 0.824 | F = 0.559 p = 0.456 | F = 0.073 p = 0.788 |
| Cognition | Early LPP | Middle LPP | Late LPP | ||||
|---|---|---|---|---|---|---|---|
| Failure | Success | Failure | Success | Failure | Success | ||
| MCI | Neutral-view | 1.58 (0.47) | 0.90 (0.55) | 0.04 (0.61) | −0.71 (0.60) | 0.13 (0.63) | −1.43 (0.74) |
| Negative-watch | 3.04 (0.48) | 3.27 (0.77) | 0.75 (0.54) | 1.03 (0.52) | 0.58 (0.62) | −0.11 (0.58) | |
| Negative-reappraisal | 2.24 (0.50) | 3.25 (0.76) | 0.34 (0.57) | 1.86 (0.71) | 0.35 (0.69) | 0.45 (0.62) | |
| Negative-reappraisal minus Negative-watch | −0.8 (0.26) | −0.02 (0.27) | −0.41 (0.37) | 0.83 (0.31) | −0.22 (0.66) | 0.55 (0.37) | |
| HEC | Neutral-view | 0.86 (0.34) | 2.15 (0.29) | 0.31 (0.50) | 1.13 (0.28) | 1.04 (0.71) | 1.11 (0.36) |
| Negative-watch | 2.36 (0.47) | 4.03 (0.35) | 0.64 (0.58) | 2.59 (0.31) | 0.68 (0.63) | 2.13 (0.39) | |
| Negative-reappraisal | 2.11 (0.42) | 3.36 (0.36) | 1.21 (0.46) | 1.91 (0.38) | 1.02 (0.56) | 1.67 (0.44) | |
| Negative-reappraisal minus Negative-watch | −0.25 (0.31) | −0.67 (0.19) | 0.57 (0.51) | −0.68 (0.31) | 0.34 (0.56) | −0.46 (0.39) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiao, S.; Li, Y.; Liu, M.; Li, Y. Electrophysiological Studies of Cognitive Reappraisal Success and Failure in aMCI. Brain Sci. 2021, 11, 855. https://doi.org/10.3390/brainsci11070855
Xiao S, Li Y, Liu M, Li Y. Electrophysiological Studies of Cognitive Reappraisal Success and Failure in aMCI. Brain Sciences. 2021; 11(7):855. https://doi.org/10.3390/brainsci11070855
Chicago/Turabian StyleXiao, Shasha, Yingjie Li, Meng Liu, and Yunxia Li. 2021. "Electrophysiological Studies of Cognitive Reappraisal Success and Failure in aMCI" Brain Sciences 11, no. 7: 855. https://doi.org/10.3390/brainsci11070855