
Procedural Learning through Action Observation: Preliminary Evidence from Virtual Gardening Activity in Intellectual Disability

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Ethical Approval
2.3. Materials and Apparatus
2.4. Clinical Data
2.5. Procedure
2.6. Data Analysis
3. Results
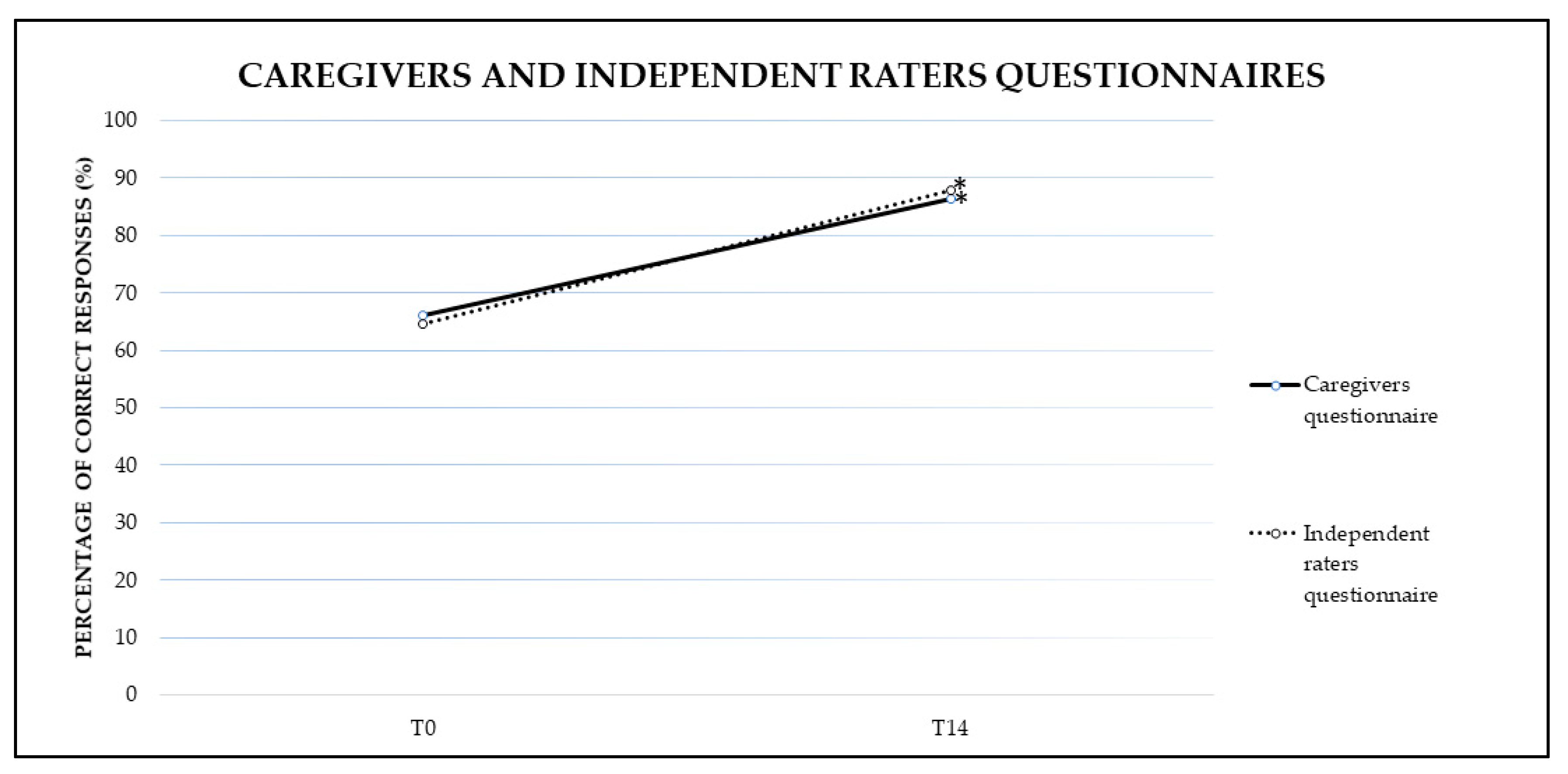
3.1. Caregivers and Independent Raters Questionnaires
3.1.1. Caregivers Questionnaire
3.1.2. Independent Raters Questionnaire
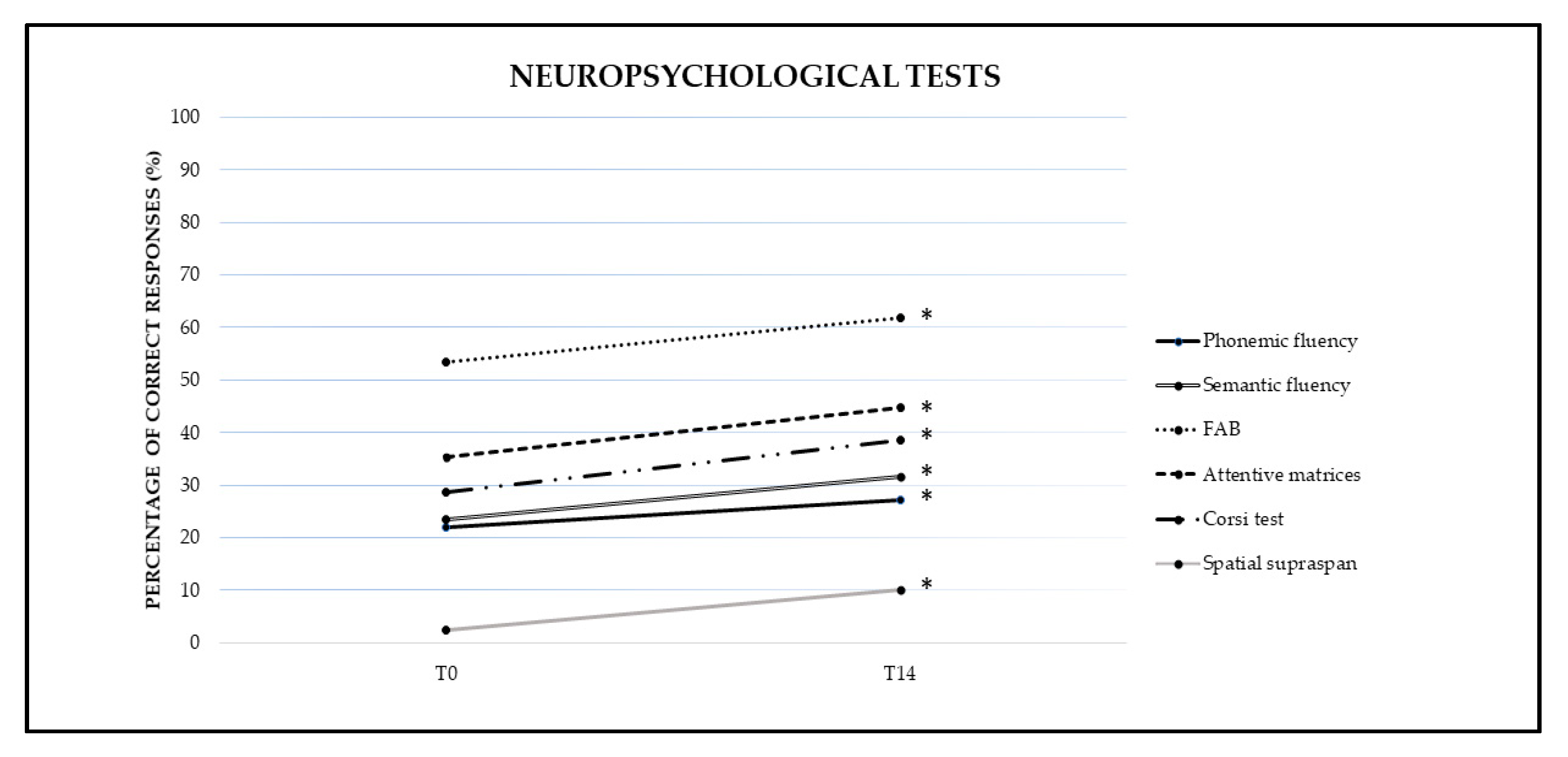
3.2. Neuropsychological Tests
3.2.1. Phonemic Fluency
3.2.2. Semantic Fluency
3.2.3. Frontal Assessment Battery (FAB)
3.2.4. Attentive Matrices
3.2.5. Corsi Test
3.2.6. Spatial Supra-Span
3.2.7. Token Test
3.2.8. Verbal Span
3.2.9. Prose Memory Test
3.2.10. Mini Mental State Examination (MMSE)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schalock, R.L.; Borthwick-Duffy, V.S.; Bradley, W.H.; Buntinx, D.L.; Coulter, D.L. Intellectual Disability: Definition, Classification, and Systems of Support, 11th ed.; American Association on Intellectual and Developmental Disabilities: Washington, DC, USA, 2010. [Google Scholar]
- Petersen, M.C.; Kube, D.A.; Palmer, F.B. Classification of developmental delays. Semin. Paediatr. Neurol. 1998, 5, 2–14. [Google Scholar] [CrossRef]
- Vasudevan, P.; Suri, M. A clinical approach to developmental delay and intellectual disability. Clin. Med. 2017, 17, 558–561. [Google Scholar] [CrossRef]
- Nemerimana, M.; Chege, M.N.; Odhiambo, E.A. Risk Factors Associated with Severity of Nongenetic Intellectual Disability (Mental Retardation) among Children Aged 2–18 Years Attending Kenyatta National Hospital. Neurol. Res. Int. 2018, 2018, 6956703. [Google Scholar] [CrossRef]
- Huang, J.; Zhu, T.; Qu, Y.; Mu, D. Prenatal, Perinatal and Neonatal Risk Factors for Intellectual Disability: A Systemic Review and Meta-Analysis. PLoS ONE 2016, 11, e0153655. [Google Scholar] [CrossRef] [Green Version]
- Katz, G.; Lazcano-Ponce, E. Intellectual disability: Definition, etiological factors, classification, diagnosis, treatment and prognosis. Salud Publica Mex. 2008, 50 (Suppl. 2), s132–s141. [Google Scholar] [CrossRef]
- Bendix, I.; Hadamitzky, M.; Herz, J.; Felderhoff-Müser, U. Adverse neuropsychiatric development following perinatal brain injury: From a preclinical perspective. Pediatri. Res. 2019, 85, 198–215. [Google Scholar] [CrossRef]
- Ergaz, Z.; Ornoy, A. Perinatal and early postnatal factors underlying developmental delay and disabilities. Dev. Disabil. Res. Rev. 2011, 17, 59–70. [Google Scholar] [CrossRef]
- Ismail, F.Y.; Fatemi, A.; Johnston, M.V. Cerebral plasticity: Windows of opportunity in the developing brain. Eur. J. Paediatr. Neurol. 2017, 21, 23–48. [Google Scholar] [CrossRef]
- Brown, K.A.; Parikh, S.; Patel, D.R. Understanding basic concepts of developmental diagnosis in children. Transl. Pediatr. 2020, 9 (Suppl. 1), S9–S22. [Google Scholar] [CrossRef]
- Sarkar, T.; Patro, N.; Patro, I.K. Cumulative multiple early life hits—A potent threat leading to neurological disorders. Brain Res. Bull. 2019, 147, 58–68. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Khan, I.; Leventhal, B.L. Developmental Delay. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Srour, M.; Shevell, M. Genetics and the investigation of developmental delay/intellectual disability. Arch. Dis. Child. 2014, 99, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Nevala, N.; Pehkonen, I.; Teittinen, A.; Vesala, H.T.; Pörtfors, P.; Anttila, H. The Effectiveness of Rehabilitation Interventions on the Employment and Functioning of People with Intellectual Disabilities: A Systematic Review. J. Occup. Rehabil. 2019, 29, 773–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Icht, M. Introducing the Beatalk technique: Using beatbox sounds and rhythms to improve speech characteristics of adults with intellectual disability. Int. J. Lang. Commun. Disord. 2019, 54, 401–416. [Google Scholar] [CrossRef]
- Đorđević, M.; Glumbić, N.; Brojčin, B. Paralinguistic abilities of adults with intellectual disability. Res. Dev. Disabil. 2016, 48, 211–219. [Google Scholar] [CrossRef]
- García, J.C.; Díez, E.; Wojcik, D.Z.; Santamaría, M.X. Communication Support Needs in Adults with Intellectual Disabilities and Its Relation to Quality of Life. Int. J. Environ. Res. Public Health 2020, 17, 7370. [Google Scholar] [CrossRef]
- Smith, M.; Manduchi, B.; Burke, É.; Carroll, R.; McCallion, P.; McCarron, M. Communication difficulties in adults with Intellectual Disability: Results from a national cross-sectional study. Res. Dev. Disabil. 2020, 97, 103557. [Google Scholar] [CrossRef]
- Fajardo, I.; Ávila, V.; Ferrer, A.; Tavares, G.; Gómez, M.; Hernández, A. Easy-to-read texts for students with intellectual disability: Linguistic factors affecting comprehension. J. Appl. Res. Intellect. Disabil. 2014, 27, 212–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Channell, M.M.; Loveall, S.J.; Conners, F.A. Strengths and weaknesses in reading skills of youth with intellectual disabilities. Res. Dev. Disabil. 2013, 34, 776–787. [Google Scholar] [CrossRef] [Green Version]
- Arvey, R.D.; Bourchard, T.J., Jr.; Carroll, J.B.; Cattell, R.B.; Cohen, D.B.; Davis, R.V.; Willerman, L. Mainstream science on intelligence. Wall Str. J. 1994, 4, B1. [Google Scholar]
- Gottfredson, L.S. Mainstream science on intelligence: An editorial of 52 signatories, history, and bibliography. Intelligence 1997, 24, 13–23. [Google Scholar] [CrossRef]
- Aronow, H.U.; Hahn, J.E. Stay well and healthy! Pilot study findings from an in-home preventive healthcare programme for persons ageing with intellectual and/or developmental disabilities. J. Appl. Resintel. Disabil. 2005, 18, 163–173. [Google Scholar] [CrossRef]
- Suto, W.M.; Clare, I.C.; Holland, A.J.; Watson, P.C. Understanding of basic financial concepts among adults with mild learning disabilities. Br. J. Clin. Psychol. 2006, 45, 261–266. [Google Scholar] [CrossRef]
- Patwardhan, I.; Nelson, T.D.; McClelland, M.M.; Mason, W.A. Childhood Cognitive Flexibility and Externalizing and Internalizing Behavior Problems: Examination of Prospective Bidirectional Associations. Res. Child Adolesc. Psychopathol. 2021, 49, 413–427. [Google Scholar] [CrossRef] [PubMed]
- Barisnikov, K.; Straccia, C. Social adaptive skills and psychopathology in adults with intellectual disabilities of non-specific origin and those with Down syndrome. Res. Dev. Disabil. 2019, 87, 31–42. [Google Scholar] [CrossRef]
- Waldman-Levi, A.; Golisz, K.; Swierat, R.P.; Toglia, J. Scoping review: Interventions that promote functional performance for adolescents and adults with Intellectual and Developmental Disabilities. Aust. Occup. Ther. J. 2019, 66, 458–468. [Google Scholar] [CrossRef] [PubMed]
- Applegate, S.L.; Rice, M.S.; Stein, F.; Maitra, K.K. Knowledge of results and learning to tell the time in an adult male with an intellectual disability: A single-subject research design. Occup. Ther. Int. 2008, 15, 32–44. [Google Scholar] [CrossRef]
- Miller, U.C.; Test, D.W. A comparison of constant time delay and most-to-least prompting in teaching laundry skills to students with moderate retardation. Ed. Train. Men Retar. 1989, 24, 363–370. [Google Scholar]
- Sandknop, P.A.; Schuster, J.W.; Wolery, M.; Cross, D.P. The use of an adaptive device to teach students with moderate mental retardation to select lower priced grocery items. Ed. Train. Men Retar. 1992, 27, 219–229. [Google Scholar]
- Cantone, M.; Catalano, M.A.; Lanza, G.; La Delfa, G.; Ferri, R.; Pennisi, M.; Bella, R.; Pennisi, G.; Bramanti, A. Motor and Perceptual Recovery in Adult Patients with Mild Intellectual Disability. Neural Plast. 2018, 2018, 3273246. [Google Scholar] [CrossRef] [Green Version]
- Gómez Álvarez, N.; Venegas Mortecinos, A.; Zapata Rodríguez, V.; López Fontanilla, M.; Maudier Vásquez, M.; Pavez-Adasme, G.; Hemández-Mosqueira, C. Efecto de una intervención basada en realidad virtual sobre las habi lidades motrices básicas y control postural de niños con Síndrome de Down [Effect of an intervention based on virtual reality on motor development and postural control in children with Down Syndrome]. Rev. Chil. Pediatr. 2018, 89, 747–752. [Google Scholar] [CrossRef]
- Wuang, Y.P.; Chiang, C.S.; Su, C.Y.; Wang, C.C. Effectiveness of virtual reality using Wii gaming technology in children with Down syndrome. Res. Dev. Disabil. 2011, 32, 312–321. [Google Scholar] [CrossRef]
- Maïano, C.; Hue, O.; April, J. Effects of motor skill interventions on fundamental movement skills in children and adolescents with intellectual disabilities: A systematic review. J. Intellect. Disabil. Res. 2019, 63, 1163–1179. [Google Scholar] [CrossRef] [Green Version]
- Cratty, B.J. Sensory-motor and perceptual-motor theories and practices: An overview and evaluation. In Intersensory Perception and Sensory Integration; Pick, H.L., Walk, R.D., Eds.; Cambridge University Press: New York, NY, USA, 1981; pp. 345–373. [Google Scholar]
- Gallese, V.; Lakoff, G. The Brain’s concepts: The role of the Sensory-motor system in conceptual knowledge. Cogn. Neuropsychol. 2005, 22, 455–479. [Google Scholar] [CrossRef]
- Craighero, L. The role of motor system in cognitive functions. In The Routledge Handbook of Embodied Cognition; Shapiro, L., Ed.; Routledge: London, UK, 2014. [Google Scholar]
- Barsalou, L.W. Perceptions of perceptual symbols. Behav. Brain Sci. 1999, 22, 637–660. [Google Scholar] [CrossRef] [Green Version]
- Fadiga, L.; Craighero, L.; Buccino, G.; Rizzolatti, G. Speech listening specifically modulates the excitability of tongue muscles: A TMS study. Eur. J. Neurosci. 2002, 15, 399–402. [Google Scholar] [CrossRef] [Green Version]
- Quadrelli, E.; Roberti, E.; Turati, C.; Craighero, L. Observation of the point-light animation of a grasping hand activates sensorimotor cortex in nine-month-old infants. Cortex 2019, 119, 373–385. [Google Scholar] [CrossRef]
- Rizzolatti, G.; Craighero, L. The mirror-neuron system. Annu. Rev. Neurosci. 2004, 27, 169–192. [Google Scholar] [CrossRef] [Green Version]
- Buccino, G. Action observation treatment: A novel tool in neurorehabilitation. Philos. Trans. R. Soc. B Biol. Sci. 2014, 369, 20130185. [Google Scholar] [CrossRef]
- Craighero, L.; Bonetti, F.; Massarenti, L.; Canto, R.; Fabbri Destro, M.; Fadiga, L. Temporal prediction of touch instant during observation of human and robot grasping. Brain Res. Bull. 2008, 75, 770–774. [Google Scholar] [CrossRef]
- Craighero, L.; Metta, G.; Sandini, G.; Fadiga, L. The mirror-neurons system: Data and models. Prog. Brain Res. 2007, 164, 39–59. [Google Scholar] [CrossRef]
- Buccino, G.; Solodkin, A.; Small, S.L. Functions of the mirror neuron system: Implications for neurorehabilitation. Cogn. Behav. Neurol. 2006, 1, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Borges, L.R.; Fernandes, A.B.; Melo, L.P.; Guerra, R.O.; Campos, T.F. Action observation for upper limb rehabilitation after stroke. Cochrane Database Syst. Rev. 2018, 10, CD011887. [Google Scholar] [CrossRef] [PubMed]
- Ertelt, D.; Small, S.; Solodkin, A.; Dettmers, C.; McNamara, A.; Binkofski, F.; Buccino, G. Action observation has a positive impact on rehabilitation of motor deficits after stroke. Neuroimage 2007, 36 (Suppl. 2), T164–T173. [Google Scholar] [CrossRef]
- Marangolo, P.; Bonifazi, S.; Tomaiuolo, F.; Craighero, L.; Coccia, M.; Altoè, G.; Provinciali, L.; Cantagallo, A. Improving language without words: First evidence from aphasia. Neuropsychologia 2010, 48, 3824–3833. [Google Scholar] [CrossRef]
- Marangolo, P.; Cipollari, S.; Fiori, V.; Razzano, C.; Caltagirone, C. Walking but not barking improves verb recovery: Implications for action observation treatment in aphasia rehabilitation. PLoS ONE 2012, 7, e38610. [Google Scholar] [CrossRef] [Green Version]
- Bonifazi, S.; Tomaiuolo, F.; Altoè, G.; Ceravolo, M.G.; Provinciali, L.; Marangolo, P. Action observation as a useful approach for enhancing recovery of verb production: New evidence from aphasia. Eur. J. Phys. Rehabil. Med. 2013, 49, 473–481. [Google Scholar]
- Foti, F.; Piras, F.; Vicari, S.; Mandolesi, L.; Petrosini, L.; Menghini, D. Observational Learning in Low-Functioning Children with Autism Spectrum Disorders: A Behavioral and Neuroimaging Study. Front. Psychol. 2019, 9, 2737. [Google Scholar] [CrossRef] [Green Version]
- Foti, F.; Menghini, D.; Alfieri, P.; Costanzo, F.; Mandolesi, L.; Petrosini, L.; Vicari, S. Learning by observation and learning by doing in Down and Williams syndromes. Dev. Sci. 2018, 21, e12642. [Google Scholar] [CrossRef] [PubMed]
- Foti, F.; Mazzone, L.; Menghini, D.; De Peppo, L.; Federico, F.; Postorino, V.; Baumgartner, E.; Valeri, G.; Petrosini, L.; Vicari, S. Learning by observation in children with autism spectrum disorder. Psychol. Med. 2014, 44, 2437–2447. [Google Scholar] [CrossRef] [Green Version]
- Kagohara, D.M.; Sigafoos, J.; Achmadi, D.; van der Meer, L.; O’Reilly, M.F.; Lancioni, G.E. Teaching students with developmental disabilities to operate an iPod Touch® to listen to music. Res. Dev. Disabil. 2011, 32, 2987–2992. [Google Scholar] [CrossRef]
- Kagohara, D.M.; van der Meer, L.; Ramdoss, S.; O’Reilly, M.F.; Lancioni, G.E.; Davis, T.N.; Rispoli, M.; Lang, R.; Marschik, P.B.; Sutherland, D.; et al. Using iPods® and iPads® in teaching programs for individuals with developmental disabilities: A systematic review. Res. Dev. Disabil. 2013, 34, 147–156. [Google Scholar] [CrossRef]
- Joseph, A.; Browning, M.H.E.M.; Jiang, S. Using Immersive Virtual Environments (IVEs) to Conduct Environmental Design Research: A Primer and Decision Framework. HERD 2020, 13, 11–25. [Google Scholar] [CrossRef]
- Maggio, M.G.; Maresca, G.; De Luca, R.; Stagnitti, M.C.; Porcari, B.; Ferrera, M.C.; Galletti, F.; Casella, C.; Manuli, A.; Calabrò, R.S. The Growing Use of Virtual Reality in Cognitive Rehabilitation: Fact, Fake or Vision? A Scoping Review. J. Natl. Med. Assoc. 2019, 111, 457–463. [Google Scholar] [CrossRef]
- De Luca, R.; Russo, M.; Naro, A.; Tomasello, P.; Leonardi, S.; Santamaria, F.; Desireè, L.; Bramanti, A.; Silvestri, G.; Bramanti, P.; et al. Effects of virtual reality-based training with BTs-Nirvana on functional recovery in stroke patients: Preliminary considerations. Int. J. Neurosci. 2018, 128, 791–796. [Google Scholar] [CrossRef]
- De Luca, R.; Lo Buono, V.; Leo, A.; Russo, M.; Aragona, B.; Leonardi, S.; Buda, A.; Naro, A.; Calabrò, R.S. Use of virtual reality in improving poststroke neglect: Promising neuropsychological and neurophysiological findings from a case study. Appl. Neuropsychol. Adult 2019, 26, 96–100. [Google Scholar] [CrossRef]
- Giachero, A.; Calati, M.; Pia, L.; La Vista, L.; Molo, M.; Rugiero, C.; Fornaro, C.; Marangolo, P. Conversational Therapy through Semi-Immersive Virtual Reality Environments for Language Recovery and Psychological Well-Being in Post Stroke Aphasia. Behav. Neurol. 2020, 6, 2846046. [Google Scholar] [CrossRef] [PubMed]
- Tieri, G.; Morone, G.; Paolucci, S.; Iosa, M. Virtual reality in cognitive and motor rehabilitation: Facts, fiction and fallacies. Expert. Rev. Med. Devices 2018, 15, 107–117. [Google Scholar] [CrossRef]
- Keil, J.; Edler, D.; O’Meara, D.; Korte, A.; Dickmann, F. Effects of Virtual Reality Locomotion Techniques on Distance Estimations. ISPRS Int. J. Geo-Inf. 2021, 10, 150. [Google Scholar] [CrossRef]
- Tabrizian, P.; Petrasova, A.; Baran, P.K.; Vukomanovic, J.; Mitasova, H.; Meentemeyer, R.K. High Resolution Viewscape Modeling Evaluated Through Immersive Virtual Environments. ISPRS Int. J. Geo-Inf. 2020, 9, 445. [Google Scholar] [CrossRef]
- Boletsis, C.; Cedergren, J.E. VR Locomotion in the New Era of Virtual Reality: An Empirical Comparison of Prevalent Techniques. Adv. Hum. Comput. Int. 2019, 2019, 7420781. [Google Scholar] [CrossRef]
- Varela-Aldás, J.; Palacios-Navarro, G.; Amariglio, R.; García-Magariño, I. Head-Mounted Display-Based Application for Cognitive Training. Sensors 2020, 20, 6552. [Google Scholar] [CrossRef] [PubMed]
- Saldana, D.; Neureither, M.; Schmiesing, A.; Jahng, E.; Kysh, L.; Roll, S.C.; Liew, S.L. Applications of Head-Mounted Displays for Virtual Reality in Adult Physical Rehabilitation: A Scoping Review. Am. J. Occup. Ther. 2020, 74, 7405205060p1–7405205060p15. [Google Scholar] [CrossRef] [PubMed]
- Knobel, S.E.J.; Kaufmann, B.C.; Gerber, S.M.; Cazzoli, D.; Müri, R.M.; Nyffeler, T.; Nef, T. Immersive 3D Virtual Reality Cancellation Task for Visual Neglect Assessment: A Pilot Study. Front. Hum. Neurosci. 2020, 14, 180. [Google Scholar] [CrossRef] [PubMed]
- Erhardsson, M.; Alt Murphy, M.; Sunnerhagen, K.S. Commercial head-mounted display virtual reality for upper extremity rehabilitation in chronic stroke: A single-case design study. J. Neuroeng. Rehabil. 2020, 17, 154. [Google Scholar] [CrossRef]
- Attwell, C.; Jöhr, J.; Pincherle, A.; Pignat, J.M.; Kaufmann, N.; Knebel, J.F.; Berney, L.; Ryvlin, P.; Diserens, K. Neurosensory stimulation outdoors enhances cognition recovery in cognitive motor dissociation: A prospective crossover study. NeuroRehabilitation 2019, 44, 545–554. [Google Scholar] [CrossRef] [Green Version]
- Standen, P.J.; Brown, D.J. Virtual reality in the rehabilitation of people with intellectual disabilities: Review. Cyberpsychol. Behav. 2005, 8, 272–282. [Google Scholar] [CrossRef]
- Nabors, L.; Monnin, J.; Jimenez, S. A Scoping Review of Studies on Virtual Reality for Individuals with Intellectual Disabilities. Adv. Neurodev. Disord. 2020, 4, 344–356. [Google Scholar] [CrossRef]
- Thornson, C.A.; Goldiez, B.F.; Le, H. Predicting presence: Constructing the Tendency toward Presence Inventory. Int. J. Hum. Comp. Stud. 2009, 67, 62–78. [Google Scholar] [CrossRef]
- Adamovich, S.V.; Fluet, G.G.; Tunik, E.; Merians, A.S. Sensorimotor training in virtual reality: A review. NeuroRehabilitation 2009, 25, 29–44. [Google Scholar] [CrossRef] [Green Version]
- Saposnik, G.; Teasell, R.; Mamdani, M.; Hal, J.; McIlroy, W.; Cheung, D.; Thorpe, K.; Cohen, L.G.; Bayley, M. Stroke Outcome Research Canada (SORCan) Working Group. Effectiveness of virtual reality using Wii gaming technology in stroke rehabilitation: A pilot randomized clinical trial and proof of principle. Stroke 2010, 41, 1477–1484. [Google Scholar] [CrossRef] [Green Version]
- Spinelli, G.; Tieri, G.; Pavone, E.F.; Aglioti, S.M. Wronger than wrong: Graded mapping of the errors of an avatar in the performance monitoring system of the onlooker. Neuroimage 2018, 167, 1–10. [Google Scholar] [CrossRef]
- Seidler, R.D.; Kwak, Y.; Fling, B.W.; Bernard, J.A. Neurocognitive mechanisms of error-based motor learning. Adv. Exp. Med. Biol. 2013, 782, 39–60. [Google Scholar] [CrossRef] [Green Version]
- Nishizawa, H.; Kimura, T. Enhancement of motor skill learning by a combination of ideal model-observation and self-observation. J. Phys. Ther. Sci. 2017, 29, 1555–1560. [Google Scholar] [CrossRef] [Green Version]
- Brooks, B.M.; Rose, F.D.; Attree, E.A.; Elliot-Square, A. An evaluation of the efficacy of training people with learning disabilities in a virtual environment. Disabil. Rehabil. 2002, 24, 622–626. [Google Scholar] [CrossRef] [PubMed]
- Oldfield, R.C. The assessment and analysis of handedness: The Edinburgh inventory. Neuropsychologia 1971, 9, 97–113. [Google Scholar] [CrossRef]
- Orsini, A.; Laicardi, C. WAIS-R: Contributo Alla Taratura Italiana; Organizzazioni Speciali: Firenze, Italy, 2009; pp. 1–119. [Google Scholar]
- Morganti, F.; Riva, G. Conoscenza, Comunicazione e Tecnologia: Aspetti Cognitivi Della Realtà Virtuale; LED Edizioni Universitarie: Milano, Italy, 2006. [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Dubois, B.; Slachevsky, A.; Litvan, I.; Pillon, B. The FAB: A Frontal Assessment Battery at bedside. Neurology 2000, 55, 1621–1626. [Google Scholar] [CrossRef] [Green Version]
- Spinnler, H.; Tognoni, G. Standardizzazione e taratura italiana di test neuropsicologici. Ital. J. Neurol. Sci. 1987, 6, 1–120. [Google Scholar]
- Meltzoff, A.N.; Williamson, R.A. Imitation: Social, cognitive, and theoretical perspectives. In Oxford Library of Psychology. The Oxford Handbook of Developmental Psychology; Zelazo, P.D., Ed.; Oxford University Press: Oxford, UK, 2013; pp. 651–682. [Google Scholar]
- Meltzoff, A.N. The ‘like me’ framework for recognizing and becoming an intentional agent. Acta Psychol. 2007, 124, 26–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandura, A. Social Learning Theory; Prentice Hall: Englewood Cliffs, IL, USA, 1977. [Google Scholar]
- Meltzoff, A.N.; Kuhl, P.K.; Movellan, J.; Sejnowski, T.J. Foundations for a new science of learning. Science 2009, 325, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Binkofski, F.; Buccino, G. The role of ventral premotor cortex in action execution and action understanding. J. Physiol. Paris 2006, 99, 396–405. [Google Scholar] [CrossRef] [PubMed]
- Karmiloff-Smith, A. Development itself is the key to understanding developmental disorders. Trends Cogn. Sci. 1998, 2, 389–397. [Google Scholar] [CrossRef]
- Danielsson, H.; Henry, L.; Rönnberg, J.; Nilsson, L.G. Executive functions in individuals with intellectual disability. Res. Dev. Disabil. 2010, 31, 1299–1304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Udhnani, M.; Perez, M.; Clasen, L.S.; Adeyemi, E.; Lee, N.R. Relations between Everyday Executive Functioning and Language in Youth with Down Syndrome and Youth with Autism Spectrum Disorder. Dev. Neuropsychol. 2020, 45, 79–93. [Google Scholar] [CrossRef]
- Amadó, A.; Serrat, E.; Vallès-Majoral, E. The Role of Executive Functions in Social Cognition among Children with Down Syndrome: Relationship Patterns. Front. Psychol. 2016, 7, 1363. [Google Scholar] [CrossRef] [Green Version]
- Akbar, M.; Loomis, R.; Paul, R. The interplay of language on executive functions in children with ASD. Res. Autism Spectr. Disord. 2013, 7, 494–501. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group | Participants | WAIS-R | Sex | Age | Educational Level | Etiology |
|---|---|---|---|---|---|---|
| 1 Mild | 1 | 69 | F | 72 | 8 | Neonatal cerebropathy |
| 1-Mild | 2 | 63 | F | 56 | 8 | Neonatal cerebropathy |
| 1-Mild | 3 | 65 | F | 68 | 5 | Neonatal cerebropathy |
| 1-Mild | 4 | 68 | F | 52 | 8 | Perinatal cerebropathy |
| 2-Moderate | 5 | 57 | M | 36 | 8 | Neonatal cerebropathy |
| 2-Moderate | 6 | 57 | M | 44 | 8 | Perinatal cerebropathy |
| 2-Moderate | 7 | 53 | F | 59 | 5 | Epileptogenic encephalopathy |
| 2-Moderate | 8 | 52 | F | 28 | 8 | Neonatal cerebropathy |
| 2-Moderate | 9 | 58 | F | 61 | 5 | Perinatal asphyxia |
| 3-Severe | 10 | <45 | M | 38 | 13 | Perinatal asphyxia |
| 3-Severe | 11 | <45 | F | 34 | 8 | Neonatal cerebropathy |
| 3-Severe | 12 | <45 | F | 31 | 13 | Neonatal cerebropathy |
| 3-Severe | 13 | <45 | M | 42 | 8 | Perinatal cerebropathy |
| 3-Severe | 14 | <45 | F | 47 | 8 | Perinatal asphyxia |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giachero, A.; Quadrini, A.; Pisano, F.; Calati, M.; Rugiero, C.; Ferrero, L.; Pia, L.; Marangolo, P. Procedural Learning through Action Observation: Preliminary Evidence from Virtual Gardening Activity in Intellectual Disability. Brain Sci. 2021, 11, 766. https://doi.org/10.3390/brainsci11060766
Giachero A, Quadrini A, Pisano F, Calati M, Rugiero C, Ferrero L, Pia L, Marangolo P. Procedural Learning through Action Observation: Preliminary Evidence from Virtual Gardening Activity in Intellectual Disability. Brain Sciences. 2021; 11(6):766. https://doi.org/10.3390/brainsci11060766
Chicago/Turabian StyleGiachero, Alberto, Agnese Quadrini, Francesca Pisano, Melanie Calati, Cristian Rugiero, Laura Ferrero, Lorenzo Pia, and Paola Marangolo. 2021. "Procedural Learning through Action Observation: Preliminary Evidence from Virtual Gardening Activity in Intellectual Disability" Brain Sciences 11, no. 6: 766. https://doi.org/10.3390/brainsci11060766