
Changes in Brain Volume Resulting from Cognitive Intervention by Means of the Feuerstein Instrumental Enrichment Program in Older Adults with Mild Cognitive Impairment (MCI): A Pilot Study

 ,
,  , , and
, , and
Abstract
:1. Introduction
1.1. MRI and Cognitive Function
1.2. Study Goals
2. Methods
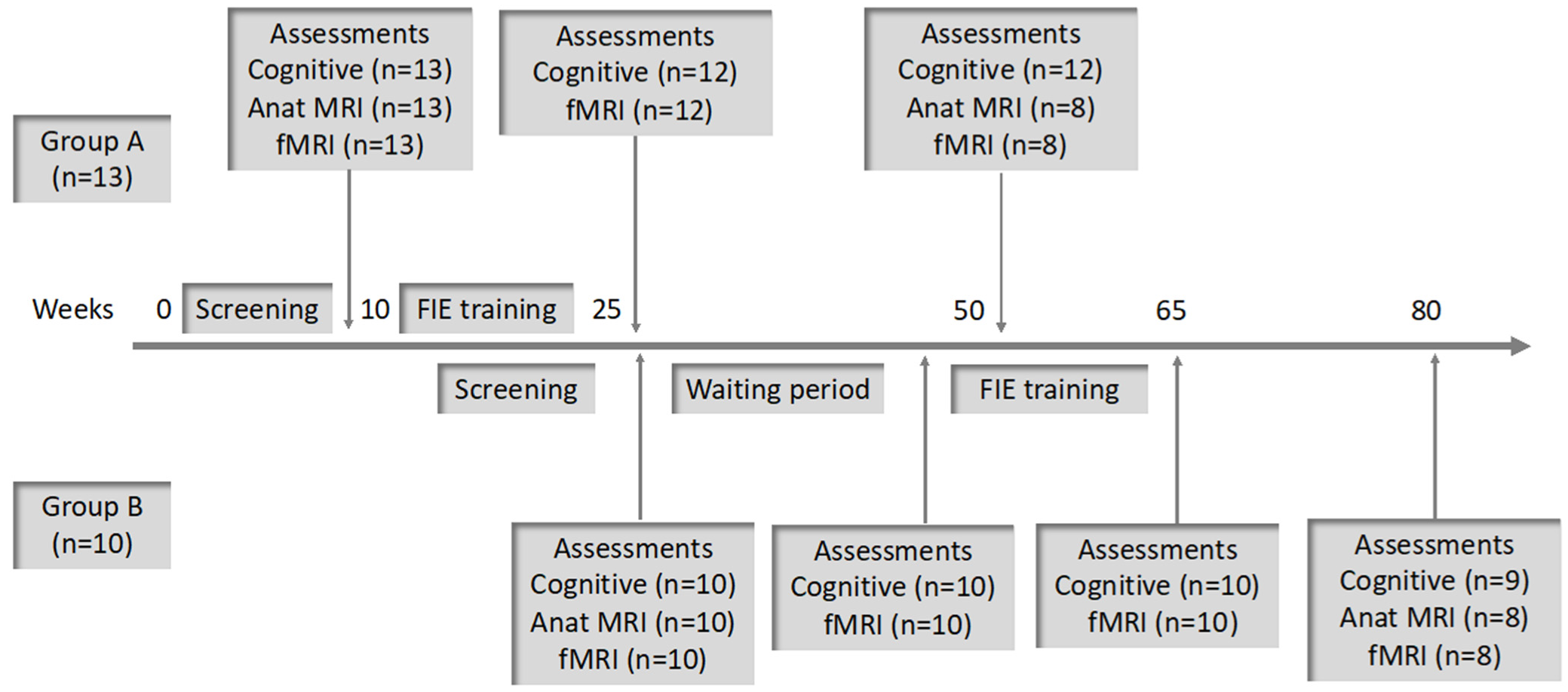
2.1. Study Description
2.2. Participants
2.3. Procedure
2.4. Instruments
2.4.1. The Montreal Cognitive Assessment (MoCA)
2.4.2. CogSym Metacognition Questionnaire
2.4.3. Well-Being Questionnaire
2.4.4. “NeuroTrax” Computerized Neuropsychological Assessment Battery
2.5. Cognitive Data Analysis
2.6. MRI Data Acquisition and Processing
2.7. Intervention
3. Results
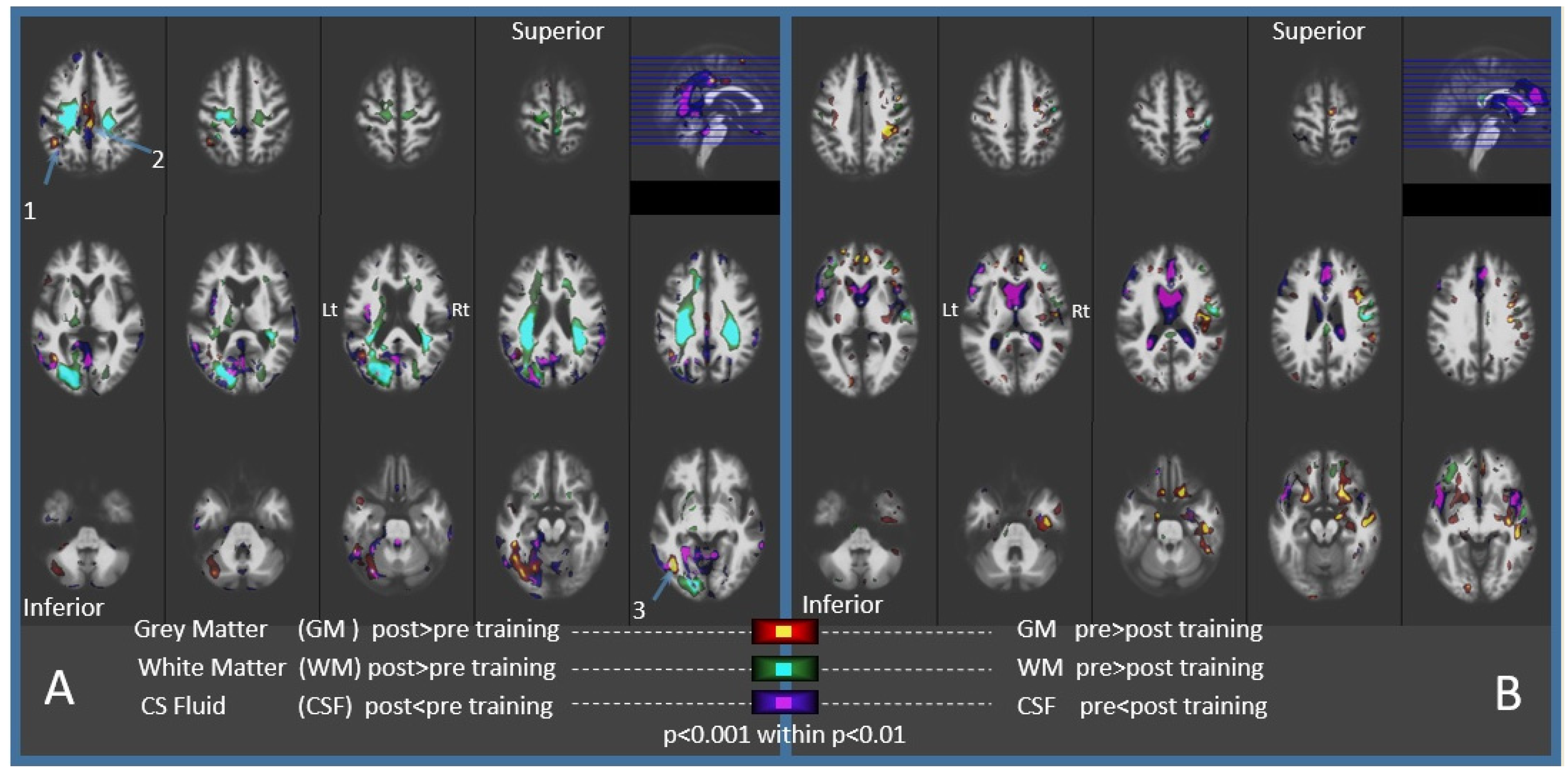
3.1. Imaging Results
3.2. Cognitive Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Morley, J.E.; Morris, J.C.; Berg-Weger, M.; Borson, S.; Carpenter, B.D.; Del Campo, N.; Dubois, B.; Fargo, K.; Fitten, L.J.; Flaherty, J.H.; et al. Brain health: The importance of recognizing cognitive impairment: An IAGG consensus conference. J. Am. Med. Dir. Assoc. 2015, 16, 731–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. The Lancet Commissions Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef] [Green Version]
- Petersen, R.C.; Lopez, O.; Armstrong, M.J.; Getchius, T.S.D.; Ganguli, M.; Gloss, D.; Gronseth, G.S.; Marson, D.; Pringsheim, T.; Day, G.S.; et al. Practice guideline update summary: Mild cognitive impairment report of theguideline development, dissemination, and implementation. Neurology 2018, 90, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Winblad, B.; Palmer, K.; Kivipelto, M.; Jelic, V.; Fratiglioni, L.; Wahlund, L.-O. Mild cognitive impairment—Beyond controversies, towards a consensus: Report of the International Working Group on Mild Cognitive Impairment. J. Intern. Med. 2004, 256, 240–246. [Google Scholar] [CrossRef]
- Dua, T.; Seeher, K.M.; Sivananthan, S.; Chowdhary, N.; Pot, A.M.; Saxena, S. Risk Reduction of Cognitive Decline and Dementia; World Health Organization: Geneva, Switzerland, 2019; Volume 13, ISBN 9789241550543.
- Simon, S.S.; Castellani, M.; Belleville, S.; Dwolatzky, T.; Hampstead, B.M.; Bahar-Fuchs, A.C. The design, evaluation, and reporting on non-pharmacological, cognition-oriented treatments for older adults: Results of a survey of experts. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2020, 6, e12024. [Google Scholar] [CrossRef]
- Barban, F.; Mancini, M.; Cercignani, M.; Adriano, F.; Perri, R.; Annicchiarico, R.; Carlesimo, G.A.; Ricci, C.; Lombardi, M.G.; Teodonno, V.; et al. A pilot study on brain plasticity of functional connectivity modulated by cognitive training in mild Alzheimer’s disease and mild cognitive impairment. Brain Sci. 2017, 7, 50. [Google Scholar] [CrossRef]
- Brum, P.S.; Borella, E.; Carretti, B.; Sanches Yassuda, M. Verbal working memory training in older adults: An investigation of dose response. Aging Ment. Health 2020, 24, 81–91. [Google Scholar] [CrossRef]
- Nguyen, L.; Murphy, K.; Andrews, G. Cognitive and neural plasticity in old age: A systematic review of evidence from executive functions cognitive training. Ageing Res. Rev. 2019, 53, 100912. [Google Scholar] [CrossRef]
- Smith, G.E.; Housen, P.; Yaffe, K.; Ruff, R.; Kennison, R.F.; Mahncke, H.W.; Zelinski, E.M. A cognitive training program based on principles of brain plasticity: Results from the improvement in memory with plasticity-based adaptive cognitive training (IMPACT) study. J. Am. Geriatr. Soc. 2009, 57, 594–603. [Google Scholar] [CrossRef] [Green Version]
- Márquez, F.; Yassa, M.A. Neuroimaging Biomarkers for Alzheimer’ s Disease. Mol. Neurodegener. 2019, 14, 21. [Google Scholar] [CrossRef] [Green Version]
- Tsapanou, A.; Habeck, C.; Gazes, Y.; Razlighi, Q.; Sakhardande, J.; Stern, Y.; Salthouse, T.A. Brain biomarkers and cognition across adulthood. Hum. Brain Mapp. 2019, 40, 3832–3842. [Google Scholar] [CrossRef] [Green Version]
- Esposito, R.; Mosca, A.; Pieramico, V.; Cieri, F.; Cera, N.; Sensi, S.L. Characterization of resting state activity in MCI individuals. PeerJ 2013, 2013, e135. [Google Scholar] [CrossRef] [PubMed]
- Karahanoʇlu, F.I.; Van De Ville, D. Transient brain activity disentangles fMRI resting-state dynamics in terms of spatially and temporally overlapping networks. Nat. Commun. 2015, 6, 7751. [Google Scholar] [CrossRef]
- Meskaldji, D.E.; Preti, M.G.; Bolton, T.A.; Montandon, M.L.; Rodriguez, C.; Morgenthaler, S.; Giannakopoulos, P.; Haller, S.; Van De Ville, D. Prediction of long-term memory scores in MCI based on resting-state fMRI. NeuroImage Clin. 2016, 12, 785–795. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Liu, S.; Ng, K.K.; Wang, J. Applications of Resting-State Functional Connectivity to Neurodegenerative Disease. Neuroimaging Clin. N. Am. 2017, 27, 663–683. [Google Scholar] [CrossRef]
- Li, R.; Zhu, X.; Yin, S.; Niu, Y.; Zheng, Z.; Huang, X.; Wang, B.; Li, J. Multimodal intervention in older adults improves resting-state functional connectivity between the medial prefrontal cortex and medial temporal lobe. Front. Aging Neurosci. 2014, 6, 39. [Google Scholar] [CrossRef]
- Pievani, M.; Pini, L.; Cappa, S.F.; Frisoni, G.B. Brain networks stimulation in dementia: Insights from functional imaging. Curr. Opin. Neurol. 2016, 29, 756–762. [Google Scholar] [CrossRef] [PubMed]
- Miotto, E.C.; Batista, A.X.; Simon, S.S.; Hampstead, B.M. Neurophysiologic and cognitive changes arising from cognitive training interventions in persons with mild cognitive impairment: A systematic review. Neural Plast. 2018, 2018, 7301530. [Google Scholar] [CrossRef]
- Noble, S.; Spann, M.N.; Tokoglu, F.; Shen, X.; Constable, R.T.; Scheinost, D. Influences on the Test-Retest Reliability of Functional Connectivity MRI and its Relationship with Behavioral Utility. Cereb. Cortex 2017, 27, 5415–5429. [Google Scholar] [CrossRef] [Green Version]
- Betzel, R.F.; Byrge, L.; He, Y.; Goñi, J.; Zuo, X.N.; Sporns, O. Changes in structural and functional connectivity among resting-state networks across the human lifespan. Neuroimage 2014, 102, 345–357. [Google Scholar] [CrossRef]
- Mayo, C.D.; Mazerolle, E.L.; Ritchie, L.; Fisk, J.D.; Gawryluk, J.R. Longitudinal changes in microstructural white matter metrics in Alzheimer’s disease. NeuroImage Clin. 2017, 13, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Blamire, A.M. MR approaches in neurodegenerative disorders. Prog. Nucl. Magn. Reson. Spectrosc. 2018, 108, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Firbank, M.J.; Watson, R.; Mak, E.; Aribisala, B.; Barber, R.; Colloby, S.J.; He, J.; Blamire, A.M.; O’Brien, J.T. Longitudinal diffusion tensor imaging in dementia with Lewy bodies and Alzheimer’s disease. Park. Relat. Disord. 2016, 24, 76–80. [Google Scholar] [CrossRef] [Green Version]
- Damoiseaux, J.S. Effects of aging on functional and structural brain connectivity. Neuroimage 2017, 160, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Scarpazza, C.; Nichols, T.E.; Seramondi, D.; Maumet, C.; Sartori, G.; Mechelli, A. When the single matters more than the Group (II): Addressing the problem of high false positive rates in single case voxel based morphometry using non-parametric statistics. Front. Neurosci. 2016, 10, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spina, S.; Brown, J.A.; Deng, J.; Gardner, R.C.; Nana, A.L.; Hwang, J.H.L.; Gaus, S.E.; Huang, E.J.; Kramer, J.H.; Rosen, H.J.; et al. Neuropathological correlates of structural and functional imaging biomarkers in 4-repeat tauopathies. Brain 2019, 142, 2068–2081. [Google Scholar] [CrossRef] [PubMed]
- Moscoso, A.; Silva-Rodríguez, J.; Aldrey, J.M.; Cortés, J.; Fernández-Ferreiro, A.; Gómez-Lado, N.; Ruibal, Á.; Aguiar, P. Prediction of Alzheimer’s disease dementia with MRI beyond the short-term: Implications for the design of predictive models. NeuroImage Clin. 2019, 23, 101837. [Google Scholar] [CrossRef]
- Ottoy, J.; Niemantsverdriet, E.; Verhaeghe, J.; De Roeck, E.; Struyfs, H.; Somers, C.; Wyffels, L.; Ceyssens, S.; Van Mossevelde, S.; Van den Bossche, T.; et al. Association of short-term cognitive decline and MCI-to-AD dementia conversion with CSF, MRI, amyloid- and 18 F-FDG-PET imaging. NeuroImage Clin. 2019, 22, 101771. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.; Liu, T.; Tao, D.; Fan, Y.; Zhang, J.; Li, S.; Jiang, J.; Zhu, W.; Wang, Y.; Wang, Y.; et al. Variation in longitudinal trajectories of cortical sulci in normal elderly. Neuroimage 2018, 166, 1–9. [Google Scholar] [CrossRef]
- Ledig, C.; Schuh, A.; Guerrero, R.; Heckemann, R.A.; Rueckert, D. Structural brain imaging in Alzheimer’s disease and mild cognitive impairment: Biomarker analysis and shared morphometry database. Sci. Rep. 2018, 8, 11258. [Google Scholar] [CrossRef] [Green Version]
- Pini, L.; Pievani, M.; Bocchetta, M.; Altomare, D.; Bosco, P.; Cavedo, E.; Galluzzi, S.; Marizzoni, M.; Frisoni, G.B. Brain atrophy in Alzheimer’s Disease and aging. Ageing Res. Rev. 2016, 30, 25–48. [Google Scholar] [CrossRef] [PubMed]
- Bookheimer, S.Y.; Salat, D.H.; Terpstra, M.; Ances, B.M.; Barch, D.M.; Buckner, R.L.; Burgess, G.C.; Curtiss, S.W.; Diaz-Santos, M.; Elam, J.S.; et al. The Lifespan Human Connectome Project in Aging: An overview. Neuroimage 2019, 185, 335–348. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Lifshitz, M.; Dwolatzky, T.; Press, Y. Validation of the Hebrew Version of the MoCA Test as a Screening Instrument for the Early Detection of Mild Cognitive Impairment in Elderly Individuals. J. Geriatr. Psychiatry Neurol. 2012, 25, 155–161. [Google Scholar] [CrossRef]
- Dwolatzky, T.; Dimant, L.; Friger, M.; Grinshpun, Y. The evaluation of the CogSym instrument in screening older patients for dementia. In Proceedings of the 17th Biennial Meeting of the Israel Gerontological Society, Tel Aviv, Israel, 17–18 February 2008. [Google Scholar]
- Katz, J.R.; Dwolatzky, T.; Aharon-Peretz, J. The Modified Cognitive Symptom (ModCogSym) Test as a screening tool for mild cognitive impairment in older individuals. Eur. Geriatr. Med. 2019, 10, S59. [Google Scholar]
- World Health Organisation. Wellbeing Measures in Primary Health Care/The Depcare Project; World Health Organisation: Copenhagen, Denmark, 1998.
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 well-being index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Dwolatzky, T.; Whitehead, V.; Doniger, G.M.; Simon, E.S.; Schweiger, A.; Jaffe, D.; Chertkow, H. Validity of a novel computerized cognitive battery for mild cognitive impairment. BMC Geriatr 2003, 3, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doniger, G.M.; Dwolatzky, T.; Zucker, D.M.; Chertkow, H.; Crystal, H.; Schweiger, A.; Simon, E.S. Computerized cognitive testing battery identifies mild cognitive impairment and mild dementia even in the presence of depressive symptoms. Am. J. Alzheimers. Dis. Other Demen. 2006, 21, 28–36. [Google Scholar] [CrossRef]
- Feuerstein, R.; Falik, L.; Rand, Y.; Feuerstein, R. Creating and Enhancing Cognitive Modifiability: The Feuerstein Instrumental Enrichment Program; ICELP Publications: Jerusalem, Israel, 2006. [Google Scholar]
- Van de Putte, E.; De Baene, W.; García-Pentón, L.; Woumans, E.; Dijkgraaf, A.; Duyck, W. Anatomical and functional changes in the brain after simultaneous interpreting training: A longitudinal study. Cortex 2018, 99, 243–257. [Google Scholar] [CrossRef]
- Durazzo, T.C.; Mon, A.; Gazdzinski, S.; Meyerhoff, D.J. Regional brain volume changes in alcohol-dependent individuals during early abstinence: Associations with relapse following treatment. Addict. Biol. 2017, 22, 1416–1424. [Google Scholar] [CrossRef]
- Zou, X.; Durazzo, T.C.; Meyerhoff, D.J. Regional Brain Volume Changes in Alcohol-Dependent Individuals During Short-Term and Long-Term Abstinence. Alcohol. Clin. Exp. Res. 2018, 42, 1062–1072. [Google Scholar] [CrossRef]
- Diarra, M.; Zendel, B.R.; Benady-Chorney, J.; Blanchette, C.A.; Lepore, F.; Peretz, I.; Belleville, S.; West, G.L. Playing Super Mario increases oculomotor inhibition and frontal eye field grey matter in older adults. Exp. Brain Res. 2019, 237, 723–733. [Google Scholar] [CrossRef] [PubMed]
- Anderson-Hanley, C.; Barcelos, N.M.; Zimmerman, E.A.; Gillen, R.W.; Dunnam, M.; Cohen, B.D.; Yerokhin, V.; Miller, K.E.; Hayes, D.J.; Arciero, P.J.; et al. The Aerobic and Cognitive Exercise Study (ACES) for community-dwelling older adults with or at-risk for mild cognitive impairment (MCI): Neuropsychological, neurobiological and neuroimaging outcomes of a randomized clinical trial. Front. Aging Neurosci. 2018, 10, 76. [Google Scholar] [CrossRef]
- Engvig, A.; Fjell, A.M.; Westlye, L.T.; Skaane, N.V.; Dale, A.M.; Holland, D.; Due-Tønnessen, P.; Sundseth, O.; Walhovd, K.B. Effects of cognitive training on gray matter volumes in memory clinic patients with subjective memory impairment. J. Alzheimers. Dis. 2014, 41, 779–791. [Google Scholar] [CrossRef] [Green Version]
- Suo, C.; Singh, M.F.; Gates, N.; Wen, W.; Sachdev, P.; Brodaty, H.; Saigal, N.; Wilson, G.C.; Meiklejohn, J.; Singh, N.; et al. Therapeutically relevant structural and functional mechanisms triggered by physical and cognitive exercise. Mol. Psychiatry 2016, 21, 1633–1642. [Google Scholar] [CrossRef] [Green Version]
- Rehfeld, K.; Lüders, A.; Hökelmann, A.; Lessmann, V.; Kaufmann, J.; Brigadski, T.; Müller, P.; Müller, N.G. Dance training is superior to repetitive physical exercise in inducing brain plasticity in the elderly. PLoS ONE 2018, 13, e0196636. [Google Scholar] [CrossRef] [Green Version]
- De Marco, M.; Meneghello, F.; Duzzi, D.; Rigon, J.; Pilosio, C.; Venneri, A. Cognitive stimulation of the default-mode network modulates functional connectivity in healthy aging. Brain Res. Bull. 2016, 121, 26–41. [Google Scholar] [CrossRef] [Green Version]
- De Marco, M.; Meneghello, F.; Pilosio, C.; Rigon, J.; Venneri, A. Up-regulation of DMN Connectivity in Mild Cognitive Impairment via Network-based Cognitive Training. Curr. Alzheimer Res. 2017, 15, 578–589. [Google Scholar] [CrossRef] [Green Version]
- Lyu, X.; Yuan, H.; Wang, Z.; Yu, X.; Liu, Y.; Zeng, X.; Wang, J.; Zhang, H.; Wang, H.; Wang, X. Computerized multi-domain cognitive training reduces brain atrophy in patients with amnestic mild cognitive impairment. Transl. Psychiatry 2019, 9, 48. [Google Scholar] [CrossRef] [Green Version]
- Apps, M.A.J.; Lockwood, P.L.; Balsters, J.H. The role of the midcingulate cortex in monitoring others’ decisions. Front. Neurosci. 2013, 7, 251. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Group A (n = 13) | Group B (n = 10) | p-Values | |
|---|---|---|---|
| Sex | |||
| Female | 76.9% | 80.0% | 0.73 |
| Age (years) | 82.8 | 83.7 | 0.72 |
| Education (years) | 11.4 | 11.6 | 0.82 |
| MoCA | 20.9 | 22.7 | 0.06 |
| CogSym | 23.3 | 21.2 | 0.38 |
| Well-being | 18.1 | 18.6 | 0.75 |
| Region | x,y,z (mm) a | Gyri | Cluster (mm3) | Effect (%) | T Value | p (FDR) b |
|---|---|---|---|---|---|---|
| 1 | −43, −50, +43 | Left Angular | 610 | 2.13 | 5.34 | 0.043 |
| Left Supramarginal | ||||||
| Left Inferior Parietal | ||||||
| 2 | +2, −27, +40 | Left Middle Cingulate | 520 | 1.14 | 7.97 | 0.050 |
| Right Middle Cingulate | ||||||
| 3 | −45, −65, −7 | Left Inferior Temporal | 2850 | 4.19 | 7.22 | <0.001 |
| Left Fusiform | ||||||
| Left Inferior Occipital |
| Group A (n = 13) | Group B (n = 10) | Repeated Measures a | |||||
|---|---|---|---|---|---|---|---|
| Time | Pre | Post | Pre | Post | Effect | F | p-Value |
| Global Score | 91.5 (9.6) | 93.4 (7.0) | 99.2 (8.8) | 99.5 (7.6) | Time | 0.51 | 0.48 |
| Group | 4.75 | 0.04 | |||||
| Time × Group | 0.30 | 0.59 | |||||
| Memory Domain | 91.8 (13.4) | 99.7 (9.1) | 97.6 (9.7) | 99.9 (9.2) | Time | 4.29 | 0.05 |
| Group | 0.64 | 0.43 | |||||
| Time × Group | 1.32 | 0.26 | |||||
| Verbal Memory | 91.3 (17.8) | 104.3 (12.7) | 91.3 (15.5) | 101.1 (11.4) | Time | 9.48 | <0.01 |
| Group | 0.10 | 0.75 | |||||
| Time × Group | 0.19 | 0.67 | |||||
| Delayed Verbal Memory | 93.6 (21.8) | 100.6 (13.8) | 90.3 (18.9) | 101.2 (10.5) | Time | 4.40 | <0.05 |
| Group | 0.06 | 0.82 | |||||
| Time × Group | 0.21 | 0.66 | |||||
| Non-Verbal Memory | 92.7 (12.3) | 96.5 (15.1) | 103.8 (14.6) | 100.9 (17.7) | Time | 0.03 | 0.88 |
| Group | 1.95 | 0.18 | |||||
| Time × Group | 1.44 | 0.24 | |||||
| Delayed Non-Verbal Memory | 89.8 (11.7) | 97.2 (13.8) | 105.1 (10.4) | 96.1 (12.6) | Time | 0.05 | 0.82 |
| Group | 3.37 | 0.08 | |||||
| Time × Group | 5.75 | <0.05 | |||||
| Executive Functions | 92.0 (11.4) | 92.2 (8.1) | 100.6 (11.1) | 101.1 (10.4) | Time | 0.03 | 0.86 |
| Group | 5.12 | <0.05 | |||||
| Time × Group | 0.01 | 0.93 | |||||
| Attention | 91.0 (17.9) | 97.5 (11.4) | 104.5 (13.9) | 103.5 (12.9) | Time | 1.02 | 0.32 |
| Group | 3.25 | 0.09 | |||||
| Time × Group | 1.95 | 0.18 | |||||
| Visual Spatial | 91.7 (12.0) | 84.1 (11.8) | 94.2 (15.2) | 93.5 (16.2) | Time | 3.22 | 0.09 |
| Group | 1.37 | 0.26 | |||||
| Time × Group | 2.09 | 0.16 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dwolatzky, T.; Feuerstein, R.S.; Manor, D.; Cohen, S.; Devisheim, H.; Inspector, M.; Eran, A.; Tzuriel, D. Changes in Brain Volume Resulting from Cognitive Intervention by Means of the Feuerstein Instrumental Enrichment Program in Older Adults with Mild Cognitive Impairment (MCI): A Pilot Study. Brain Sci. 2021, 11, 1637. https://doi.org/10.3390/brainsci11121637
Dwolatzky T, Feuerstein RS, Manor D, Cohen S, Devisheim H, Inspector M, Eran A, Tzuriel D. Changes in Brain Volume Resulting from Cognitive Intervention by Means of the Feuerstein Instrumental Enrichment Program in Older Adults with Mild Cognitive Impairment (MCI): A Pilot Study. Brain Sciences. 2021; 11(12):1637. https://doi.org/10.3390/brainsci11121637
Chicago/Turabian StyleDwolatzky, Tzvi, Refael S. Feuerstein, David Manor, Shlomit Cohen, Haim Devisheim, Michael Inspector, Ayelet Eran, and David Tzuriel. 2021. "Changes in Brain Volume Resulting from Cognitive Intervention by Means of the Feuerstein Instrumental Enrichment Program in Older Adults with Mild Cognitive Impairment (MCI): A Pilot Study" Brain Sciences 11, no. 12: 1637. https://doi.org/10.3390/brainsci11121637