
Effects of Intraoperative Dexmedetomidine Infusion on Postoperative Pain after Craniotomy: A Narrative Review


Abstract
:1. Introduction
2. Materials and Methods
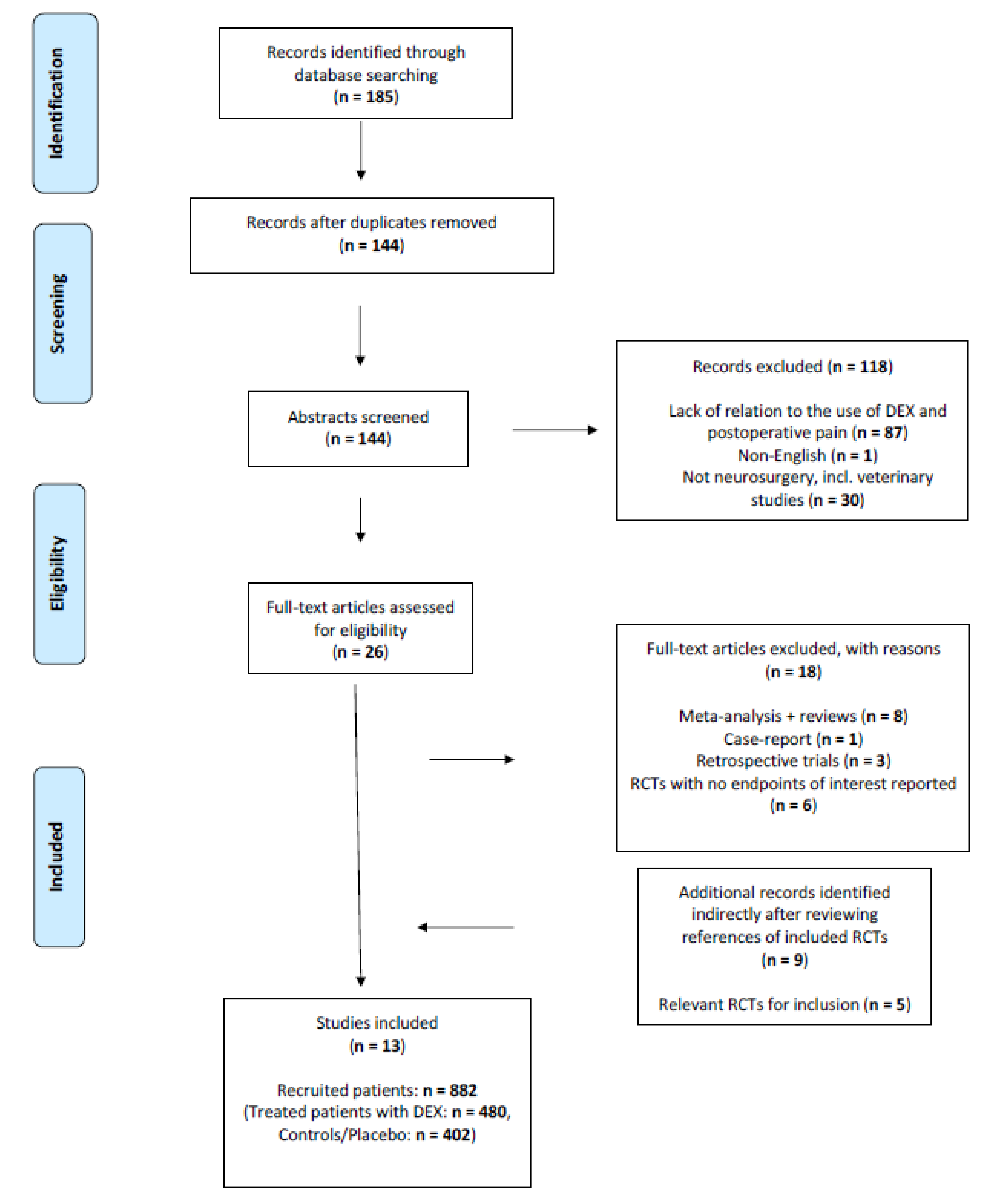
2.1. Search Strategy and Inclusion Criteria
- Clinical RCT study design.
- Patient groups >18 years of age.
- Patients underwent elective craniotomy under general anaesthesia and were extubated immediately after surgery.
- Intraoperative intravenous administration of DEX compared to any control group.
- One or several of the following outcomes reported: postoperative pain intensity, opioid/analgesic consumption at the postoperative care unit, postoperative pain-scores and/or number of patients experiencing pain at the postoperative pain unit.
- Descriptions of protocols for anaesthesia, analgesia and rescue analgesics.
- Availability of full text in English.
2.2. Outcomes of Interest
2.3. Data Extraction
3. Results
3.1. Included Trials
3.2. Pain Management
3.3. Trials Reporting Opioid Consumption in the Post-Anaesthesia Care Unit
3.4. Reported Pain Intensity in the Post-Anaesthesia Care Unit
3.5. Safety and Side Effects
4. Discussion
4.1. Pain
4.2. Haemodynamic Quality
4.3. Cost-Effectiveness
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Flexman, A.M.; Ng, J.L.; Gelb, A.W. Acute and chronic pain following craniotomy. Curr. Opin. Anaesthesiol. 2010, 23, 551–557. [Google Scholar] [CrossRef] [PubMed]
- Sriganesh, K.; Syeda, S.; Shanthanna, H.; Venkataramaiah, S.; Palaniswamy, S.R. Comparison of intraoperative fentanyl with dexmedetomidine for perioperative analgesia and opioid consumption during craniotomies: A randomised controlled pilot study with non-inferiority design. Int. J. Clin. Pract. 2019, 73, e13338. [Google Scholar] [CrossRef]
- Mosek, A.C.; Dodick, D.W.; Ebersold, M.J.; Swanson, J.W. Headache after resection of acoustic neuroma. Headache 1999, 39, 89–94. [Google Scholar] [CrossRef]
- Vacas, S.; Van de Wiele, B. Designing a pain management protocol for craniotomy: A narrative review and consideration of promising practices. Surg. Neurol. Int. 2017, 8, 291. [Google Scholar] [PubMed]
- Mordhorst, C.; Latz, B.; Kerz, T.; Wisser, G.; Schmidt, A.; Schneider, A.; Jahn-Eimermacher, A.; Werner, C.; Engelhard, K. Prospective assessment of postoperative pain after craniotomy. J. Neurosurg. Anesthesiol. 2010, 22, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Gottschalk, A.; Berkow, L.C.; Stevens, R.D.; Mirski, M.; Thompson, R.E.; White, E.D.; Weingart, J.D.; Long, D.M.; Yaster, M. Prospective evaluation of pain and analgesic use following major elective intracranial surgery. J. Neurosurg. 2007, 106, 210–216. [Google Scholar] [CrossRef]
- Peng, K.; Jin, X.H.; Liu, S.L.; Ji, F.H. Effect of Intraoperative Dexmedetomidine on Post-Craniotomy Pain. Clin. Ther. 2015, 37, 1114–1121.e1111. [Google Scholar] [CrossRef]
- de Gray, L.C.; Matta, B.F. Acute and chronic pain following craniotomy: A review. Anaesthesia 2005, 60, 693–704. [Google Scholar] [CrossRef]
- Basali, A.; Mascha, E.J.; Kalfas, I.; Schubert, A. Relation between Perioperative Hypertension and Intracranial Hemorrhage after Craniotomy. Anesthesiology 2000, 93, 48–54. [Google Scholar] [CrossRef]
- Mariappan, R.; Ashokkumar, H.; Kuppuswamy, B. Comparing the effects of oral clonidine premedication with intraoperative dexmedetomidine infusion on anesthetic requirement and recovery from anesthesia in patients undergoing major spine surgery. J. Neurosurg. Anesthesiol. 2014, 26, 192–197. [Google Scholar] [CrossRef] [Green Version]
- Venn, R.M.; Bradshaw, C.J.; Spencer, R.; Brealey, D.; Caudwell, E.; Naughton, C.; Vedio, A.; Singer, M.; Feneck, R.; Treacher, D.; et al. Preliminary UK experience of dexmedetomidine, a novel agent for postoperative sedation in the intensive care unit. Anaesthesia 1999, 54, 1136–1142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bekker, A.; Sturaitis, M.K. Dexmedetomidine for neurological surgery. Neurosurgery 2005, 57, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, E.; Ramsay, G.; Mantz, J.; Sum-Ping, S.T. The role of the alpha2-adrenoceptor agonist dexmedetomidine in postsurgical sedation in the intensive care unit. J. Intensive Care Med. 2003, 18, 29–41. [Google Scholar] [CrossRef]
- Hall, J.E.; Uhrich, T.D.; Barney, J.A.; Arain, S.R.; Ebert, T.J. Sedative, amnestic, and analgesic properties of small-dose dexmedetomidine infusions. Anesth. Analg. 2000, 90, 699–705. [Google Scholar] [CrossRef]
- Bajwa, S.; Kulshrestha, A. Dexmedetomidine: An adjuvant making large inroads into clinical practice. Ann. Med. Health Sci. Res. 2013, 3, 475–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bekker, A.; Sturaitis, M.; Bloom, M.; Moric, M.; Golfinos, J.; Parker, E.; Babu, R.; Pitti, A. The effect of dexmedetomidine on perioperative hemodynamics in patients undergoing craniotomy. Anesth. Analg. 2008, 107, 1340–1347. [Google Scholar] [CrossRef]
- Rajan, S.; Hutcherson, M.T.; Sessler, D.I.; Kurz, A.; Yang, D.; Ghobrial, M.; Liu, J.; Avitsian, R. The Effects of Dexmedetomidine and Remifentanil on Hemodynamic Stability and Analgesic Requirement After Craniotomy: A Randomized Controlled Trial. J. Neurosurg. Anesthesiol. 2016, 28, 282–290. [Google Scholar] [CrossRef] [Green Version]
- Song, J.; Ji, Q.; Sun, Q.; Gao, T.; Liu, K.; Li, L. The Opioid-sparing Effect of Intraoperative Dexmedetomidine Infusion After Craniotomy. J. Neurosurg. Anesthesiol. 2016, 28, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Turgut, N.; Turkmen, A.; Ali, A.; Altan, A. Remifentanil-propofol vs dexmedetomidine-propofol--anesthesia for supratentorial craniotomy. Middle East J. Anesthesiol. 2009, 20, 63–70. [Google Scholar]
- Yun, Y.; Wang, J.; Tang, R.R.; Yin, X.R.; Zhou, H.; Pei, L. Effects of an Intraoperative Dexmedetomidine Bolus on the Postoperative Blood Pressure and Pain Subsequent to Craniotomy for Supratentorial Tumors. J. Neurosurg. Anesthesiol. 2017, 29, 211–218. [Google Scholar] [CrossRef]
- Goettel, N.; Bharadwaj, S.; Venkatraghavan, L.; Mehta, J.; Bernstein, M.; Manninen, P.H. Dexmedetomidine vs propofol-remifentanil conscious sedation for awake craniotomy: A prospective randomized controlled trial. Br. J. Anaesth. 2016, 116, 811–821. [Google Scholar] [CrossRef] [Green Version]
- Tanskanen, P.E.; Kytta, J.V.; Randell, T.T.; Aantaa, R.E. Dexmedetomidine as an anaesthetic adjuvant in patients undergoing intracranial tumour surgery: A double-blind, randomized and placebo-controlled study. Br. J. Anaesth. 2006, 97, 658–665. [Google Scholar] [CrossRef] [Green Version]
- Günes, Y.; Gündüz, M.; Özcengiz, D.; Özbek, H.; Isik, G. Dexmedetomidine-Remifentanil or Propofol-Remifentanil Anesthesia in Patients Undergoing Intracranial Surgery. Neurosurg. Q. 2005, 15, 122–126. [Google Scholar] [CrossRef]
- Kim, H.; Min, K.T.; Lee, J.R.; Ha, S.H.; Lee, W.K.; Seo, J.H.; Choi, S.H. Comparison of Dexmedetomidine and Remifentanil on Airway Reflex and Hemodynamic Changes during Recovery after Craniotomy. Yonsei Med. J. 2016, 57, 980–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, D.; Zhao, S.; Zhang, N.; Shi, J. Brain protective effect and hemodynamics of dexmedetomidine hydrochloride in patients with intracranial aneurysm. Saudi J. Biol. Sci. 2020, 27, 1850–1855. [Google Scholar] [CrossRef]
- Prathapadas, U.; Hrishi, A.P.; Appavoo, A.; Vimala, S.; Sethuraman, M. Effect of Low-Dose Dexmedetomidine on the Anesthetic and Recovery Profile of Sevoflurane-Based Anesthesia in Patients Presenting for Supratentorial Neurosurgeries: A Randomized Double-Blind Placebo-Controlled Trial. J. Neurosci. Rural. Pract. 2020, 11, 267–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Liang, F.; Liu, X.; Shao, X.; Jiang, N.; Gan, X. Dexmedetomidine Reduces Perioperative Opioid Consumption and Postoperative Pain Intensity in Neurosurgery: A Meta-analysis. J. Neurosurg. Anesthesiol. 2018, 30, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Arain, S.R.; Ruehlow, R.M.; Uhrich, T.D.; Ebert, T.J. The efficacy of dexmedetomidine versus morphine for postoperative analgesia after major inpatient surgery. Anesth. Analg. 2004, 98, 153–158. [Google Scholar] [CrossRef]
- Xin, X.; Chen, J.; Hua, W.; Wang, H. Intraoperative dexmedetomidine for prevention of postoperative delirium in elderly patients with mild cognitive impairment. Int. J. Geriatr. Psychiatry 2021, 36, 143–151. [Google Scholar] [CrossRef]
- Halpin, E.; Inch, H.; O’Neill, M. Dexmedetomidine’s Relationship to Delirium in Patients Undergoing Cardiac Surgery: A Systematic Review. Crit. Care Nurs. Q. 2020, 43, 28–38. [Google Scholar] [CrossRef]
- Zhao, W.; Hu, Y.; Chen, H.; Wang, X.; Wang, L.; Wang, Y.; Wu, X.; Han, F. The Effect and Optimal Dosage of Dexmedetomidine Plus Sufentanil for Postoperative Analgesia in Elderly Patients With Postoperative Delirium and Early Postoperative Cognitive Dysfunction: A Single-Center, Prospective, Randomized, Double-Blind, Controlled Trial. Front. Neurosci. 2020, 14, 549516. [Google Scholar] [CrossRef]
- Guignard, B.; Bossard, A.E.; Coste, C.; Sessler, D.I.; Lebrault, C.; Alfonsi, P.; Fletcher, D.; Chauvin, M. Acute opioid tolerance: Intraoperative remifentanil increases postoperative pain and morphine requirement. Anesthesiology 2000, 93, 409–417. [Google Scholar] [CrossRef]
- Gopalakrishna, K.N.; Dash, P.K.; Chatterjee, N.; Easwer, H.V.; Ganesamoorthi, A. Dexmedetomidine as an Anesthetic Adjuvant in Patients Undergoing Transsphenoidal Resection of Pituitary Tumor. J. Neurosurg. Anesthesiol. 2015, 27, 209–215. [Google Scholar] [CrossRef]
- Gertler, R.; Brown, H.C.; Mitchell, D.H.; Silvius, E.N. Dexmedetomidine: A novel sedative-analgesic agent. Bayl. Univ. Med Cent. Proc. 2001, 14, 13–21. [Google Scholar] [CrossRef]
- Turunen, H.; Jakob, S.M.; Ruokonen, E.; Kaukonen, K.M.; Sarapohja, T.; Apajasalo, M.; Takala, J. Dexmedetomidine versus standard care sedation with propofol or midazolam in intensive care: An economic evaluation. Crit. Care 2015, 19, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dasta, J.F.; Kane-Gill, S.L.; Pencina, M.; Shehabi, Y.; Bokesch, P.M.; Wisemandle, W.; Riker, R.R. A cost-minimization analysis of dexmedetomidine compared with midazolam for long-term sedation in the intensive care unit. Crit. Care Med. 2010, 38, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.; Cheng, D. The real cost of care: Focus on value for money, rather than price-tags. Can. J. Anaesth. 2015, 62, 1034–1041. [Google Scholar] [CrossRef] [Green Version]
- Ter Bruggen, F.; Ceuppens, C.; Leliveld, L.; Stronks, D.L.; Huygen, F. Dexmedetomidine vs propofol as sedation for implantation of neurostimulators: A single-center single-blinded randomized controlled trial. Acta Anaesthesiol. Scand. 2019, 63, 1321–1329. [Google Scholar] [CrossRef] [PubMed]
- Ter Bruggen, F.; Stronks, D.L.; Huygen, F. Cost analysis of dexmedetomidine versus propofol during the implantation of a neurostimulator. Acta Anaesthesiol. Scand. 2020, 64, 861–862. [Google Scholar] [CrossRef] [PubMed]
- Fabritius, M.L.; Afshari, A. Is clinical heterogeneity the foremost prominent threat to the validity of meta-analyses? Acta Anaesthesiol. Scand. 2021, 65, 863–864. [Google Scholar] [CrossRef]


{kind=link}
| References | Country | ASA | Age (y) | Type of Surgery | DEX (n) | Control/ Placebo (n) | Bolus | Continuous Infusion (Per Hour) | Anaesthesia Protocol |
|---|---|---|---|---|---|---|---|---|---|
| Bekker, 2008 [16] | USA | I-II | 18–65 | Craniotomy (resection of brain tumour) | 28 | 28 | 1. DEX: 1 μg.kg−1 2. 0.9% Saline: 1 μg.kg−1 | 1. DEX: 0.5 μg.kg−1 2. 0.9% Saline: 0.5 μg.kg−1 | Propofol + Vecuronium + Fentanyl + Sevoflurane + Remifentanil |
| Peng, 2015 [7] | China | I-II | 18–65 | Supratentorial craniotomy | 38 | 38 | NO BOLUS | 1. DEX: 0.5 μg.kg−1 2. Saline: 0.5 μg.kg−1 | Propofol + Fentanyl + Cisatracium + Sevoflurane |
| Rajan, 2016 [17] | USA | Not mentioned | Not mentioned | Craniotomy (resection of a brain tumour) | 68 | 71 | 1. DEX: 0.5−1 μg.kg−1 2. Remifentanil: No bolus | 1. DEX:0.2–0.7 μg.kg−1 2. Remifentanil: 0.08–0.15 μg.kg−1 | Propofol + Recoronium + Fentanyl + Sevoflurane |
| Song, 2016 [18] | China | I-III | 18–60 | Supratentorial craniotomy | 25 | 27 | 1. DEX: 0.5 μg.kg−1 2. 0.9% Saline | 1. DEX: 0.2–0.5 μg.kg−1 2. 0.9% Saline | Midazolam + Fentanyl + Propofol + Remifentanil + Cisatracurium |
| Sriganesh, 2019 [2] | India | Not mentioned | 18–60 | Supratentorial craniotomy | 12 | 12 | NO BOLUS | 1. DEX: 0.5 μg.kg−1 2. Fentanyl: 1 μg.kg−1 | Thiopentone + Lignocaine + Vecuronium + Fentanyl + Isoflurane |
| Turgut, 2009 [19] | Turkey | I-III | 18–80 | Supratentorial craniotomy | 25 | 25 | 1. DEX: 1 μg.kg−1 2. Remifentanil: 1 μg.kg−1 | 1. DEX: 0.2–1 μg.kg−1 2. Remifentanil: 0.05μg.kg−1 | Propofol + Cisatracurium |
| Yun, 2017 [20] | China | I-II | 35–65 | Supratentorial craniotomy | D1: 43, D2: 46 | 45 | 1. D1: 0.4 μg.kg−1 2. D2: 0.8 μg.kg−1 3. 0.9% Saline | NO CONTINUOUS INFUSION | Pantoprazole + Propofol + Sufentanil + Cisatracurium + Sevoflurane, Remifentanil |
| Goettel, 2016 [21] | Canada | I-III | 18–80 | Supratentorial craniotomy (awake procedure) | 25 | 25 | 1. DEX: 1 μg.kg−1 2. Propofol/Remifentanil: no bolus | 1. DEX: 0.2–1 μg.kg−1 2. Propofol/Remifentanil: 25–150 μg.kg−1, 0.01–0.1 μg.kg−1 | Fentanyl + Bupivacaine |
| Tanskanen, 2006 [22] | Finland | Not mentioned | 20–65 | Supratentorial craniotomy | 35 | 18 | NO BOLUS | 1. D1: 0.2 ng.ml−1 2. D2: 0.4 ng.ml−1 3. 0.9% Saline | Fentanyl + Thiopental + Pancuronium + NO + Isoflurane |
| Günes, 2005 [23] | Turkey | I-II | 19–70 | Craniotomy (resection of vascular or space-occupying lesions) | 39 | 39 | NO BOLUS | 1. DEX: 0.6–1.2 mg.kg−1 2. Remifentanil: 0.25 μg.kg−1 | Propofol + Remifentanil + Vecuronium + NO |
| Kim, 2016 [24] | South Korea | I-II | 20–70 | Craniotomy (clipping of unruptured cerebral aneurysm) | 32 | 32 | 1. DEX: 0.5 μg.kg−1 2. Remifentanil: 0.5 μg.kg−1 | NO CONTINUOUS INFUSION | Propofol + Remifentanil + Rocuronium + Sevoflurane |
| Zheng, 2020 [25] | China | I-II | 27–59 | Craniotomy (intracranial aneurysm) | 44 | 22 | NO BOLUS | 1. D1: 1 μg.kg−1 2. D2: 0.5 μg.kg−1 3. Control: 0.9% Saline | Midazolam + Sufentanil + Atracurium + Etomidate |
| Prathapadas, 2020 [26] | India | I-II | 18–50 | Supratentorial craniotomy | 20 | 20 | NO BOLUS | 1. DEX: 0.2 μg.kg−1 2. Control: 0.9% Saline | Fentanyl + Propofol + Vecuronium + Sevoflurane |
| References | Favourable Effect of DEX | Reported p-Value Intervention vs. Control | Reported Pain Variable and Raw Numbers | Results |
|---|---|---|---|---|
| Bekker et al. [16] | No | P = 0.4151 | Opioid consumption | No significant difference between the groups |
| Peng et al. [7] | Yes | Pain scores: p < 0.05 Opioid consumption: p < 0.05 | Pain scores (VRS), also comments on opioid consumption | Lower pain scores and opioid consumption in the DEX group |
| Rajan et al. [17] | Yes | Pain scores: p < 0.001 Opioid consumption: p < 0.001 | Pain scores (VAS), also comments on opioid consumption | Lower pain scores and opioid consumption in the DEX group |
| Song et al. [18] | Yes | Pain scores: p < 0.001 Opioid consumption: p < 0.001 | Pain scores (NRS), also comments on opioid consumption | Lower pain scores and opioid consumption in the DEX group |
| Sriganesh et al. [2] | No | Pain scores: p > 0.05 | Pain scores (NRS), also comments on opioid consumption | No significant difference between the groups |
| Turgut et al. [19] | Yes | Not described | Opioid consumption | Lower opioid consumption in the DEX group |
| Yun et al. [20] | Yes | Pain scores: Difference between control- and medium-dose DEX group: p < 0.05 Difference between control- and small-dose DEX group: p < 0.05. | Number of patients having no pain with the lowest pain scores (VRS) | Number of patients without pain greater in DEX group |
| Goettel et al. [21] | Yes | Pain scores: p = 0.026 and 0.031 | Pain scores (VAS), also comments on opioid consumption | Lower pain scores and opioid consumption in the DEX group |
| Tanskanen et al. [22] | No | Not reported | Pain scores (VAS), also comments on opioid consumption | Described as not significant |
| Gunes et al. [23] | Yes | p = 0.013 | Opioid consumption | Lower opioid consumption in the DEX group |
| Kim et al. [24] | No | Pain scores: p = 0.57 Opioid consumption: p = 0.59 | Pain scores (VAS), also comments on opioid consumption | No significant difference in pain scores or opioid consumption between the groups |
| Zheng et al. [25] | Yes | p < 0.05 | Pain scores (VAS) | Lower pain scores in DEX groups compared to the control group. |
| Prathapadas et al. [26] | No | Not reported | Pain scores (VAS) | Pain scores were comparable between the groups |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Syrous, N.S.; Sundstrøm, T.; Søfteland, E.; Jammer, I. Effects of Intraoperative Dexmedetomidine Infusion on Postoperative Pain after Craniotomy: A Narrative Review. Brain Sci. 2021, 11, 1636. https://doi.org/10.3390/brainsci11121636
Syrous NS, Sundstrøm T, Søfteland E, Jammer I. Effects of Intraoperative Dexmedetomidine Infusion on Postoperative Pain after Craniotomy: A Narrative Review. Brain Sciences. 2021; 11(12):1636. https://doi.org/10.3390/brainsci11121636
Chicago/Turabian StyleSyrous, Nesjla Sofia, Terje Sundstrøm, Eirik Søfteland, and Ib Jammer. 2021. "Effects of Intraoperative Dexmedetomidine Infusion on Postoperative Pain after Craniotomy: A Narrative Review" Brain Sciences 11, no. 12: 1636. https://doi.org/10.3390/brainsci11121636