
Automated Analysis of the Two-Minute Walk Test in Clinical Practice Using Accelerometer Data

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Procedure of the 2-Min Walk Test (2MWT)
2.3. Distance Measurement with Acceleration Sensors
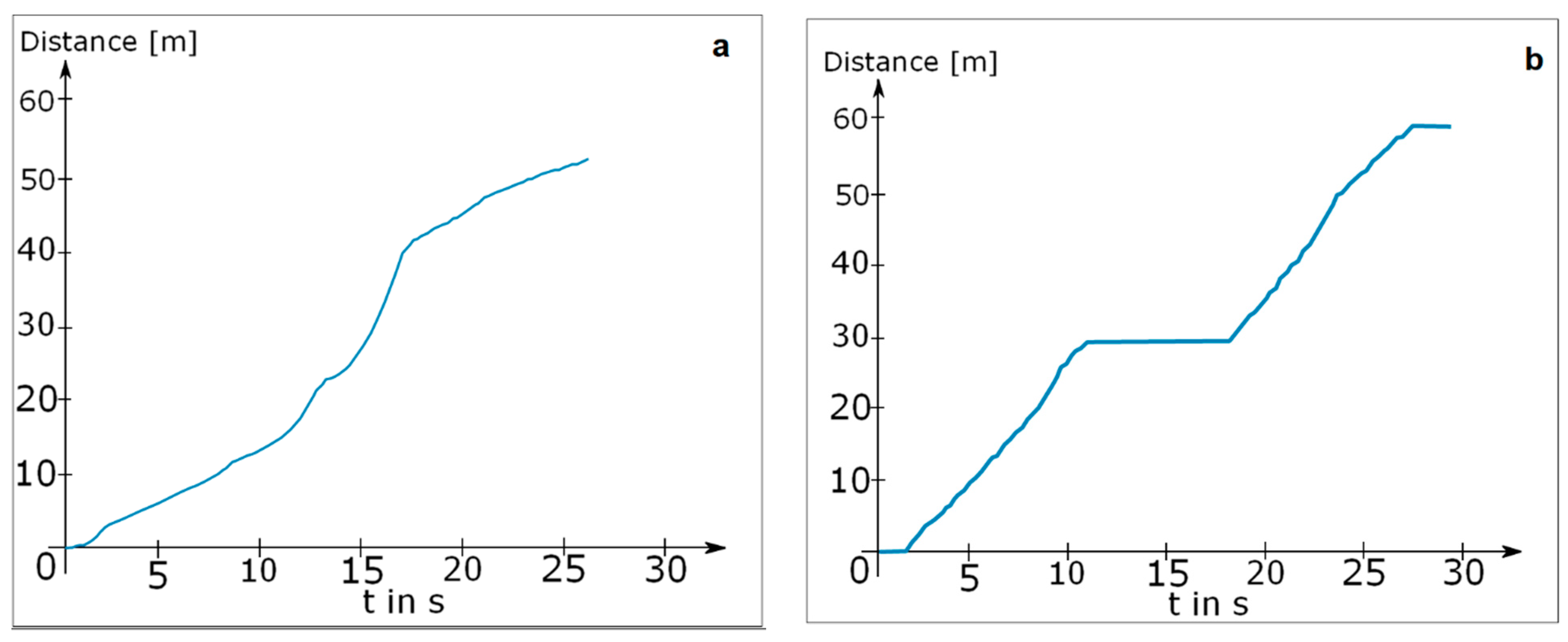
2.3.1. Digiwalk Algorithm (DWA)
2.3.2. Mobility Lab Algorithm (MLA)
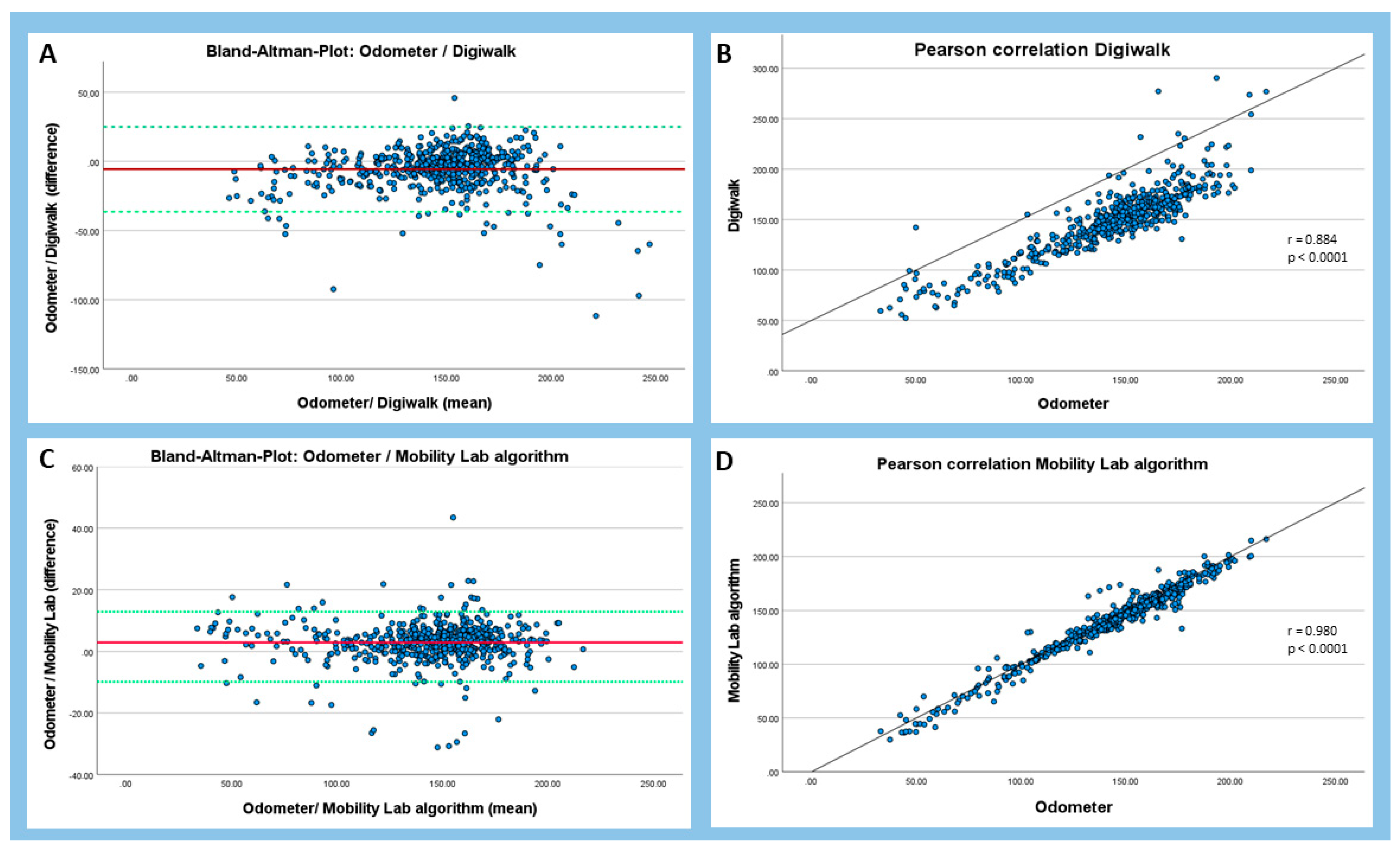
2.4. Statistical Methods
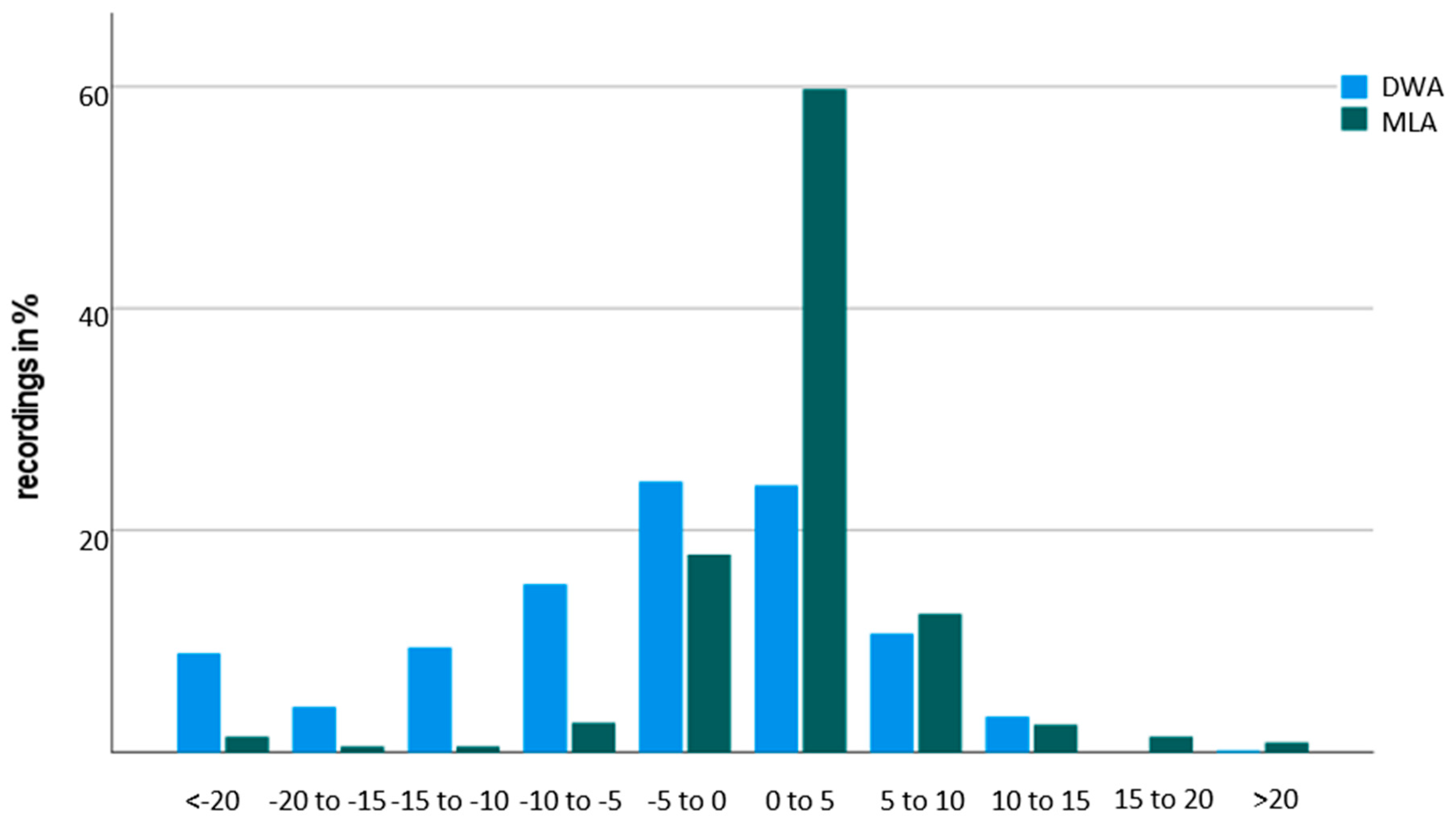
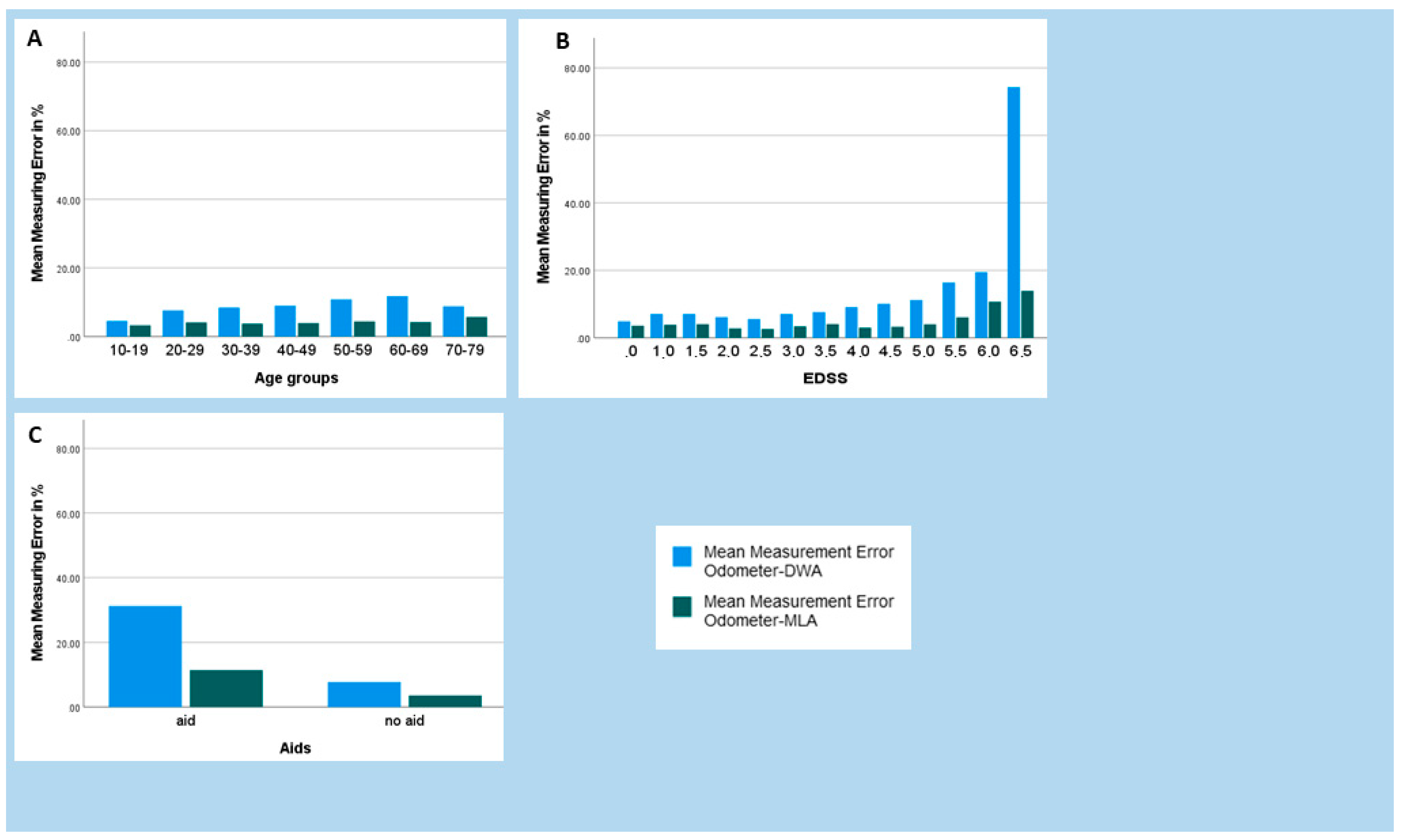
3. Results
4. Discussion
5. Future
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goldenberg, M.M. Multiple Sclerosis Review. Pharm. Ther. 2012, 37, 175–184. [Google Scholar]
- Lindner, M.; Klotz, L.; Wiendl, H. Mechanisms underlying lesion development and lesion distribution in CNS autoimmunity. J. Neurochem. 2018, 146, 122–132. [Google Scholar] [CrossRef]
- Voigt, I.; Inojosa, H.; Dillenseger, A.; Haase, R.; Akgün, K.; Ziemssen, T. Digital Twins for Multiple Sclerosis. Front. Immunol. 2021, 12, 669811. [Google Scholar] [CrossRef] [PubMed]
- Ziemssen, T.; Kern, R.; Thomas, K. Multiple sclerosis: Clinical profiling and data collection as prerequisite for personalized medicine approach. BMC Neurol. 2016, 16, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comber, L.; Sosnoff, J.J.; Galvin, R.; Coote, S. Postural control deficits in people with Multiple Sclerosis: A systematic review and meta-analysis. Gait Posture 2018, 61, 445–452. [Google Scholar] [CrossRef] [Green Version]
- Kister, I.; Chamot, E.; Salter, A.R.; Cutter, G.R.; Bacon, T.E.; Herbert, J. Disability in multiple sclerosis: A reference for patients and clinicians. Neurology 2013, 80, 1018–1024. [Google Scholar] [CrossRef] [Green Version]
- Goldman, M.D.; Marrie, R.A.; Cohen, J. Evaluation of the six-minute walk in multiple sclerosis subjects and healthy controls. Mult. Scler. J. 2008, 14, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Shanahan, C.J.; Boonstra, F.M.C.; Lizama, L.E.C.; Strik, M.; Moffat, B.A.; Khan, F.; Kilpatrick, T.J.; Van Der Walt, A.; Galea, M.P.; Kolbe, S.C. Technologies for Advanced Gait and Balance Assessments in People with Multiple Sclerosis. Front. Neurol. 2018, 8, 708. [Google Scholar] [CrossRef] [Green Version]
- Cameron, M.H.; Wagner, J.M. Gait Abnormalities in Multiple Sclerosis: Pathogenesis, Evaluation, and Advances in Treatment. Curr. Neurol. Neurosci. Rep. 2011, 11, 507–515. [Google Scholar] [CrossRef]
- Sosnoff, J.J.; Sandroff, B.; Motl, R.W. Quantifying gait abnormalities in persons with multiple sclerosis with minimal disability. Gait Posture 2012, 36, 154–156. [Google Scholar] [CrossRef]
- Dujmovic, I.; Radovanovic, S.; Martinovic, V.; Dackovic, J.; Maric, G.; Mesaros, S.; Pekmezovic, T.; Kostic, V.; Drulovic, J. Gait pattern in patients with different multiple sclerosis phenotypes. Mult. Scler. Relat. Disord. 2017, 13, 13–20. [Google Scholar] [CrossRef]
- Meyer-Moock, S.; Feng, Y.-S.; Maeurer, M.; Dippel, F.-W.; Kohlmann, T. Systematic literature review and validity evaluation of the Expanded Disability Status Scale (EDSS) and the Multiple Sclerosis Functional Composite (MSFC) in patients with multiple sclerosis. BMC Neurol. 2014, 14, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodkin, D.E.; Cookfair, D.; Wende, K.; Bourdette, D.; Pullicino, P.; Scherokman, B.; Whitham, R. Inter- and intrarater scoring agreement using grades 1.0 to 3.5 of the Kurtzke Expanded Disability Status Scale (EDSS). Neurology 1992, 42, 859–863. [Google Scholar] [CrossRef] [PubMed]
- Hobart, J.; Freeman, J.; Thompson, A. Kurtzke scales revisited: The application of psychometric methods to clinical intuition. Brain 2000, 123, 1027–1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Decavel, P.; Sagawa, Y. Gait quantification in multiple sclerosis: A single-centre experience of systematic evaluation. Neurophysiol. Clin. Neurophysiol. 2019, 49, 165–171. [Google Scholar] [CrossRef]
- Trentzsch, K.; Weidemann, M.L.; Torp, C.; Inojosa, H.; Scholz, M.; Haase, R.; Schriefer, D.; Akgün, K.; Ziemssen, T. The Dresden Protocol for Multidimensional Walking Assessment (DMWA) in Clinical Practice. Front. Neurosci. 2020, 14, 582046. [Google Scholar] [CrossRef] [PubMed]
- Scholz, M.; Haase, R.; Trentzsch, K.; Stölzer-Hutsch, H.; Ziemssen, T. Improving Digital Patient Care: Lessons Learned from Patient-Reported and Expert-Reported Experience Measures for the Clinical Practice of Multidimensional Walking Assessment. Brain Sci. 2021, 11, 786. [Google Scholar] [CrossRef] [PubMed]
- Cooper, K.H. A Means of Assessing Maximal Oxygen Intake. JAMA 1968, 203, 201–204. [Google Scholar] [CrossRef]
- Butland, R.; Pang, J.; Gross, E.; Woodcock, A.; Geddes, D. Two-, six-, and 12-minute walking tests in respiratory disease. Br. Med. J. 1982, 284, 1607–1608. [Google Scholar] [CrossRef] [Green Version]
- Gijbels, D.; Eijnde, B.; Feys, P. Comparison of the 2- and 6-minute walk test in multiple sclerosis. Mult. Scler. J. 2011, 17, 1269–1272. [Google Scholar] [CrossRef]
- Brooks, D.; Parsons, J.; Tran, D.; Jeng, B.; Gorczyca, B.; Newton, J.; Lo, V.; Dear, C.; Silaj, E.; Hawn, T. The two-minute walk test as a measure of functional capacity in cardiac surgery patients. Arch. Phys. Med. Rehabil. 2004, 85, 1525–1530. [Google Scholar] [CrossRef]
- Rossier, P.; Wade, D. Validity and reliability comparison of 4 mobility measures in patients presenting with neurologic impairment. Arch. Phys. Med. Rehabil. 2001, 82, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Scalzitti, D.; Harwood, K.J.; Maring, J.R.; Leach, S.J.; Ruckert, E.A.; Costello, E. Validation of the 2-Minute Walk Test with the 6-Minute Walk Test and Other Functional Measures in Persons with Multiple Sclerosis. Int. J. MS Care 2018, 20, 158–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Messrädern, P. Merkblatt. 2015, pp. 1–9. Available online: https://www.ptb.de/cms/fileadmin/internet/fachabteilungen/abteilung_5/5.4_interferometrie_an_masverkoerperungen/5.45/merkblatt/Merkblatt_Messrad_a2.pdf (accessed on 20 May 2021).
- Créange, A.; Serre, I.; Levasseur, M.; Audry, D.; Nineb, A.; Boerio, D.; Moreau, T.; Maison, P.; Sindefi-Sep, R. Walking capacities in multiple sclerosis measured by global positioning system odometer. Mult. Scler. J. 2007, 13, 220–223. [Google Scholar] [CrossRef]
- Donovan, K.; Lord, S.; McNaughton, H.K.; Weatherall, M. Mobility beyond the clinic: The effect of environment on gait and its measurement in community-ambulant stroke survivors. Clin. Rehabil. 2008, 22, 556–563. [Google Scholar] [CrossRef] [PubMed]
- Stockman, J. Six-Minute Walk Test in Children and Adolescents. Yearb. Pediatr. 2007, 150, 395–399. [Google Scholar] [CrossRef]
- Peralta-Brenes, M.; Briceño-Torres, J.M.; Chacón-Araya, Y.; Moncada-Jiménez, J.; Villanea, M.S.; Johnson, D.K.; Campos-Salazar, C. Prediction of Peak Aerobic Power among Costa Rican Older Adults. J. Clin. Diagn. Res. 2018, 12, CC01–CC04. [Google Scholar] [CrossRef]
- Scholz, M.; Haase, R.; Schriefer, D.; Voigt, I.; Ziemssen, T. Electronic Health Interventions in the Case of Multiple Sclerosis: From Theory to Practice. Brain Sci. 2021, 11, 180. [Google Scholar] [CrossRef]
- Storm, F.A.; Cesareo, A.; Reni, G.; Biffi, E. Wearable Inertial Sensors to Assess Gait during the 6-Minute Walk Test: A Systematic Review. Sensors 2020, 20, 2660. [Google Scholar] [CrossRef]
- Brooks, G.C.; Vittinghoff, E.; Iyer, S.; Tandon, D.; Kuhar, P.; Madsen, K.A.; Marcus, G.M.; Pletcher, M.J.; Olgin, J.E. Accuracy and Usability of a Self-Administered 6-Minute Walk Test Smartphone Application. Circ. Heart Fail. 2015, 8, 905–913. [Google Scholar] [CrossRef] [Green Version]
- Retory, Y.; David, P.; Niedzialkowski, P.; De Picciotto, C.; Bonay, M.; Petitjean, M. Gait Monitoring and Walk Distance Estimation with an Accelerometer During 6-Minute Walk Test. Respir. Care 2019, 64, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Vienne-Jumeau, A.; Oudre, L.; Moreau, A.; Quijoux, F.; Edmond, S.; Dandrieux, M.; Legendre, E.; Vidal, P.P.; Ricard, D. Personalized Template-Based Step Detection from Inertial Measurement Units Signals in Multiple Sclerosis. Front. Neurol. 2020, 11, 261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wearable Sensors—APDM Wearable Technologies. Available online: https://apdm.com/mobility/ (accessed on 31 May 2020).
- Spain, R.; George, R.S.; Salarian, A.; Mancini, M.; Wagner, J.; Horak, F.; Bourdette, D. Body-worn motion sensors detect balance and gait deficits in people with multiple sclerosis who have normal walking speed. Gait Posture 2012, 35, 573–578. [Google Scholar] [CrossRef] [Green Version]
- Mancini, M.; Horak, F.B. Potential of APDM mobility lab for the monitoring of the progression of Parkinson’s disease. Expert Rev. Med. Devices 2016, 13, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Mancini, M.; Salarian, A.; Carlson-Kuhta, P.; Zampieri, C.; King, L.; Chiari, L.; Horak, F.B. ISway: A sensitive, valid and reliable measure of postural control. J. Neuroeng. Rehabil. 2012, 9, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Killeen, T.; Elshehabi, M.; Filli, L.; Hobert, M.A.; Hansen, C.; Rieger, D.; Brockmann, K.; Nussbaum, S.; Zörner, B.; Bolliger, M.; et al. Arm swing asymmetry in overground walking. Sci. Rep. 2018, 8, 12803. [Google Scholar] [CrossRef] [PubMed]
- Washabaugh, E.P.; Kalyanaraman, T.; Adamczyk, P.; Claflin, E.S.; Krishnan, C. Validity and repeatability of inertial measurement units for measuring gait parameters. Gait Posture 2017, 55, 87–93. [Google Scholar] [CrossRef] [Green Version]
- Werner, C.; Heldmann, P.; Hummel, S.; Bauknecht, L.; Bauer, J.M.; Hauer, K. Concurrent Validity, Test-Retest Reliability, and Sensitivity to Change of a Single Body-Fixed Sensor for Gait Analysis during Rollator-Assisted Walking in Acute Geriatric Patients. Sensors 2020, 20, 4866. [Google Scholar] [CrossRef] [PubMed]
- APDM Wearable Technologies Inc. User Guide Mobility Lab; APDM Wearable Technologies Inc.: Portland, OR, USA, 2020. [Google Scholar]
- Weidemann, M.L.; Trentzsch, K.; Torp, C.; Ziemssen, T. Remote-Sensoring—Neue Optionen des Progressionsmonitorings bei Multipler Sklerose. Nervenarzt 2019, 90, 1239–1244. [Google Scholar] [CrossRef] [PubMed]
- Foxlin, E.; Intersense, A. Pedestrian tracking with shoe-mounted inertial sensors. IEEE Comput. Graph. Appl. 2005, 25, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Bebek, O.; Suster, M.A.; Rajgopal, S.; Fu, M.J.; Huang, X.; Cavusoglu, M.C.; Young, D.J.; Mehregany, M.; Bogert, A.J.V.D.; Mastrangelo, C.H. Personal navigation via shoe mounted inertial measurement units. ISEEE Trans. Instrum. Meas. 2010, 59, 3018–3027. [Google Scholar] [CrossRef]
- Capela, N.; Lemaire, E.D.; Baddour, N. Novel algorithm for a smartphone-based 6-minute walk test application: Algorithm, application development, and evaluation. J. Neuroeng. Rehabil. 2015, 12, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropract. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Creagh, A.P.; Simillion, C.; Bourke, A.K.; Scotland, A.; Lipsmeier, F.; Bernasconi, C.; van Beek, J.; Baker, M.; Gossens, C.; Lindemann, M.; et al. Smartphone- and Smartwatch-Based Remote Characterisation of Ambulation in Multiple Sclerosis During the Two-Minute Walk Test. IEEE J. Biomed. Health Inform. 2020, 25, 838–849. [Google Scholar] [CrossRef]
- Karle, V.; Hartung, V.; Ivanovska, K.; Mäurer, M.; Flachenecker, P.; Pfeifer, K.; Tallner, A. The Two-Minute Walk Test in Persons with Multiple Sclerosis: Correlations of Cadence with Free-Living Walking Do Not Support Ecological Validity. Int. J. Environ. Res. Public Health 2020, 17, 9044. [Google Scholar] [CrossRef]
- Truong, P.H.; Lee, J.; Kwon, A.-R.; Jeong, G.-M. Stride Counting in Human Walking and Walking Distance Estimation Using Insole Sensors. Sensors 2016, 16, 823. [Google Scholar] [CrossRef]
- El-Gohary, M.; Pearson, S.; McNames, J.; Mancini, M.; Horak, F.; Mellone, S.; Chiari, L. Continuous Monitoring of Turning in Patients with Movement Disability. Sensors 2013, 14, 356–369. [Google Scholar] [CrossRef] [Green Version]
- Cheng, W.-Y.; Bourke, A.K.; Lipsmeier, F.; Bernasconi, C.; Belachew, S.; Gossens, C.; Graves, J.S.; Montalban, X.; Lindemann, M. U-turn speed is a valid and reliable smartphone-based measure of multiple sclerosis-related gait and balance impairment. Gait Posture 2021, 84, 120–126. [Google Scholar] [CrossRef]
- Trentzsch, K.; Schumann, P.; Śliwiński, G.; Bartscht, P.; Haase, R.; Schriefer, D.; Zink, A.; Heinke, A.; Jochim, T.; Malberg, H.; et al. Using Machine Learning Algorithms for Identifying Gait Parameters Suitable to Evaluate Subtle Changes in Gait in People with Multiple Sclerosis. Brain Sci. 2021, 11, 1049. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| pwMS (n = 562) | ||
|---|---|---|
| Mean age (years; mean ± SD) | 43.15 ± 12.31 | |
| Females (N, %) | 392 (69.8%) | |
| Disease duration (years; mean ± SD) | 8.57 ± 7.51 | |
| MS Subtype | ||
| RRMS (N, %) | 490 (87.2%) | |
| PPMS (N, %) | 55 (9.8%) | |
| SPMS (N, %) | 13 (3.0%) | |
| EDSS (median, IQR) | 2.5 (1.5–3.5) | |
| Aids | ||
| with | 35 (6.2%) | |
| without | 527 (93.8%) | |
| 2MWT | ||
| 2MWT with odometer in m (mean, SD) | 143.52 ± 32.57 | |
| 2MWT with Digiwalk in m (mean, SD) | 149.20 ± 32.33 | |
| 2MWT with MobiLab in m (mean, SD) | 140.61 ± 32.58 | |
| With Aids | Without Aids | p | |
|---|---|---|---|
| 2MWT OM | 70.98 ± 22.89 | 148.34 ± 29.91 | <0.001 |
| 2MWT DWA | 85.42 ± 16.55 | 153.44 ± 28.44 | <0.001 |
| 2MWT ML | 66.16 ± 23.19 | 145.55 ± 26.53 | <0.001 |
| Difference OM-DWA | −14.44 ± 16.39 | −5.10 ± 15.44 | 0.001 |
| Difference OM-MLA | 4.82 ± 7.28 | 2.79 ± 6.45 | 0.074 |
| Measurement Error DWA | Measurement Error MLA | |||
|---|---|---|---|---|
| Age | τ | 0.173 ** | 0.091 ** | |
| Sex | τ | 0.041 | −0.007 | |
| Aids | τ | −0.159 ** | 0.147 | |
| Disease Duration | τ | 0.073 * | 0.001 | |
| Disease Disability (EDSS) | τ | 0.241 ** | −0.029 | |
| Parameter of gait | ||||
| Cadence | τ | −0.116 ** | 0.155 ** | |
| Stride Length | τ | −0.191 ** | 0.119 ** | |
| Double Support | τ | 0.359 ** | −0.010 | |
| Gait speed | τ | −0.184 ** | 0.143 ** | |
| Lateral Step variability | τ | 0.177 ** | 0.075 ** | |
| Number of turns | τ | −0.164 ** | 0.051 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trentzsch, K.; Melzer, B.; Stölzer-Hutsch, H.; Haase, R.; Bartscht, P.; Meyer, P.; Ziemssen, T. Automated Analysis of the Two-Minute Walk Test in Clinical Practice Using Accelerometer Data. Brain Sci. 2021, 11, 1507. https://doi.org/10.3390/brainsci11111507
Trentzsch K, Melzer B, Stölzer-Hutsch H, Haase R, Bartscht P, Meyer P, Ziemssen T. Automated Analysis of the Two-Minute Walk Test in Clinical Practice Using Accelerometer Data. Brain Sciences. 2021; 11(11):1507. https://doi.org/10.3390/brainsci11111507
Chicago/Turabian StyleTrentzsch, Katrin, Benjamin Melzer, Heidi Stölzer-Hutsch, Rocco Haase, Paul Bartscht, Paul Meyer, and Tjalf Ziemssen. 2021. "Automated Analysis of the Two-Minute Walk Test in Clinical Practice Using Accelerometer Data" Brain Sciences 11, no. 11: 1507. https://doi.org/10.3390/brainsci11111507