
The Potential Impact of Digital Biomarkers in Multiple Sclerosis in The Netherlands: An Early Health Technology Assessment of MS Sherpa

 ,
,
Abstract
:1. Introduction
1.1. eHealth Interventions in MS
1.2. (Early) Health Technology Assessment ((e)HTA)
2. Materials and Methods
2.1. Early Health Technology Assesment (HTA), Concept and Analyses
standard care) = € per QALY
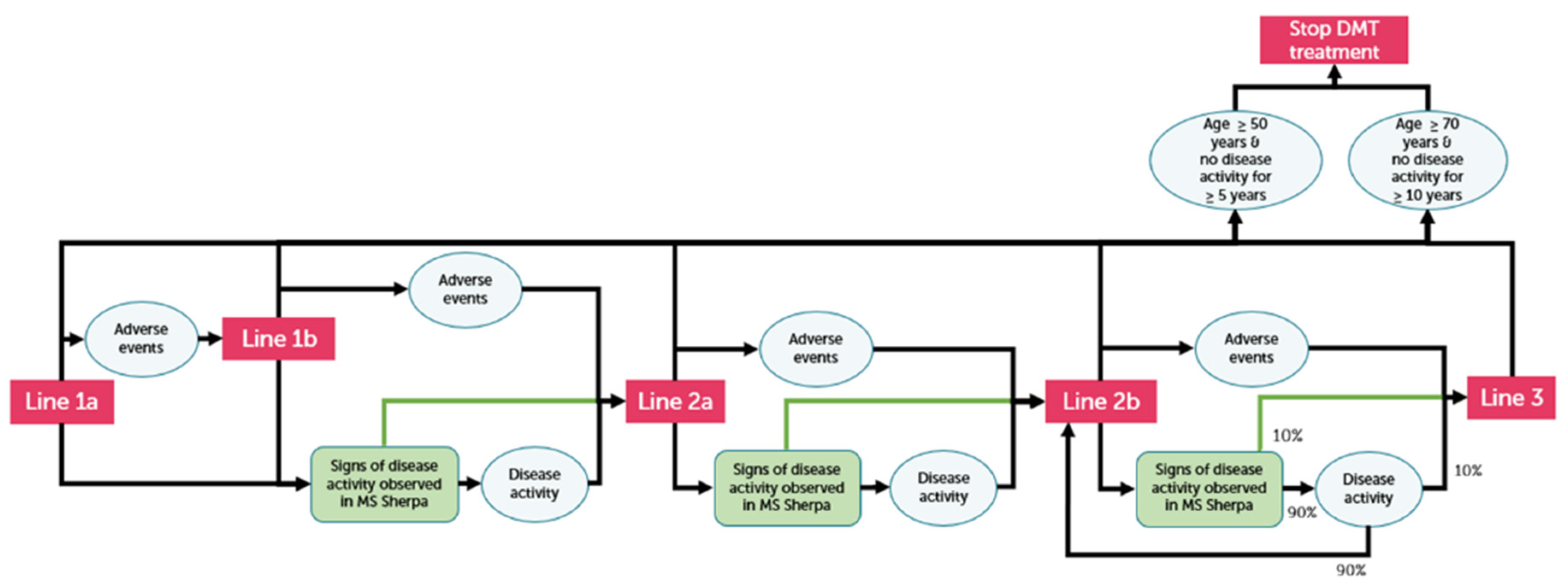
2.2. MS Model and Clinical, Costs and Quality of Life Input
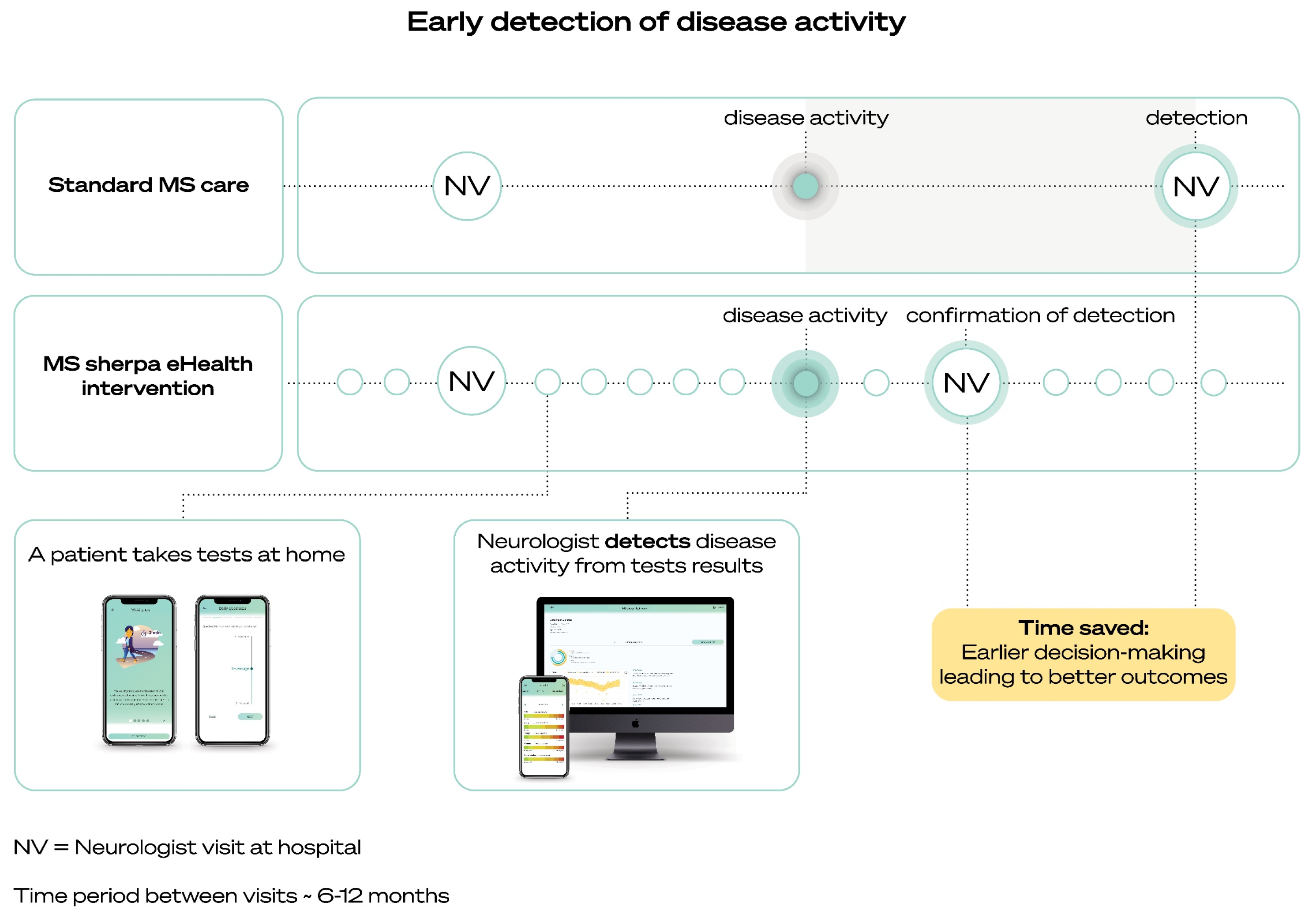
2.3. MS Sherpa and Potential Effects
3. Results
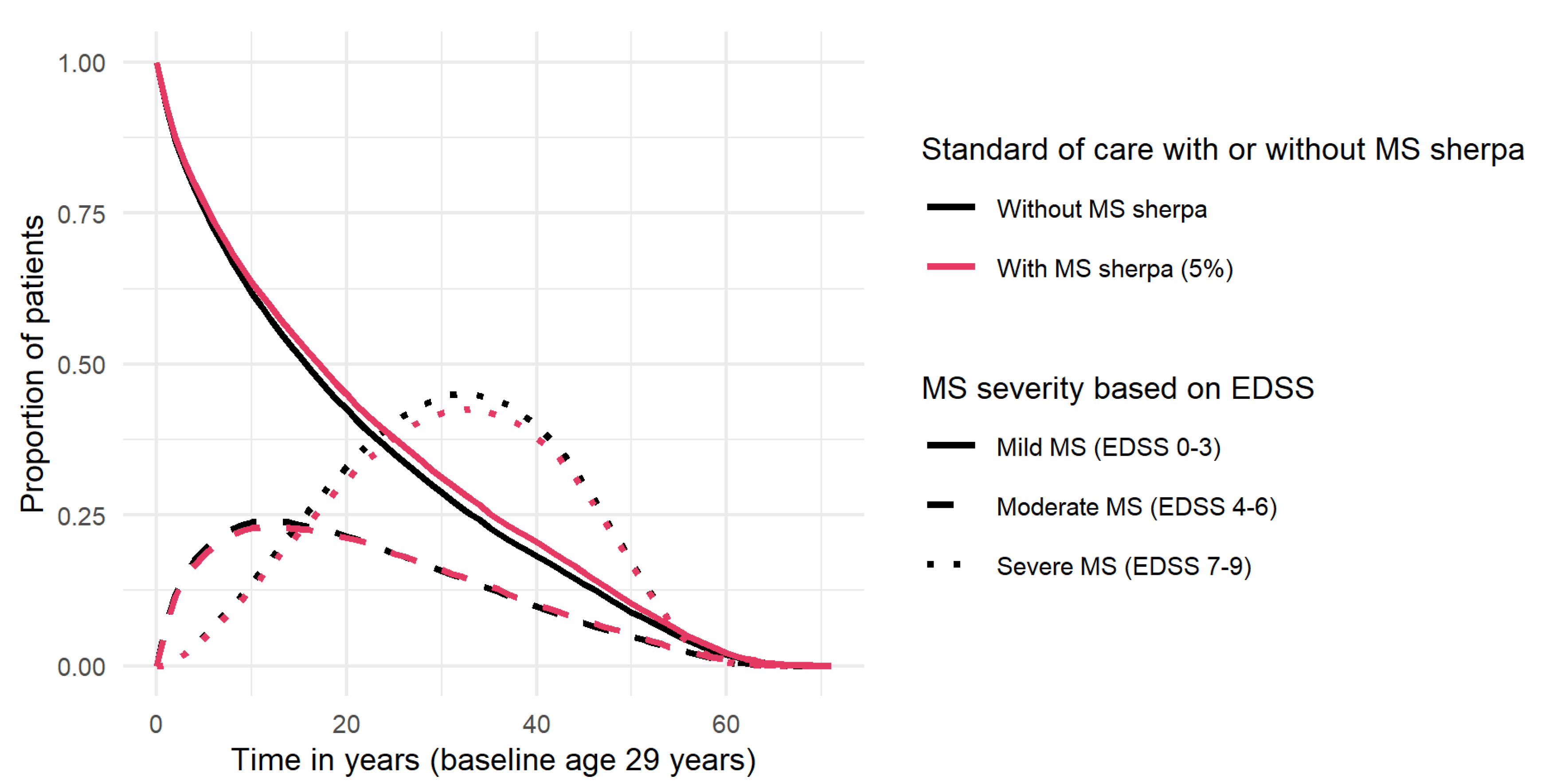
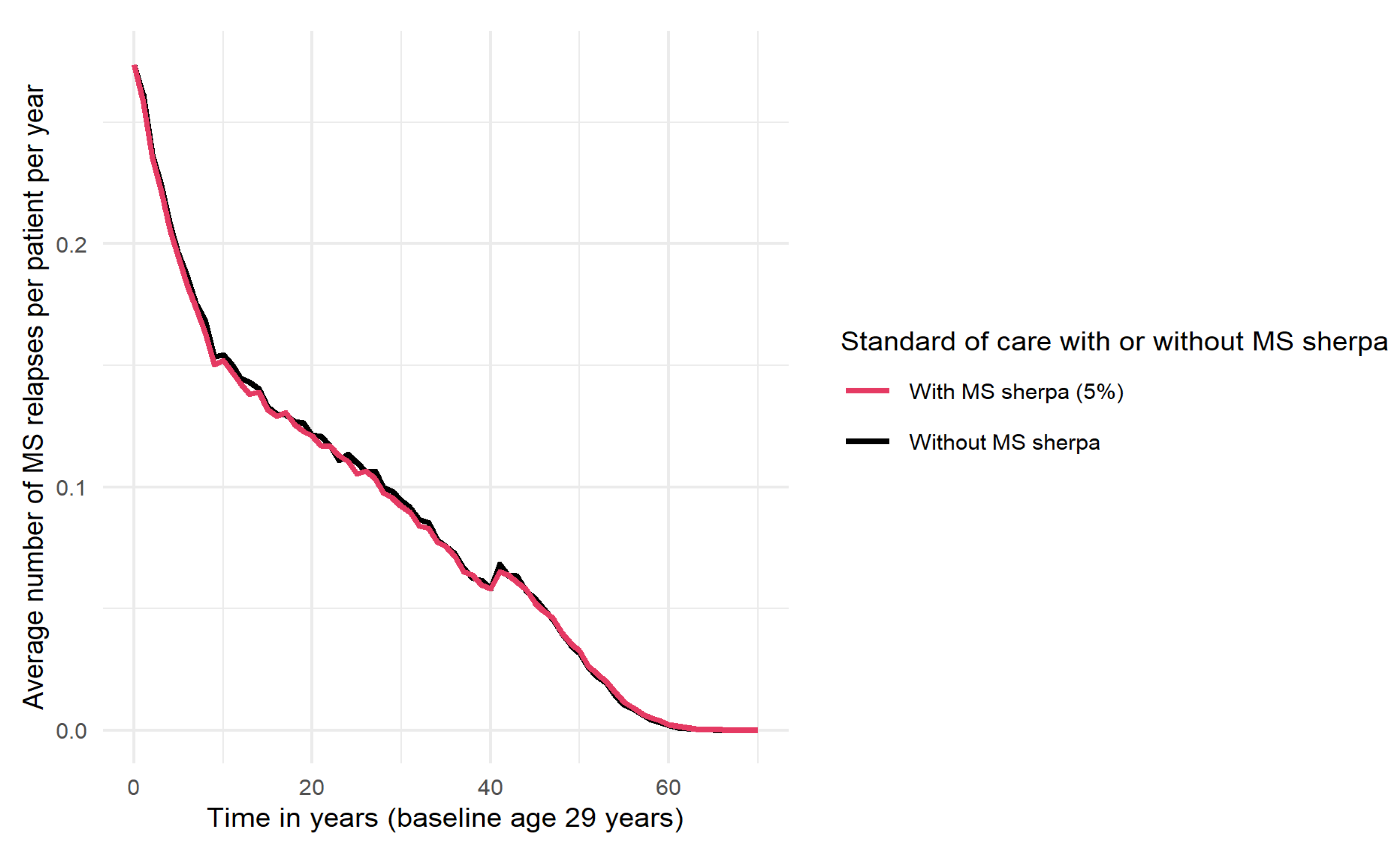
3.1. Clinical Effects (Benefits) of MS Sherpa (Modeled)
3.2. Cost-Effectiveness of MS Sherpa, Societal Perspective
3.3. Cost-Effectiveness of MS Sherpa, Health Care Perspective
3.4. Sensitivity Analysis, Tornado Diagram
4. Discussion
4.1. Principal Results and Implications for Clinical Practice and MS Society
4.2. Relation to Previous Work
4.3. Considerations and Limitations
4.4. Further Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scholz, M.; Haase, R.; Schriefer, D.; Voigt, I.; Ziemssen, T. Electronic Health Interventions in the Case of Multiple Sclerosis: From Theory to Practice. Brain Sci. 2021, 11, 180. [Google Scholar] [CrossRef]
- Baumol, W.J. Health care, education and the cost disease. A looming crisis for public choice. Public Choice 1993, 77, 17–28. Available online: https://www.jstor.org/stable/30027203 (accessed on 15 June 2021). [CrossRef]
- Embrey, N. Multiple sclerosis: Managing a complex neurological disease. Nurs. Stand. 2014, 29, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Compston, A.; Coles, A. Multiple sclerosis. Lancet 2002, 359, 1221–1231. [Google Scholar] [CrossRef]
- Tillery, E.; Clements, J.; Howard, Z. What’s new in multiple sclerosis? Ment. Health Clin. 2017, 7, 213–220. [Google Scholar] [CrossRef]
- Gasperini, C.; Prosperini, L.; Tintoŕe, M.; Sormani Filippi, M.; Rio, J.; Palace, J.; Rocca, M.A.; Ciccarelli, O.; Barkhof, F.; Sastre-Garriga, J.; et al. MAGNIMS Study Group. Unraveling treatment response in multiple sclerosis: A clinical and MRI challenge. Neurology 2019, 92, 180–192. [Google Scholar] [CrossRef] [PubMed]
- Giovannoni, G.; Butzkueven, H.; Dhib-Jalbut, S.; Hobart, J.; Kobelt, G.; Pepper, G.; Sormani, M.P.; Thalheim, C.; Traboulsee, A.; Vollmer, T. Brain Health, Time Matters in Multiple Sclerosis; Oxford Pharma Genesis Ltd.: Oxford, UK, 2015; Reprinted 2017; pp. 46–47. Available online: https://www.msbrainhealth.org/wp-content/uploads/2021/05/brain-health-time-matters-in-multiple-sclerosis-policy-report-1-1.png (accessed on 29 July 2021).
- The Dutch Society for Neurology. 2012. Available online: https://richtlijnendatabase.nl/richtlijn/multipele_sclerose_2012/multipele_sclerose_-_startpagina_2012.html (accessed on 29 July 2021).
- The Dutch Society for Neurology. 2020. Available online: https://richtlijnendatabase.nl/richtlijn/ziektemodulerende_behandeling_van_multiple_sclerose_bij_volwassenen/radiologically_isolated_syndrome.html (accessed on 29 July 2021).
- Marziniak, M.; Brichetto, G.; Feys, P.; Meyding-Lamadé, U.; Vernon, K.; Meuth, S.G. The Use of Digital and Remote Communication Technologies as a Tool for Multiple Sclerosis Management: Narrative Review. JMIR Rehabil. Assist. Technol. 2018, 5, e5. [Google Scholar] [CrossRef] [PubMed]
- Landtblom, A.M.; Guala, D.; Martin, C.; Olsson-Hau, S.; Haghighi, S.; Jansson, L.; Fredrikson, S. RebiQoL: A randomized trial of telemedicine patient support program for health-related quality of life and adherence in people with MS treated with Rebif. PLoS ONE 2019, 14, e0218453. [Google Scholar] [CrossRef] [PubMed]
- Mercier, H.W.; Ni, P.; Houlihan, B.V.; Jette, A.M. Differential impact and use of a telehealth intervention by persons with MS or SCI. Am. J. Phys. Med. Rehabil. 2015, 94, 987–999. [Google Scholar] [CrossRef] [PubMed]
- Kahraman, T.; Savci, S.; Ozdogar, A.T.; Gedik, Z.; Idiman, E. Physical, cognitive and psychosocial effects of telerehabilitation-based motor imagery training in people with multiple sclerosis: A randomized controlled pilot trial. J. Telemed. Telecare 2020, 26, 251–260. [Google Scholar] [CrossRef]
- Van Oirschot, P.; Heerings, M.; Wendrich, K.; Den Teuling, B.; Martens, M.; Jongen, P.J. Symbol Digit Modalities Test Variant in a Smartphone App for Persons With Multiple Sclerosis: Validation Study. JMIR Mhealth Uhealth 2020, 8, e18160. [Google Scholar] [CrossRef]
- Lam, K.H.; Van Oirschot, P.; Den Teuling, B.; Hulst, H.; De Jong, B.; Uitdehaag, B.; De Groot, V.; Killestein, J. Reliability, construct and concurrent validity of a smartphone-based cognition test in multiple sclerosis. Mult. Scler. J. 2021. [Google Scholar] [CrossRef] [PubMed]
- Van Oirschot, P.; Heerings, M.; Wendrich, K.; Den Teuling, B.; Dorssers, F.; Van Ee, R.; Martens, M.; Jongen, P.J. Two Minute Walking Test with a Smartphone App for Persons with Multiple Sclerosis: Validation Study. JMIR Mhealth Uhealth 2021. submitted. [Google Scholar]
- International Electrotechnical Commission, IEC 62366-1: 2015 Medical Devices—Part 1: Application of Usability Engineering to Medical Devices. Available online: https://webstore.iec.ch/publication/67220 (accessed on 30 July 2021).
- International Electrotechnical Commission, IEC TR 62366-2: 2016 Medical Devices—Part 2: Guidance on the Application of Usability Engineering to Medical Devices. Available online: https://webstore.iec.ch/publication/24664 (accessed on 30 July 2021).
- Conway, N.; Webster, C.; Smith, B.; Wake, D. eHealth and the use of individually tailored information: A systematic review. Health Inform. J. 2017, 23, 218–233. [Google Scholar] [CrossRef] [Green Version]
- Wendrich, K.; Van Oirschot, P.; Martens, M.; Heerings, M.; Jongen, P.; Krabbenborg, L. Toward Digital Self-monitoring of Multiple Sclerosis: Investigating First Experiences, Needs, and Wishes of People with MS. Int. J. MS Care 2019, 21, 282–291. [Google Scholar] [CrossRef] [Green Version]
- Midalgia, L.; Mulero, P.; Montalban, X.; Graves, J.; Hauser, S.L.; Julian, L.; Baker, M.; Schadrack, J.; Gossens, C.; Scotland, A.; et al. Adherence and satisfaction of smartphone- and smartwatch-based remote active testing and passive monitoring in people with multiple sclerosis: Nonrandomized interventional feasibility study. J. Med. Int. Res. 2019, 21, e14863. [Google Scholar]
- Maillart, E.; Labauge, P.; Cohen, M.; Maarouf, A.; Vukusic, S.; Donze, C.; De Seze, J.; Bourre, B.; Moreau, T.; Bieuvelet, S.; et al. Acceptability in clinical practice of MSCopilot®, a smartphone application for the digital self-assessment of patients living with MS. ECTRIMS Online Libr. 2018, E228545, P702. [Google Scholar]
- Brouwer, W.; Van Baal, P.; Van Exel, J.; Versteegh, M. When is it too expensive? Cost-effectiveness thresholds and health care decision-making. Eur. J. Health Econ. 2019, 20, 175–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Health Care Institute. Ziektelast in de Praktijk De theorie en Praktijk Van Het Berekenen Van Ziektelast Bij Pakketbeoordelingen. 2018. Available online: https://www.zorginstituutnederland.nl/binaries/zinl/documenten/rapport/2018/05/07/ziektelast-in-de-praktijk/Ziektelast+in+de+praktijk_definitief.pdf (accessed on 29 July 2021).
- Huygens, S.; Versteegh, M. Modeling the cost-utility of treatment sequences for multiple sclerosis. Value Health 2021. [Google Scholar] [CrossRef]
- National Health Care Institute. Richtlijn Voor Het Uitvoeren Van Economische Evaluaties in De Gezondheidszorg. 2016. Available online: https://www.zorginstituutnederland.nl/binaries/zinl/documenten/publicatie/2016/02/29/richtlijn-voor-het-uitvoeren-van-economische-evaluaties-in-de-gezondheidszorg/richtlijn-voor-het-uitvoeren-van-economische-evaluaties-in-de-gezondheidszorg.pdf (accessed on 15 May 2021).
- Benedict, R.H.; De Luca, J.; Phillips, G.; LaRocca, N.; Hudson, L.; Rudick, R. Multiple Sclerosis Outcome Assessments Consortium. Validity of the Symbol Digit Modalities Test as a cognition performance outcome measure for multiple sclerosis. Mult. Scler. J. 2017, 23, 721–733. [Google Scholar] [CrossRef]
- Pardini, M.; Uccelli, A.; Grafman, J.; Yaldizli, O.; Mancardi, G.; Roccatagliata, L. Isolated cognitive relapses in multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2014, 85, 1035–1037. [Google Scholar] [CrossRef] [PubMed]
- Morrow, S.; Jurgensen, S.; Forrestal, F.; Munchauer, F.; Benedict, R. Effects of acute relapses on neuropsychological status in multiple sclerosis patients. J. Neurol. 2011, 258, 1603–1608. [Google Scholar] [CrossRef] [PubMed]
- Bethoux, F.; Bennett, S. Evaluating walking in patients with multiple sclerosis: Which assessment tools are useful in clinical practice? Int. J. MS Care 2011, 13, 4–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, K.H.; Bucur, I.G.; Oirschot, P.; de Graaf, F.; Weda, H.; Uitdehaag, B.; Heskes, T.; Killestein, J.; de Groot, V. Smartphone-based monitoring of cognition in multiple sclerosis. 2021; in preparation. [Google Scholar]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [Green Version]
- Noyes, K.; Bajorska, A.; Chappel, A.; Schwid, S.R.; Mehta, L.R.; Weinstock-Guttman, B.; Holloway, R.G.; Dick, A.W. Cost-effectiveness of disease-modifying therapy for multiple sclerosis, A population-based study. Neurology 2011, 77, 355–363. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, A.S.; Halamka, J.D.; Kinkel, R.P. Internet portal use in an academic multiple sclerosis center. J. Am. Med. Inform. Assoc. JAMIA 2012, 19, 128–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Difference between Standard Care and MS Sherpa | ||||
|---|---|---|---|---|---|
| Scenario | Costs | QALYs | Costs | QALYs | ICER |
| MS standard Care | €614,732 | 20.51 | |||
| MS sherpa 5% | €620,990 | 20.94 | €6258 | 0.43 | €14,535 |
| MS sherpa 10% | €618,288 | 21.38 | €3556 | 0.87 | €4069 |
| MS sherpa 15% | €614,538 | 21.84 | €−194 | 1.33 | D |
| MS sherpa 20% | €611,073 | 22.29 | €−3659 | 1.78 | D |
| Total | Difference between Standard Care and MS Sherpa | ||||
|---|---|---|---|---|---|
| Scenario | Costs | QALYs | Costs | QALYs | ICER |
| MS Standard Care | €540,345 | 20.51 | |||
| MS sherpa 5% | €539,528 | 20.94 | €9183 | 0.43 | €21,328 |
| MS sherpa 10% | €539,803 | 21.38 | €9458 | 0.87 | €10,822 |
| MS sherpa 15% | €539,101 | 21.84 | €8756 | 1.33 | €6574 |
| MS sherpa 20% | €538,703 | 22.29 | €8358 | 1.78 | €4696 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cloosterman, S.; Wijnands, I.; Huygens, S.; Wester, V.; Lam, K.-H.; Strijbis, E.; den Teuling, B.; Versteegh, M. The Potential Impact of Digital Biomarkers in Multiple Sclerosis in The Netherlands: An Early Health Technology Assessment of MS Sherpa. Brain Sci. 2021, 11, 1305. https://doi.org/10.3390/brainsci11101305
Cloosterman S, Wijnands I, Huygens S, Wester V, Lam K-H, Strijbis E, den Teuling B, Versteegh M. The Potential Impact of Digital Biomarkers in Multiple Sclerosis in The Netherlands: An Early Health Technology Assessment of MS Sherpa. Brain Sciences. 2021; 11(10):1305. https://doi.org/10.3390/brainsci11101305
Chicago/Turabian StyleCloosterman, Sonja, Inez Wijnands, Simone Huygens, Valérie Wester, Ka-Hoo Lam, Eva Strijbis, Bram den Teuling, and Matthijs Versteegh. 2021. "The Potential Impact of Digital Biomarkers in Multiple Sclerosis in The Netherlands: An Early Health Technology Assessment of MS Sherpa" Brain Sciences 11, no. 10: 1305. https://doi.org/10.3390/brainsci11101305