
Treatment for Anomia in Bilingual Speakers with Progressive Aphasia

 , ,
, ,
Abstract
:1. Introduction
1.1. Progressive Anomia
1.2. Treatment for Progressive Anomia in Primary Progressive Aphasia
1.3. Cross-Linguistic Transfer in Treatment for Anomia in Bilingual Aphasia and the Role of Cognates
1.4. The Present Study
2. Materials and Methods
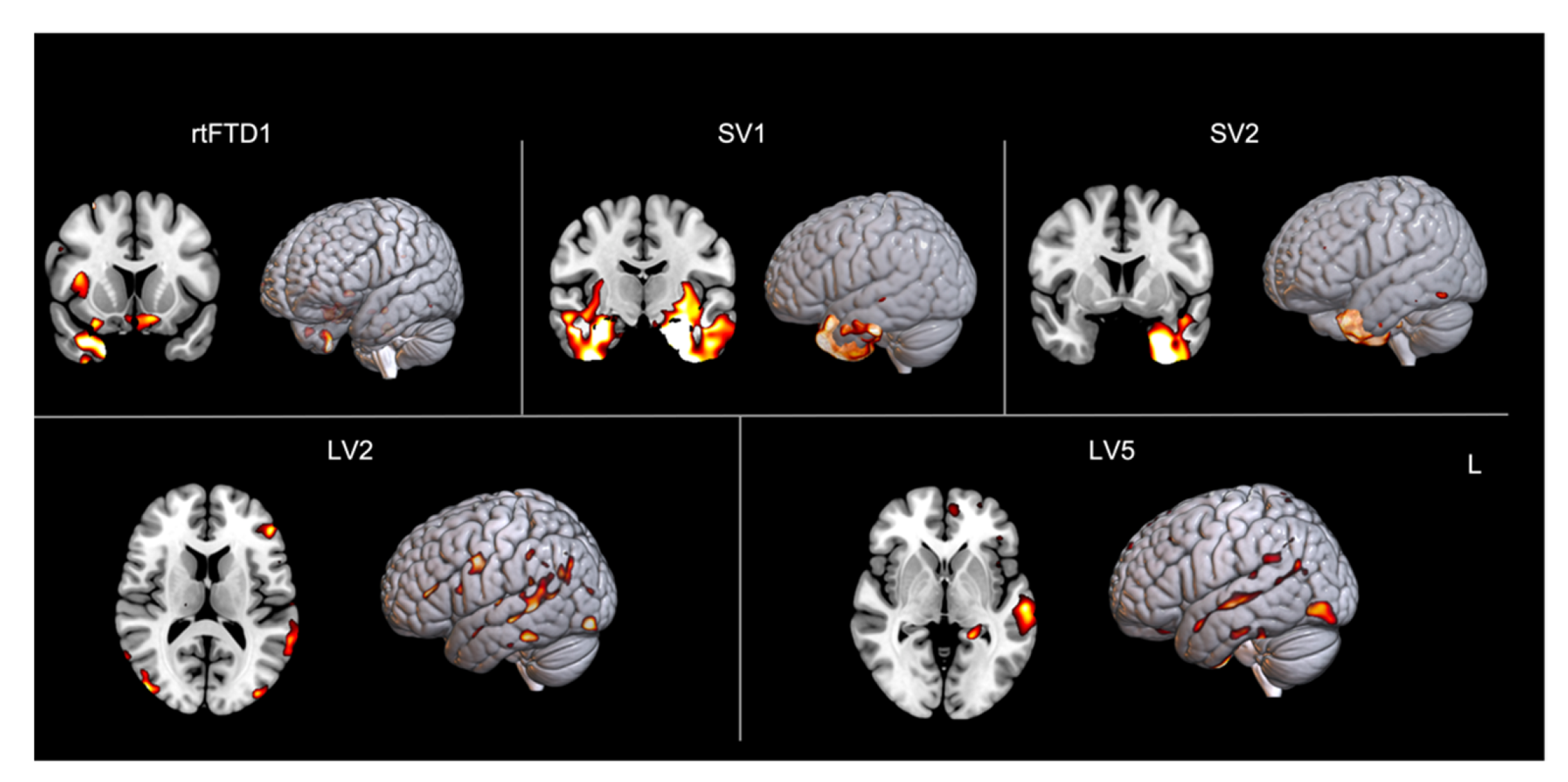
2.1. Participants
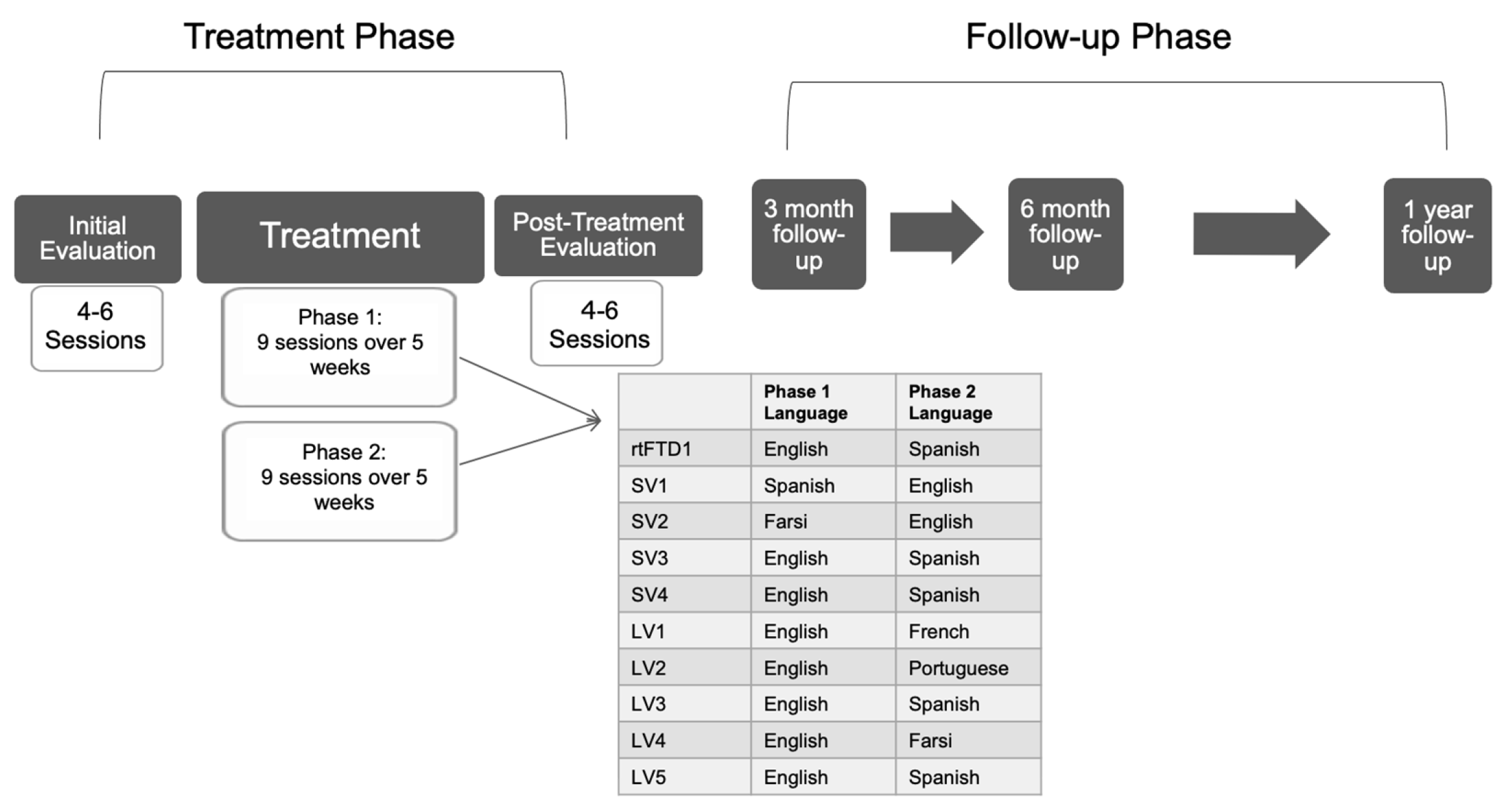
2.2. Treatment Design and Procedures
2.3. Treatment Fidelity
2.4. Self- and Communication Partner-Assessment of Change Following Treatment
2.5. Follow-Up Assessment
2.6. Outcome Measures and Statistical Analysis
3. Results
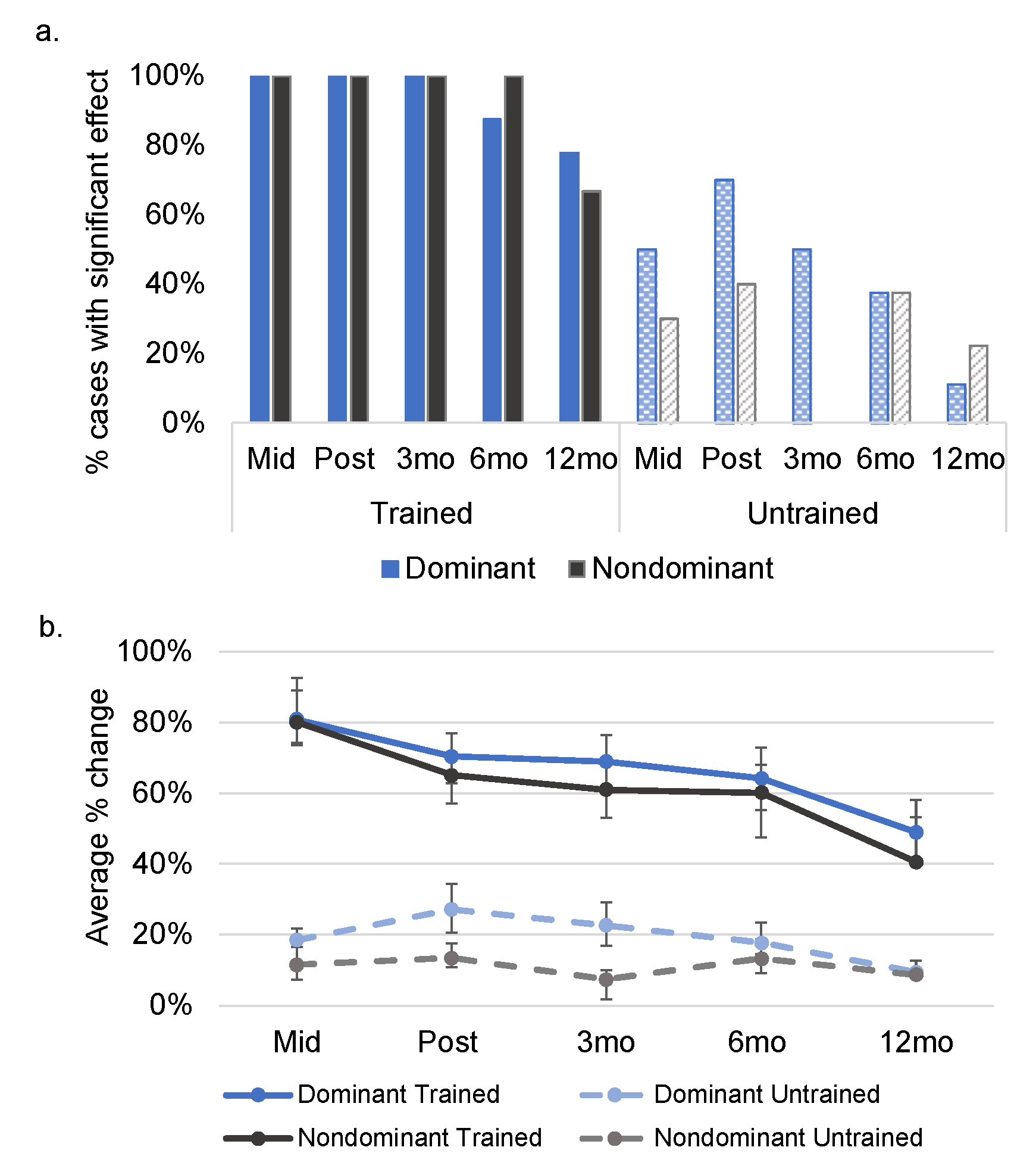
3.1. Treatment and Maintenance Effects
3.2. Within-Language Generalization to Untrained Items
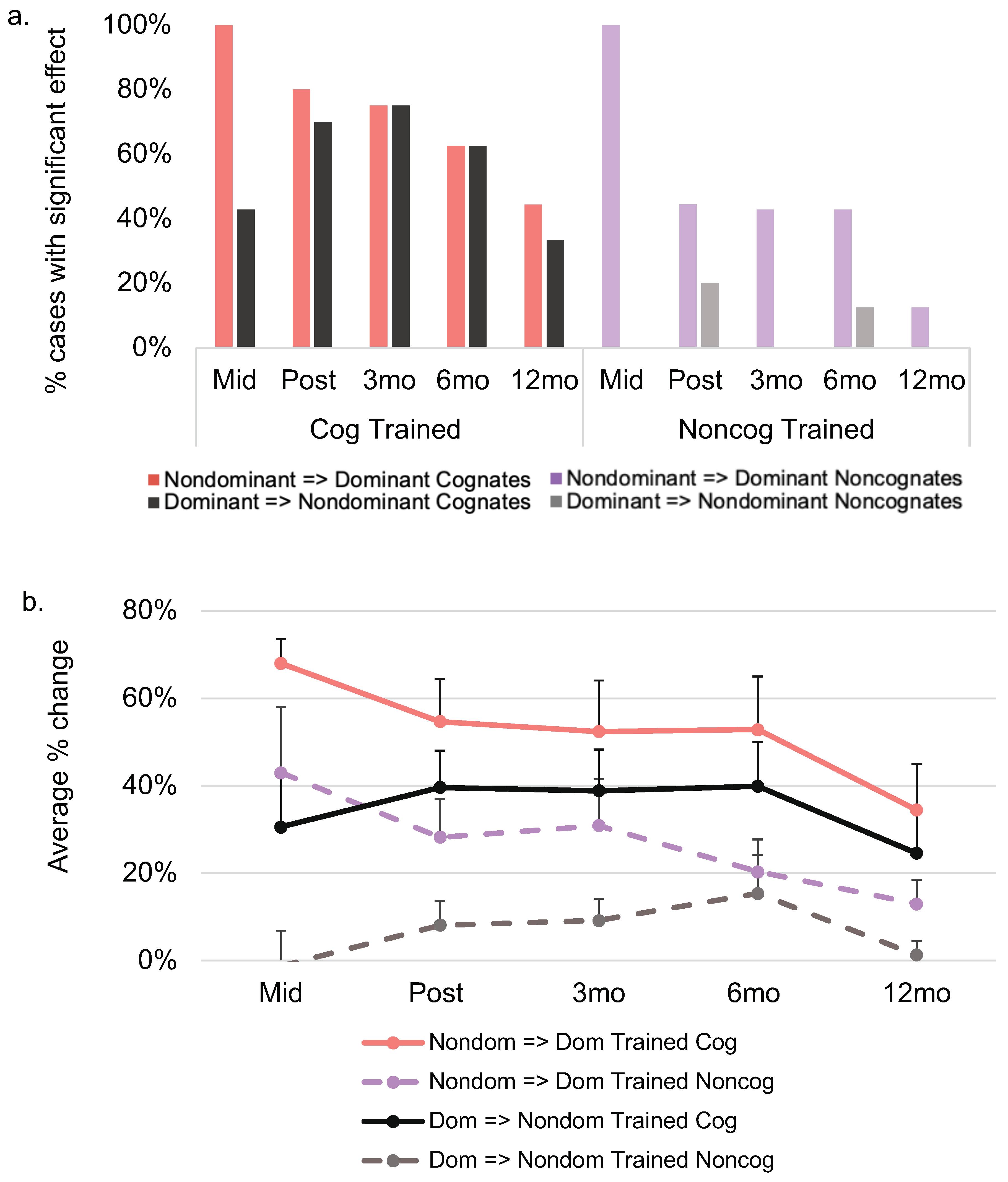
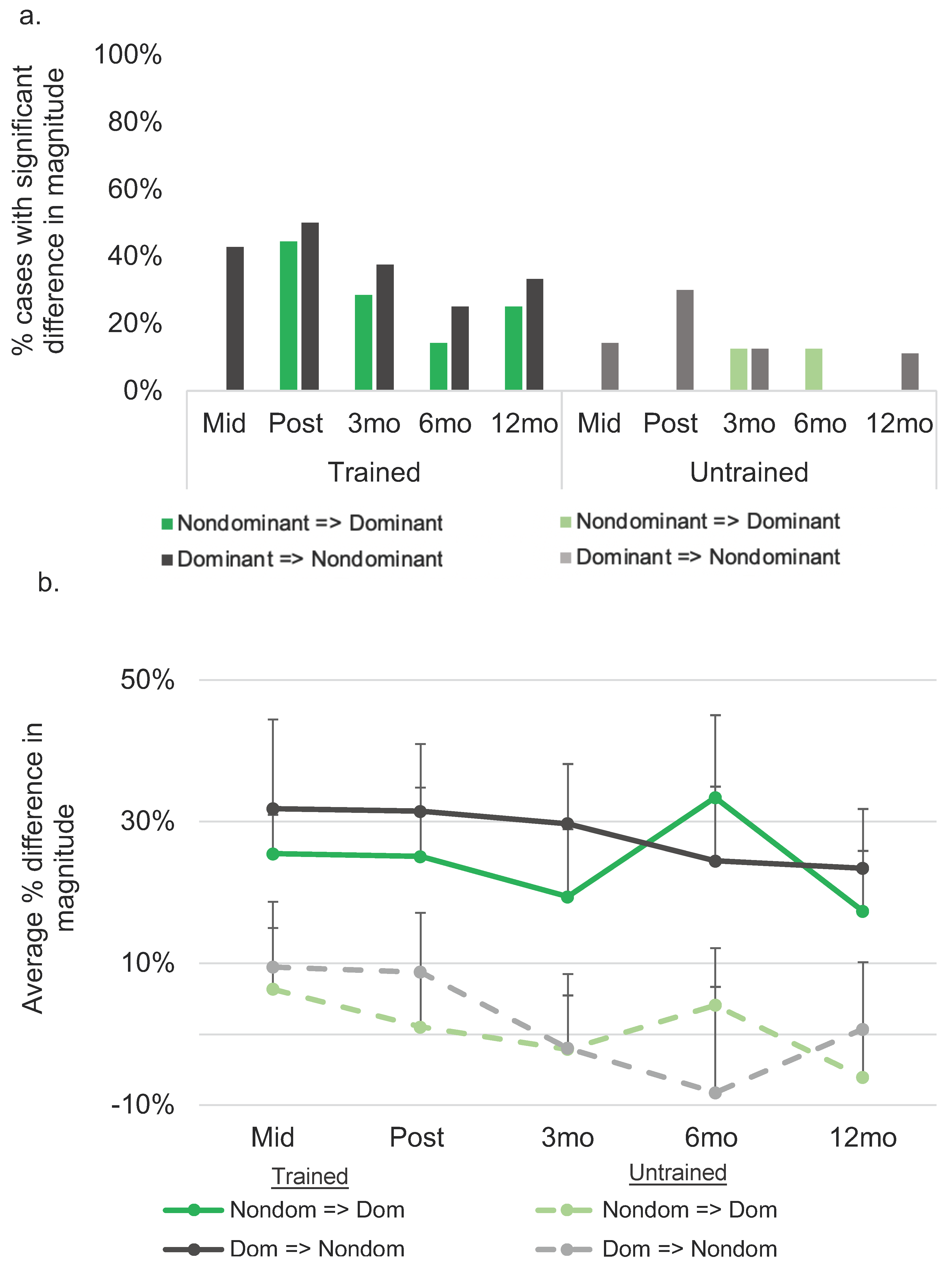
3.3. Cross-Linguistic Translation Effects
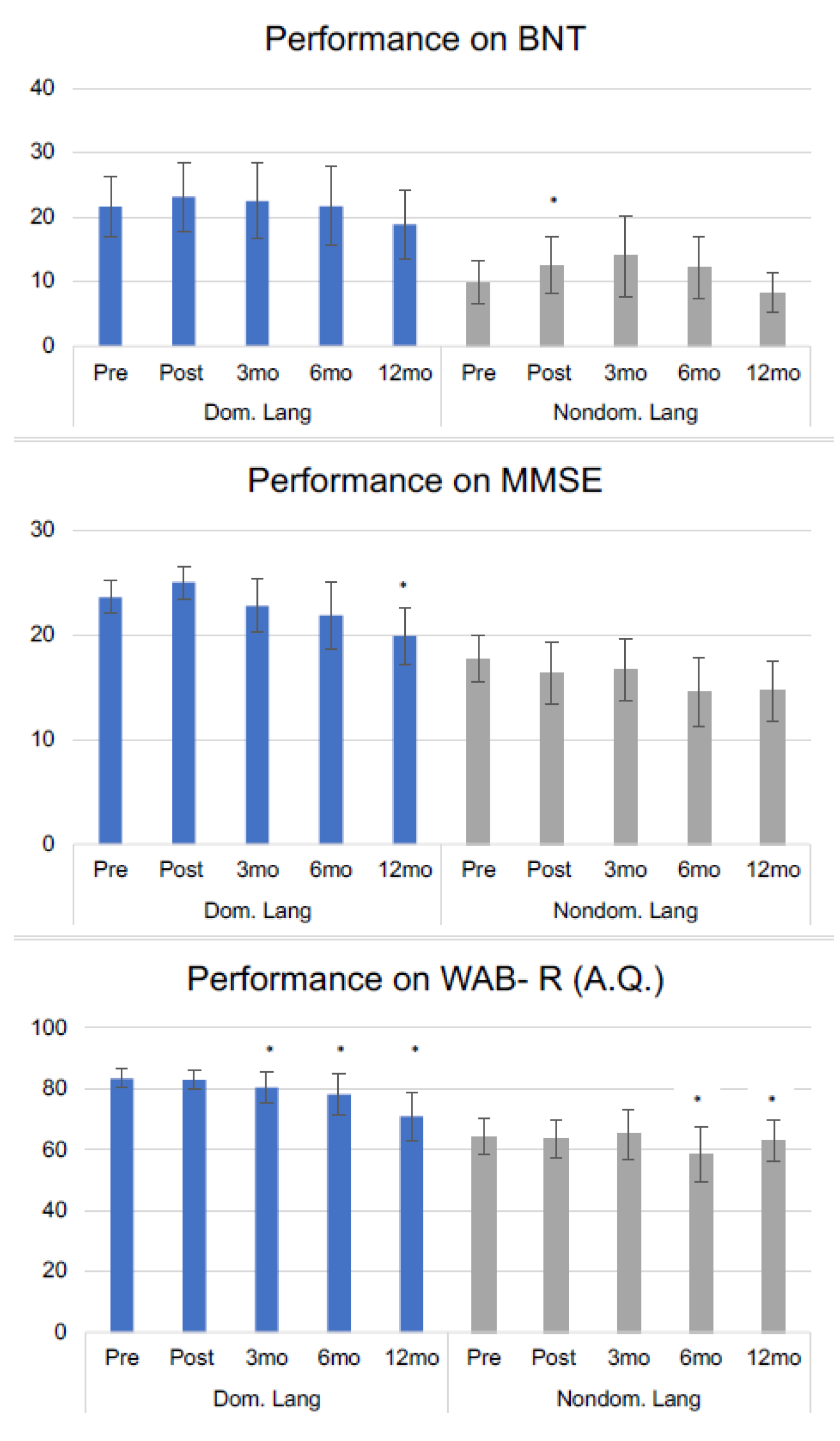
3.4. Performance on Additional Outcome Measures
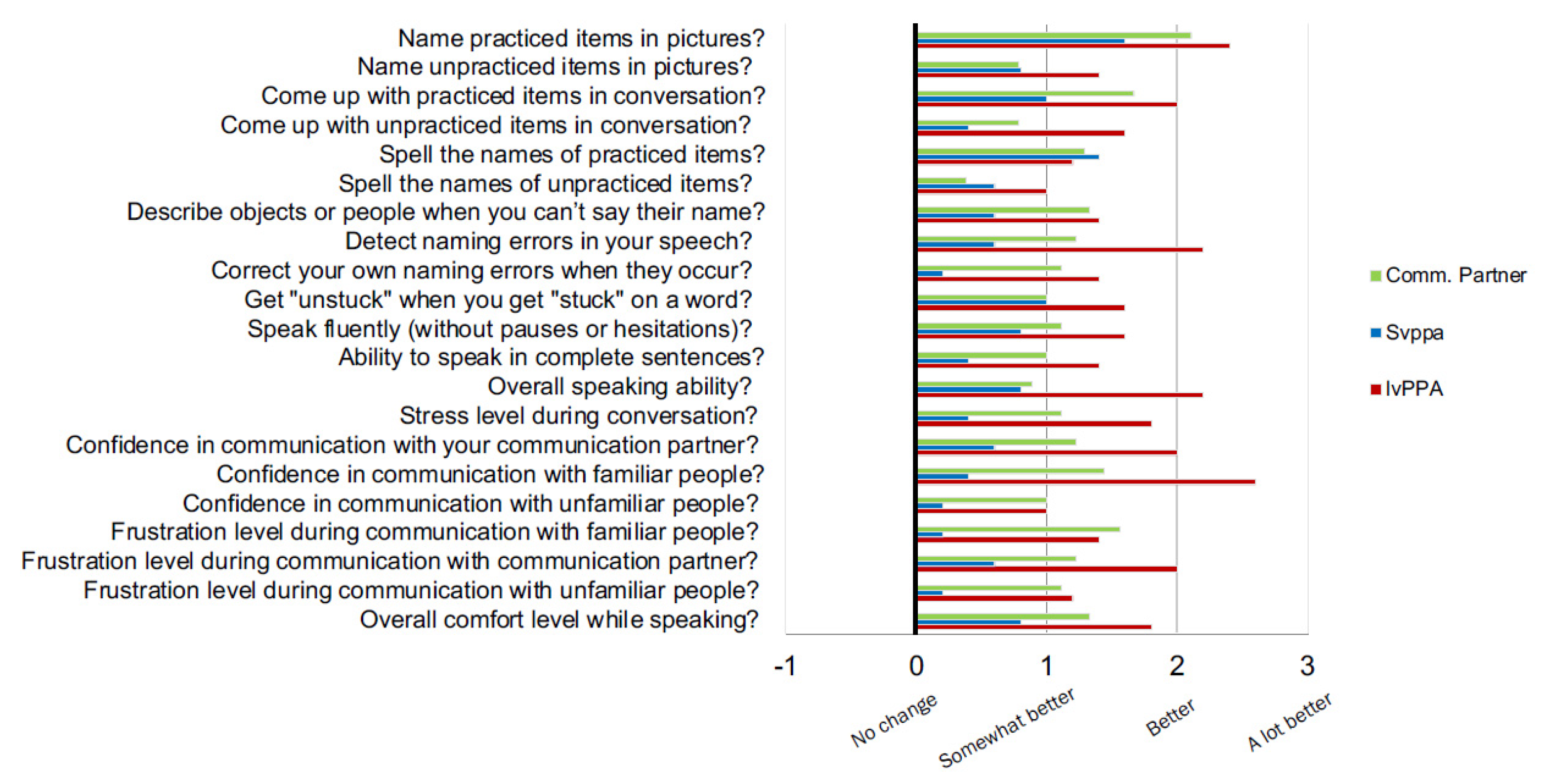
3.5. Self and Communication Partner Assessment of Change
4. Discussion
4.1. Within-Language Gains and Generalization Effects
4.2. Maintenance of Treatment Gains
4.3. Cross-Linguistic Translation Effects
4.4. Treatment and Translation Effects by PPA Variant
4.5. Additional Considerations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B

References
- Grosjean, F. Bilingual: Life and Reality; Harvard University Press: Cambridge, MA, USA, 2010. [Google Scholar] [CrossRef]
- Marian, V.; Shook, A. The Cognitive Benefits of Being Bilingual. Cerebrum Dana Forum Brain Sci. 2012, 2012, 13. [Google Scholar]
- Faroqi-Shah, Y.; Frymark, T.; Mullen, R.; Wang, B. Effect of treatment for bilingual individuals with aphasia: A systematic review of the evidence. J. Neurolinguist. 2010, 23, 319–341. [Google Scholar] [CrossRef]
- Kohnert, K. Cross-Language Generalization following Treatment in Bilingual Speakers with Aphasia: A Review. Semin. Speech Lang. 2009, 30, 174–186. [Google Scholar] [CrossRef]
- Ansaldo, A.I.; Saidi, L.G. Aphasia Therapy in the Age of Globalization: Cross-Linguistic Therapy Effects in Bilingual Aphasia. Behav. Neurol. 2014, 2014, 603085. [Google Scholar] [CrossRef] [PubMed]
- Sandberg, C.W.; Zacharewicz, M.; Gray, T. Bilingual Abstract Semantic Associative Network Training (BAbSANT): A Polish-English case study. J. Commun. Disord. 2021, 93, 106143. [Google Scholar] [CrossRef]
- Peñaloza, C.; Scimeca, M.; Gaona, A.; Carpenter, E.; Mukadam, N.; Gray, T.; Shamapant, S.; Kiran, S. Telerehabilitation for Word Retrieval Deficits in Bilinguals With Aphasia: Effectiveness and Reliability as Compared to In-person Language Therapy. Front. Neurol. 2021, 12, 598. [Google Scholar] [CrossRef]
- Aziz, M.A.A.; Razak, R.A.; Garraffa, M. Targeting Complex Orthography in the Treatment of a Bilingual Aphasia with Acquired Dysgraphia: The Case of a Malay/English Speaker with Conduction Aphasia. Behav. Sci. 2020, 10, 109. [Google Scholar] [CrossRef]
- Costa, A.S.; Jokel, R.; Villarejo, A.; Llamas-Velasco, S.; Domoto-Reilley, K.; Wojtala, J.; Reetz, K.; Machado, Á. Bilingualism in Primary Progressive Aphasia. Alzheimer Dis. Assoc. Disord. 2019, 33, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Meyer, A.M.; Snider, S.F.; Eckmann, C.B.; Friedman, R.B. Prophylactic treatments for anomia in the logopenic variant of primary progressive aphasia: Cross-language transfer. Aphasiology 2015, 29, 1062–1081. [Google Scholar] [CrossRef] [Green Version]
- Rumbaut, R.G.; Massey, D.S. Immigration & Language Diversity in the United States. Daedalus 2013, 142, 141–154. [Google Scholar] [CrossRef]
- Santhanam, S.P.; Parveen, S. Serving Culturally and Linguistically Diverse Clients: A Review of Changing Trends in Speech-Language Pathologists’ Self-efficacy and Implications for Stakeholders. Clin. Arch. Commun. Disord. 2018, 3, 165–177. [Google Scholar] [CrossRef] [Green Version]
- ASHA. Demographic Profile of ASHA Members Providing Bilingual Services. 2020. Available online: https://www.asha.org/siteassets/surveys/demographic-profile-bilingual-spanish-service-members.pdf (accessed on 15 October 2021).
- Henry, M.; Rising, K.; DeMarco, A.; Miller, B.; Gorno-Tempini, M.; Beeson, P. Examining the value of lexical retrieval treatment in primary progressive aphasia: Two positive cases. Brain Lang. 2013, 127, 145–156. [Google Scholar] [CrossRef] [Green Version]
- Henry, M.L.; Hubbard, H.I.; Grasso, S.M.; Dial, H.R.; Beeson, P.M.; Miller, B.L.; Gorno-Tempini, M.L. Treatment for Word Retrieval in Semantic and Logopenic Variants of Primary Progressive Aphasia: Immediate and Long-Term Outcomes. J. Speech Lang. Hear. Res. 2019, 62, 2723–2749. [Google Scholar] [CrossRef]
- Beeson, P.M.; King, R.M.; Bonakdarpour, B.; Henry, M.L.; Cho, H.; Rapcsak, S.Z. Positive Effects of Language Treatment for the Logopenic Variant of Primary Progressive Aphasia. J. Mol. Neurosci. 2011, 45, 724–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mesulam, M.-M. Slowly progressive aphasia without generalized dementia. Ann. Neurol. 1982, 11, 592–598. [Google Scholar] [CrossRef]
- Gorno-Tempini, M.L.; Hillis, A.E.; Weintraub, S.; Kertesz, A.; Mendez, M.; Cappa, S.F.; Ogar, J.M.; Rohrer, J.D.; Black, S.; Boeve, B.F.; et al. Classification of primary progressive aphasia and its variants. Neurology 2011, 76, 1006–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montembeault, M.; Brambati, S.M.; Gorno-Tempini, M.L.; Migliaccio, R. Clinical, Anatomical, and Pathological Features in the Three Variants of Primary Progressive Aphasia: A Review. Front. Neurol. 2018, 9, 692. [Google Scholar] [CrossRef] [Green Version]
- Henry, M.L.; Gorno-Tempini, M.L. The logopenic variant of primary progressive aphasia. Curr. Opin. Neurol. 2010, 23, 633–637. [Google Scholar] [CrossRef]
- Rohrer, J.; Rossor, M.; Warren, J.D. Alzheimer’s pathology in primary progressive aphasia. Neurobiol. Aging 2012, 33, 744–752. [Google Scholar] [CrossRef] [Green Version]
- Spinelli, E.G.; Mandelli, M.L.; Miller, Z.A.; Santos-Santos, M.A.; Wilson, S.M.; Agosta, F.; Grinberg, L.T.; Huang, E.J.; Trojanowski, J.Q.; Meyer, M.; et al. Typical and atypical pathology in primary progressive aphasia variants. Ann. Neurol. 2017, 81, 430–443. [Google Scholar] [CrossRef]
- Hodges, J.R.; Patterson, K. Semantic dementia: A unique clinicopathological syndrome. Lancet Neurol. 2007, 6, 1004–1014. [Google Scholar] [CrossRef]
- Iaccarino, L.; Crespi, C.; Della Rosa, P.A.; Catricalà, E.; Guidi, L.; Marcone, A.; Tagliavini, F.; Magnani, G.; Cappa, S.; Perani, D. The Semantic Variant of Primary Progressive Aphasia: Clinical and Neuroimaging Evidence in Single Subjects. PLoS ONE 2015, 10, e0120197. [Google Scholar] [CrossRef] [Green Version]
- Binney, R.J.; Henry, M.; Babiak, M.; Pressman, P.S.; Santos-Santos, M.A.; Narvid, J.; Mandelli, M.L.; Strain, P.J.; Miller, B.L.; Rankin, K.P.; et al. Reading words and other people: A comparison of exception word, familiar face and affect processing in the left and right temporal variants of primary progressive aphasia. Cortex 2016, 82, 147–163. [Google Scholar] [CrossRef] [Green Version]
- Josephs, K.A.; Whitwell, J.L.; Knopman, D.S.; Boeve, B.F.; Vemuri, P.; Senjem, M.L.; Parisi, J.E.; Ivnik, R.J.; Dickson, D.W.; Petersen, R.C.; et al. Two distinct subtypes of right temporal variant frontotemporal dementia. Neurology 2009, 73, 1443–1450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, D.; Anderson, V.; Pijnenburg, Y.; Whitwell, J.; Barnes, J.; Scahill, R.; Stevens, J.M.; Barkhof, F.; Scheltens, P.; Rossor, M.; et al. The clinical profile of right temporal lobe atrophy. Brain 2009, 132, 1287–1298. [Google Scholar] [CrossRef] [PubMed]
- Henry, M.L.; Wilson, S.M.; Ogar, J.M.; Sidhu, M.S.; Rankin, K.P.; Cattaruzza, T.; Miller, B.L.; Gorno-Tempini, M.L.; Seeley, W.W. Neuropsychological, behavioral, and anatomical evolution in right temporal variant frontotemporal dementia: A longitudinal and post-mortem single case analysis. Neurocase 2014, 20, 100–109. [Google Scholar] [CrossRef]
- Carthery-Goulart, M.T.; Silveira, A.D.C.D.; Machado, T.H.; Mansur, L.L.; Parente, M.A.D.M.P.; Senaha, M.L.H.; Brucki, S.; Nitrini, R. Nonpharmacological interventions for cognitive impairments following primary progressive aphasia: A systematic review of the literature. Dement. Neuropsychol. 2013, 7, 122–131. [Google Scholar] [CrossRef] [Green Version]
- Croot, K.; Nickels, L.; Laurence, F.; Manning, M. Impairment- and activity/participation-directed interventions in progressive language impairment: Clinical and theoretical issues. Aphasiology 2009, 23, 125–160. [Google Scholar] [CrossRef]
- Jokel, R.; Graham, N.L.; Rochon, E.; Leonard, C. Word retrieval therapies in primary progressive aphasia. Aphasiology 2014, 28, 1038–1068. [Google Scholar] [CrossRef]
- Rising, K. Treatment for Lexical Retrieval in Primary Progressive Aphasia Lexical Retrieval Treatments in PPA. Perspect. Neurophysiol. Neurogenic Speech Lang. Disord. 2016, 24, 137–144. [Google Scholar] [CrossRef]
- Tippett, D.C.; Hillis, A.E.; Tsapkini, K. Treatment of Primary Progressive Aphasia. Curr. Treat. Options Neurol. 2015, 17, 1–11. [Google Scholar] [CrossRef]
- Croot, K. Treatment for Lexical Retrieval Impairments in Primary Progressive Aphasia: A Research Update with Implications for Clinical Practice. Semin. Speech Lang. 2018, 39, 242–256. [Google Scholar] [CrossRef]
- Cadório, I.; Lousada, M.; Martins, P.; Figueiredo, D. Generalization and maintenance of treatment gains in primary progressive aphasia (PPA): A systematic review. Int. J. Lang. Commun. Disord. 2017, 52, 543–560. [Google Scholar] [CrossRef] [PubMed]
- Cotelli, M.; Manenti, R.; Ferrari, C.; Gobbi, E.; Macis, A.; Cappa, S.F. Effectiveness of language training and non-invasive brain stimulation on oral and written naming performance in Primary Progressive Aphasia: A meta-analysis and systematic review. Neurosci. Biobehav. Rev. 2020, 108, 498–525. [Google Scholar] [CrossRef]
- Graham, K.S.; Patterson, K.; Pratt, K.H.; Hodges, J.R. Relearning and Subsequent Forgetting of Semantic Category Exemplars in a Case of Semantic Dementia. Neuropsychology 1999, 13, 359–380. [Google Scholar] [CrossRef]
- Heredia, C.G.; Sage, K.; Ralph, M.A.L.; Berthier, M.L. Relearning and retention of verbal labels in a case of semantic dementia. Aphasiology 2009, 23, 192–209. [Google Scholar] [CrossRef]
- Mayberry, E.; Sage, K.; Ehsan, S.; Ralph, M.A.L. Relearning in semantic dementia reflects contributions from both medial temporal lobe episodic and degraded neocortical semantic systems: Evidence in support of the complementary learning systems theory. Neuropsychologia 2011, 49, 3591–3598. [Google Scholar] [CrossRef]
- Jokel, R.; Rochon, E.; Anderson, N. Errorless learning of computer-generated words in a patient with semantic dementia. Neuropsychol. Rehabil. 2010, 20, 16–41. [Google Scholar] [CrossRef]
- Savage, S.; Ballard, K.; Piguet, O.; Hodges, J.R. Bringing words back to mind—Improving word production in semantic dementia. Cortex 2013, 49, 1823–1832. [Google Scholar] [CrossRef]
- Savage, S.A.; Piguet, O.; Hodges, J.R. Cognitive Intervention in Semantic Dementia Maintaining Words over Time. Alzheimer Dis. Assoc. Disord. 2015, 29, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Snowden, J.S.; Neary, D. Relearning of verbal labels in semantic dementia. Neuropsychologia 2002, 40, 1715–1728. [Google Scholar] [CrossRef]
- Suarez-Gonzalez, A.; Heredia, C.G.; Savage, S.A.; Gil-Néciga, E.; García-Casares, N.; Franco-Macías, E.; Berthier, M.L.; Caine, D. Restoration of conceptual knowledge in a case of semantic dementia. Neurocase 2014, 21, 309–321. [Google Scholar] [CrossRef] [PubMed]
- Suárez-González, A.; A Savage, S.; Caine, D. Successful short-term re-learning and generalisation of concepts in semantic dementia. Neuropsychol. Rehabil. 2016, 28, 1095–1109. [Google Scholar] [CrossRef] [Green Version]
- Meyer, A.M.; Tippett, D.C.; Friedman, R.B. Prophylaxis and remediation of anomia in the semantic and logopenic variants of primary progressive aphasia. Neuropsychol. Rehabil. 2016, 28, 352–368. [Google Scholar] [CrossRef]
- Croot, K.; Raiser, T.; Taylor-Rubin, C.; Ruggero, L.; Ackl, N.; Wlasich, E.; Danek, A.; Scharfenberg, A.; Foxe, D.; Hodges, J.R.; et al. Lexical retrieval treatment in primary progressive aphasia: An investigation of treatment duration in a heterogeneous case series. Cortex 2019, 115, 133–158. [Google Scholar] [CrossRef]
- Lavoie, M.; Bier, N.; Laforce, R., Jr.; Macoir, J. Improvement in functional vocabulary and generalization to conversation following a self-administered treatment using a smart tablet in primary progressive aphasia. Neuropsychol. Rehabil. 2020, 30, 1224–1254. [Google Scholar] [CrossRef]
- Krajenbrink, T.; Croot, K.; Taylor-Rubin, C.; Nickels, L. Treatment for spoken and written word retrieval in the semantic variant of primary progressive aphasia. Neuropsychol. Rehabil. 2018, 30, 915–947. [Google Scholar] [CrossRef] [PubMed]
- Dressel, K.; Huber, W.; Frings, L.; Kümmerer, D.; Saur, D.; Mader, I.; Hüll, M.; Weiller, C.; Abel, S. Model-oriented naming therapy in semantic dementia: A single-case fMRI study. Aphasiology 2010, 24, 1537–1558. [Google Scholar] [CrossRef]
- Jokel, R.; Anderson, N. Quest for the best: Effects of errorless and active encoding on word re-learning in semantic dementia. Neuropsychol. Rehabil. 2012, 22, 187–214. [Google Scholar] [CrossRef] [PubMed]
- Newhart, M.; Davis, C.; Kannan, V.; Heidler-Gary, J.; Cloutman, L.; Hillis, A.E. Therapy for naming deficits in two variants of primary progressive aphasia. Aphasiology 2009, 23, 823–834. [Google Scholar] [CrossRef]
- Grasso, S.M.; Shuster, K.M.; Henry, M.L. Comparing the effects of clinician and caregiver-administered lexical retrieval training for progressive anomia. Neuropsychol. Rehabil. 2017, 29, 866–895. [Google Scholar] [CrossRef] [PubMed]
- Meyer, A.M.; Tippett, D.C.; Turner, R.S.; Friedman, R.B. Long-Term maintenance of anomia treatment effects in primary progressive aphasia. Neuropsychol. Rehabil. 2019, 29, 1439–1463. [Google Scholar] [CrossRef] [PubMed]
- Beales, A.; Cartwright, J.; Whitworth, A.; Panegyres, P.K. Exploring generalisation processes following lexical retrieval intervention in primary progressive aphasia. Int. J. Speech-Lang. Pathol. 2016, 18, 299–314. [Google Scholar] [CrossRef] [PubMed]
- Kroll, J.; Stewart, E. Category Interference in Translation and Picture Naming: Evidence for Asymmetric Connections between Bilingual Memory Representations. J. Mem. Lang. 1994, 33, 149–174. [Google Scholar] [CrossRef]
- Kroll, J.F.; Michael, E.; Tokowicz, N.; Dufour, R. The development of lexical fluency in a second language. Second. Lang. Res. 2002, 18, 137–171. [Google Scholar] [CrossRef]
- Kroll, J.F.; Van Hell, J.G.; Tokowicz, N.; Green, D.W. The Revised Hierarchical Model: A critical review and assessment. Biling. Lang. Cogn. 2010, 13, 373–381. [Google Scholar] [CrossRef] [Green Version]
- van Hell, J.G.; de Groot, A.M. Sentence context modulates visual word recognition and translation in bilinguals. Acta Psychol. 2008, 128, 431–451. [Google Scholar] [CrossRef] [PubMed]
- Christoffels, I.; De Groot, A.; Kroll, J. Memory and language skills in simultaneous interpreters: The role of expertise and language proficiency. J. Mem. Lang. 2006, 54, 324–345. [Google Scholar] [CrossRef]
- De Groot, A.M.B. Determinants of word translation. J. Exp. Psychol. Learn. Mem. Cogn. 1992, 18, 1001–1018. [Google Scholar] [CrossRef]
- DeGroot, A.; Dannenburg, L.; Vanhell, J. Forward and Backward Word Translation by Bilinguals. J. Mem. Lang. 1994, 33, 600–629. [Google Scholar] [CrossRef]
- de Groot, A.M.B.; Nas, G.L.J. Lexical Representation of Cognates and Noncognates Compound Bilinguals. J. Mem. Lang. 1991, 123, 90–123. [Google Scholar] [CrossRef]
- Costa, A.; Caramazza, A.; Sebastian-Galles, N. The Cognate Facilitation Effect: Implications for Models of Lexical Access. J. Exp. Psychology Learn. Mem. Cogn. 2000, 26, 1283–1296. [Google Scholar] [CrossRef]
- Costa, A.; Santesteban, M.; Caño, A. On the facilitatory effects of cognate words in bilingual speech production. Brain Lang. 2005, 94, 94–103. [Google Scholar] [CrossRef]
- Sáchez-Casas, R.M.; García-Albea, J.E.; Davis, C.W. Bilingual lexical processing: Exploring the cognate/non-cognate distinction. Eur. J. Cogn. Psychol. 1992, 4, 293–310. [Google Scholar] [CrossRef]
- Rosselli, M.; Ardila, A.; Jurado, M.B.; Salvatierra, J.L. Cognate facilitation effect in balanced and non-balanced Spanish–English bilinguals using the Boston Naming Test. Int. J. Biling. 2014, 18, 649–662. [Google Scholar] [CrossRef]
- Murray, L.L. Bilingual aphasia treatment: Clinical recommendations regarding secondary language treatment, cross-language transfer, and the use of language brokers await additional research. Evid.-Based Commun. Assess. Interv. 2014, 9, 1–6. [Google Scholar] [CrossRef]
- Hameau, S.; Köpke, B. Cross-Language Transfer for Cognates in Aphasia Therapy with Multilingual Patients: A Case Study. Aphasie Verwandte Geb. 2015, 3, 13–19. [Google Scholar]
- Marangolo, P.; Rizzi, C.; Peran, P.; Piras, F.; Sabatini, U. Parallel recovery in a bilingual aphasic: A neurolinguistic and fMRI study. Neuropsychology 2009, 23, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Miertsch, B.; Meisel, J.M.; Isel, F. Non-treated languages in aphasia therapy of polyglots benefit from improvement in the treated language. J. Neurolinguist. 2009, 22, 135–150. [Google Scholar] [CrossRef]
- Kiran, S.; Sandberg, C.; Gray, T.; Ascenso, E.; Kester, E. Rehabilitation in Bilingual Aphasia: Evidence for Within- and Between-Language Generalization. Am. J. Speech-Lang. Pathol. 2013, 22, S298–S309. [Google Scholar] [CrossRef]
- Kiran, S.; Iakupova, R. Understanding the relationship between language proficiency, language impairment and rehabilitation: Evidence from a case study. Clin. Linguist. Phon. 2011, 25, 565–583. [Google Scholar] [CrossRef]
- Ansaldo, A.I.; Saidi, L.G.; Ruiz, A. Model-driven intervention in bilingual aphasia: Evidence from a case of pathological language mixing. Aphasiology 2009, 24, 309–324. [Google Scholar] [CrossRef]
- Edmonds, L.A.; Kiran, S. Effect of Semantic Naming Treatment on Crosslinguistic Generalization in Bilingual Aphasia. J. Speech Lang. Hear. Res. 2006, 49, 729–748. [Google Scholar] [CrossRef]
- Junqué, C.; Vendrell, P.; Vendrell-Brucet, J.M.; Tobena, A. Differential recovery in naming in bilingual aphasics. Brain Lang. 1989, 36, 16–22. [Google Scholar] [CrossRef]
- Kiran, S.; Roberts, P.M. Semantic feature analysis treatment in Spanish–English and French–English bilingual aphasia. Aphasiology 2009, 24, 231–261. [Google Scholar] [CrossRef]
- Kohnert, K. Cognitive and cognate-based treatments for bilingual aphasia: A case study. Brain Lang. 2004, 91, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Goral, M.; Rosas, J.; Conner, P.S.; Maul, K.K.; Obler, L.K. Effects of language proficiency and language of the environment on aphasia therapy in a multilingual. J. Neurolinguist. 2012, 25, 538–551. [Google Scholar] [CrossRef] [Green Version]
- Meinzer, M.; Obleser, J.; Flaisch, T.; Eulitz, C.; Rockstroh, B. Recovery from aphasia as a function of language therapy in an early bilingual patient demonstrated by fMRI. Neuropsychologia 2007, 45, 1247–1256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurland, J.; Falcon, M. Effects of cognate status and language of therapy during intensive semantic naming treatment in a case of severe nonfluent bilingual aphasia. Clin. Linguist. Phon. 2011, 25, 584–600. [Google Scholar] [CrossRef]
- Bedore, L.M.; Peña, E.D.; García, M.; Cortez, C. Scoring: When Does It Make a Difference? Lang. Speech Hear. Serv. Sch. 2005, 36, 188–201. [Google Scholar] [CrossRef] [Green Version]
- Kohnert, K.J.; Hernandez, A.E.; Bates, E. Bilingual Performance on the Boston Naming Test: Preliminary Norms in Spanish and English. Brain Lang. 1998, 65, 422–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Umbel, V.M.; Pearson, B.Z.; Fernandez, M.C.; Oller, D.K. Measuring Bilingual Children’s Receptive Vocabularies. Child Dev. 1992, 63, 1012–1020. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Dial, H.R.; A Hinshelwood, H.; Grasso, S.M.; Hubbard, H.I.; Gorno-Tempini, M.-L.; Henry, M. Investigating the utility of teletherapy in individuals with primary progressive aphasia. Clin. Interv. Aging 2019, 14, 453–471. [Google Scholar] [CrossRef] [Green Version]
- Kiran, S.; Peña, E.; Bedore, L.; Sheng, L. Evaluating the Relationship between Category Generation and Language Use and Proficiency. Presented at the Donostia Workshop on Neurobilingualism, San Sebastian, Spain, 30 September–2 October 2010. [Google Scholar]
- Beeson, P.M.; Egnor, H. Combining treatment for written and spoken naming. J. Int. Neuropsychol. Soc. 2006, 12, 816–827. [Google Scholar] [CrossRef] [PubMed]
- Coltheart, M. The MRC Psycholinguistic Database. Q. J. Exp. Psychol. Sect. A 1981, 33, 497–505. [Google Scholar] [CrossRef]
- Davies, M. The Corpus of Contemporary American English as the first reliable monitor corpus of English. Lit. Linguist. Comput. 2010, 25, 447–464. [Google Scholar] [CrossRef]
- Marian, V.; Bartolotti, J.; Chabal, S.; Shook, A. CLEARPOND: Cross-Linguistic Easy-Access Resource for Phonological and Orthographic Neighborhood Densities. PLoS ONE 2012, 7, e43230. [Google Scholar] [CrossRef] [Green Version]
- Davies, M. Corpus Del Español: Two Billion Words, 21 Countries. 2006. Available online: http://www.corpusdelespanol.org/web-dial/ (accessed on 15 October 2021).
- Duchon, A.; Perea, M.; Sebastian-Galles, N.; Martí, M.A.; Carreiras, M. EsPal: One-stop shopping for Spanish word properties. Behav. Res. Methods 2013, 45, 1246–1258. [Google Scholar] [CrossRef] [Green Version]
- New, B.; Pallier, C.; Brysbaert, M.; Ferrand, L. Lexique 2: A new French lexical database. Behav. Res. Methods Instrum. Comput. 2004, 36, 516–524. [Google Scholar] [CrossRef] [Green Version]
- Davies, M. Corpus Do Português: One Billion Words, 4 Countries. Available online: http://www.corpusdoportugues.org/web-dial/ (accessed on 15 October 2021).
- Kilgarriff, A.; Baisa, V.; Bušta, J.; Jakubíček, M.; Kovář, V.; Michelfeit, J.; Rychlý, P.; Suchomel, V. The Sketch Engine: Ten years on. Lexicography 2014, 1, 7–36. [Google Scholar] [CrossRef] [Green Version]
- Rasooli, M.S.; Kouhestani, M.; Moloodi, A. Development of a Persian Syntactic Dependency Treebank. In Proceedings of the NAACL-HLT, Atlanta, GA, USA, 9–13 June 2013; pp. 306–314. [Google Scholar]
- Dial, H.; Martin, R. Evaluating the relationship between sublexical and lexical processing in speech perception: Evidence from aphasia. Neuropsychologia 2017, 96, 192–212. [Google Scholar] [CrossRef] [Green Version]
- Kertesz, A. Western Aphasia Battery—Revised; Pearson: San Antonio, TX, USA, 2012. [Google Scholar]
- Kaplan, E.; Goodglass, H.; Weintraub, S. Boston Naming Test; Pro-Ed: Austin, TX, USA, 2001. [Google Scholar]
- Paul, N.; Mehrhoff, J. Descriptive Analysis: Survey of Direct and Indirect Interventions for Persons with Dementia-Based Communication Disorders. Perspect. Neurophysiol. Neurogenic Speech Lang. Disord. 2015, 25, 125–141. [Google Scholar] [CrossRef]
- Francis, W.S. Cognitive integration of language and memory in bilinguals: Semantic representation. Psychol. Bull. 1999, 125, 193–222. [Google Scholar] [CrossRef] [Green Version]
- Francis, W.S. Shared core meanings and shared associations in bilingual semantic memory: Evidence from research on implicit memory. Int. J. Biling. 2018, 24, 464–477. [Google Scholar] [CrossRef]
- Hoshino, N.; Kroll, J.F. Cognate effects in picture naming: Does cross-language activation survive a change of script? Cognition 2008, 106, 501–511. [Google Scholar] [CrossRef]
- Mendez, M.F.; Perryman, K.M.; Pontón, M.O.; Cummings, J.L. Bilingualism and Dementia. J. Neuropsychiatry Clin. Neurosci. 1999, 11, 411–412. [Google Scholar] [CrossRef] [PubMed]
- Ivanova, I.; Salmon, D.P.; Gollan, T.H. Which Language Declines More? Longitudinal versus Cross-sectional Decline of Picture Naming in Bilinguals with Alzheimer’s Disease. J. Int. Neuropsychol. Soc. 2014, 20, 534–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henry, M.L.; Wilson, S.M.; Babiak, M.C.; Mandelli, M.L.; Beeson, P.M.; Miller, Z.A.; Gorno-Tempini, M.L. Phonological Processing in Primary Progressive Aphasia. J. Cogn. Neurosci. 2016, 28, 210–222. [Google Scholar] [CrossRef] [Green Version]
- Graham, K.S.; Patterson, K.; Pratt, K.H.; Hodges, J.R. Can repeated exposure to “forgotten” vocabulary help alleviate word-finding difficulties in semantic dementia? An illustrative case study. Neuropsychol. Rehabil. 2001, 11, 429–454. [Google Scholar] [CrossRef]
- Jokel, R.; Rochon, E.; Leonard, C. Treating anomia in semantic dementia: Improvement, maintenance, or both? Neuropsychol. Rehabil. 2006, 16, 241–256. [Google Scholar] [CrossRef] [PubMed]
- Lind, M.; Simonsen, H.G.; Ribu, I.S.B.; Svendsen, B.A.; Svennevig, J.; De Bot, K. Lexical access in a bilingual speaker with dementia: Changes over time. Clin. Linguist. Phon. 2017, 32, 353–377. [Google Scholar] [CrossRef]
- Ou, L.; Przybilla, M.; Koniar, B.; Whitley, C.B. RTB lectin-mediated delivery of lysosomal α-L-iduronidase mitigates disease manifestations systemically including the central nervous system. Mol. Genet. Metab. 2018, 123, 105–111. [Google Scholar] [CrossRef]
- Mahendra, N.; Spicer, J. Access to Speech-Language Pathology Services for African-American Clients with Aphasia: A Qualitative Study Racial and Ethnic Disparities in Stroke Care. Div. 14 Newsl. 2014, 21, 53–62. [Google Scholar]
- Prince, M.; Ali, G.-C.; Guerchet, M.; Prina, M.; Albanese, E.; Wu, Y.-T. Recent global trends in the prevalence and incidence of dementia, and survival with dementia. Alzheimer’s Res. Ther. 2016, 8, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Prince, M.; Acosta, D.; Albanese, E.; Arizaga, R.; Ferri, C.P.; Guerra, M.; Huang, Y.; Jacob, K.; Jiménez-Velázquez, I.Z.; Rodriguez, J.L.; et al. Ageing and dementia in low and middle income countries–Using research to engage with public and policy makers. Int. Rev. Psychiatry 2008, 20, 332–343. [Google Scholar] [CrossRef] [PubMed]
- Ortman, J.M.; Shin, H.B. Language Projections: 2010 to 2020. Presented at the Annual Meetings of the American Sociological Association, Las Vegas, NV, USA, 20–23 August 2011. [Google Scholar]
- Zeigler, K.; Camarota, S.A. 67.3 Million in the United States Spoke a Foreign Language at Home in 2018; Center for Immigration Studies: Washington, DC, USA, 2019. Available online: https://cis.org/Report/673-Million-United-States-Spoke-Foreign-Language-Home-2018 (accessed on 15 October 2021).
- Grandpierre, V.; Milloy, V.; Sikora, L.; Fitzpatrick, E.; Thomas, R.; Potter, B. Barriers and facilitators to cultural competence in rehabilitation services: A scoping review. BMC Health Serv. Res. 2018, 18, 1–14. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant | rtFTD1 | SV1 | SV2 | SV3 | SV4 | LV1 | LV2 | LV3 | LV4 | LV5 | ||||||||||
| Demographics | ||||||||||||||||||||
| Sex | M | M | M | F | F | F | M | F | M | M | ||||||||||
| Age (years) | 67 | 72 | 64 | 60 | 63 | 78 | 80 | 59 | 64 | 62 | ||||||||||
| Education (years) | 16 | 12 | 18 | 20 | 20 | 16 | 20 | 18 | 18 | 13 | ||||||||||
| Years Post Onset | 3 | 5 | 3 | 3 | 9 | 2 | 4 | 2 | 2.5 | 1.5 | ||||||||||
| Handedness | Right | Right | Right | Ambidextrous | Right | Right | Right | Right | Right | Right | ||||||||||
| Language History Variables | ||||||||||||||||||||
| Language | Span | Eng | Span | Eng | Farsi | Eng | Span | Eng | Span | Eng | French | Eng | Port | Eng | Span | Eng | Farsi | Eng | Span | Eng |
| Age of acquisition (years) | Birth | 6 | Birth | 5 | Birth | 18 | 11 | Birth | 9 | Birth | 17 | Birth | Birth | Birth | Birth | 16 | Birth | 14 | Birth | 17 |
| Premorbid proficiency (5-point scale; with 5 indicating native-like proficiency) | 3 | 5 | 4 | 5 | 4 | 5 | 3 | 5 | 5 | 5 | 5 | 5 | 4 | 5 | 5 | 5 | 5 | 4 | 5 | 5 |
| Premorbid daily usage (out of 100%) | 7% | 93% | 16% | 85% | 60% | 40% | 8% | 93% | 12% | 88% | 13% | 88% | 10% | 90% | 20% | 80% | 37% | 63% | 48% | 52% |
| Weekday | 13% | 87% | 18% | 82% | 38% | 62% | 15% | 85% | 12% | 88% | 13% | 88% | 13% | 87% | 20% | 80% | 53% | 47% | 46% | 54% |
| Weekend | 1% | 99% | 13% | 87% | 82% | 18% | 0% | 100% | 12% | 88% | 13% | 88% | 6% | 94% | 20% | 80% | 21% | 79% | 50% | 50% |
| Postmorbid proficiency (5-point scale; with 5 indicating native-like proficiency) | 3 | 5 | 3 | 5 | 4 | 5 | 2 | 4 | 2 | 3 | 5 | 5 | 2 | 4 | 2 | 2 | 5 | 4 | 3 | 4 |
| Postmorbid daily usage (out of 100%) | 5% | 94% | 7% | 93% | 60% | 40% | 8% | 93% | 97% | 3% | 13% | 88% | 6% | 94% | 10% | 90% | 80% | 20% | 85% | 15% |
| Weekday | 6% | 91% | 7% | 93% | 38% | 62% | 15% | 85% | 100% | 0% | 13% | 88% | 6% | 94% | 10% | 90% | 80% | 20% | 87% | 13% |
| Weekend | 3% | 97% | 7% | 93% | 82% | 18% | 0% | 100% | 94% | 6% | 13% | 88% | 6% | 94% | 10% | 90% | 80% | 20% | 83% | 17% |
| Self-reported dominance | English | English | Farsi | English | English | English | English | English | Farsi | Spanish | ||||||||||
| Dominance index (lower BNT score/ higher BNT score) | 0.39 | 0.15 | 0.50 | 0.33 | 0.82 | 0.50 | 0.14 | 0.22 | 0.47 | 0.97 | ||||||||||
| Participant ID | rtFTD1 | SV1 | SV2 | SV3 | SV4 | LV1 | LV2 | LV3 | LV4 | LV5 | ||||||||||
| Language | Span | Eng | Span | Eng | Farsi | Eng | Span | Eng | Span | Eng | Fre | Eng | Port | Eng | Spa | Eng | Farsi | Eng | Span | Eng |
| Mini-Mental State Examination 1 (30) | 23 | 22 | 15 | 25 | 30 | 27 | 17 | 23 | 14 | 17 | 23 | 26 | 6 | 29 | 9 | 14 | 29 | 27 | 26 | 27 |
| CVLT Total (36) 2 | 15 | 16 | 13 | 18 | - | 15 | 0 | 13 | - | 13 | - | 19 | - | 17 | - | 11 | - | 24 | 9 | 11 |
| CVLT 10-min Recall 2 | 1 | 3 | 0 | 0 | - | 0 | 0 | 0 | - | 1 | - | 5 | - | 2 | - | 3 | - | 3 | 0 | 0 |
| Stroop Color naming 2 | 26 | 38 | 12 | 45 | - | 38 | - | 35 | 11 | 48 | - | 42 | - | 52 | - | 7 | - | 69 | 38 | 38 |
| Stroop interference 2 | 14 | 24 | 7 | 30 | - | 12 | - | 21 | 9 | 31 | - | 31 | - | 20 | - | 4 | - | 49 | 23 | 22 |
| Complex Figure Copy (17) 2 | - | 14 | - | 14 | - | 15 | - | 17 | - | 17 | - | 13 | - | 15 | - | 7 | - | 16 | 16 | - |
| Complex Figure Recall (17) 2 | - | 6 | - | 3 | - | 13 | - | 15 | - | 11 | - | 10 | - | 6 | - | 4 | - | 17 | 5 | - |
| Calculations (5) 2 | - | 5 | - | 4 | - | 5 | - | - | - | - | - | 3 | - | - | - | 0 | - | 5 | - | - |
| Digit Span Forward 2 | 4 | 5 | 5 | 6 | - | 6 | 5 | 7 | 4 | 6 | - | 6 | - | 5 | - | 3 | - | 6 | 3 | 3 |
| Digit Span Backward 2 | 3 | 4 | 3 | 5 | - | 5 | 4 | 5 | 5 | 5 | - | 4 | - | 4 | - | 2 | - | 4 | 4 | 3 |
| PPVT Short (16) 2 | - | 14 | - | 10 | - | 8 | - | 1 | - | 4 | - | - | - | 12 | - | 9 | - | 8 | - | 13 |
| Western Aphasia Battery (AQ; 100) 3 | 78.2 | 92.6 | 69.2 | 87.5 | 90.2 | 81.3 | 42.9 | 75.9 | 51 | 74.4 | 77.3 | 88.7 | 38.4 | 86.8 | 39.3 | 61.3 | 92 | 82.1 | 84.4 | 82.8 |
| Motor Speech Eval: AOS (0–7) 4 | 0 | 0 | 0 | 0 | - | 0 | N/A | N/A | - | 0 | - | 0 | - | 0 | - | 0 | - | 0 | 0 | 0 |
| Motor Speech Eval: Dysarthria (0–7) 4 | 0 | 0 | 0 | 0 | - | 0 | N/A | N/A | - | 0 | - | 0 | - | 0 | - | 0 | - | 0 | 0 | 0 |
| Pyramids and Palm Trees Test 5 (short; 14 6; * = /25, ^ = /20 7) | - | 14 | - | 14 | 12 | 14 | - | 7 | 14 ^ | 14 * | - | 13 | - | 14 | - | 13 | - | 14 | - | 13 |
| Boston Naming Test (60; * = /18) 8 | 11 | 28 | 4 | 27 | 8 | 4 | 1 | 3 | 2 * | 2 | 17 | 34 | 4 | 29 | 2 | 9 | 43 | 20 | 33 | 34 |
| UCSF Syntax Comprehension Test (%) 9 | - | 97 | - | 100 | - | 97 | - | - | - | - | - | 97 | - | 100 | - | 75 | - | 92 | - | - |
| BAT Syntax Comprehension Subtest (%) 10 | 92 | 100 | 79 | 98 | 93 | 92 | 69 | 95 | 84 | 84 | 74 | 91 | 76 | 91 | 51 | 53 | 94 | 92 | 8 | 85 |
| Arizona Phonological Battery (%) 11 | - | 50 | - | 80 | - | 53 | - | 97 | - | 94 | - | 58 | - | 56 | - | 8 | - | 69 | - | 50 |
| 1. (Picture is presented) Semantic self-cue | Clinician prompts semantic description with, “Tell me about it.” Additional prompting follows, as needed: “Where would you find this? What is it used for? Do you have any memories about this?” (If the item is named in this step, the clinician proceeds to step 5.) |
| 2. Orthographic self-cue | Clinician requests written form of the word: “Can you write the word?” If unable to, the participant is encouraged to think of the first letter and/or sound of the word and any other characteristics about the word (i.e., “Is it a long or a short word?”). If the participant cannot come up with the first letter, the clinician writes the first grapheme. |
| 3. Phonemic self-cue | Clinician asks the participant to make the sound associated with the letter. (If the item is named in this step, the clinician proceeds to step 5.) |
| 4. Oral reading | If the item is not yet named, the clinician writes out the remainder of the word and the participant reads it aloud. |
| 5. Written and Spoken Repetition | The participant writes and says the word three times. |
| 6. Semantic Plausibility Judgments | Clinician asks three yes/no questions regarding semantic features of the item (e.g., “would you find this in a toolbox?”) |
| 7. Recall | Clinician asks the participant to provide the most salient semantic features and write and say the word one time. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grasso, S.M.; Peña, E.D.; Kazemi, N.; Mirzapour, H.; Neupane, R.; Bonakdarpour, B.; Gorno-Tempini, M.L.; Henry, M.L. Treatment for Anomia in Bilingual Speakers with Progressive Aphasia. Brain Sci. 2021, 11, 1371. https://doi.org/10.3390/brainsci11111371
Grasso SM, Peña ED, Kazemi N, Mirzapour H, Neupane R, Bonakdarpour B, Gorno-Tempini ML, Henry ML. Treatment for Anomia in Bilingual Speakers with Progressive Aphasia. Brain Sciences. 2021; 11(11):1371. https://doi.org/10.3390/brainsci11111371
Chicago/Turabian StyleGrasso, Stephanie M., Elizabeth D. Peña, Nina Kazemi, Haideh Mirzapour, Rozen Neupane, Borna Bonakdarpour, Maria Luisa Gorno-Tempini, and Maya L. Henry. 2021. "Treatment for Anomia in Bilingual Speakers with Progressive Aphasia" Brain Sciences 11, no. 11: 1371. https://doi.org/10.3390/brainsci11111371