Anhedonia to Gentle Touch in Fibromyalgia: Normal Sensory Processing but Abnormal Evaluation

 , and
, and 
Depression and Anxiety: The Significance of Touch in Psychiatry—Clinical and Neuroscientific Approaches
)
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Background Data
2.2.1. Pain Intensity Aspects
2.2.2. Psychological Distress
2.2.3. Sleeping Problems
2.2.4. Pain Catastrophizing Scale (PCS)
2.2.5. Impact of the Pain Aspects
2.2.6. The European Quality of Life Instrument (EQ-5D)
2.2.7. Pharmacological Treatments
2.3. Stimuli and Procedures
2.3.1. Task
2.3.2. MRI
2.3.3. Analysis
2.3.4. VBM
3. Results
3.1. Clinical Characteristics
3.2. Behavior
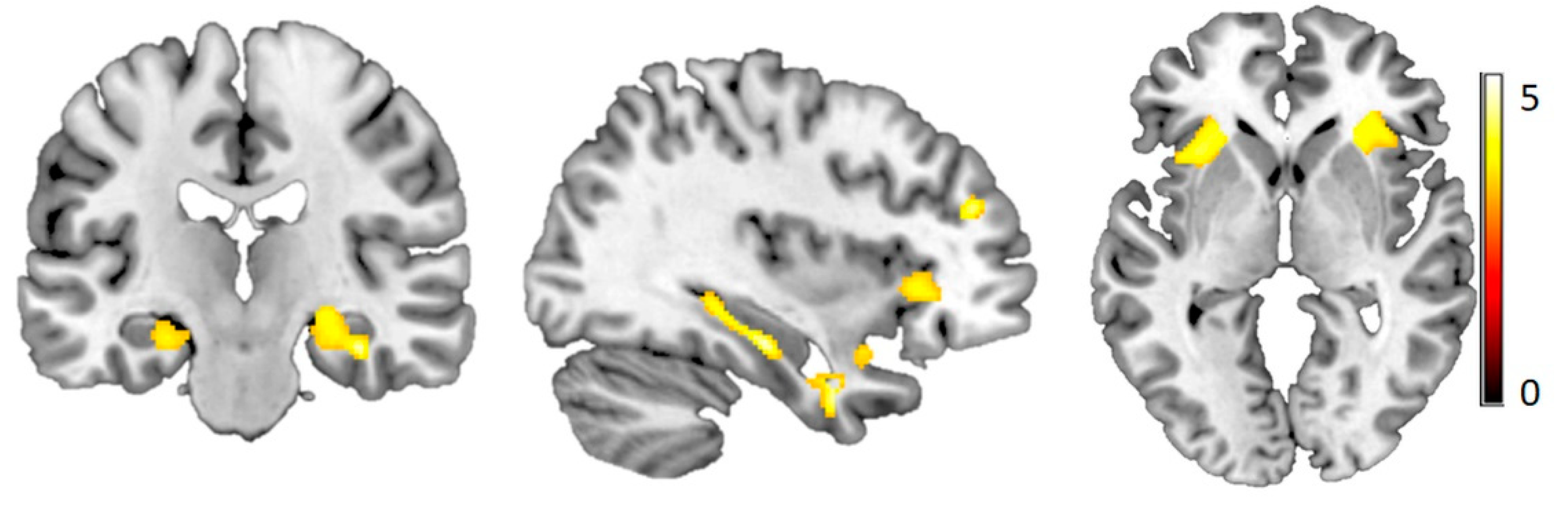
3.3. Functional Imaging
3.4. Voxel-Based Morphometry
4. Discussion
4.1. Behavior
4.2. Functional Imaging
4.3. VBM
4.4. Limitations and Future Direction
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P.; et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990, 33, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Ross, K.; Anderson, J.; Russell, I.J.; Hebert, L. The prevalence and characteristics of fibromyalgia in the general population. Arthritis Rheum. 1995, 38, 19–28. [Google Scholar] [CrossRef] [PubMed]
- McGlone, F.; Wessberg, J.; Olausson, H. Discriminative and affective touch: Sensing and feeling. Neuron 2014, 82, 737–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Löken, L.S.; Wessberg, J.; McGlone, F.; Olausson, H. Coding of pleasant touch by unmyelinated afferents in humans. Nat. Neurosci. 2009, 12, 547. [Google Scholar] [CrossRef]
- Liljencrantz, J.; Strigo, I.; Ellingsen, D.; Krämer, H.; Lundblad, L.; Nagi, S.; Leknes, S.; Olausson, H. Slow brushing reduces heat pain in humans. Eur. J. Pain 2017, 21, 1173–1185. [Google Scholar] [CrossRef] [PubMed]
- Nagi, S.S.; Rubin, T.K.; Chelvanayagam, D.K.; Macefield, V.G.; Mahns, D.A. Allodynia mediated by C-tactile afferents in human hairy skin. J. Physiol. 2011, 589, 4065–4075. [Google Scholar] [CrossRef]
- Serra, J.; Collado, A.; Solà, R.; Antonelli, F.; Torres, X.; Salgueiro, M.; Quiles, C.; Bostock, H. Hyperexcitable C nociceptors in fibromyalgia. Ann. Neurol. 2014, 75, 196–208. [Google Scholar] [CrossRef]
- Case, L.K.; Ceko, M.; Gracely, J.L.; Richards, E.A.; Olausson, H.; Bushnell, M.C. Touch Perception Altered by Chronic Pain and by Opioid Blockade. eNeuro 2016, 3, ENEURO.0138-15.2016. [Google Scholar] [CrossRef]
- Henderson, L.A.; Gandevia, S.C.; Macefield, V.G. Somatotopic organization of the processing of muscle and cutaneous pain in the left and right insula cortex: A single-trial fMRI study. Pain 2007, 128, 20–30. [Google Scholar] [CrossRef]
- Bjornsdotter, M.; Loken, L.; Olausson, H.; Vallbo, A.; Wessberg, J. Somatotopic organization of gentle touch processing in the posterior insular cortex. J. Neurosci. 2009, 29, 9314–9320. [Google Scholar] [CrossRef] [Green Version]
- Harris, R.E.; Sundgren, P.C.; Pang, Y.; Hsu, M.; Petrou, M.; Kim, S.H.; McLean, S.A.; Gracely, R.H.; Clauw, D.J. Dynamic levels of glutamate within the insula are associated with improvements in multiple pain domains in fibromyalgia. Arthritis Rheum. 2008, 58, 903–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Hauser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Arnold, L.M.; Bennett, R.M.; Crofford, L.J.; Dean, L.E.; Clauw, D.J.; Goldenberg, D.L.; Fitzcharles, M.A.; Paiva, E.S.; Staud, R.; Sarzi-Puttini, P.; et al. AAPT Diagnostic Criteria for Fibromyalgia. J. Pain 2019, 20, 611–628. [Google Scholar] [CrossRef] [Green Version]
- Lisspers, J.; Nygren, A.; Söderman, E. Hospital Anxiety and Depression Scale (HAD): Some psychometric data for a Swedish sample. Acta Psychiatr. Scand. 1997, 96, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Bastien, C.H.; Vallieres, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Morin, C.M.; Belleville, G.; Belanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [Green Version]
- Miro, J.; Nieto, R.; Huguet, A. The Catalan version of the Pain Catastrophizing Scale: A useful instrument to assess catastrophic thinking in whiplash patients. J. Pain 2008, 9, 397–406. [Google Scholar] [CrossRef]
- Sullivan, M.; Bishop, S.; Pivik, J. The Pain catastrophizing scale: Development and validation. Psychol. Assess. 1995, 7, 524–532. [Google Scholar] [CrossRef]
- Kemani, M.K.; Grimby-Ekman, A.; Lundgren, J.; Sullivan, M.; Lundberg, M. Factor structure and internal consistency of a Swedish version of the Pain Catastrophizing Scale. Acta Anaesthesiol. Scand. 2019, 63, 259–266. [Google Scholar] [CrossRef] [PubMed]
- EuroQol. EuroQol: A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Brooks, R. EuroQol: The current state of play. Health Policy 1996, 37, 53–72. [Google Scholar] [CrossRef]
- Dolan, P.; Sutton, M. Mapping visual analogue scale health state valuations onto standard gamble and time trade-off values. Soc. Sci. Med. 1997, 44, 1519–1530. [Google Scholar] [CrossRef]
- Ashburner, J.; Friston, K.J. Unified segmentation. Neuroimage 2005, 26, 839–851. [Google Scholar] [CrossRef]
- Morrison, I.; Bjornsdotter, M.; Olausson, H. Vicarious responses to social touch in posterior insular cortex are tuned to pleasant caressing speeds. J. Neurosci. 2011, 31, 9554–9562. [Google Scholar] [CrossRef] [Green Version]
- Larsson, M.B.; Tillisch, K.; Craig, A.; Engström, M.; Labus, J.; Naliboff, B.; Lundberg, P.; Ström, M.; Mayer, E.A.; Walter, S.A. Brain responses to visceral stimuli reflect visceral sensitivity thresholds in patients with irritable bowel syndrome. Gastroenterology 2012, 142, 463–472.e3. [Google Scholar] [CrossRef] [Green Version]
- Backryd, E.; Tanum, L.; Lind, A.L.; Larsson, A.; Gordh, T. Evidence of both systemic inflammation and neuroinflammation in fibromyalgia patients, as assessed by a multiplex protein panel applied to the cerebrospinal fluid and to plasma. J. Pain Res. 2017, 10, 515–525. [Google Scholar] [CrossRef] [Green Version]
- Furer, V.; Hazan, E.; Mor, A.; Segal, M.; Katav, A.; Aloush, V.; Elkayam, O.; George, J.; Ablin, J.N. Elevated Levels of Eotaxin-2 in Serum of Fibromyalgia Patients. Pain Res. Manag. 2018, 2018, 7257681. [Google Scholar] [CrossRef]
- Rodriguez-Pinto, I.; Agmon-Levin, N.; Howard, A.; Shoenfeld, Y. Fibromyalgia and cytokines. Immunol. Lett. 2014, 161, 200–203. [Google Scholar] [CrossRef]
- Stensson, N.; Ghafouri, N.; Ernberg, M.; Mannerkorpi, K.; Kosek, E.; Gerdle, B.; Ghafouri, B. The Relationship of Endocannabinoidome Lipid Mediators With Pain and Psychological Stress in Women With Fibromyalgia: A Case-Control Study. J. Pain 2018, 19, 1318–1328. [Google Scholar] [CrossRef] [PubMed]
- Sluka, K.A.; Clauw, D.J. Neurobiology of fibromyalgia and chronic widespread pain. Neuroscience 2016, 338, 114–129. [Google Scholar] [CrossRef] [PubMed]
- Schrepf, A.; Harper, D.E.; Harte, S.E.; Wang, H.; Ichesco, E.; Hampson, J.P.; Zubieta, J.K.; Clauw, D.J.; Harris, R.E. Endogenous opioidergic dysregulation of pain in fibromyalgia: A PET and fMRI study. Pain 2016, 157, 2217–2225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Üçeyler, N.; Sommer, C. Small nerve fiber pathology. In Fibromylagia Syndrome and Widespread Pain—From Construction to Relevant Recognition; Häuser, W., Perrot, S., Eds.; Wolters Kluwer: Philadelphia, PA, USA, 2018; pp. 204–214. [Google Scholar]
- Gerdle, B.; Larsson, B. Muscle. In Fibromyalgia Syndrome and Widespread Pain—From Construction to Relevant Recognition; Häuser, W., Perrot, S., Eds.; Wolters Kluwer: Philadelphia, PA, USA, 2018; pp. 215–231. [Google Scholar]
- Albrecht, D.S.; Forsberg, A.; Sandstrom, A.; Bergan, C.; Kadetoff, D.; Protsenko, E.; Lampa, J.; Lee, Y.C.; Hoglund, C.O.; Catana, C.; et al. Brain glial activation in fibromyalgia—A multi-site positron emission tomography investigation. Brain Behav. Immun. 2019, 75, 72–83. [Google Scholar] [CrossRef]
- Jensen, K.B.; Kosek, E.; Petzke, F.; Carville, S.; Fransson, P.; Marcus, H.; Williams, S.C.R.; Choy, E.; Giesecke, T.; Mainguy, Y.; et al. Evidence of dysfunctional pain inhibition in Fibromyalgia reflected in rACC during provoked pain. Pain 2009, 144, 95–100. [Google Scholar] [CrossRef]
- Olausson, P.; Gerdle, B.; Ghafouri, N.; Larsson, B.; Ghafouri, B. Identification of proteins from interstitium of trapezius muscle in women with chronic myalgia using microdialysis in combination with proteomics. PLoS ONE 2012, 7, e52560. [Google Scholar] [CrossRef] [Green Version]
- Olausson, P.; Gerdle, B.; Ghafouri, N.; Sjostrom, D.; Blixt, E.; Ghafouri, B. Protein alterations in women with chronic widespread pain—An explorative proteomic study of the trapezius muscle. Sci. Rep. 2015, 5, 11894. [Google Scholar] [CrossRef] [Green Version]
- Hadrevi, J.; Ghafouri, B.; Larsson, B.; Gerdle, B.; Hellstrom, F. Multivariate modeling of proteins related to trapezius myalgia, a comparative study of female cleaners with or without pain. PLoS ONE 2013, 8, e73285. [Google Scholar] [CrossRef] [Green Version]
- Hurtig, I.M.; Raak, R.I.; Kendall, S.A.; Gerdle, B.; Wahren, L.K. Quantitative sensory testing in fibromyalgia patients and in healthy subjects: Identification of subgroups. Clin. J. Pain 2001, 17, 316–322. [Google Scholar] [CrossRef]
- Olausson, H.; Wessberg, J.; Morrison, I.; McGlone, F.; Vallbo, A. The neurophysiology of unmyelinated tactile afferents. Neurosci. Biobehav. Rev. 2010, 34, 185–191. [Google Scholar] [CrossRef]
- Croy, I.; Bierling, A.; Sailer, U.; Ackerley, R. Individual variability of pleasantness ratings to stroking touch over different velocities. Neuroscience 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Frot, M.; Faillenot, I.; Mauguière, F. Processing of nociceptive input from posterior to anterior insula in humans. Hum. Brain Mapp. 2014, 35, 5486–5499. [Google Scholar] [CrossRef] [PubMed]
- Kurth, F.; Zilles, K.; Fox, P.T.; Laird, A.R.; Eickhoff, S.B. A link between the systems: Functional differentiation and integration within the human insula revealed by meta-analysis. Brain Struct. Funct. 2010, 214, 519–534. [Google Scholar] [CrossRef] [PubMed]
- Uddin, L.Q.; Kinnison, J.; Pessoa, L.; Anderson, M.L. Beyond the tripartite cognition–emotion–interoception model of the human insular cortex. J. Cognit. Neurosci. 2014, 26, 16–27. [Google Scholar] [CrossRef] [Green Version]
- Evrard, H.C. The organization of the primate insular cortex. Front. Neuroanat. 2019, 13, 43. [Google Scholar] [CrossRef] [Green Version]
- Craig, A.D. How do you feel—Now? The anterior insula and human awareness. Nat. Rev. Neurosci. 2009, 10, 59–70. [Google Scholar] [CrossRef]
- Geisser, M.E.; Glass, J.M.; Rajcevska, L.D.; Clauw, D.J.; Williams, D.A.; Kileny, P.R.; Gracely, R.H. A psychophysical study of auditory and pressure sensitivity in patients with fibromyalgia and healthy controls. J. Pain 2008, 9, 417–422. [Google Scholar] [CrossRef]
- B Yunus, M. Editorial review (thematic issue: An update on central sensitivity syndromes and the issues of nosology and psychobiology). Curr. Rheumatol. Rev. 2015, 11, 70–85. [Google Scholar] [CrossRef]
- Pollok, B.; Krause, V.; Legrain, V.; Ploner, M.; Freynhagen, R.; Melchior, I.; Schnitzler, A. Differential effects of painful and non-painful stimulation on tactile processing in fibromyalgia syndrome and subjects with masochistic behaviour. PLoS ONE 2010, 5, e15804. [Google Scholar] [CrossRef] [Green Version]
- Kamping, S.; Bomba, I.C.; Kanske, P.; Diesch, E.; Flor, H. Deficient modulation of pain by a positive emotional context in fibromyalgia patients. PAIN® 2013, 154, 1846–1855. [Google Scholar] [CrossRef]
- Wallin, M.; Liedberg, G.; Börsbo, B.; Gerdle, B. Thermal detection and pain thresholds but not pressure pain thresholds are correlated with psychological factors in women with chronic whiplash-associated pain. Clin. J. Pain 2012, 28, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Grundström, H.; Larsson, B.; Arendt-Nielsen, L.; Gerdle, B.; Kjølhede, P. Pain catastrophizing is associated with pain thresholds for heat, cold and pressure in women with chronic pelvic pain. Scand. J. Pain 2020, in press. [Google Scholar]
- Martínez, M.P.; Sánchez, A.I.; Miró, E.; Medina, A.; Lami, M.J. The relationship between the fear-avoidance model of pain and personality traits in fibromyalgia patients. J. Clin. Psychol. Med. Settings 2011, 18, 380–391. [Google Scholar] [CrossRef]
- Lambin, D.I.; Thibault, P.; Simmonds, M.; Lariviere, C.; Sullivan, M.J. Repetition-induced activity-related summation of pain in patients with fibromyalgia. Pain 2011, 152, 1424–1430. [Google Scholar] [CrossRef]
- Burri, A.; Ogata, S.; Rice, D.; Williams, F. Pain catastrophizing, neuroticism, fear of pain, and anxiety: Defining the genetic and environmental factors in a sample of female twins. PLoS ONE 2018, 13, e0194562. [Google Scholar] [CrossRef] [Green Version]
- Shi, H.; Yuan, C.; Dai, Z.; Ma, H.; Sheng, L. Gray matter abnormalities associated with fibromyalgia: A meta-analysis of voxel-based morphometric studies. Semin. Arthritis Rheum. 2016, 46, 330–337. [Google Scholar] [CrossRef]
- Schmidt-Wilcke, T.; Luerding, R.; Weigand, T.; Jürgens, T.; Schuierer, G.; Leinisch, E.; Bogdahn, U. Striatal grey matter increase in patients suffering from fibromyalgia—A voxel-based morphometry study. Pain 2007, 132, S109–S116. [Google Scholar] [CrossRef]
- Burgmer, M.; Gaubitz, M.; Konrad, C.; Wrenger, M.; Hilgart, S.; Heuft, G.; Pfleiderer, B. Decreased gray matter volumes in the cingulo-frontal cortex and the amygdala in patients with fibromyalgia. Psychosom. Med. 2009, 71, 566–573. [Google Scholar] [CrossRef]
- Fallon, N.; Alghamdi, J.; Chiu, Y.; Sluming, V.; Nurmikko, T.; Stancak, A. Structural alterations in brainstem of fibromyalgia syndrome patients correlate with sensitivity to mechanical pressure. NeuroImage Clin. 2013, 3, 163–170. [Google Scholar] [CrossRef] [Green Version]
- Ceko, M.; Bushnell, M.C.; Fitzcharles, M.-A.; Schweinhardt, P. Fibromyalgia interacts with age to change the brain. NeuroImage Clin. 2013, 3, 249–260. [Google Scholar] [CrossRef] [Green Version]
- Gianaros, P.J.; Jennings, J.R.; Sheu, L.K.; Greer, P.J.; Kuller, L.H.; Matthews, K.A. Prospective reports of chronic life stress predict decreased grey matter volume in the hippocampus. Neuroimage 2007, 35, 795–803. [Google Scholar] [CrossRef] [Green Version]
- Felmingham, K.; Williams, L.M.; Whitford, T.J.; Falconer, E.; Kemp, A.H.; Peduto, A.; Bryant, R.A. Duration of posttraumatic stress disorder predicts hippocampal grey matter loss. Neuroreport 2009, 20, 1402–1406. [Google Scholar] [CrossRef]
- Haviland, M.G.; Morton, K.R.; Oda, K.; Fraser, G.E. Traumatic experiences, major life stressors, and self-reporting a physician-given fibromyalgia diagnosis. Psychiatry Res. 2010, 177, 335–341. [Google Scholar] [CrossRef] [Green Version]
- Anderberg, U.; Marteinsdottir, I.; Theorell, T.; Von Knorring, L. The impact of life events in female patients with fibromyalgia and in female healthy controls. Eur. Psychiatry 2000, 15, 295–301. [Google Scholar] [CrossRef]
- Segerdahl, A.R.; Mezue, M.; Okell, T.W.; Farrar, J.T.; Tracey, I. The dorsal posterior insula subserves a fundamental role in human pain. Nat. Neurosci. 2015, 18, 499–500. [Google Scholar] [CrossRef]
- Wiech, K.; Lin, C.-s.; Brodersen, K.H.; Bingel, U.; Ploner, M.; Tracey, I. Anterior insula integrates information about salience into perceptual decisions about pain. J. Neurosci. 2010, 30, 16324–16331. [Google Scholar] [CrossRef]
- Cagnie, B.; Coppieters, I.; Denecker, S.; Six, J.; Danneels, L.; Meeus, M. Central sensitization in fibromyalgia? A systematic review on structural and functional brain MRI. Semin. Arthritis Rheum. 2014, 44, 68–75. [Google Scholar] [CrossRef]
- Uddin, Z.; MacDermid, J.C.; Ham, H.H. Test–retest reliability and validity of normative cut-offs of the two devices measuring touch threshold: Weinstein Enhanced Sensory Test and Pressure-Specified Sensory Device. Hand Ther. 2014, 19, 3–10. [Google Scholar] [CrossRef]
- Rolke, R.; Baron, R.; Maier, C.A.; Tölle, T.; Treede, R.-D.; Beyer, A.; Binder, A.; Birbaumer, N.; Birklein, F.; Bötefür, I. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): Standardized protocol and reference values. Pain 2006, 123, 231–243. [Google Scholar] [CrossRef]
- Pickering, G.; Achard, A.; Corriger, A.; Sickout-Arondo, S.; Macian, N.; Leray, V.; Lucchini, C.; Cardot, J.M.; Pereira, B. Electrochemical Skin Conductance and Quantitative Sensory Testing on Fibromyalgia. Pain Pract. 2020, 20, 348–356. [Google Scholar] [CrossRef]
- Wilbarger, J.L.; Cook, D.B. Multisensory hypersensitivity in women with fibromyalgia: Implications for well being and intervention. Arch. Phys. Med. Rehabilit. 2011, 92, 653–656. [Google Scholar] [CrossRef] [Green Version]
- Vierck, C.J., Jr.; Staud, R.; Price, D.D.; Cannon, R.L.; Mauderli, A.P.; Martin, A.D. The effect of maximal exercise on temporal summation of second pain (windup) in patients with fibromyalgia syndrome. J. Pain 2001, 2, 334–344. [Google Scholar] [CrossRef]
- Woznowski-Vu, A.; Uddin, Z.; Flegg, D.; Aternali, A.; Wickens, R.; Sullivan, M.J.; Sweet, S.N.; Skou, S.T.; Wideman, T.H. Comparing Novel and Existing Measures of Sensitivity to Physical Activity Among People With Chronic Musculoskeletal Pain. Clin. J. Pain 2019, 35, 656–667. [Google Scholar] [CrossRef]
- Schultz, J.; Uddin, Z.; Singh, G.; Howlader, M.M. Glutamate sensing in biofluids: Recent advances and research challenges of electrochemical sensors. Analyst 2020, 145, 321–347. [Google Scholar] [CrossRef]
- Gleich, T.; Deserno, L.; Lorenz, R.C.; Boehme, R.; Pankow, A.; Buchert, R.; Kühn, S.; Heinz, A.; Schlagenhauf, F.; Gallinat, J. Prefrontal and striatal glutamate differently relate to striatal dopamine: Potential regulatory mechanisms of striatal presynaptic dopamine function? J. Neurosci. 2015, 35, 9615–9621. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | HC | n = 29 | FM | n = 31 | Statistics |
|---|---|---|---|---|---|
| Variables | Mean | SD | Mean | SD | p-Value |
| Age (years) | 42.7 | 10.1 | 39.2 | 11.4 | 0.219 |
| Systolic BP (mm Hg) | 113.2 | 8.8 | 121.5 | 12.9 | 0.006 |
| Diastolic BP (mm Hg) | 75.3 | 8.5 | 80.6 | 10.6 | 0.040 |
| Number of tender points | 0.3 | 0.9 | 16.7 | 1.5 | <0.001 |
| FM duration (years) | 4.4 | 5.0 | NA | ||
| Height (m) | 1.69 | 0.06 | 1.66 | 0.06 | 0.090 |
| Weight (kg) | 68.4 | 10.9 | 81.4 | 19.2 | 0.002 |
| BMI (kg/m2) | 23.8 | 3.1 | 29.3 | 6.3 | <0.001 |
| Pain intensity current | 0.0 | 0.0 | 5.7 | 1.8 | <0.001 |
| Pain intensity 4w | 0.0 | 0.0 | 5.9 | 1.8 | <0.001 |
| HADS-Depression | 1.4 | 1.7 | 6.0 | 3.6 | <0.001 |
| HADS-Anxiety | 2.6 | 2.3 | 7.8 | 4.0 | <0.001 |
| PCS | 11.8 | 9.2 | 20.3 | 10.5 | 0.001 |
| ISI | 4.5 | 4.5 | 13.4 | 5.9 | <0.001 |
| Pain hindrance ADL | 5.7 | 2.3 | NA | ||
| Pain hindrance leisure | 5.7 | 2.5 | NA | ||
| Pain hindrance work | 4.9 | 2.7 | NA | ||
| EQ-VAS | 86.8 | 7.8 | 53.3 | 19.5 | <0.001 |
| Region | x | y | z | Hemi-Sphere | Cluster Size | t | p |
|---|---|---|---|---|---|---|---|
| Hippocampus | 36 | −22.5 | −18 | Right | 469 | 4.98 | >0.0001 |
| Parahippocampal Gyrus | 37.5 | −31.5 | −12 | Right | 4.68 | >0.0001 | |
| 24 | −19.5 | −9 | 3.91 | 0.0001 | |||
| −24 | −19.5 | −16.5 | Left | 146 | 3.94 | 0.0002 | |
| Middle Frontal Gyrus | 31.5 | 45 | 22.5 | Right | 233 | 4.69 | >0.0001 |
| Rectal Gyrus | 3 | 37.5 | −28.5 | Right | 339 | 4.51 | >0.0001 |
| Uncus | 34.5 | 0 | −34.5 | Right | 505 | 4.43 | >0.0001 |
| −34.5 | 1.5 | −28.5 | Left | 215 | 3.69 | 0.0003 | |
| Superior Temporal Gyrus | 46.5 | 0 | −16.5 | Right | 3.91 | 0.0001 | |
| −40.5 | 6 | −18 | Left | 3.49 | 0.0005 | ||
| Subcallosal Gyrus | 13.5 | 6 | −19.5 | Right | 288 | 4.29 | >0.0001 |
| Anterior Cingulate | 9 | 18 | −12 | Right | 3.51 | 0.0004 | |
| Anterior Insula | −28.5 | 21 | 1.5 | Left | 764 | 4.20 | >0.0001 |
| 27 | 25.5 | 0 | Right | 430 | 4.13 | 0.0001 | |
| Middle Occipital Gyrus | −22.5 | −88.5 | 4.5 | Left | 175 | 4.18 | 0.0001 |
| Inferior Frontal Gyrus | 37.5 | 24 | −1.5 | Right | 3.77 | 0.0002 | |
| Cingulate Gyrus | −6 | −10.5 | 43.5 | Left | 131 | 4.07 | 0.0001 |
| −9 | −10.5 | 36 | 3.72 | 0.0001 | |||
| Cerebellum | −22.5 | −31.5 | −33 | Left | 72 | 3.69 | 0.0003 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boehme, R.; van Ettinger-Veenstra, H.; Olausson, H.; Gerdle, B.; Nagi, S.S. Anhedonia to Gentle Touch in Fibromyalgia: Normal Sensory Processing but Abnormal Evaluation. Brain Sci. 2020, 10, 306. https://doi.org/10.3390/brainsci10050306
Boehme R, van Ettinger-Veenstra H, Olausson H, Gerdle B, Nagi SS. Anhedonia to Gentle Touch in Fibromyalgia: Normal Sensory Processing but Abnormal Evaluation. Brain Sciences. 2020; 10(5):306. https://doi.org/10.3390/brainsci10050306
Chicago/Turabian StyleBoehme, Rebecca, Helene van Ettinger-Veenstra, Håkan Olausson, Björn Gerdle, and Saad S. Nagi. 2020. "Anhedonia to Gentle Touch in Fibromyalgia: Normal Sensory Processing but Abnormal Evaluation" Brain Sciences 10, no. 5: 306. https://doi.org/10.3390/brainsci10050306