Comparative Study of the Trueness of the Inner Surface of Crowns Fabricated from Three Types of Lithium Disilicate Blocks



Abstract
:1. Introduction
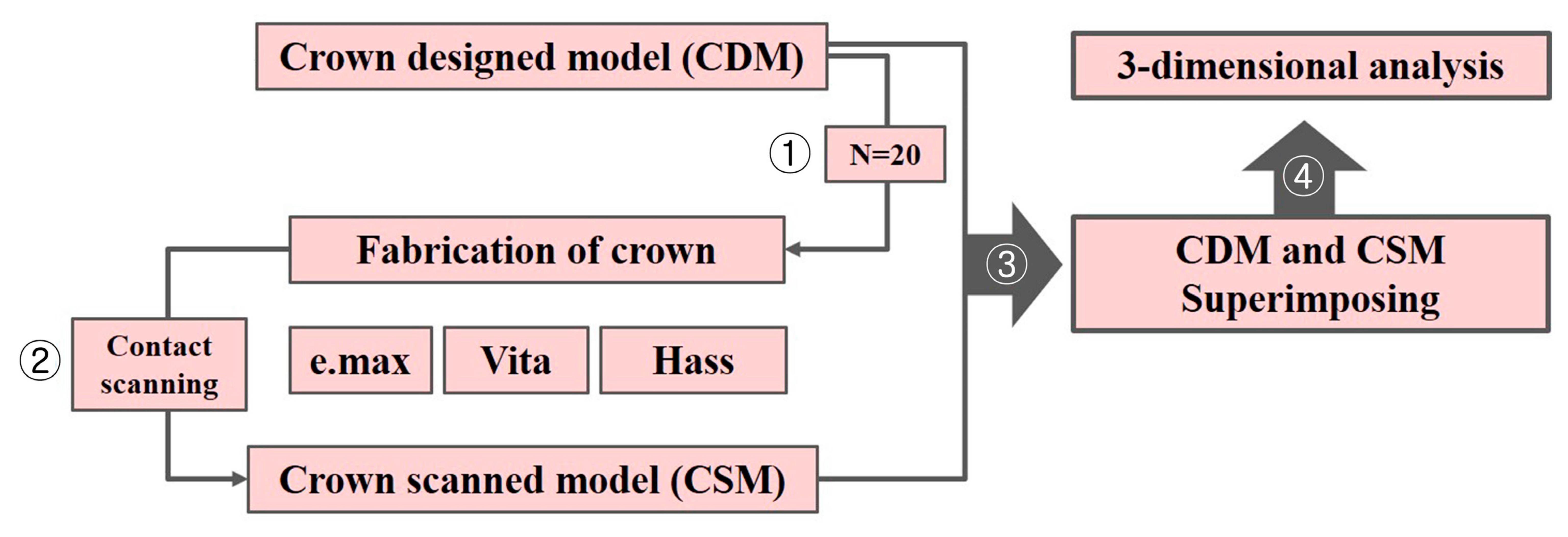
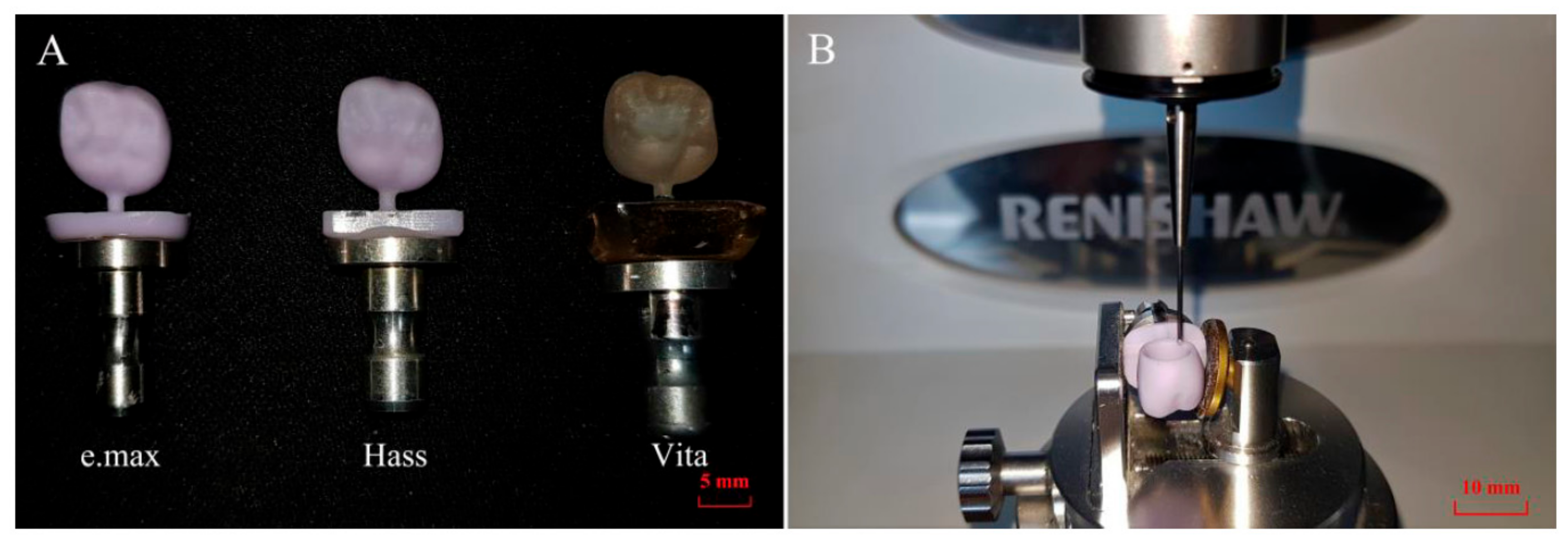
2. Materials and Methods
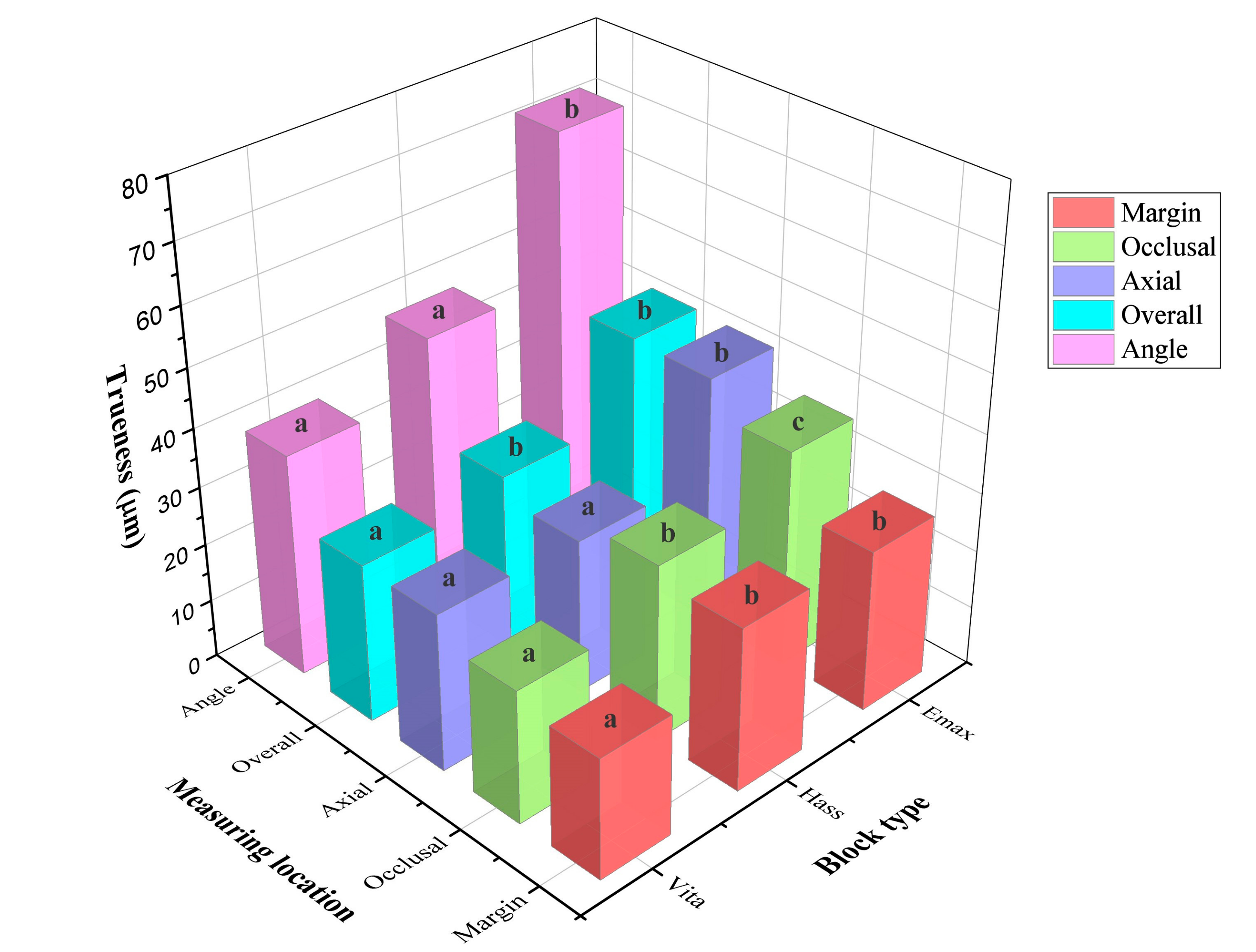
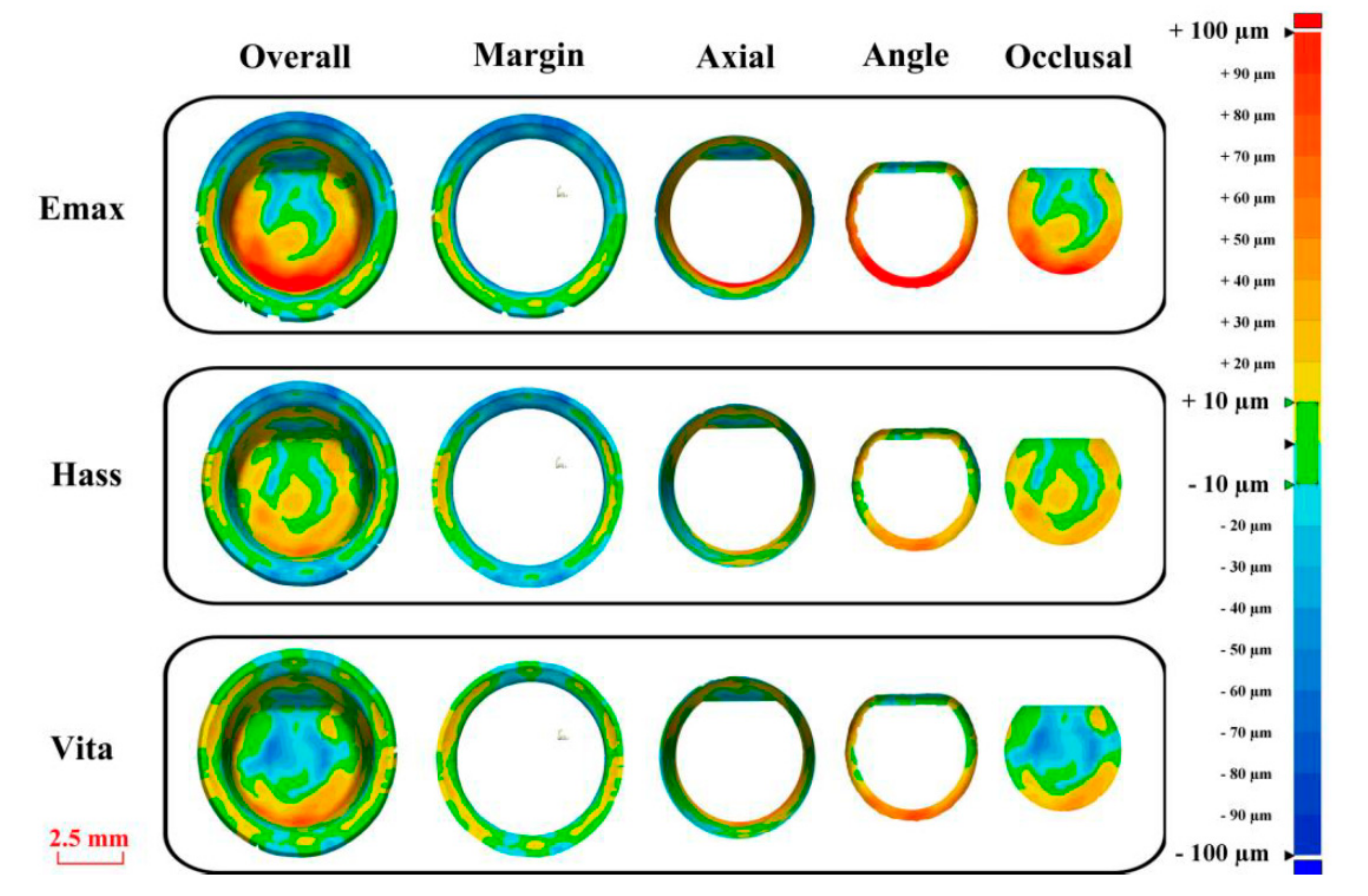
3. Results
4. Discussion
5. Conclusions
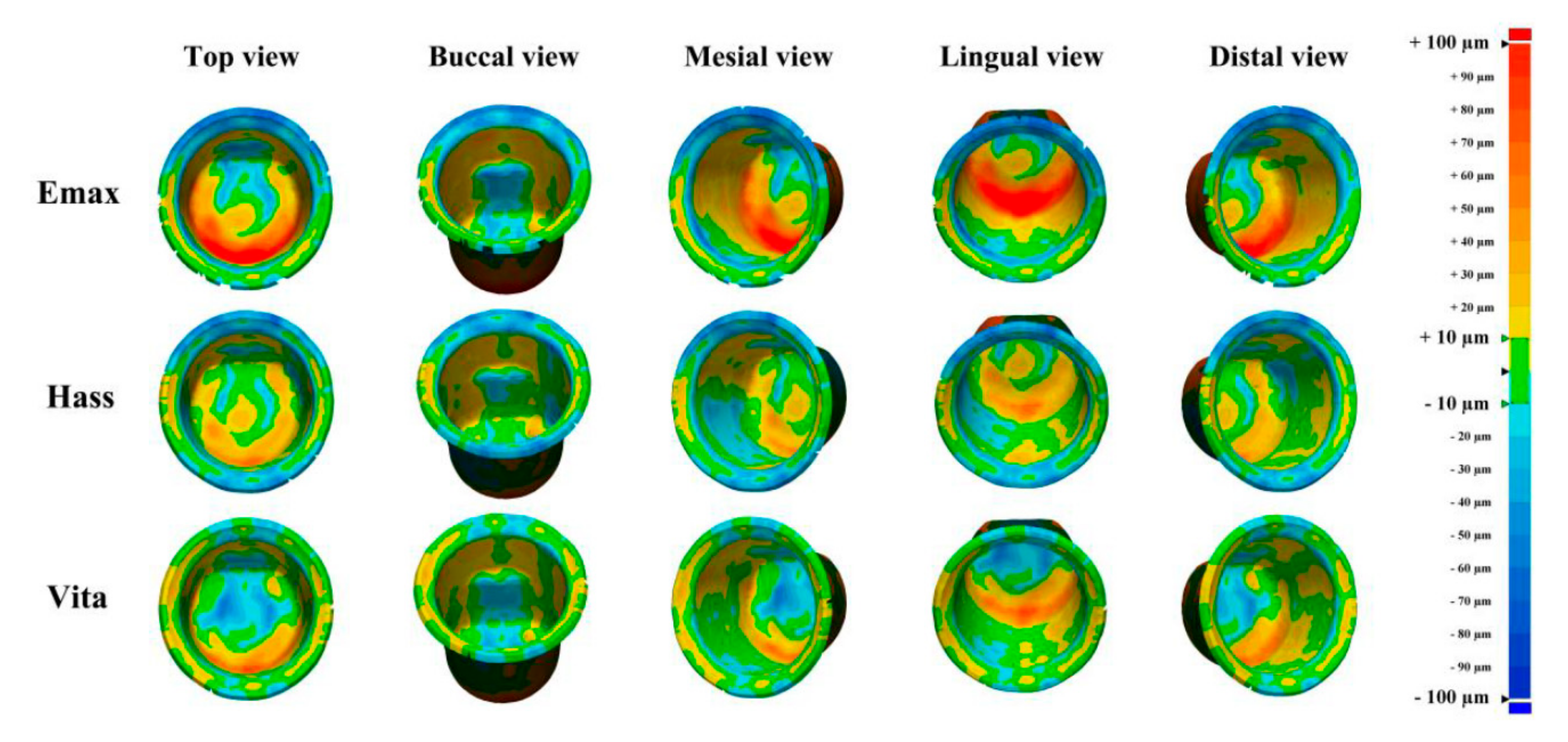
- The trueness of the fabricated crown depended on the type of lithium disilicate block used;
- Therefore, to ensure an excellent marginal and internal fit, consideration should be given to the marginal and internal setting space in the CAD process by referring to the variation in the trueness of the fabricated crown with the type of lithium disilicate block;
- The inner surface of the crown exhibited a different degree of trueness depending on the milling;
- The angular regions of the crown exhibited the greatest degree of error, so compensation in the CAD process is necessary.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Christensen, G.J. Will digital impressions eliminate the current problems with conventional impressions. J. Am. Dent. Assoc. 2008, 139, 761–763. [Google Scholar] [CrossRef]
- Haddadi, Y.; Bahrami, G.; Isidor, F. Accuracy of crowns based on digital intraoral scanning compared to conventional impression—A split-mouth randomised clinical study. Clin. Oral. Investig. 2019, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Mühlemann, S.; Benic, G.I.; Fehmer, V.; Hämmerle, C.H.; Sailer, I. Randomized controlled clinical trial of digital and conventional workflows for the fabrication of zirconia-ceramic posterior fixed partial dentures. Part II: Time efficiency of CAD-CAM versus conventional laboratory procedures. J. Prosthet. Dent. 2019, 1, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Mehl, A.; Ender, A.; Mörmann, W.; Attin, T. Accuracy testing of a new intraoral 3D camera. Int. J. Comput. Dent. 2009, 12, 11–28. [Google Scholar] [PubMed]
- Chun, J.; Tahk, J.; Chun, Y.S.; Park, J.M.; Kim, M. Analysis on the accuracy of intraoral scanners: The effects of mandibular anterior interdental space. Appl. Sci. 2017, 7, 719. [Google Scholar] [CrossRef]
- Kaizer, M.R.; Gierthmuehlen, P.C.; dos Santos, M.B.; Cava, S.S.; Zhang, Y. Speed sintering translucent zirconia for chairside one-visit dental restorations: Optical, mechanical, and wear characteristics. Ceram. Int. 2017, 43, 10999–11005. [Google Scholar] [CrossRef]
- Ho, T.K.; Satterthwaite, J.D.; Silikas, N. The effect of chewing simulation on surface roughness of resin composite when opposed by zirconia ceramic and lithium disilicate ceramic. Dent. Mater. 2018, 34, e15–e24. [Google Scholar] [CrossRef]
- Araujo, N.S.; Moda, M.D.; Silva, E.A.; Zavanelli, A.C.; Mazaro, Q.; Vitor, J. Survival of all-ceramic restorations after a minimum follow-up of five years: A systematic review. Quintessence Int. 2016, 47, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Maietta, S.; De Santis, R.; Catauro, M.; Martorelli, M.; Gloria, A. Theoretical design of multilayer dental posts using CAD-based approach and sol-gel chemistry. Materials 2018, 11, 738. [Google Scholar] [CrossRef]
- De Santis, R.; Gloria, A.; Maietta, S.; Martorelli, M.; De Luca, A.; Spagnuolo, G.; Rengo, S. Mechanical and thermal properties of dental composites cured with CAD/CAM assisted solid-state laser. Materials 2018, 11, 504. [Google Scholar] [CrossRef]
- Bosch, G.; Ender, A.; Mehl, A. A 3-dimensional accuracy analysis of chairside CAD/CAM milling processes. J. Prosthet. Dent. 2014, 112, 1425–1431. [Google Scholar] [CrossRef]
- Zeltner, M.; Sailer, I.; Mühlemann, S.; Özcan, M.; Hämmerle, C.H.; Benic, G.I. Randomized controlled within-subject evaluation of digital and conventional workflows for the fabrication of lithium disilicate single crowns. Part III: Marginal and internal fit. J. Prosthet. Dent. 2017, 117, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Kirsch, C.; Ender, A.; Attin, T.; Mehl, A. Trueness of four different milling procedures used in dental CAD/CAM systems. Clin. Oral. Investig. 2017, 21, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Bohez, E.L. Compensating for systematic errors in 5-axis NC machining. Comput. Aided Des. 2002, 34, 391–403. [Google Scholar] [CrossRef]
- Neves, F.D.; Prado, C.J.; Prudente, M.S.; Carneiro, T.A.; Zancopé, K.; Davi, L.R. Micro-computed tomography evaluation of marginal fit of lithium disilicate crowns fabricated by using chairside CAD/CAM systems or the heat-pressing technique. J. Prosthet. Dent. 2014, 112, 1134–1140. [Google Scholar] [CrossRef]
- Dolev, E.; Bitterman, Y.; Meirowitz, A. Comparison of marginal fit between CAD-CAM and hot-press lithium disilicate crowns. J. Prosthet. Dent. 2019, 121, 124–128. [Google Scholar] [CrossRef]
- Lu, T.; Peng, L.; Xiong, F.; Lin, X.Y.; Zhang, P.; Lin, Z.T. A 3-year clinical evaluation of endodontically treated posterior teeth restored with two different materials using the CEREC AC chair-side system. J. Prosthet. Dent. 2018, 119, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Renne, W.; Wolf, B.; Kessler, R.; McPherson, K.; Mennito, A.S. Evaluation of the marginal fit of CAD/CAM crowns fabricated using two different chairside CAD/CAM systems on preparations of varying quality. J. Esthet. Restor. Dent. 2015, 27, 194–202. [Google Scholar] [CrossRef]
- De Paula Silveira, A.C.; Chaves, S.B.; Hilgert, L.A.; Ribeiro, A.P.D. Marginal and internal fit of CAD-CAM-fabricated composite resin and ceramic crowns scanned by 2 intraoral cameras. J. Prosthet. Dent. 2017, 117, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Papadiochou, S.; Pissiotis, A.L. Marginal adaptation and CAD-CAM technology: A systematic review of restorative material and fabrication techniques. J. Prosthet. Dent. 2018, 119, 545–551. [Google Scholar] [CrossRef]
- Martínez, S.; Cuesta, E.; Barreiro, J.; Álvarez, B. Analysis of laser scanning and strategies for dimensional and geometrical control. Int. J. Adv. Manuf. Technol. 2010, 46, 621–629. [Google Scholar] [CrossRef]
- Choi, Y.K.; Banerjee, A. Tool path generation and tolerance analysis for free-form surfaces. Int. J. Mach. Tools Manufac. 2007, 47, 689–696. [Google Scholar] [CrossRef]
- Xiao, Z.; Yang, Y.; Xiao, R.; Bai, Y.; Song, C.; Wang, D. Evaluation of topology-optimized lattice structures manufactured via selective laser melting. Mater. Des. 2018, 143, 27–37. [Google Scholar] [CrossRef]
- Ender, A.; Attin, T.; Mehl, A. In vivo precision of conventional and digital methods of obtaining complete-arch dental impressions. J. Prosthet. Dent. 2016, 115, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Camardella, L.T.; Breuning, H.; de Vasconcellos Vilella, O. Accuracy and reproducibility of measurements on plaster models and digital models created using an intraoral scanner. J. Orofac. Orthop. 2017, 78, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.; Koller, C.; Rumetsch, M.; Ender, A.; Mehl, A. Precision of guided scanning procedures for full-arch digital impressions in vivo. J. Orofac. Orthop. 2017, 78, 466–471. [Google Scholar] [CrossRef]
- Park, G.H.; Son, K.; Lee, K.B. Feasibility of using an intraoral scanner for a complete-arch digital scan. J. Prosthet. Dent. 2018, (in press). [Google Scholar] [CrossRef]
- Kim, C.M.; Kim, S.R.; Kim, J.H.; Kim, H.Y.; Kim., W.C. Trueness of milled prostheses according to number of ball-end mill burs. J. Prosthet. Dent. 2016, 115, 624–629. [Google Scholar] [CrossRef]
- Nouri, M.; Asefi, S.; Baghban, A.A.; Aminian, A.; Shamsa, M.; Massudi, R. Validity and reliability of a three-dimensional dental cast simulator for arch dimension measurements. Dent. Res. J. 2014, 11, 656–662. [Google Scholar]
- Zhang, F.; Suh, K.J.; Lee, K.M. Validity of intraoral scans compared with plaster models: An in-vivo comparison of dental measurements and 3D surface analysis. PLoS ONE 2016, 11, 1–10. [Google Scholar] [CrossRef]
- Lim, J.H.; Park, J.M.; Kim, M.; Heo, S.J.; Myung, J.Y. Comparison of digital intraoral scanner reproducibility and image trueness considering repetitive experience. J. Prosthet. Dent. 2018, 119, 225–232. [Google Scholar] [CrossRef]
- Marghalani, A.; Weber, H.P.; Finkelman, M.; Kudara, Y.; El Rafie, K.; Papaspyridakos, P. Digital versus conventional implant impressions for partially edentulous arches: An evaluation of accuracy. J. Prosthet. Dent. 2018, 119, 574–579. [Google Scholar] [CrossRef]
- Patzelt, S.B.; Bishti, S.; Stampf, S.; Att, W. Accuracy of computer-aided design/computer-aided manufacturing–generated dental casts based on intraoral scanner data. J. Am. Dent. Assoc. 2014, 145, 1133–1140. [Google Scholar] [CrossRef]
- Accuracy (Trueness and Precision) of Measurement Methods and Results–General Principles and Definitions; ISO 5725-1; International Organization for Standardization: Geneva, Switzerland, 1994.
- Renne, W.; Ludlow, M.; Fryml, J.; Schurch, Z.; Mennito, A.; Kessler, R. Evaluation of the accuracy of 7 digital scanners: An in vitro analysis based on 3-dimensional comparisons. J. Prosthet. Dent. 2017, 118, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Kalberer, N.; Mehl, A.; Schimmel, M.; Müller, F.; Srinivasan, M. CAD-CAM milled versus rapidly prototyped (3D-printed) complete dentures: An in vitro evaluation of trueness. J. Prosthet. Dent. 2018, (in press). [Google Scholar] [CrossRef] [PubMed]
- Hwang, H.J.; Lee, S.J.; Park, E.J.; Yoon, H.I. Assessment of the trueness and tissue surface adaptation of CAD-CAM maxillary denture bases manufactured using digital light processing. J. Prosthet. Dent. 2019, 121, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.Y.; Park, J.H.; Kim, J.H.; Kim, W.C. Accuracy of provisional crowns made using stereolithography apparatus and subtractive technique. J. Adv. Prosthodont. 2018, 10, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Dimitrova, M. A 3D Evaluation of the Repeatability of Accuracy in Optical and Contact Scanners. Ph.D. Thesis, Cardiff Metropolitan University, Cardiff, UK, 2017. [Google Scholar]
- Son, K.; Lee, W.S.; Lee, K.B. Prediction of the learning curves of 2 dental CAD software programs. J. Prosthet. Dent. 2019, 121, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Song, X.F.; Ren, H.T.; Yin, L. Machinability of lithium disilicate glass ceramic in in vitro dental diamond bur adjusting process. J. Mech. Behav. Biomed. Mater. 2016, 53, 78–92. [Google Scholar] [CrossRef]
- Gold, S.A.; Ferracane, J.L.; da Costa, J. Effect of crystallization firing on marginal gap of CAD/CAM fabricated lithium disilicate crowns. J. Prosthodont. 2018, 27, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Izadi, A.; Vafaee, F.; Shishehian, A.; Roshanaei, G.; Afkari, B.F. Evaluation of dimensional accuracy of dental bridges manufactured with conventional casting technique and CAD/CAM system with Ceramill Sintron blocks using CMM. J. Dent. Res. Dent. Clin. Dent. Prospects 2018, 12, 264. [Google Scholar] [CrossRef] [PubMed]
- Persson, A.; Andersson, M.; Oden, A.; Sandborgh-Englund, G. A three-dimensional evaluation of a laser scanner and a touch-probe scanner. J. Prosthet. Dent. 2006, 95, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Yu, H.; Liu, Y.; Jiang, X.; Gao, B. Trueness analysis of zirconia crowns fabricated with 3-dimensional printing. J. Prosthet. Dent. 2019, 121, 285–291. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lithium Disilicate Block | Material | Lot Number/Manufacturer |
|---|---|---|
| IPS e.max CAD (e.max) | Lithium disilicate glass ceramic | V36449/Ivoclar Vivadent |
| Rosetta SM (HASS) | Lithium disilicate glass ceramic | ABD06KE1502/HASS |
| VITA Suprinity (VITA) | Zirconia-reinforced lithium silicate glass ceramic | 46191/VITA |
| e.max | HASS | VITA | p | |
|---|---|---|---|---|
| Crown Inner Region | RMS (µm), Mean ± SD | |||
| Margin | 27.7 ± 2.9Aa | 28.0 ± 3.4Aa | 20.7 ± 6.6Ab | <0.001 * |
| Axis | 42.6 ± 6.5Ba | 26.6 ± 11.1Ab | 27.1 ± 10.4Ab | <0.001 * |
| Angular | 71.4 ± 6.3Ca | 46.8 ± 14.5Bb | 38.1 ± 7.5Bb | <0.001 * |
| Occlusal | 37.2 ± 4.2Ba | 30.3 ± 5.9Ab | 22.8 ± 4.0Ac | <0.001 * |
| p | <0.001 * | <0.001 * | <0.001 * | |
| Overall RMS value | 42.9 ± 4.4a | 30.1 ± 9.0b | 27.3 ± 7.9b | <0.001 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Son, K.; Yu, B.-y.; Yoon, T.H.; Lee, K.-b. Comparative Study of the Trueness of the Inner Surface of Crowns Fabricated from Three Types of Lithium Disilicate Blocks. Appl. Sci. 2019, 9, 1798. https://doi.org/10.3390/app9091798
Son K, Yu B-y, Yoon TH, Lee K-b. Comparative Study of the Trueness of the Inner Surface of Crowns Fabricated from Three Types of Lithium Disilicate Blocks. Applied Sciences. 2019; 9(9):1798. https://doi.org/10.3390/app9091798
Chicago/Turabian StyleSon, Keunbada, Beom-young Yu, Tae Ho Yoon, and Kyu-bok Lee. 2019. "Comparative Study of the Trueness of the Inner Surface of Crowns Fabricated from Three Types of Lithium Disilicate Blocks" Applied Sciences 9, no. 9: 1798. https://doi.org/10.3390/app9091798