Effectiveness of Collagen Membrane in the Treatment of Schneiderian Membrane Perforation


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
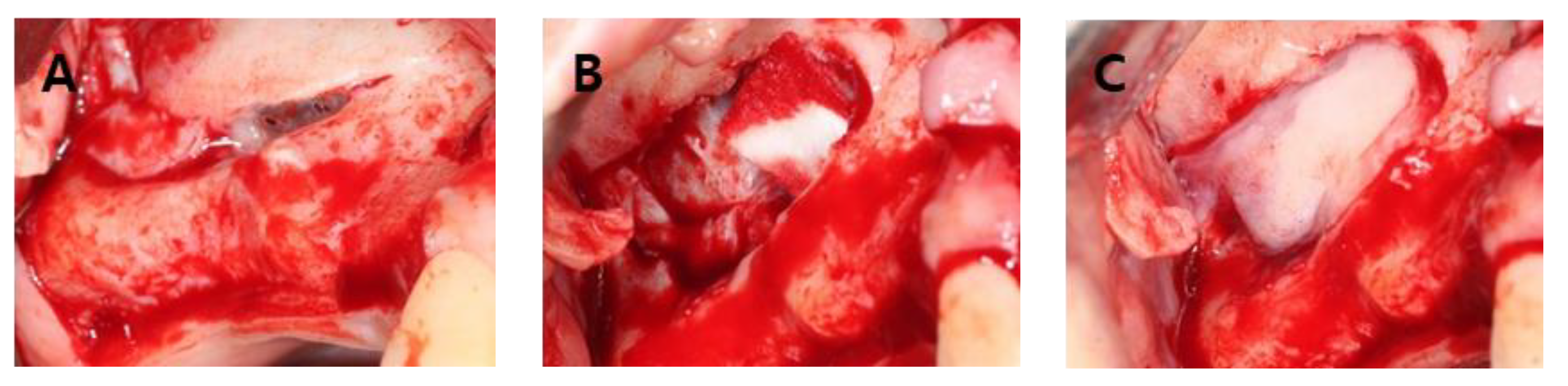
- (A)
- Group 1: No SMP but the membrane was weakened (or thinned) during sinus lift procedure;
- (B)
- Group 2: SMP was small to medium in size (< 10 mm) during sinus lift procedure;
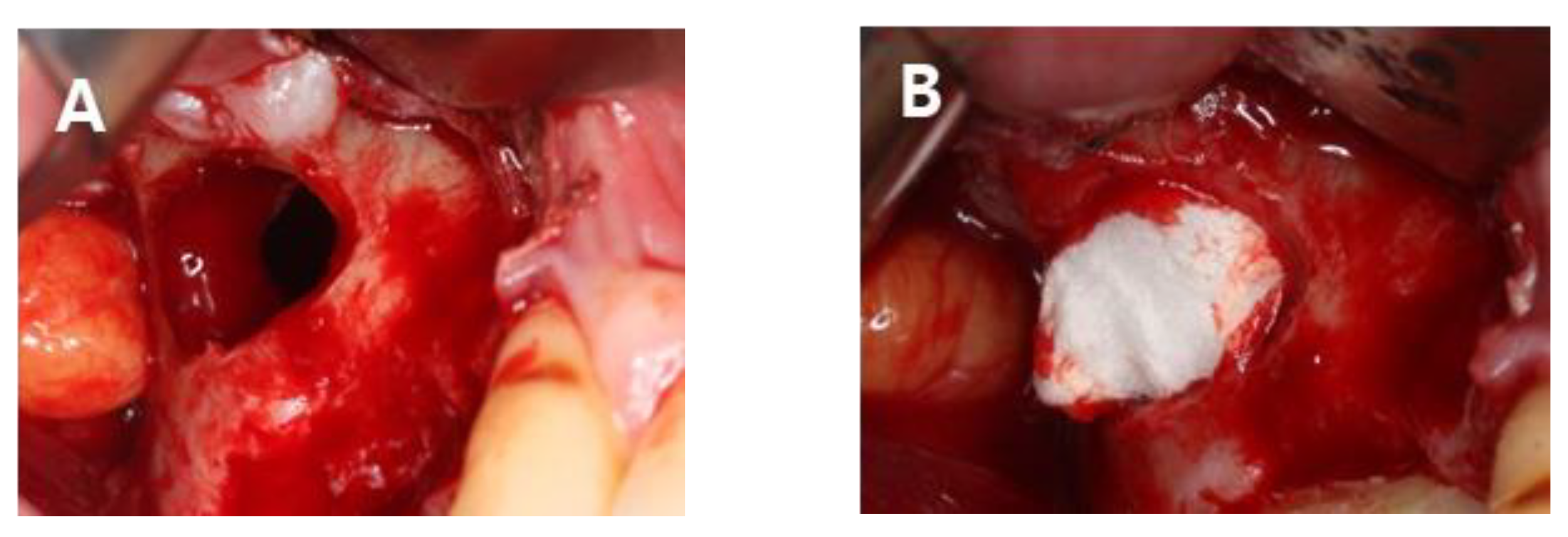
- (C)
- Group 3: SMP was large in size (> 10 mm) during sinus lift procedure;
- (D)
- Control: Sinus membrane was not perforated during sinus lift procedure.
2.2. Maxillary Sinus Lift Procedure
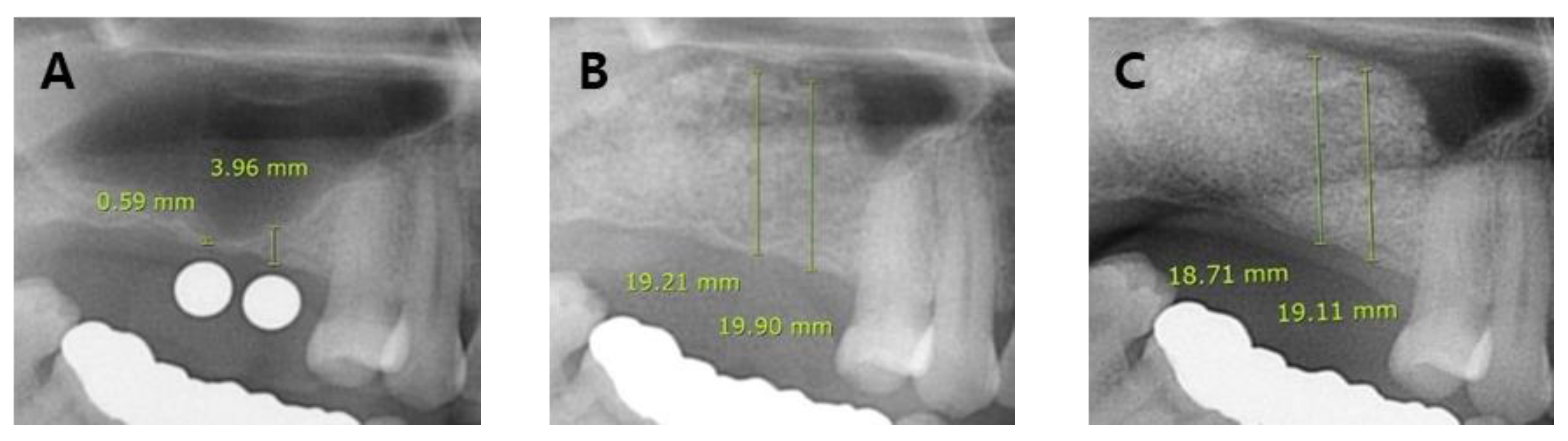
2.3. Radiographic Examination
2.4. Statistical Analysis
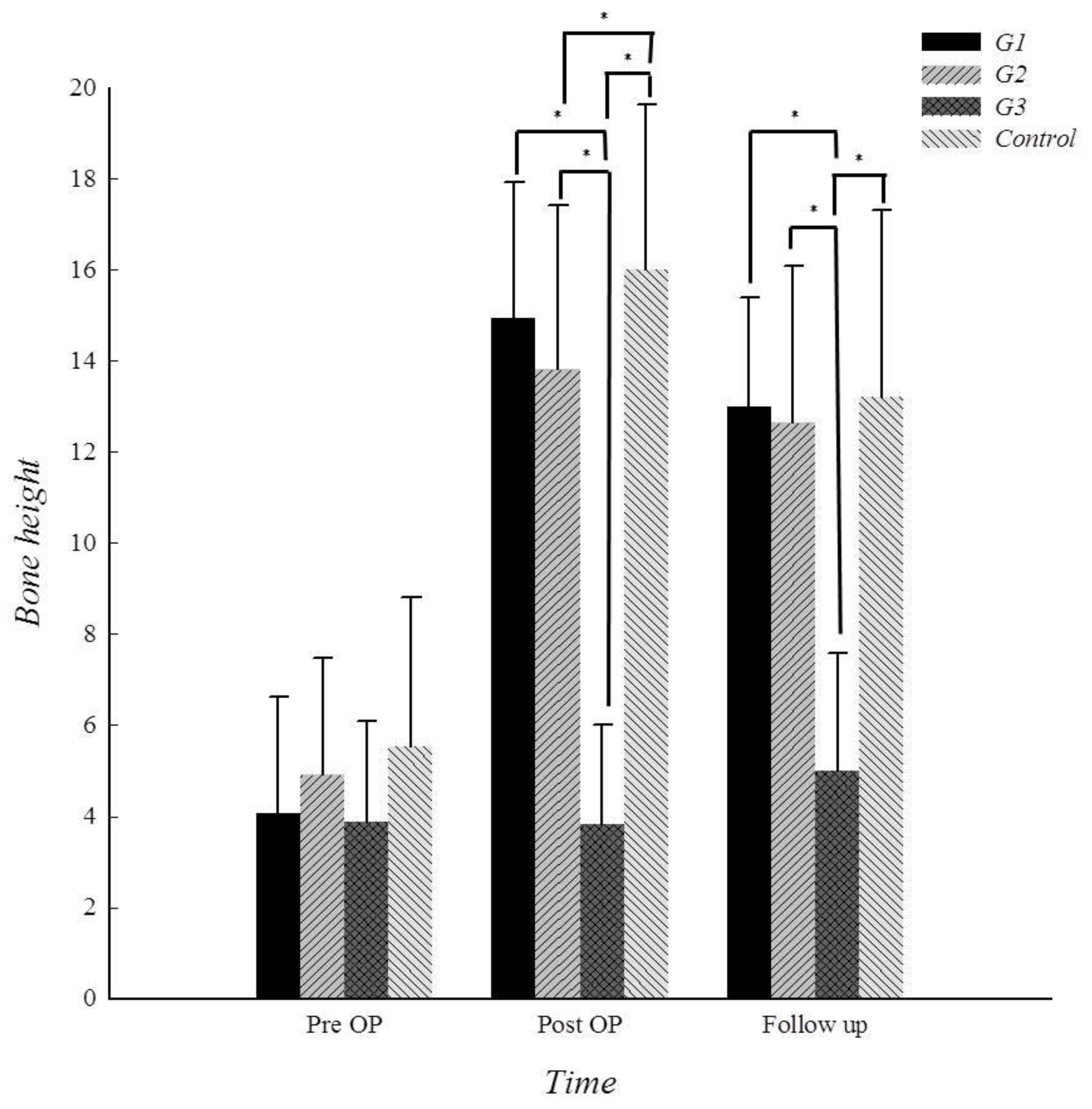
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Tatum, H., Jr. Maxillary and sinus implant reconstructions. Dent. Clin. North. Am. 1986, 30, 207–229. [Google Scholar] [PubMed]
- Boyne, P.J.; James, R.A. Grafting of the maxillary sinus floor with autogenous marrow and bone. J. Oral. Surg. 1980, 38, 613–616. [Google Scholar] [PubMed]
- Stern, A.; Green, J. Sinus lift procedures: An overview of current techniques. Dent. Clin. North. Am. 2012, 56, 219–233. [Google Scholar] [CrossRef] [PubMed]
- Katranji, A.; Fotek, P.; Wang, H.L. Sinus augmentation complications: Etiology and treatment. Implant. Dent. 2008, 17, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Al-Dajani, M. Incidence, Risk Factors, and Complications of Schneiderian Membrane Perforation in Sinus Lift Surgery: A Meta-Analysis. Implant. Dent. 2016, 25, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Fugazzotto, P.A.; Vlassis, J. A simplified classification and repair system for sinus membrane perforations. J. Periodontol. 2003, 74, 1534–1541. [Google Scholar] [CrossRef] [PubMed]
- Choi, B.H.; Zhu, S.J.; Jung, J.H.; Lee, S.H.; Huh, J.Y. The use of autologous fibrin glue for closing sinus membrane perforations during sinus lifts. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2006, 101, 150–154. [Google Scholar] [CrossRef] [PubMed]
- An, J.H.; Park, S.H.; Han, J.J.; Jung, S.; Kook, M.S.; Park, H.J.; Ryu, S.Y.; Oh, H.K. Treatment of dental implant displacement into the maxillary sinus. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 35. [Google Scholar] [CrossRef] [PubMed]
- Pikos, M.A. Maxillary sinus membrane repair: Report of a technique for large perforations. Implant. Dent. 1990, 8, 29–34. [Google Scholar] [CrossRef]
- Proussaefs, P.; Lozada, J.; Kim, J.; Rohrer, M.D. Repair of the perforated sinus membrane with a resorbable collagen membrane: A human study. Int. J. Oral. Maxillofac. Implants. 2004, 19, 413–420. [Google Scholar] [PubMed]
- Pikos, M.A. Maxillary sinus membrane repair: Update on technique for large and complete perforations. Implant. Dent. 2008, 17, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.J.; Na, I.C.; Jang, H.W.; Jung, M.J.; Kim, B.O. The increase of keratinized and attached gingiva using collagen wound dressing in dogs: A clinical and histomorphometric comparative study. Oral. Biology Research. 2015, 39, 10–17. [Google Scholar]
- de Oliveira, H.A.A.B.; de Moraes, R.P.F.; Limirio, P.H.J.O.; Dechichi, P. Repair of a perforated sinus membrane with an autogenous periosteal graft: A study in 24 patients. Br. J. Oral. Maxillofac. Surg. 2018, 56, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Proussaefs, P.; Lozada, J. The “Loma Linda pouch”: A technique for repairing the perforated sinus membrane. Int. J. Periodontics Restorative Dent. 2003, 23, 593–597. [Google Scholar] [PubMed]
- Chanavaz, M. Maxillary sinus: Anatomy, physiology, surgery and bone grafting related to implantology—eleven years of surgical experience (1979–1990). J. Oral. Implantol. 1990, 16, 199–209. [Google Scholar] [PubMed]
- Cricchio, G.; Palma, V.C.; Faria, P.E.P.; de Olivera, J.A.; Lundgren, S.; Sennerby, L.; Salata, L.A. Histological outcomes on the development of new space-making devices for maxillary sinus floor augmentation. Clin. Implant. Dent. Relat. Res. 2011, 13, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Lundgren, S.; Andersson, S.; Gualini, F.; Sennerby, L. Bone reformation with sinus membrane elevation: A new surgical technique for maxillary sinus floor augmentation. Clin. Implant. Dent. Relat. Res. 2004, 6, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Thor, A.; Sennerby, L.; Hirsch, J.M.; Rasmusson, L. Bone formation at the maxillary sinus floor following simultaneous elevation of the mucosal lining and implant installation without graft material: An evaluation of 20 patients treated with 44 Astra Tech implants. J. Oral. Maxillofac. Surg. 2007, 65, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Sul, S.H.; Choi, B.H.; Li, J.; Jeong, S.M.; Xuan, F. Effects of sinus membrane elevation on bone formation around implants placed in the maxillary sinus cavity: An experimental study. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2008, 105, 684–687. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characters | .. | Group 1 | Group 2 | Group 3 | Control | ||||
|---|---|---|---|---|---|---|---|---|---|
| n (%) | Average ± SD | n (%) | Average ± SD | n (%) | Average ± SD | n (%) | Average ± SD | ||
| Gender | F | 11 (73.3) | 4 (36.4) | 4 (33.3) | 18 (48.6) | ||||
| M | 4 (26.7) | 7 (63.6) | 8 (66.7) | 19 (51.4) | |||||
| Age | <65 | 13 (86.7) | 55.8 ± 12.946 | 9 (81.8) | 51.181 ± 9.042 | 8 (66.7) | 57.916 ± 14.368 | 29 (78.4) | 57.378 ± 10.034 |
| ≥65 | 2 (13.3) | 2 (18.2) | 4 (33.3) | 8 (21.6) | |||||
| Sinus Septum | Yes | 3 (20) | 6 (54.5) | 5 (41.7) | 7 (18.9) | ||||
| No | 12 (80) | 5 (45.5) | 7 (58.3) | 30 (81.1) | |||||
| Residual Bone Height | <4.0 | 13 (86.7) | 2.037 ± 1.436 | 10 (90.9) | 2.036 ± 1.415 | 10 (83.3) | 2.200 ± 1.351 | 29 (78.4) | 2.270 ± 1.441 |
| ≥4.0 | 2 (13.3) | 1 (9.1) | 2 (16.7) | 6 (22.2) | |||||
| Alveolar Width | 1–2 teeth gap | 8 (53.3) | 2.6 ± 0.910 | 4 (36.4) | 3.000 ± 0.894 | 5 (41.7) | 2.916 ± 1.083 | 30 (81.1) | 2.000 ± 0.707 |
| 3–4 teeth gap | 7 (46.7) | 7 (63.6) | 7 (58.3) | 7 (18.9) | |||||
| G | Perforation | Repair | N (site) | Grafting of BS (site) | Implant (Patient/implant) | Complication | ||
|---|---|---|---|---|---|---|---|---|
| 1 | Weakened | CM | 15 | simultaneous | 15 | Simultaneous | 14/34 | 1 |
| Delayed | 1/2 | 0 | ||||||
| None | 0 | |||||||
| 2 | Small (<10mm) | CM + FA | 11 | simultaneous | 11 | Simultaneous | 1/2 | 0 |
| Delayed | 8/23 | 1 | ||||||
| None | 2 | 0 | ||||||
| 3 | Large (>10mm) | CP | 12 | delayed | 1 | Simultaneous | 0 | 0 |
| 0 | 0 | |||||||
| Delayed | 0 | 0 | ||||||
| None | 1 | 0 | ||||||
| none | 11 | Simultaneous | 6/13 | 1 | ||||
| Delayed | 4/9 | 1 | ||||||
| None | 1/0 | 0 | ||||||
| Group | Pre op | Post op | Follow-up | Source: F(p) |
|---|---|---|---|---|
| 1 | 4.08 ± 2.55 | 14.94 ± 3.00 | 13.00 ± 2.40 | Group: 52.97 (<.001) Time: 203.67 (<.001) Group*Time: 11.67 (<.001) |
| 2 | 4.92 ± 2.55 | 13.81 ± 3.61 | 12.65 ± 3.43 | |
| 3 | 3.88 ± 2.21 | 3.82 ± 2.19 | 4.99 ± 2.59 | |
| Control | 5.53 ± 3.29 | 16.00 ± 3.63 | 13.22 ± 4.09 |
| Group | Pre op | Post op | Follow-Up |
|---|---|---|---|
| Diff. (M ± SD) | |||
| Group 1 – Group 2 | −0.84 ± 0.69 | 1.12 ± 0.89 | 0.34 ± 0.78 |
| Group 1 – Group 3 | 0.19 ± 0.72 | 11.11 ± 0.81* | 8.00 ± 0.73* |
| Group 1 – Control | −1.45 ± 0.67 | −1.05 ± 0.75 | −0.22 ± 0.65 |
| Group 2 – Group 3 | 1.04 ± 0.74 | 9.99 ± 0.96* | 7.66 ± 0.96* |
| Group 2 – Control | −0.61 ± 0.72 | −2.18 ± 0.84* | −0.56 ± 0.91 |
| Group 3 – Control | −1.65 ± 0.82 | −12.72 ± 0.67* | −8.23 ± 0.78* |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.-Y.; Kwon, J.-J.; Sándor, G.K.; Kim, Y.-D. Effectiveness of Collagen Membrane in the Treatment of Schneiderian Membrane Perforation. Appl. Sci. 2019, 9, 1514. https://doi.org/10.3390/app9071514
Lee J-Y, Kwon J-J, Sándor GK, Kim Y-D. Effectiveness of Collagen Membrane in the Treatment of Schneiderian Membrane Perforation. Applied Sciences. 2019; 9(7):1514. https://doi.org/10.3390/app9071514
Chicago/Turabian StyleLee, Jae-Yeol, Jin-Ju Kwon, George K. Sándor, and Yong-Deok Kim. 2019. "Effectiveness of Collagen Membrane in the Treatment of Schneiderian Membrane Perforation" Applied Sciences 9, no. 7: 1514. https://doi.org/10.3390/app9071514