Nano-Structured Demineralized Human Dentin Matrix to Enhance Bone and Dental Repair and Regeneration

Abstract
:1. Introduction
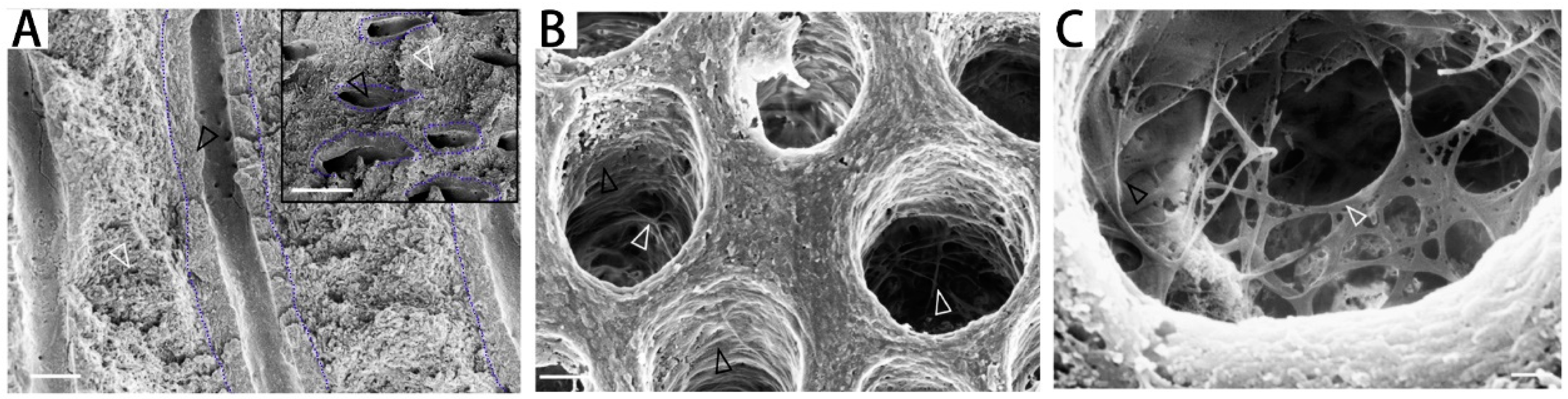
2. Demineralized Dentin Matrix (DDM) Microstructure
3. DDM Preparation
4. Application of DDM in Bone Regeneration
5. Application of DDM in Tooth Regeneration
6. DDM as a Carrier to Deliver Growth Factors
7. DDM Incorporation into Other Advanced Biomaterials
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Pereira, D.D.M.; Habibovic, P. Biomineralization-Inspired Material Design for Bone Regeneration. Adv. Healthc. Mater. 2018, 7, 1800700. [Google Scholar] [CrossRef] [PubMed]
- Dimitriou, R.; Mataliotakis, G.I.; Angoules, A.G.; Kanakaris, N.K.; Giannoudis, P.V. Complications Following Autologous Bone Graft Harvesting from the Iliac Crest and Using the Ria: A Systematic Review. Injury 2011, 42, S3–S15. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Feng, C.; Yang, G.; Li, G.; Ding, X.; Wang, S.; Dou, Y.; Zhang, Z.; Chang, J.; Wu, C.; et al. 3d-Printed Scaffolds with Synergistic Effect of Hollow-Pipe Structure and Bioactive Ions for Vascularized Bone Regeneration. Biomaterials 2017, 135, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Winkler, T.; Sass, F.A.; Duda, G.N.; Schmidt-Bleek, K. A Review of Biomaterials in Bone Defect Healing, Remaining Shortcomings and Future Opportunities for Bone Tissue Engineering: The Unsolved Challenge. Bone Joint Res. 2018, 7, 232–243. [Google Scholar] [CrossRef] [PubMed]
- Ritting, A.W.; Weber, E.W.; Lee, M.C. Exaggerated Inflammatory Response and Bony Resorption from Bmp-2 Use in a Pediatric Forearm Nonunion. J. Hand Surg. 2012, 37, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Kempen, D.H.R.; Lu, L.; Heijink, A.; Hefferan, T.E.; Creemers, L.B.; Maran, A.; Yaszemski, M.J.; Dhert, W.J.A. Effect of Local Sequential Vegf and Bmp-2 Delivery on Ectopic and Orthotopic Bone Regeneration. Biomaterials 2009, 30, 2816–2825. [Google Scholar] [CrossRef] [PubMed]
- Moya, A.; Paquet, J.; Deschepper, M.; Larochette, N.; Oudina, K.; Denoeud, C.; Bensidhoum, M.; Logeart-Avramoglou, D.; Petite, H. Human Mesenchymal Stem Cell Failure to Adapt to Glucose Shortage and Rapidly Use Intracellular Energy Reserves through Glycolysis Explains Poor Cell Survival after Implantation. Stem Cells 2018, 36, 363–376. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.K.; Lee, J.; Um, I.W.; Kim, K.W.; Murata, M.; Akazawa, T.; Mitsugi, M. Tooth-Derived Bone Graft Material. J. Korean Assoc. Oral Maxillofac. Surg. 2013, 39, 103. [Google Scholar] [CrossRef] [PubMed]
- Kruzic, J.J.; Ritchie, R.O. Fatigue of Mineralized Tissues: Cortical Bone and Dentin. Mech. Behav. Biomed. 2008, 1, 3–17. [Google Scholar] [CrossRef] [PubMed]
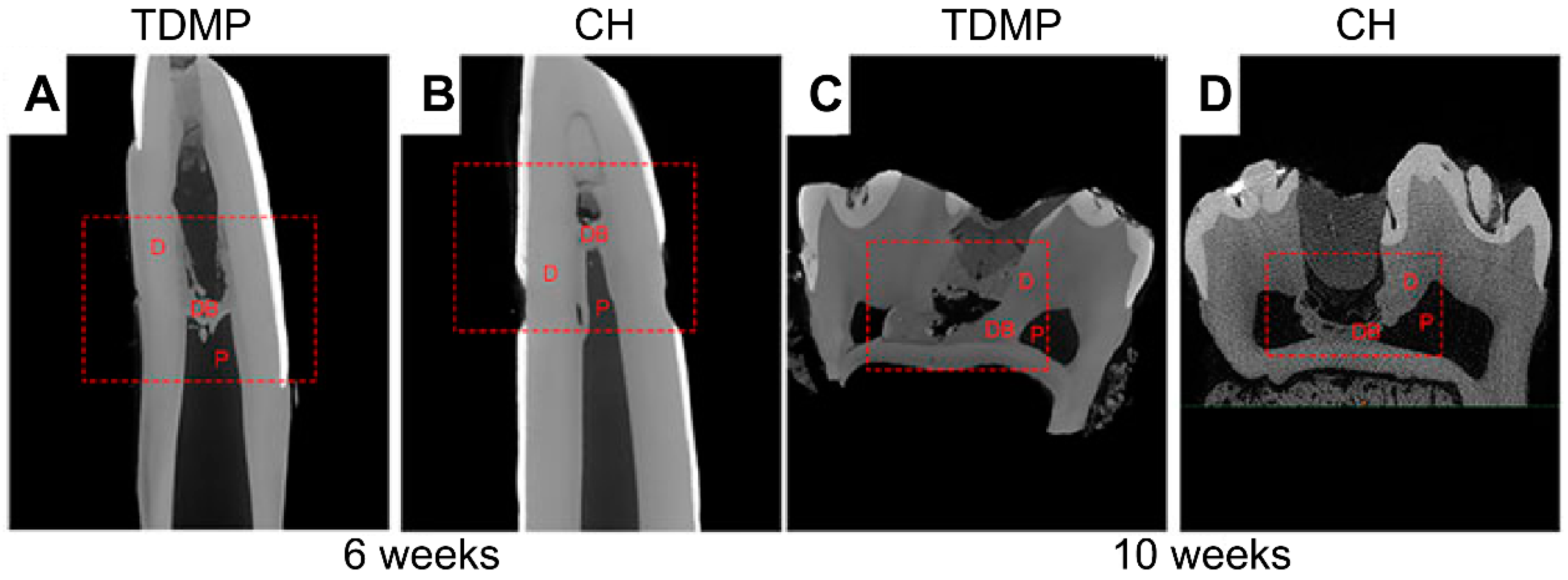
- Chen, J.; Cui, C.; Qiao, X.; Yang, B.; Yu, M.; Guo, W.; Tian, W. Treated Dentin Matrix Paste as a Novel Pulp Capping Agent for Dentin Regeneration. J. Tissue Eng. Regen. Med. 2017, 11, 3428–3436. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Ma, C.; Xie, X.; Sun, H.; Liu, X. Pulp Regeneration in a Full-Length Human Tooth Root Using a Hierarchical Nanofibrous Microsphere System. Acta Biomater. 2016, 35, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.K.; Lee, J.H.; Um, I.W.; Cho, W.J. Guided Bone Regeneration Using Demineralized Dentin Matrix: Long-Term Follow-Up. J. Oral Maxil. Surg. 2016, 74, 515. [Google Scholar] [CrossRef] [PubMed]
- Qin, X.; Zou, F.; Chen, W.; Xu, Y.; Ma, B.; Huang, Z.; Zhu, G.; Zhou, B. Demineralized Dentin as a Semi-Rigid Barrier for Guiding Periodontal Tissue Regeneration. J. Periodontol. 2015, 86, 1370–1379. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Chen, G.; Li, J.; Zou, Q.; Xie, D.; Chen, Y.; Wang, H.; Zheng, X.; Long, J.; Tang, W.; et al. Tooth Root Regeneration Using Dental Follicle Cell Sheets in Combination with a Dentin Matrix—Based Scaffold. Biomaterials 2012, 33, 2449–2461. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Gong, K.; Shi, H.; Zhu, G.; He, Y.; Ding, B.; Wen, L.; Jin, Y. Dental Follicle Cells and Treated Dentin Matrix Scaffold for Tissue Engineering the Tooth Root. Biomaterials 2012, 33, 1291–1302. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Guo, W.; Yang, B.; Guo, L.; Sheng, L.; Chen, G.; Li, Y.; Zou, Q.; Xie, D.; An, X.; et al. Human Treated Dentin Matrix as a Natural Scaffold for Complete Human Dentin Tissue Regeneration. Biomaterials 2011, 32, 4525–4538. [Google Scholar] [CrossRef] [PubMed]
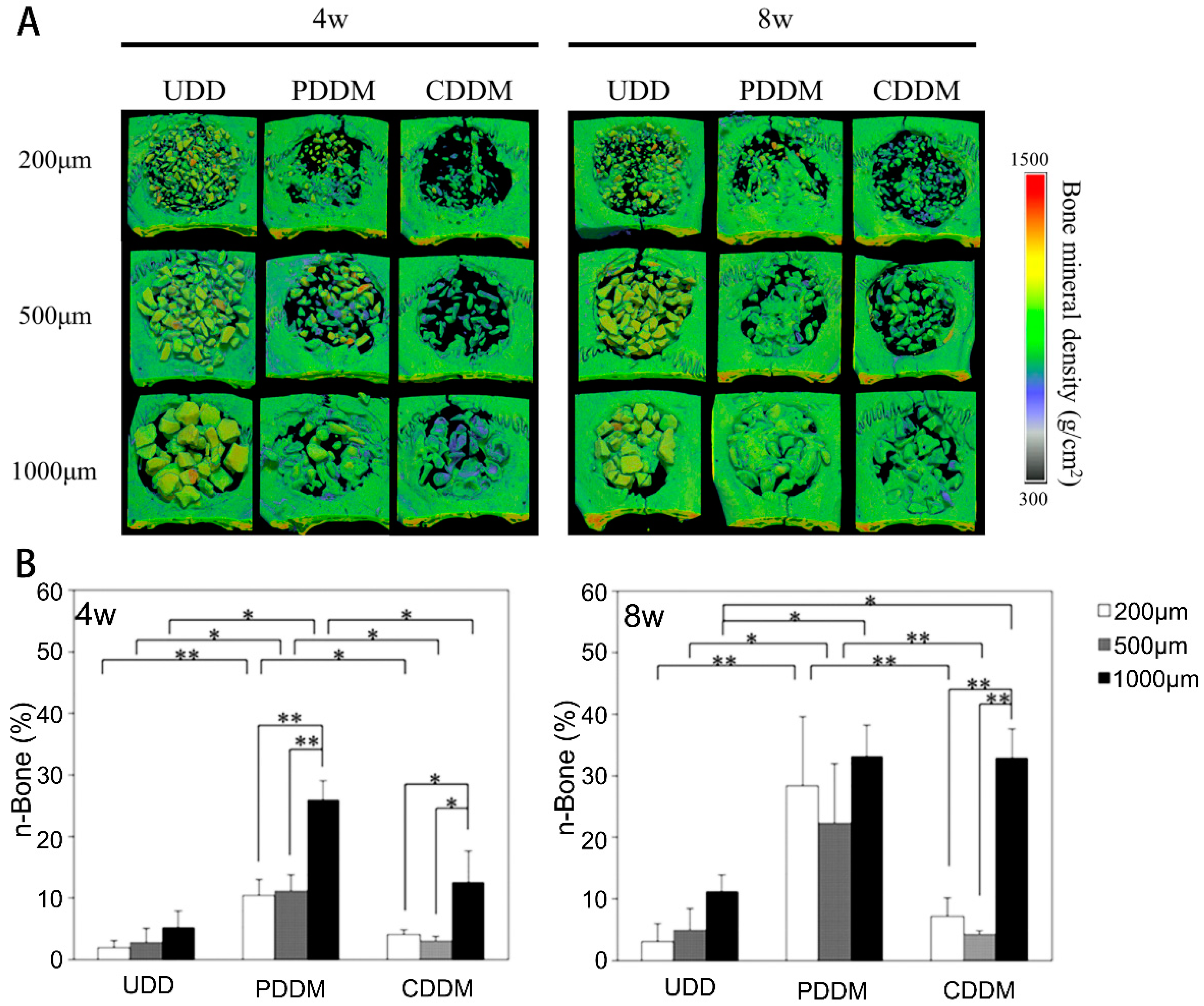
- Koga, T.; Minamizato, T.; Kawai, Y.; Miura, K.I.; Takashi, I.; Nakatani, Y.; Sumita, Y.; Asahina, I. Bone Regeneration Using Dentin Matrix Depends on the Degree of Demineralization and Particle Size. PLoS ONE 2016, 11, e0147235. [Google Scholar] [CrossRef] [PubMed]
- Togari, K.; Miyazawa, K.; Yagihashi, K.; Tabuchi, M.; Maeda, H.; Kawai, T.; Goto, S. Bone Regeneration by Demineralized Dentin Matrix in Skull Defects of Rats. J. Hard Tissue Biol. 2012, 21, 25–33. [Google Scholar] [CrossRef]
- Reis-Filho, C.R.; Silva, E.R.; Martins, A.B.; Pessoa, F.F.; Gomes, P.V.; de Araújo, M.S.; Miziara, M.N.; Alves, J.B. Demineralised Human Dentine Matrix Stimulates the Expression of Vegf and Accelerates the Bone Repair in Tooth Sockets of Rats. Arch. Oral Biol. 2012, 57, 469. [Google Scholar] [CrossRef] [PubMed]
- Yagihashi, K.; Miyazawa, K.; Togari, K.; Goto, S. Demineralized Dentin Matrix Acts as a Scaffold for Repair of Articular Cartilage Defects. Calcified Tissue Int. 2009, 84, 210–220. [Google Scholar] [CrossRef] [PubMed]
- Gomes, M.F.; dos Anjos, M.J.; Nogueira Tde, O.; Catanzaro Guimaraes, S.A. Autogenous Demineralized Dentin Matrix for Tissue Engineering Applications: Radiographic and Histomorphometric Studies. Int. J. Oral Max. Implants 2002, 17, 488–497. [Google Scholar]
- Carvalho, V.A.; Tosello Dde, O.; Salgado, M.A.; Gomes, M.F. Histomorphometric Analysis of Homogenous Demineralized Den tin Matrix as Osteopromotive Material in Rabbit Mandibles. Int. J. Oral Maxillofac Implants 2004, 19, 679–686. [Google Scholar] [PubMed]
- Bormann, K.H.; Suarez-Cunqueiro, M.M.; Sinikovic, B.; Kampmann, A.; See, C.V.; Tavassol, F.; Binger, T.; Winkler, M.; Gellrich, N.C.; Rücker, M. Dentin as a Suitable Bone Substitute Comparable to β-TCP-an Experimental Study in Mice. Microvasc. Res. 2012, 84, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Bertassoni, L.E. Dentin on the Nanoscale: Hierarchical Organization, Mechanical Behavior and Bioinspired Engineering. Dent. Mater. 2017, 33, 637–649. [Google Scholar] [CrossRef] [PubMed]
- Habelitz, S.; Balooch, M.; Marshall, S.J.; Balooch, G.; Marshall, G.W., Jr. In Situ Atomic Force Microscopy of Partially Demineralized Human Dentin Collagen Fibrils. J. Struct. Biol. 2002, 138, 227–236. [Google Scholar] [CrossRef]
- Orgel, J.P.; Irving, T.C.; Miller, A.; Wess, T.J. Microfibrillar Structure of Type I Collagen in Situ. Proc. Natl. Acad. Sci. USA 2006, 103, 9001–9005. [Google Scholar] [CrossRef] [PubMed]
- Goh, K.; Hiller, J.; Haston, J.; Kadler, K.; Murdoch, A.; Meakin, J.; Wess, T. Analysis of Collagen Fibril Diameter Distribution in Connective Tissues Using Small-Angle X-Ray Scattering. BBA Gen. Subj. 2005, 1722, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Bertassoni, L.E.; Swain, M.V. Removal of Dentin Non-Collagenous Structures Results in the Unraveling of Microfibril Bundles in Collagen Type I. Connect. Tissue Res. 2017, 58, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Butler, W.T.; Brunn, J.C.; Qin, C. Dentin Extracellular Matrix (Ecm) Proteins: Comparison to Bone Ecm and Contribution to Dynamics of Dentinogenesis. Connect. Tissue Res. 2003, 44, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Katherine, A.S.; Vicky, E.M.; Colin, F. The Importance of the Sibling Family of Proteins on Skeletal Mineralisation and Bone Remodelling. J. Endocrinol. 2012, 214, 241. [Google Scholar]
- Um, I.W.; Kim, Y.K.; Mitsugi, M. Demineralized Dentin Matrix Scaffolds for Alveolar Bone Engineering. J. Indian Prosthodont. Soc. 2017, 17, 120. [Google Scholar] [CrossRef] [PubMed]
- Avery, S.J.; Sadaghiani, L.; Sloan, A.J.; Waddington, R.J. Analysing the Bioactive Makeup of Demineralised Dentine Matrix on Bone Marrow Mesenchymal Stem Cells for Enhanced Bone Repair. Eur. Cell Mater. 2017, 34, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Ranc, V.; Zizka, R.; Chaloupkova, Z.; Sevcik, J.; Zboril, R. Imaging of Growth Factors on a Human Tooth Root Canal by Surface-Enhanced Raman Spectroscopy. Anal. Bioanal. Chem. 2018, 410, 7113–7120. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Schultz, T.; Schultz, M. Intact Growth Factors Are Conserved in the Extracellular Matrix of Ancient Human Bone and Teeth: A Storehouse for the Study of Human Evolution in Health and Disease. Biol. Chem. 2005, 386, 767. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.M.; Sugars, R.V.; Wendel, M.; Smith, A.J.; Waddington, R.J.; Cooper, P.R.; Sloan, A.J. Tgf-B/Extracellular Matrix Interactions in Dentin Matrix: A Role in Regulating Sequestration and Protection of Bioactivity. Calcified Tissue Int. 2009, 85, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Cooper, P.R.; Smith, G.; Nor, J.E.; Smith, A.J. Angiogenic Activity of Dentin Matrix Components. J. Endodon. 2011, 37, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Bertassoni, L.E.; Stankoska, K.; Swain, M.V. Insights into the Structure and Composition of the Peritubular Dentin Organic Matrix and the Lamina Limitans. Micron 2012, 43, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.; Sun, Y.; Maciejewska, I.; Qin, D.; Peng, T.; McIntyre, B.; Wygant, J.; Butler, W.T.; Qin, C. Distribution of Sibling Proteins in the Organic and Inorganic Phases of Rat Dentin and Bone. Eur. J. Oral Sci. 2008, 116, 104–112. [Google Scholar]
- Um, I.W.; Jun, S.H.; Yun, P.Y.; Kim, Y.K. Histological Comparison of Autogenous and Allogenic Demineralized Dentin Matrix Loaded with Recombinant Human Bone Morphogenetic Protein-2 for Alveolar Bone Repair: A Preliminary Report. J. Hard Tissue Biol. 2017, 26, 417–423. [Google Scholar] [CrossRef]
- Li, J.; Yang, J.; Zhong, X.; He, F.; Wu, X.; Shen, G. Demineralized Dentin Matrix Composite Collagen Material for Bone Tissue Regeneration. J. Biomater. Sci. Polym. Ed. 2013, 24, 1519–1528. [Google Scholar] [CrossRef] [PubMed]
- Kabir, M.A.; Murata, M.; Akazawa, T.; Kusano, K.; Yamada, K.; Ito, M. Evaluation of Perforated Demineralized Dentin Scaffold on Bone Regeneration in Critical-Size Sheep Iliac Defects. Clin. Oral Implants Res. 2017, 28, e227–e235. [Google Scholar] [CrossRef] [PubMed]
- Minamizato, T.; Koga, T.; Takashi, I.; Nakatani, Y.; Umebayashi, M.; Sumita, Y.; Ikeda, T.; Asahina, I. Clinical Application of Autogenous Partially Demineralized Dentin Matrix Prepared Immediately after Extraction for Alveolar Bone Regeneration in Implant Dentistry: A Pilot Study. Int. J. Oral Maxillofac. Surg. 2018, 47, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; He, Y.; Zhang, X.; Lu, W.; Wang, C.; Yu, H.; Liu, Y.; Li, Y.; Zhou, Y.; Zhou, J.; et al. The Use of Dentin Matrix Scaffold and Dental Follicle Cells for Dentin Regeneration. Biomaterials 2009, 30, 6708–6723. [Google Scholar] [CrossRef] [PubMed]
- Melling, G.E.; Colombo, J.; Avery, S.J.; Ayre, W.; Evans, S.L.; Waddington, R.J.; Sloan, A.J. Liposomal Delivery of Demineralised Dentine Matrix for Dental Tissue Regeneration. Tissue Eng. Part A 2018, 24, 1057–1065. [Google Scholar] [CrossRef] [PubMed]
- Nam, J.W.; Kim, M.Y.; Han, S.J. Cranial Bone Regeneration According to Different Particle Sizes and Densities of Demineralized Dentin Matrix in the Rabbit Model. Maxillofac. Plast. Reconstr. Surg. 2016, 38, 27. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Mah, Y.J.; Kim, D.H.; Kim, E.S.; Park, E.J. Demineralized Deciduous Tooth as a Source of Bone Graft Material: Its Biological and Physicochemical Characteristics. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 120, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Park, S.M.; Kim, D.H.; Pang, E.K. Bone Formation of Demineralized Human Dentin Block Graft with Different Demineralization Time: In Vitro and in Vivo Study. J. Craniomaxillofac. Surg. 2017, 45, 903–912. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Kim, K.W.; Um, I.W.; Kim, Y.K.; Lee, J.K. Bone Healing Capacity of Demineralized Dentin Matrix Materials in a Mini-Pig Cranium Defect. J. Korean Dent. Sci. 2012, 5, 21–28. [Google Scholar] [CrossRef]
- Lee, D.H.; Yang, K.Y.; Lee, J.K. Porcine Study on the Efficacy of Autogenous Tooth Bone in the Maxillary Sinus. J. Korean Assoc. Oral Maxillofac. Surg. 2013, 39, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Salehi, S.; Cooper, P.; Smith, A.; Ferracane, J. Dentin Matrix Components Extracted with Phosphoric Acid Enhance Cell Proliferation and Mineralization. Dent. Mater. 2016, 32, 334–342. [Google Scholar] [CrossRef] [PubMed]
- Hefeng, Y.; Yu, H.; Jingjing, S.; Weihua, G.; Weidong, T.; Song, L. Treated Dentin Matrix Enhances Proliferation and Osteogenic Differentiation of Bone Marrow Mesenchymal Stem Cells. West China J. Stomatol. 2016, 34, 281–285. [Google Scholar]
- de Oliveira, G.S.; Miziara, M.N.; Silva, E.R.; Ferreira, E.L.; Biulchi, A.P.; Alves, J.B. Enhanced Bone Formation During Healing Process of Tooth Sockets Filled with Demineralized Human Dentine Matrix. Aust. Dent. J. 2013, 58, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Pang, K.M.; Um, I.W.; Kim, Y.K.; Woo, J.M.; Kim, S.M.; Lee, J.H. Autogenous Demineralized Dentin Matrix from Extracted Tooth for the Augmentation of Alveolar Bone Defect: A Prospective Randomized Clinical Trial in Comparison with Anorganic Bovine Bone. Clin. Oral Implan. Res. 2017, 28, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.P.; Colombo, J.S.; Ayre, W.N.; Sloan, A.J.; Waddington, R.J. Elucidating the Cellular Actions of Demineralised Dentine Matrix Extract on a Clonal Dental Pulp Stem Cell Population in Orchestrating Dental Tissue Repair. J. Tissue Eng. 2015, 6. [Google Scholar] [CrossRef] [PubMed]
- Qin, W.; Gao, X.; Ma, T.; Weir, M.D.; Zou, J.; Song, B.; Lin, Z.; Schneider, A.; Xu, H.H.K. Metformin Enhances the Differentiation of Dental Pulp Cells into Odontoblasts by Activating Ampk Signaling. J. Endod. 2018, 44, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Widbiller, M.; Driesen, R.B.; Eidt, A.; Lambrichts, I.; Hiller, K.A.; Buchalla, W.; Schmalz, G.; Galler, K.M. Cell Homing for Pulp Tissue Engineering with Endogenous Dentin Matrix Proteins. J. Endod. 2018, 44, 956–962. [Google Scholar] [CrossRef] [PubMed]
- Kang, K.J.; Lee, M.S.; Moon, C.W.; Lee, J.H.; Yang, H.S.; Jang, Y.J. In Vitro and in Vivo Dentinogenic Efficacy of Human Dental Pulp-Derived Cells Induced by Demineralized Dentin Matrix and Ha-Tcp. Stem Cells Int. 2017, 2017, 2416254. [Google Scholar] [CrossRef] [PubMed]
- Jiao, L.; Xie, L.; Yang, B.; Yu, M.; Jiang, Z.; Feng, L.; Guo, W.; Tian, W. Cryopreserved Dentin Matrix as a Scaffold Material for Dentin-Pulp Tissue Regeneration. Biomaterials 2014, 35, 4929–4939. [Google Scholar] [CrossRef] [PubMed]
- Mehrvarzfar, P.; Abbott, P.V.; Akhavan, H.; Savadkouhi, S.T. Modified Revascularization in Human Teeth Using an Intracanal Formation of Treated Dentin Matrix: A Report of Two Cases. J. Int. Soc. Prev. Community Dent. 2017, 7, 218–221. [Google Scholar] [PubMed]
- Vo, T.N.; Kasper, F.K.; Mikos, A.G. Strategies for Controlled Delivery of Growth Factors and Cells for Bone Regeneration. Adv. Drug Deliv. Rev. 2012, 64, 1292–1309. [Google Scholar] [CrossRef] [PubMed]
- Um, I.W. Demineralized Dentin Matrix (Ddm) as a Carrier for Recombinant Human Bone Morphogenetic Proteins (Rhbmp-2). Adv. Exp. Med. Biol. 2018, 1077, 487–499. [Google Scholar] [PubMed]
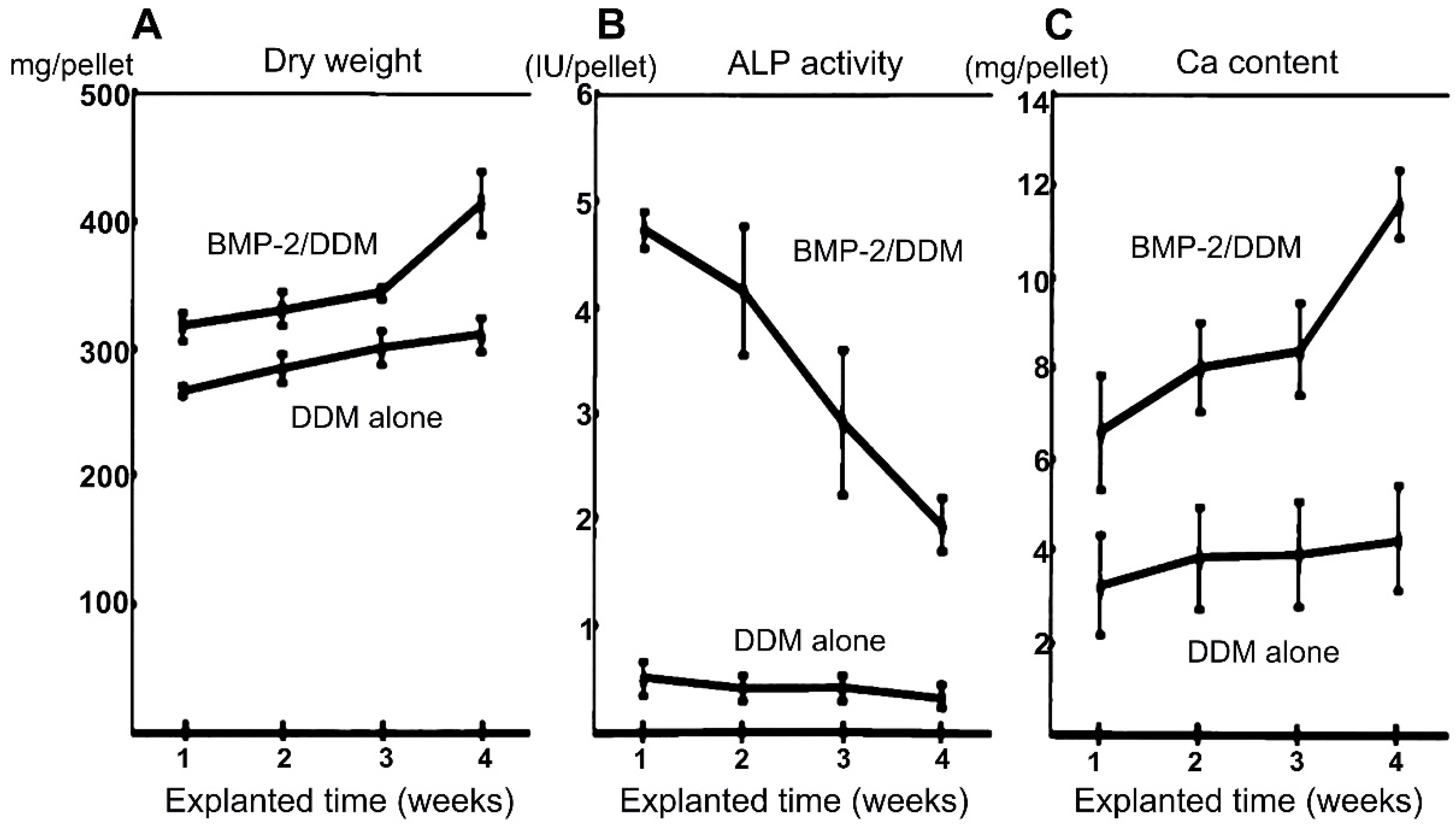
- Murata, M.; Sato, D.; Hino, J.; Akazawa, T.; Tazaki, J.; Ito, K.; Arisue, M. Acid-Insoluble Human Dentin as Carrier Material for Recombinant Human Bmp-2. J. Biomed. Mater. Res. A 2012, 100, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Kim, Y.K.; Park, Y.H.; Park, J.C.; Ku, J.K.; Um, I.W.; Kim, J.Y. Evaluation of the Healing Potential of Demineralized Dentin Matrix Fixed with Recombinant Human Bone Morphogenetic Protein-2 in Bone Grafts. Materials (Basel) 2017, 10, 1049. [Google Scholar] [CrossRef] [PubMed]
- Um, I.-W.; Kim, Y.-K.; Park, J.-C.; Lee, J.-H. Clinical Application of Autogenous Demineralized Dentin Matrix Loaded with Recombinant Human Bone Morphogenetic-2 for Socket Preservation: A Case Series. Clin. Implant Dent. Relat. Res. 2018. [Google Scholar] [CrossRef] [PubMed]
- Um, I.W.; Hwang, S.H.; Kim, Y.K.; Kim, M.Y.; Jun, S.H.; Ryu, J.J.; Jang, H.S. Demineralized Dentin Matrix Combined with Recombinant Human Bone Morphogenetic Protein-2 in Rabbit Calvarial Defects. J. Korean Assoc. Oral Maxillofac. Surg. 2016, 42, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Jung, G.-U.; Jeon, T.-H.; Kang, M.-H.; Um, I.-W.; Song, I.-S.; Ryu, J.-J.; Jun, S.-H. Volumetric, Radiographic, and Histologic Analyses of Demineralized Dentin Matrix Combined with Recombinant Human Bone Morphogenetic Protein-2 for Ridge Preservation: A Prospective Randomized Controlled Trial in Comparison with Xenograft. Appl. Sci. 2018, 8, 1288. [Google Scholar] [CrossRef]
- Bakopoulou, A.; Papachristou, E.; Bousnaki, M.; Hadjichristou, C.; Kontonasaki, E.; Theocharidou, A.; Papadopoulou, L.; Kantiranis, N.; Zachariadis, G.; Leyhausen, G.; et al. Human Treated Dentin Matrices Combined with Zn-Doped, Mg-Based Bioceramic Scaffolds and Human Dental Pulp Stem Cells Towards Targeted Dentin Regeneration. Dent. Mater. 2016, 32, e159–e175. [Google Scholar] [CrossRef] [PubMed]
- Ji, B.; Sheng, L.; Chen, G.; Guo, S.; Xie, L.; Yang, B.; Guo, W.; Tian, W. The Combination Use of Platelet-Rich Fibrin and Treated Dentin Matrix for Tooth Root Regeneration by Cell Homing. Tissue Eng. Part A 2015, 21, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Chen, J.; Yang, B.; Li, L.; Luo, X.; Zhang, X.; Feng, L.; Jiang, Z.; Yu, M.; Guo, W.; et al. Combination of Aligned Plga/Gelatin Electrospun Sheets, Native Dental Pulp Extracellular Matrix and Treated Dentin Matrix as Substrates for Tooth Root Regeneration. Biomaterials 2015, 52, 56–70. [Google Scholar] [CrossRef] [PubMed]
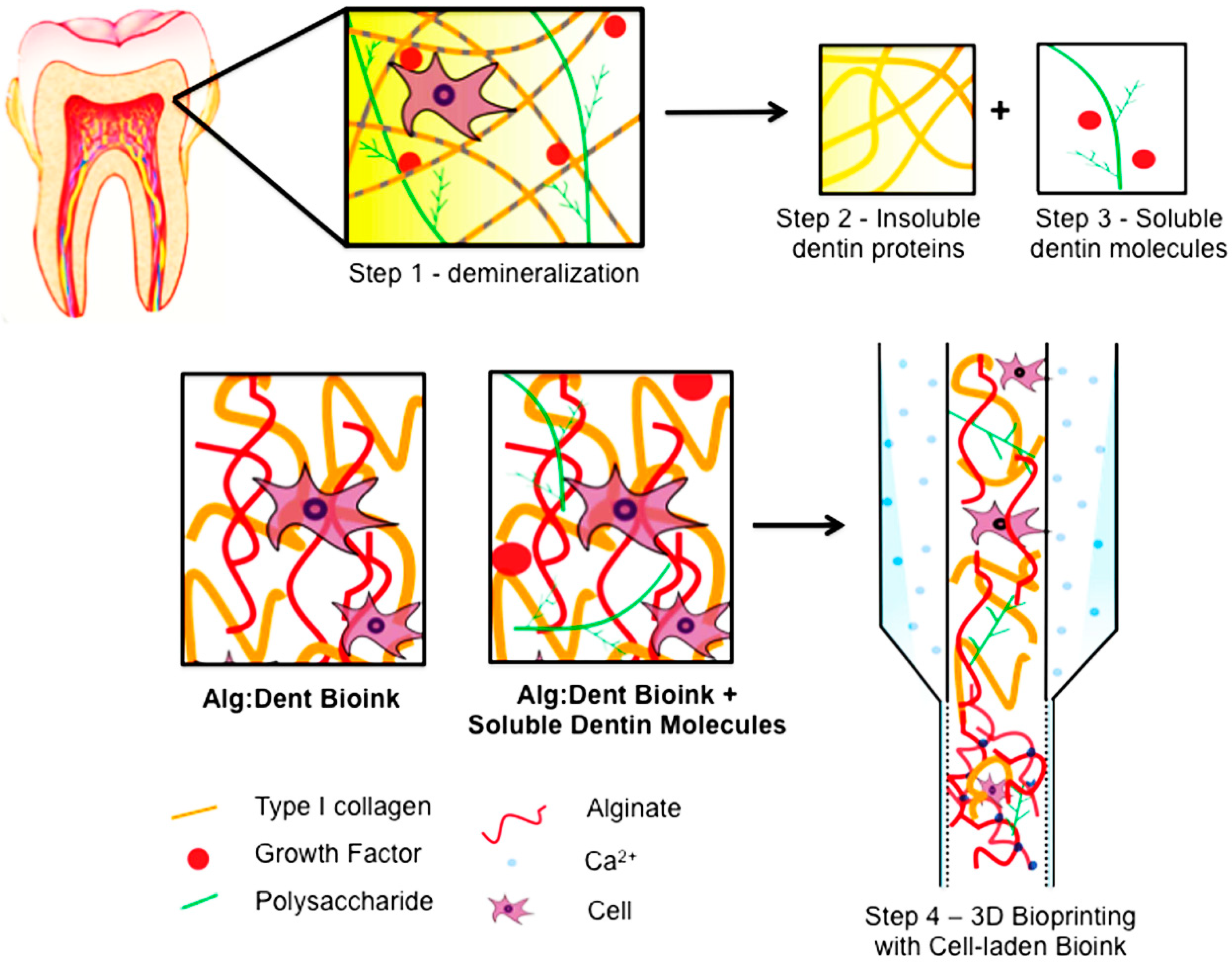
- Athirasala, A.; Tahayeri, A.; Thrivikraman, G.; Franca, C.M.; Monteiro, N.; Tran, V.; Ferracane, J.; Bertassoni, L.E. A Dentin-Derived Hydrogel Bioink for 3d Bioprinting of Cell Laden Scaffolds for Regenerative Dentistry. Biofabrication 2018, 10, 024101. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Growth Factor | TGF-β1 | VEGF | BMP-2 | IGF-1 | FGF | PDGF | BMP-4 | BMP-7 |
|---|---|---|---|---|---|---|---|---|
| ng/mg DDM | 15.6 ± 7.9 | 5.0 ± 2.4 | 6.2 ± 1.7 | 2.4 ± 1.3 | 5.5 ± 1.0 | 4.7 ± 1.5 | 0.12 ± 0.07 | 0.72 ± 0.03 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, X.; Qin, W.; Wang, P.; Wang, L.; Weir, M.D.; Reynolds, M.A.; Zhao, L.; Lin, Z.; Xu, H.H.K. Nano-Structured Demineralized Human Dentin Matrix to Enhance Bone and Dental Repair and Regeneration. Appl. Sci. 2019, 9, 1013. https://doi.org/10.3390/app9051013
Gao X, Qin W, Wang P, Wang L, Weir MD, Reynolds MA, Zhao L, Lin Z, Xu HHK. Nano-Structured Demineralized Human Dentin Matrix to Enhance Bone and Dental Repair and Regeneration. Applied Sciences. 2019; 9(5):1013. https://doi.org/10.3390/app9051013
Chicago/Turabian StyleGao, Xianling, Wei Qin, Ping Wang, Lin Wang, Michael D. Weir, Mark A. Reynolds, Liang Zhao, Zhengmei Lin, and Hockin H. K. Xu. 2019. "Nano-Structured Demineralized Human Dentin Matrix to Enhance Bone and Dental Repair and Regeneration" Applied Sciences 9, no. 5: 1013. https://doi.org/10.3390/app9051013