Hemodynamics and Wall Mechanics after Surgical Repair of Aortic Arch: Implication for Better Clinical Decisions



Abstract
:1. Introduction
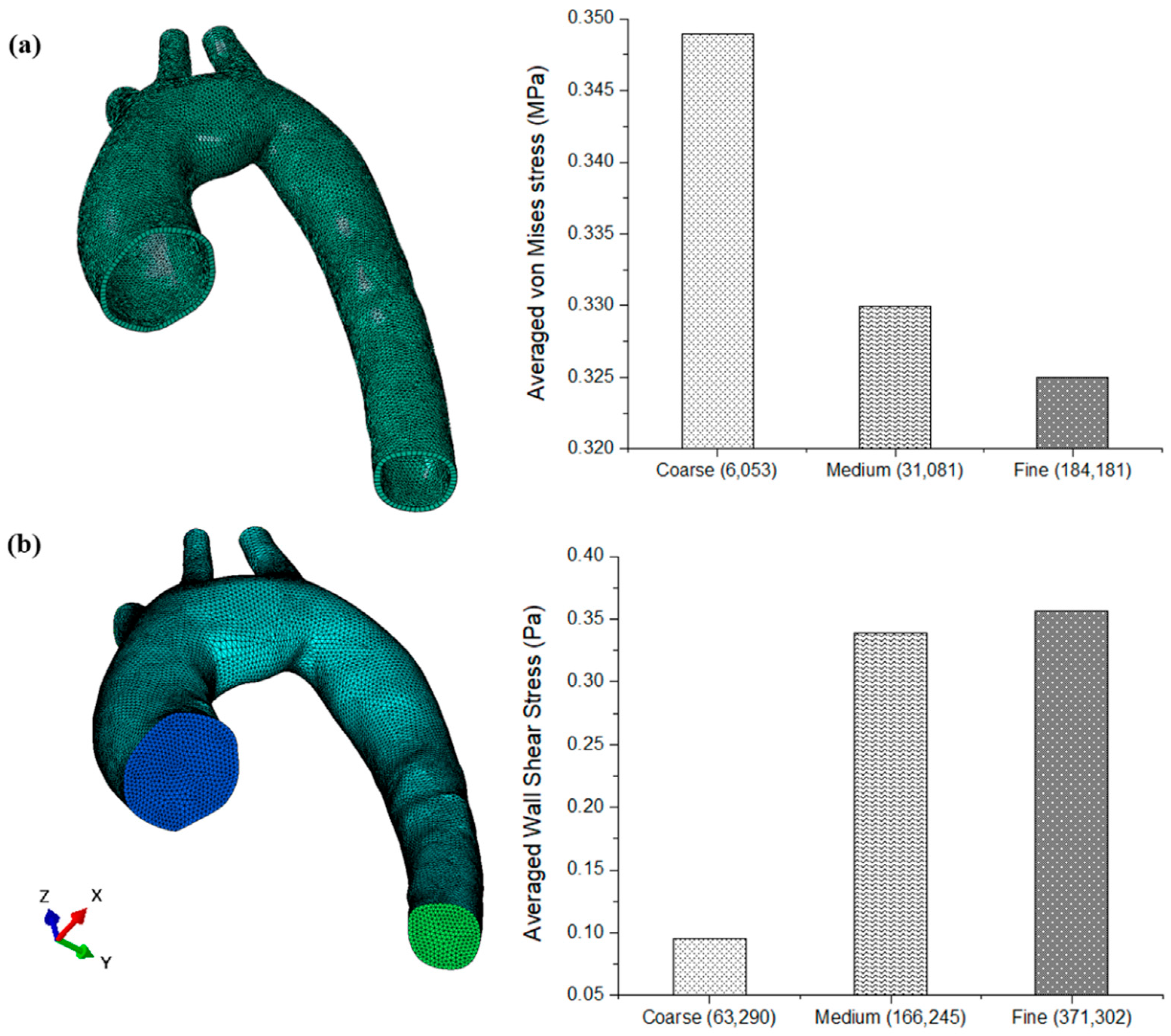
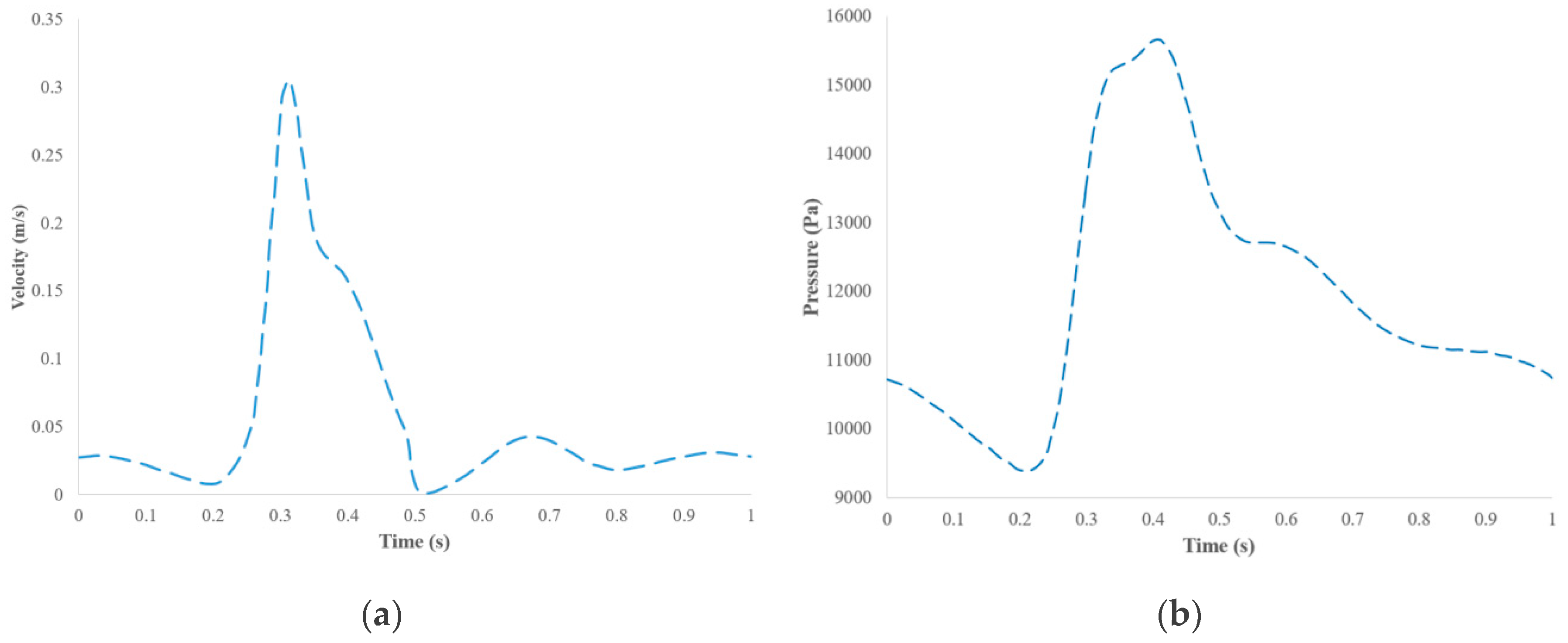
2. Materials and Methods
3. Results
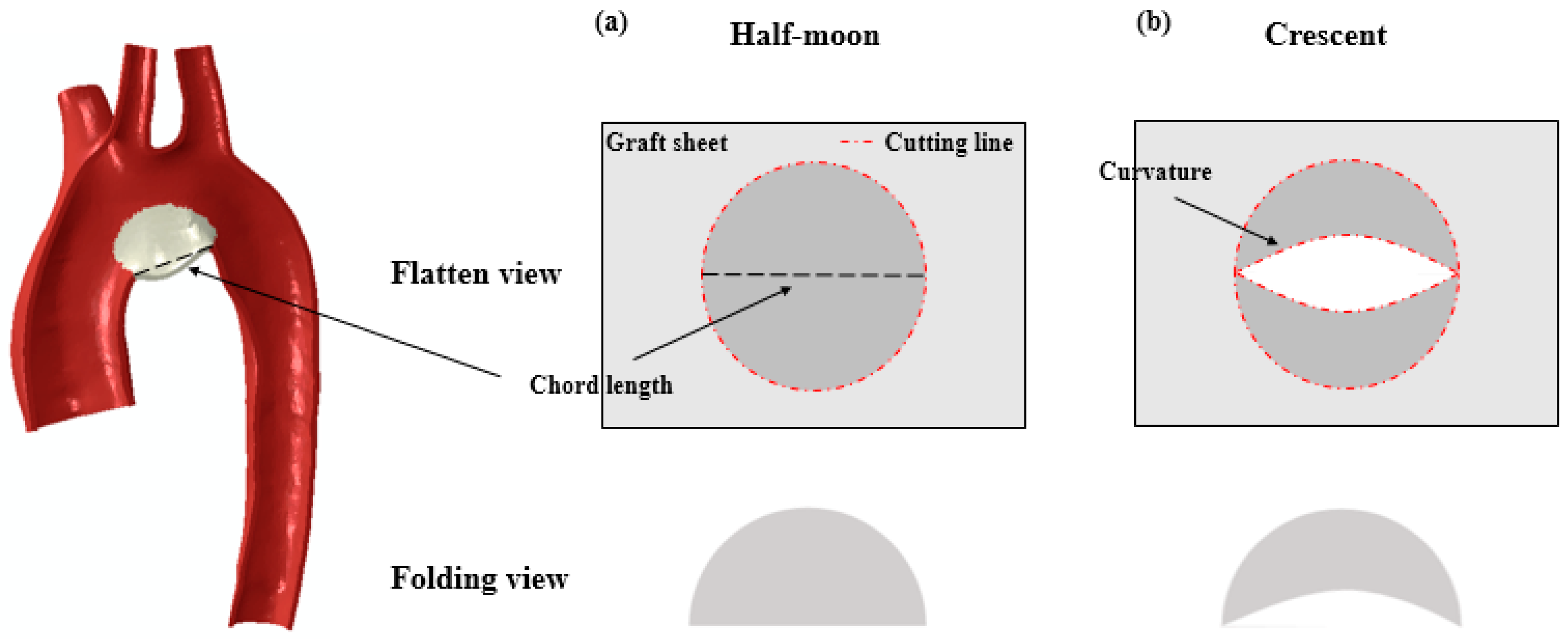
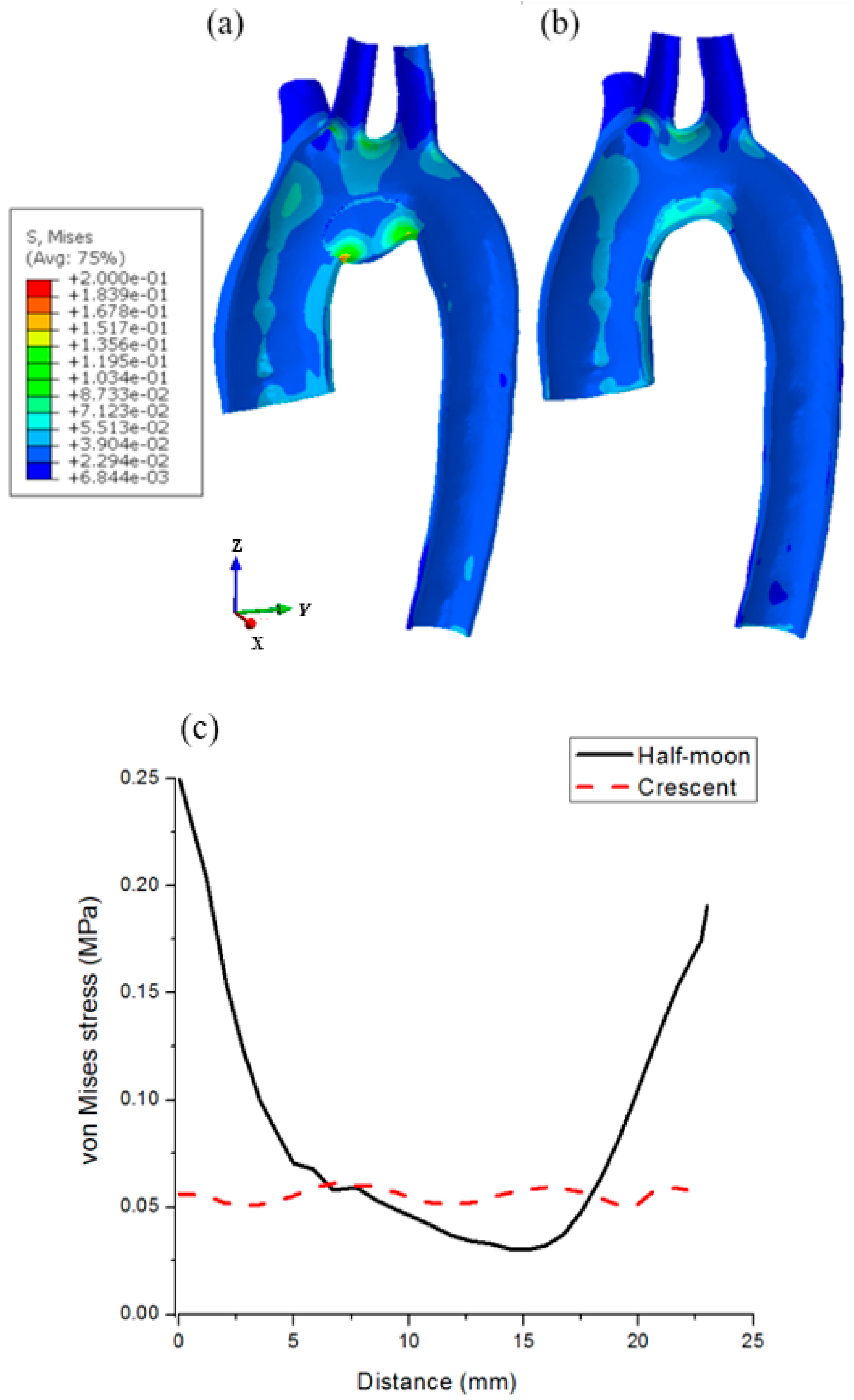
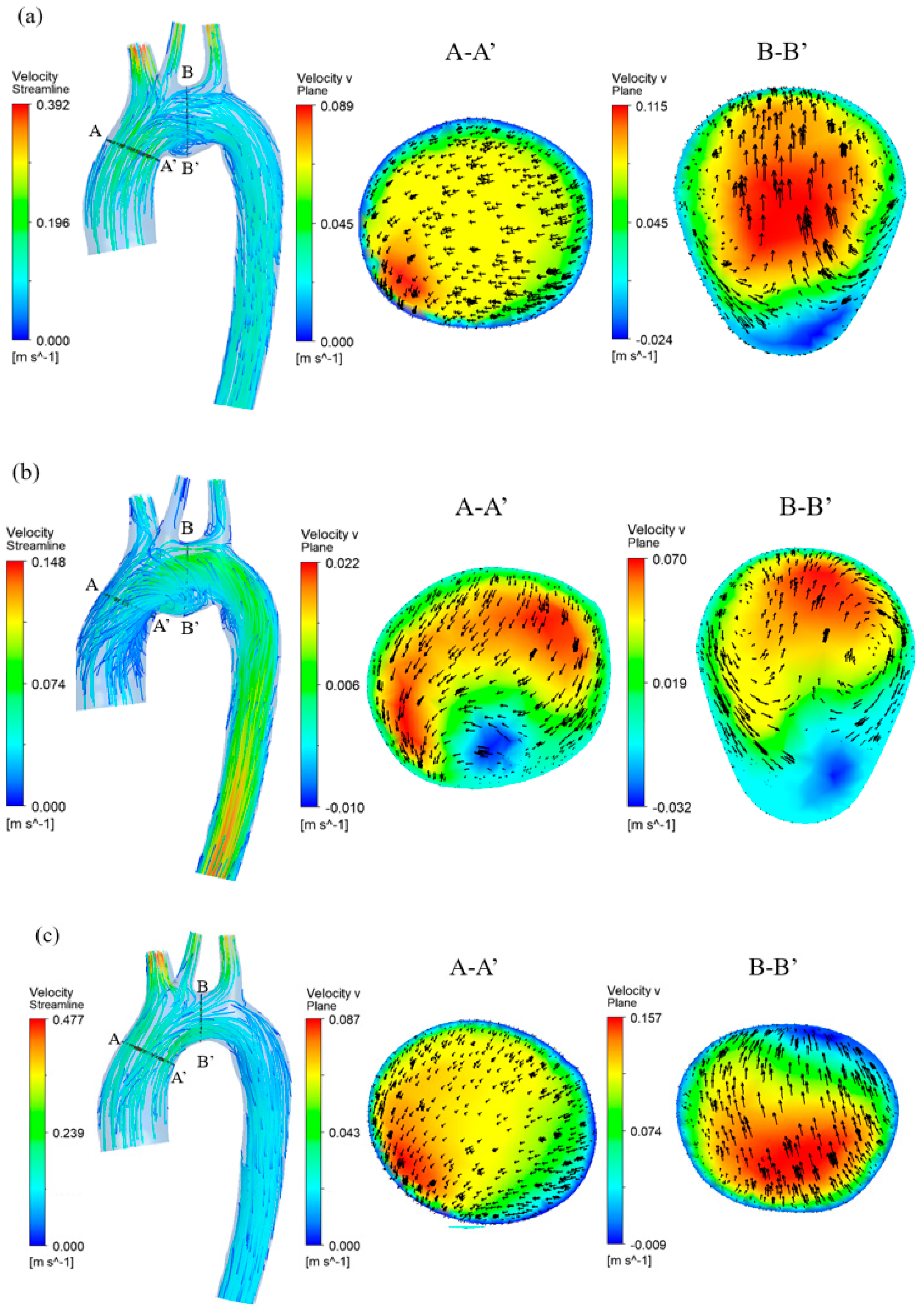
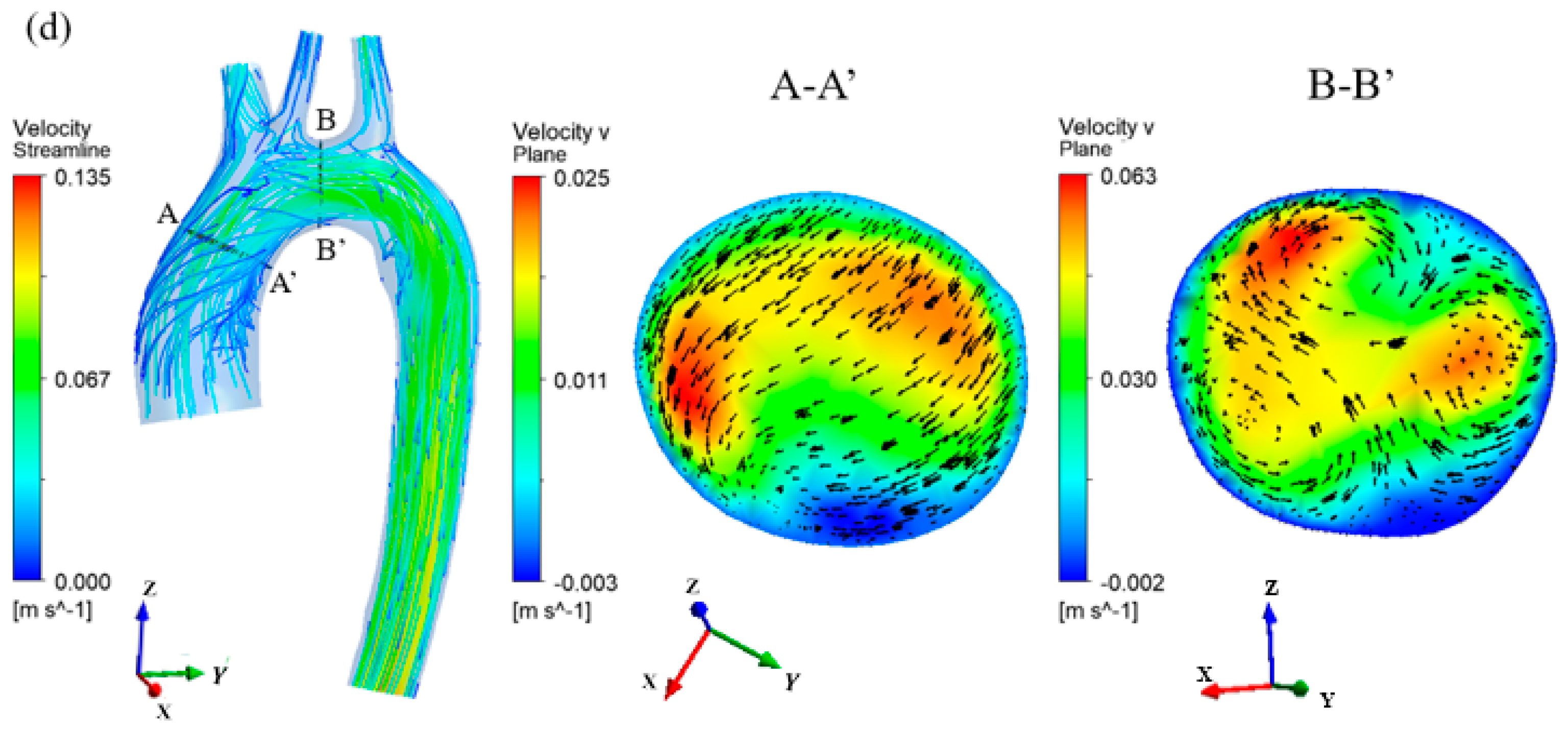
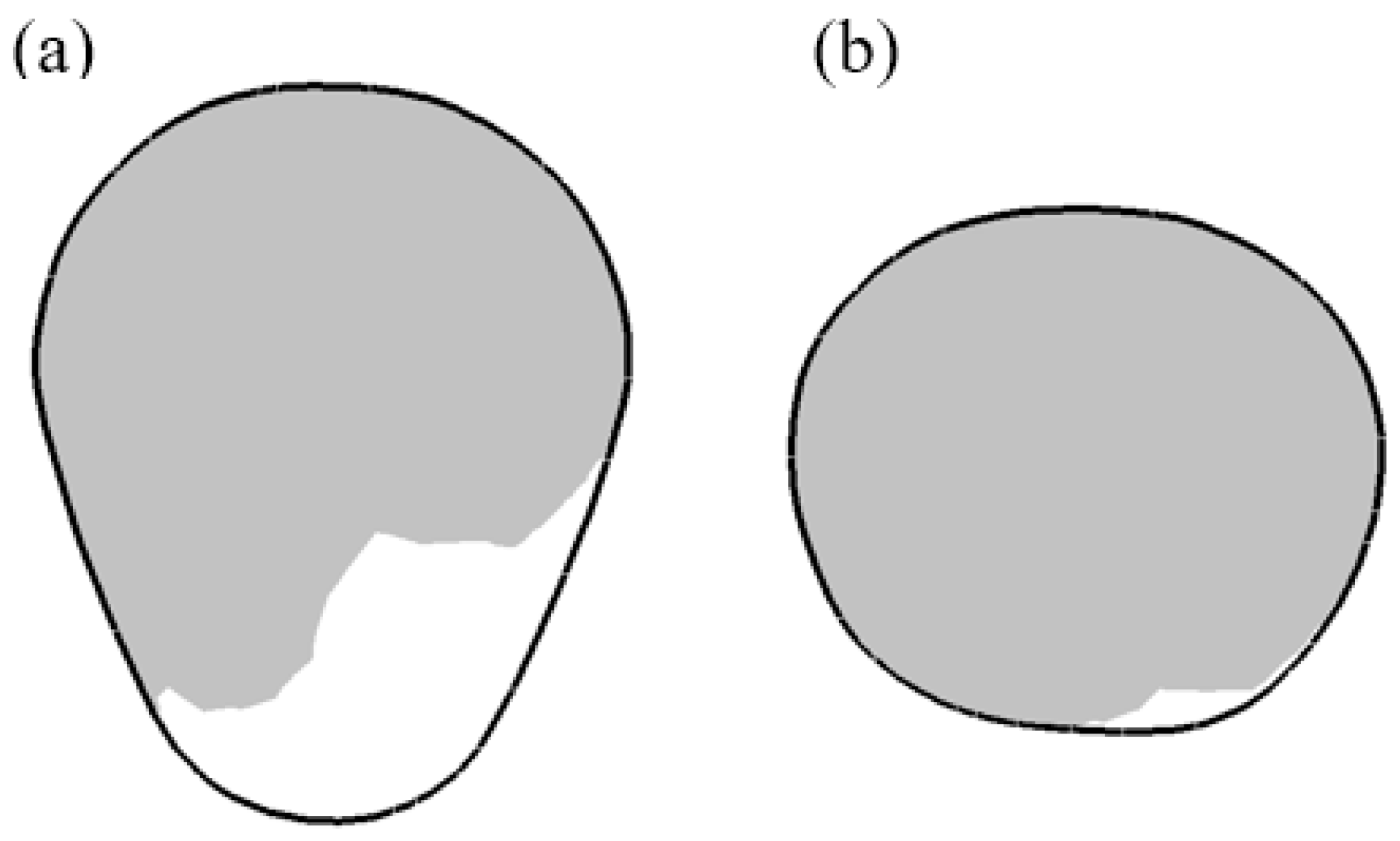
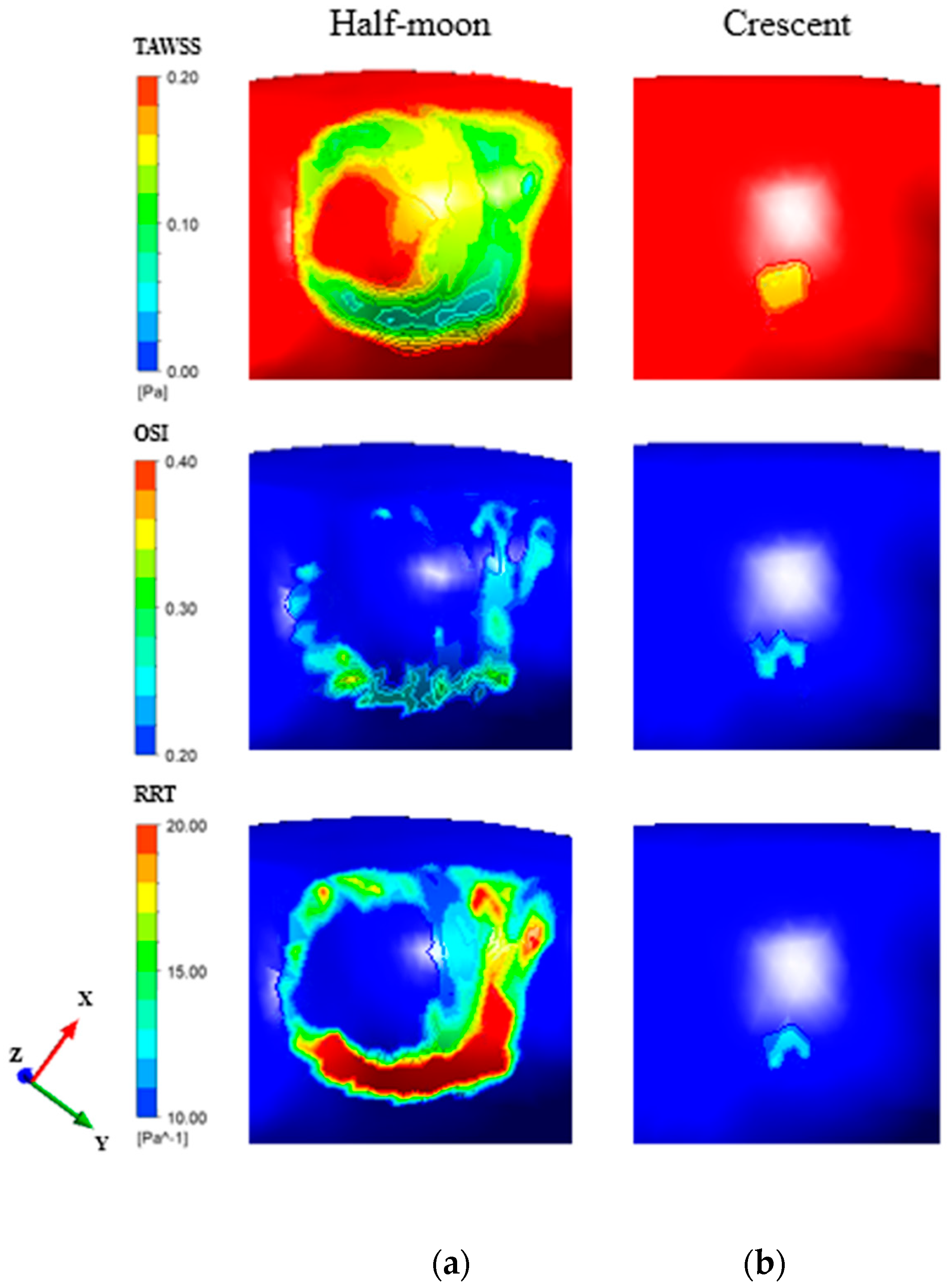
3.1. Influence of Graft Shapes
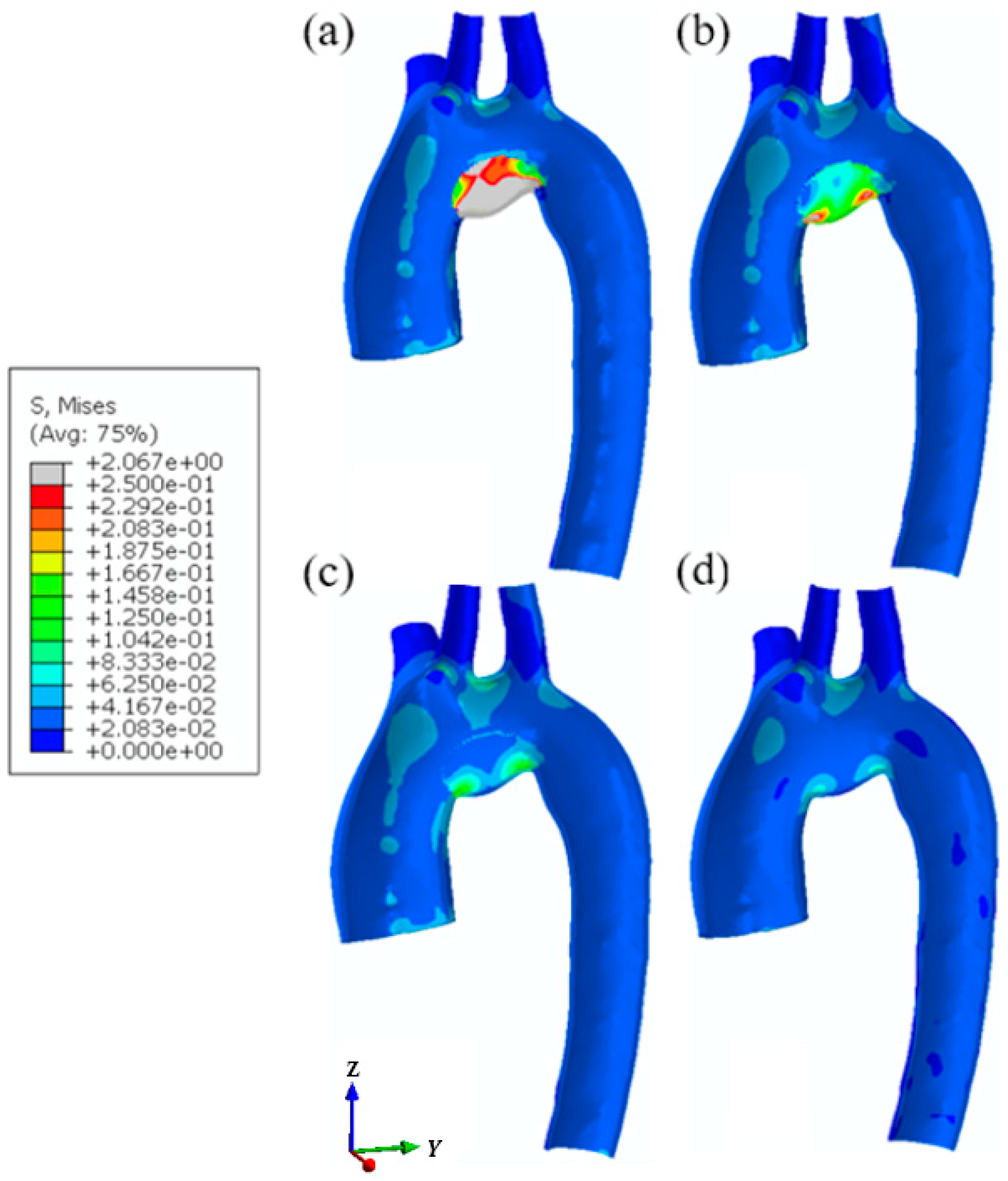
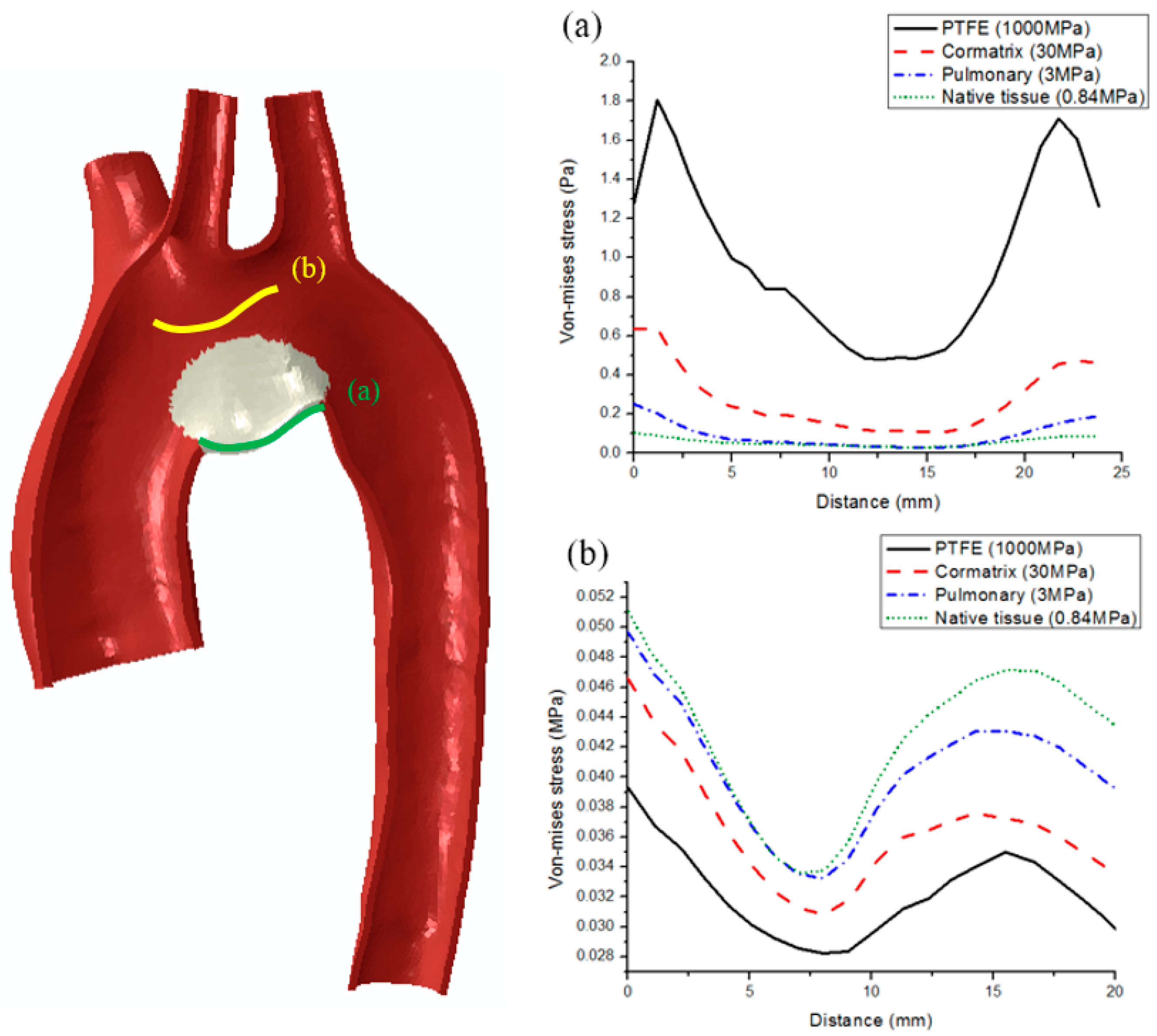
3.2. Influence of Graft Materials
4. Discussions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ringel, R.E.; Gauvreau, K.; Moses, H.; Jenkins, K.J.J.A.H.J. Coarctation of the Aorta Stent Trial (COAST): Study design and rationale. Am. Heart J. 2012, 164, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Keshavarz-Motamed, Z.; Garcia, J.; Maftoon, N.; Bedard, E.; Chetaille, P.; Kadem, L.J.J.O.B. A new approach for the evaluation of the severity of coarctation of the aorta using Doppler velocity index and effective orifice area: In vitro validation and clinical implications. J. Biomech. 2012, 45, 1239–1245. [Google Scholar] [CrossRef] [PubMed]
- Torok, R.D.; Campbell, M.J.; Fleming, G.A.; Hill, K.D. Coarctation of the aorta: Management from infancy to adulthood. World J. Cardiol. 2015, 7, 765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vergales, J.E.; Gangemi, J.J.; Rhueban, K.S.; Lim, D.S. Coarctation of the aorta-the current state of surgical and transcatheter therapies. Curr. Cardiol. Rev. 2013, 9, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Poirier, N.C.; van Arsdell, G.S.; Brindle, M.; Thyagarajan, G.K.; Coles, J.G.; Black, M.D.; Freedom, R.M.; Williams, W.G. Surgical treatment of aortic arch hypoplasia in infants and children with biventricular hearts. Ann. Thorac. Surg. 1999, 68, 2293–2297. [Google Scholar] [CrossRef]
- Boussel, L.; Rayz, V.; McCulloch, C.; Martin, A.; Acevedo-Bolton, G.; Lawton, M.; Higashida, R.; Smith, W.S.; Young, W.L.; Saloner, D. Aneurysm growth occurs at region of low wall shear stress: Patient-specific correlation of hemodynamics and growth in a longitudinal study. Stroke 2008, 39, 2997–3002. [Google Scholar] [CrossRef] [PubMed]
- Vardoulis, O.; Coppens, E.; Martin, B.; Reymond, P.; Tozzi, P.; Stergiopulos, N. Impact of aortic grafts on arterial pressure: A computational fluid dynamics study. Eur. J. Vasc. Endovasc. Surg. 2011, 42, 704–710. [Google Scholar] [CrossRef] [PubMed]
- Kannan, R.Y.; Salacinski, H.J.; Butler, P.E.; Hamilton, G.; Seifalian, A.M. Current status of prosthetic bypass grafts: A review. J. Biomed. Mater. Res. Part B Appl. Biomater. 2005, 74, 570–581. [Google Scholar] [CrossRef] [PubMed]
- Jaganathan, S.K.; Supriyanto, E.; Murugesan, S.; Balaji, A.; Asokan, M.K. Biomaterials in cardiovascular research: Applications and clinical implications. BioMed Res. Int. 2014, 45, 1239–1245. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Gao, Y.; Lu, B.; Jia, X.; Zhong, L.; Kassab, G.S.; Tan, W.; Huo, Y. Hemodynamics in coronary arterial tree of serial stenoses. PLoS ONE 2016, 11, e0163715. [Google Scholar] [CrossRef] [PubMed]
- Yanagawa, B.; Rao, V.; Yau, T.M.; Cusimano, R.J. Initial experience with intraventricular repair using CorMatrix extracellular matrix. Innovations 2013, 8, 348–352. [Google Scholar] [PubMed]
- Knyshov, G.V.; Sitar, L.L.; Glagola, M.D.; Atamanyuk, M.Y. Aortic aneurysms at the site of the repair of coarctation of the aorta: A review of 48 patients. Ann. Thorac. Surg. 1996, 61, 935–939. [Google Scholar] [CrossRef]
- Lee, S.-W.; Antiga, L.; Spence, J.D.; Steinman, D.A. Geometry of the carotid bifurcation predicts its exposure to disturbed flow. Stroke 2008, 39, 2341–2347. [Google Scholar] [CrossRef] [PubMed]
- Mori, D.; Yamaguchi, T. Computational fluid dynamics modeling and analysis of the effect of 3-D distortion of the human aortic arch. Comput. Methods Biomech. Biomed. Eng. 2002, 5, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Alberta, H.B.; Secor, J.L.; Smits, T.C.; Farber, M.A.; Jordan, W.D.; Matsumura, J.S. Differences in aortic arch radius of curvature, neck size, and taper in patients with traumatic and aortic disease. J. Surg. Res. 2013, 184, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Chiu, J.-J.; Chien, S. Effects of disturbed flow on vascular endothelium: Pathophysiological basis and clinical perspectives. Physiol. Rev. 2011, 91, 327–387. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Li, Y.-S.; Chien, S.J.A. Shear stress–initiated signaling and its regulation of endothelial function. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 2191–2198. [Google Scholar] [CrossRef] [PubMed]
- Roussin, R.; Belli, E.; Lacour-Gayet, F.; Godart, F.; Rey, C.; Bruniaux, J.; Planché, C.; Serraf, A. Aortic arch reconstruction with pulmonary autograft patch aortoplasty. J. Thorac. Cardiovasc. Surg. 2002, 123, 443–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.-K.; Chou, H.-P.; Guo, C.-Y.; Chang, H.-T.; Chang, Y.-Y.; Chen, I.-M.; Wu, M.-H.; Shih, C.-C. Interobserver and intraobserver variability in measuring the tortuosity of the thoracic aorta on computed tomography. J. Vasc. Surg. 2018, 68, 1183–1192. [Google Scholar] [CrossRef] [PubMed]
- Krüger, T.; Veseli, K.; Lausberg, H.; Vöhringer, L.; Schneider, W.; Schlensak, C.J.I.C.; Surgery, T. Regional and directional compliance of the healthy aorta: An ex vivo study in a porcine model. Interact. Cardiovasc. Thorac. Surg. 2016, 23, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Fung, Y.-C. Biomechanics: Mechanical Properties of Living Tissues; Springer Science & Business Media: Berlin, Germany, 2013. [Google Scholar]
- Giannakoulas, G.; Giannoglou, G.; Soulis, J.; Farmakis, T.; Papadopoulou, S.; Parcharidis, G.; Louridas, G. A computational model to predict aortic wall stresses in patients with systolic arterial hypertension. Med. Hypothes. 2005, 65, 1191–1195. [Google Scholar] [CrossRef] [PubMed]
- Azadani, A.N.; Chitsaz, S.; Matthews, P.B.; Jaussaud, N.; Leung, J.; Wisneski, A.; Ge, L.; Tseng, E.E. Biomechanical comparison of human pulmonary and aortic roots. Eur. J. Cardio-Thorac. Surg. 2012, 41, 1111–1116. [Google Scholar] [CrossRef] [PubMed]
- Rae, P.; Dattelbaum, D. The properties of poly (tetrafluoroethylene)(PTFE) in compression. Polymer 2004, 45, 7615–7625. [Google Scholar] [CrossRef]
- Scully, B.B.; Fan, C.; Grigoryan, B.; Jacot, J.G.; Vick, G.; Kim, J.J.; Fraser, C.D.; Grande-Allen, K.J.; Morales, D.L. Remodeling of ECM patch into functional myocardium in an ovine model: A pilot study. J. Biomed. Mater. Res. Part B Appl. Biomater. 2016, 104, 1713–1720. [Google Scholar] [CrossRef] [PubMed]
- Hoerstrup, S.P.; Kadner, A.; Breymann, C.; Maurus, C.F.; Guenter, C.I.; Sodian, R.; Visjager, J.F.; Zund, G.; Turina, M.I. Living, autologous pulmonary artery conduits tissue engineered from human umbilical cord cells. Ann. Thorac. Surg. 2002, 74, 46–52. [Google Scholar] [CrossRef]
- Donea, J.; Huerta, A.; Ponthot, J.P.; Rodríguez-Ferran, A. Arbitrary L agrangian–E ulerian Methods. In Encyclopedia of Computational Mechanics, 2nd ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2017; pp. 1–23. [Google Scholar] [CrossRef]
- Ahrem, R.; Post, P.; Steckel, B.; Wolf, K. MpCCI: A tool for coupling CFD with other disciplines. In Proceedings of the Fifth World Conference in Applied Fluid Dynamics, CFD-Efficiency and Economic Benefit in Manufacturing, Freiburg, Germany, 17–21 June 2001. [Google Scholar]
- Fraunhofer, S. MpCCI Documentation; Fraunhofer Institute for Algorithms and Scientific Computing SCAI, Germany: Sankt Augustin, Germany, 2008. [Google Scholar]
- Lin, S.; Han, X.; Bi, Y.; Ju, S.; Gu, L. Fluid-Structure Interaction in Abdominal Aortic Aneurysm: Effect of Modeling Techniques. BioMed Res. Int. 2017. [Google Scholar] [CrossRef] [PubMed]
- Dassault Systèmes SIMULIA Corp. ABAQUS Theory Manual; 2009 Version; Dassault Systèmes SIMULIA Corp.: Providence, RI, USA, 2009. [Google Scholar]
- Cattermole, G.N.; Leung, P.M.; Ho, G.Y.; Lau, P.W.; Chan, C.P.; Chan, S.S.; Smith, B.E.; Graham, C.A.; Rainer, T.H. The normal ranges of cardiovascular parameters measured using the ultrasonic cardiac output monitor. Physiol. Rep. 2017. [Google Scholar] [CrossRef] [PubMed]
- Calamandrei, M.; Mirabile, L.; Muschetta, S.; Gensini, G.F.; de Simone, L.; Romano, S.M. Assessment of cardiac output in children: A comparison between the pressure recording analytical method and Doppler echocardiography. Pediatr. Crit. Care Med. 2008, 9, 310–312. [Google Scholar] [CrossRef] [PubMed]
- Benim, A.; Nahavandi, A.; Assmann, A.; Schubert, D.; Feindt, P.; Suh, S. Simulation of blood flow in human aorta with emphasis on outlet boundary conditions. Appl. Math. Model. 2011, 35, 3175–3188. [Google Scholar] [CrossRef]
- Zeng, X.; Levine, R.A.; Hua, L.; Morris, E.L.; Kang, Y.; Flaherty, M.; Morgan, N.V.; Hung, J. Diagnostic Value of Vena Contracta Area in the Quantification of Mitral Regurgitation Severity by Color Doppler 3D EchocardiographyClinical Perspective. Circ. Cardiovasc. Imaging 2011, 4, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Gao, B.; Gu, K.; Chang, Y.; Xu, J. The study on hemodynamic effect of varied support models of BJUT-II VAD on coronary artery: A primary CFD study. ASAIO J. 2014, 60, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Tsou, J.K.; Liu, J.; Barakat, A.I.; Insana, M.F. Role of ultrasonic shear rate estimation errors in assessing inflammatory response and vascular risk. Ultrasound Med. Biol. 2008, 34, 963–972. [Google Scholar] [CrossRef] [PubMed]
- Castro, M.A. Understanding the role of hemodynamics in the initiation, progression, rupture, and treatment outcome of cerebral aneurysm from medical image-based computational studies. ISRN Radiol. 2013. [Google Scholar] [CrossRef]
- Itatani, K.; Miyaji, K.; Qian, Y.; Liu, J.L.; Miyakoshi, T.; Murakami, A.; Ono, M.; Umezu, M. Influence of surgical arch reconstruction methods on single ventricle workload in the Norwood procedure. J. Thorac. Cardiovasc. Surg. 2012, 144, 130–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruse, J.L.; Khushnood, A.; McLeod, K.; Biglino, G.; Sermesant, M.; Pennec, X.; Taylor, A.M.; Hsia, T.-Y.; Schievano, S.; Modeling of Congenital Hearts Alliance Collaborative Group. How successful is successful? Aortic arch shape after successful aortic coarctation repair correlates with left ventricular function. J. Thorac. Cardiovasc. Surg. 2017, 153, 418–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomita, H.; Zhilicheva, S.; Kim, S.; Maeda, N. Aortic Arch Curvature and Atherosclerosis Have Overlapping Quantitative Trait Loci in a Cross Between 129S6/SvEvTac and C57BL/6J Apolipoprotein E–Null Mice. Circ. Res. 2010, 106, 1052–1060. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Yang, J.-H.; Jun, T.-G.; Cho, Y.H.; Kang, I.-S.; Huh, J.; Song, J. Augmentation of the Lesser Curvature With an Autologous Vascular Patch in Complex Aortic Coarctation and Interruption. Ann. Thorac. Surg. 2016, 101, 2309–2314. [Google Scholar] [CrossRef] [PubMed]
- Kasiri, S.; Taylor, D. A critical distance study of stress concentrations in bone. J. Biomech. 2008, 41, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Broom, N. The stress/strain and fatigue behaviour of glutaraldehyde preserved heart-valve tissue. J. Biomech. 1977, 10, 707–724. [Google Scholar] [CrossRef]
- Broom, N.D. An ‘in vitro’study of mechanical fatigue in glutaraldehyde-treated porcine aortic valve tissue. Biomaterials 1980, 1, 3–8. [Google Scholar] [CrossRef]
- Soslowsky, L.; Thomopoulos, S.; Tun, S.; Flanagan, C.; Keefer, C.; Mastaw, J.; Carpenter, J. Neer Award 1999: Overuse activity injures the supraspinatus tendon in an animal model: A histologic and biomechanical study. J. Shoulder Elbow Surg. 2000, 9, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.J.; Smith, F.W. Stenosis hemodynamics: From physical principles to clinical indices. J. Vet. Intern. Med. 2002, 16, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Singh, C.; Wang, X.; Morsi, Y.; Wong, C. Importance of stent-graft design for aortic arch aneurysm repair. AIMS Bioeng. 2017, 4, 133. [Google Scholar] [CrossRef]
- Qin, F.; Dardik, H.; Pangilinan, A.; Robinson, J.; Chuy, J.; Wengerter, K. Remodeling and suppression of intimal hyperplasia of vascular grafts with a distal arteriovenous fistula in a rat model. J. Vasc. Surg. 2001, 34, 701–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, C.; Sun, W. Fatigue damage of collagenous tissues: Experiment, modeling and simulation studies. J. Long-Term Effects Med. Implants 2015, 25. [Google Scholar] [CrossRef]
- Sacks, M.S.; Smith, D.B. Effects of accelerated testing on porcine bioprosthetic heart valve fiber architecture. Biomaterials 1998, 19, 1027–1036. [Google Scholar] [CrossRef]
- Gu, L.; Kasavajhala, A.R.M.; Lang, H.; Hammel, J.M. Numerical and experimental investigation of vascular suture closure. Biomed. Eng. Lett. 2012, 2, 46–51. [Google Scholar] [CrossRef]
- Lee, P.; Carlson, B.E.; Chesler, N.; Olufsen, M.S.; Qureshi, M.U.; Smith, N.P.; Sochi, T.; Beard, D.A. Heterogeneous mechanics of the mouse pulmonary arterial network. Biomech. Model. Mechanobiol. 2016, 15, 1245–1261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madhavan, S.; Kemmerling, E.M.C. The effect of inlet and outlet boundary conditions in image-based CFD modeling of aortic flow. Biomed. Eng. Online 2018, 17, 66. [Google Scholar] [CrossRef] [PubMed]
- Ohyama, Y.; Ambale-Venkatesh, B.; Noda, C.; Chugh, A.R.; Teixido-Tura, G.; Kim, J.-Y.; Donekal, S.; Yoneyama, K.; Gjesdal, O.; Redheuil, A. Association of aortic stiffness with left ventricular remodeling and reduced left ventricular function measured by magnetic resonance imaging: The Multi-Ethnic Study of Atherosclerosis. Circ. Cardiovasc. Imaging 2016, 9, e004426. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A-A′ | B-B′ | Centerline Angle | |
|---|---|---|---|
| Half-moon | 429.3 | 444.1 | 155.85° |
| Crescent | 431.4 | 335.3 | 139.74° |
| (kg/s) at 0.4 s | (kg/s) at 0.6 s | |||||
|---|---|---|---|---|---|---|
| Half-moon (A-A′) | 454.8 | 437.7 | 0.236 | 0.073 | 0.08592 | 0.01905 |
| Crescent (A-A′) | 480.4 | 464.4 | 0.237 | 0.070 | 0.09555 | 0.02070 |
| Half-moon (B-B′) | 484.1 | 461.0 | 0.170 | 0.092 | 0.04926 | 0.01735 |
| Crescent (B-B′) | 367.0 | 354.4 | 0.224 | 0.075 | 0.05090 | 0.01771 |
| Area () at 0.6 s | ||||
|---|---|---|---|---|
| PTFE | 447.5 | 437.5 | 0.1894 | 0.0894 |
| Cormatrix | 466.2 | 448.9 | 0.1811 | 0.0916 |
| Pulmonary | 484.1 | 461.0 | 0.1701 | 0.0924 |
| Native tissue | 510.3 | 478.0 | 0.1622 | 0.0934 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ju, S.; Abdullah, I.; Lin, S.; Gu, L. Hemodynamics and Wall Mechanics after Surgical Repair of Aortic Arch: Implication for Better Clinical Decisions. Appl. Sci. 2019, 9, 807. https://doi.org/10.3390/app9040807
Ju S, Abdullah I, Lin S, Gu L. Hemodynamics and Wall Mechanics after Surgical Repair of Aortic Arch: Implication for Better Clinical Decisions. Applied Sciences. 2019; 9(4):807. https://doi.org/10.3390/app9040807
Chicago/Turabian StyleJu, Siyeong, Ibrahim Abdullah, Shengmao Lin, and Linxia Gu. 2019. "Hemodynamics and Wall Mechanics after Surgical Repair of Aortic Arch: Implication for Better Clinical Decisions" Applied Sciences 9, no. 4: 807. https://doi.org/10.3390/app9040807