

Management of Acute Life-Threatening Asthma Exacerbations in the Intensive Care Unit

Abstract
:1. Introduction
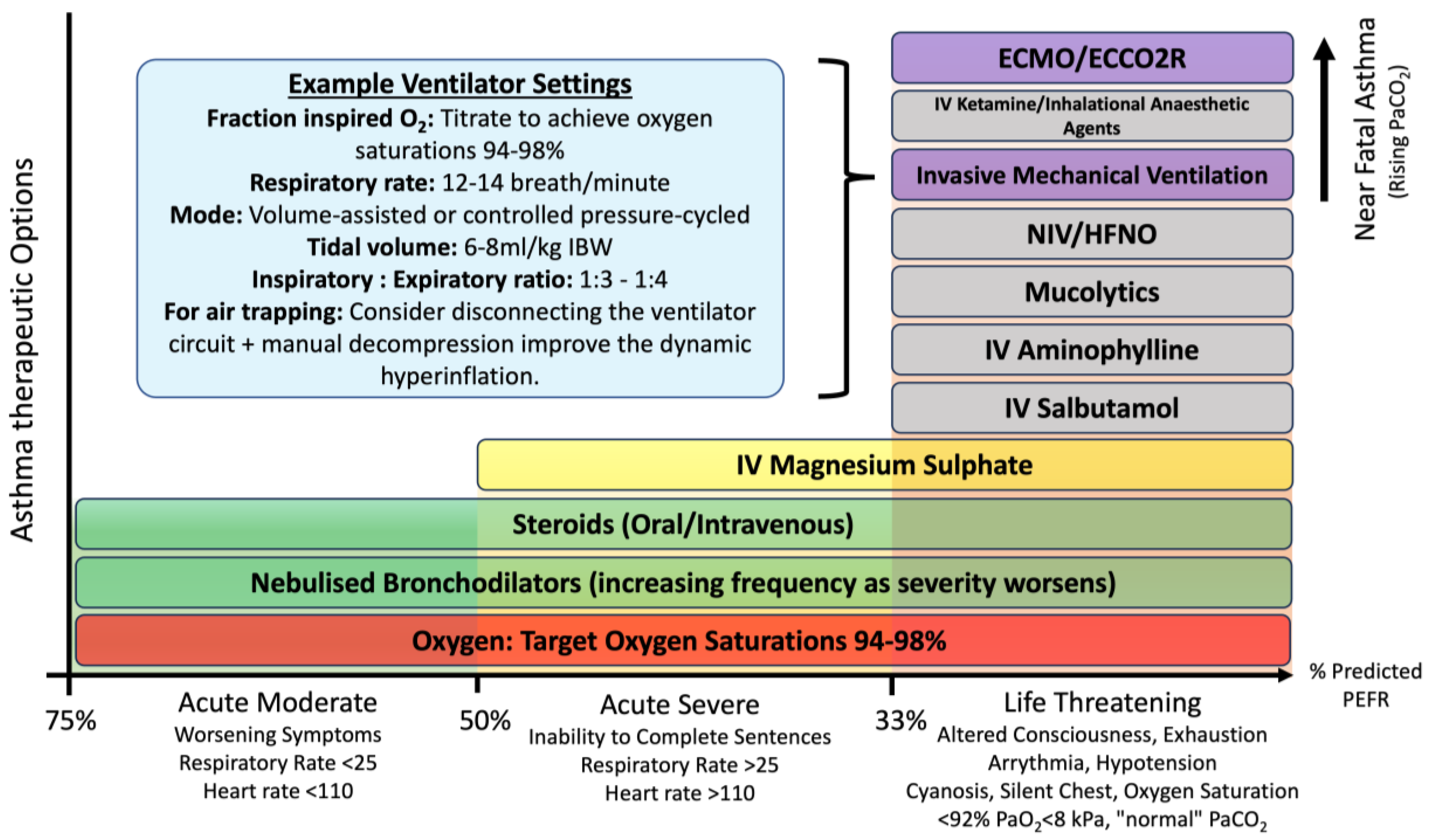
2. Classifications of Asthma Severity
3. Management of Acute Asthma Exacerbation
3.1. Oxygen Therapy and Targets
3.2. Nebulised Bronchodilators
3.3. Systemic Corticosteroids
3.4. Magnesium Sulphate
3.5. Intravenous Aminophylline
3.6. Intravenous Salbutamol
4. Acute Life-Threatening Asthma Advanced Management in the ICU
4.1. High-Flow Nasal Oxygen (HFNO)
4.2. Non-Invasive Ventilation (NIV)
4.3. Intubation
4.4. Mechanical Ventilation
4.5. Anaesthetic Agents
4.5.1. Ketamine
4.5.2. Inhalational Anaesthetic Agents
4.6. Extracorporeal CO2 Removal (ECCO2R)
4.7. ECMO
4.8. Mucolytics
4.8.1. Nebulised Heparin
4.8.2. Recombinant Human Deoxyribonuclease (rhDNase/Dornase Alfa)
4.9. Heliox
Limitations of This Review
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2019 Diseases and Injuries Collaborators. Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- Nunes, C.; Pereira, A.M.; Morais-Almeida, M. Asthma Costs and Social Impact. Asthma Res. Pract. 2017, 3, 1. [Google Scholar] [CrossRef] [PubMed]
- Louie, S.; Morrissey, B.M.; Kenyon, N.J.; Albertson, T.E.; Avdalovic, M. The Critically Ill Asthmatic—From ICU to Discharge. Clin. Rev. Allergy Immunol. 2012, 43, 30–44. [Google Scholar] [CrossRef] [PubMed]
- Office for Health Improvement and Disparities. Public Health Profiles. Available online: https://fingertips.phe.org.uk/search/asthma (accessed on 5 December 2023).
- Pendergraft, T.B.; Stanford, R.H.; Beasley, R.; Stempel, D.A.; Roberts, C.; McLaughlin, T. Rates and characteristics of intensive care unit admissions and intubations among asthma-related hospitalizations. Ann. Allergy Asthma Immunol. 2004, 93, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Stow, P.J.; Pilcher, D.; Wilson, J.; George, C.; Bailey, M.; Higlett, T.; Bellomo, R.; Hart, G.K.; Australian & New Zealand Intensive Care Society Adult Patient Database Management Committee. Improved outcomes from acute severe asthma in Australian intensive care units (1996–2003). Thorax 2007, 62, 842–847. [Google Scholar] [CrossRef] [PubMed]
- Nanchal, R.; Kumar, G.; Majumdar, T.; Taneja, A.; Patel, J.; Dagar, G.; Jacobs, E.R.; Whittle, J. Utilization of mechanical ventilation for asthma exacerbations: Analysis of a national database. Respir. Care 2014, 59, 644–653. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.; Keogh, B.; Chung, K.F.; Ayres, J.G.; Harrison, D.A.; Goldfrad, C.; Brady, A.R.; Rowan, K. Characteristics and outcome for admissions to adult, general critical care units with acute severe asthma: A secondary analysis of the ICNARC Case Mix Programme Database. Crit. Care 2004, 8, R112–R121. [Google Scholar] [CrossRef]
- Gibbison, B.; Griggs, K.; Mukherjee, M.; Sheikh, A. Ten years of asthma admissions to adult critical care units in England and Wales. BMJ Open 2013, 3, e003420. [Google Scholar] [CrossRef]
- BTS/SIGN British Guideline on the Management of Asthma. Available online: https://www.brit-thoracic.org.uk/quality-improvement/guidelines/asthma/ (accessed on 5 December 2023).
- Global Initiative for Asthma. Available online: https://ginasthma.org/gina-reports/ (accessed on 8 January 2024).
- Holguin, F.; Cardet, J.C.; Chung, K.F.; Diver, S.; Ferreira, D.S.; Fitzpatrick, A.; Gaga, M.; Kellermeyer, L.; Khurana, S.; Knight, S.; et al. Management of Severe Asthma: A European Respiratory Society/American Thoracic Society Guideline. Eur. Respir. J. 2020, 55, 1900588. [Google Scholar] [CrossRef]
- O’Driscoll, B.R.; Howard, L.S.; Earis, J.; Mak, V. British Thoracic Society Guideline for oxygen use in adults in healthcare and emergency settings. BMJ Open Respir. Res. 2017, 4, e000170. [Google Scholar] [CrossRef]
- Martin, D.S.; Grocott, M.P. Oxygen therapy in critical illness: Precise control of arterial oxygenation and permissive hypoxemia. Crit. Care Med. 2013, 41, 423–432. [Google Scholar] [CrossRef] [PubMed]
- Perrin, K.; Wijesinghe, M.; Healy, B.; Wadsworth, K.; Bowditch, R.; Bibby, S.; Baker, T.; Weatherall, M.; Beasley, R. Randomised controlled trial of high concentration versus titrated oxygen therapy in severe exacerbations of asthma. Thorax 2011, 66, 937–941. [Google Scholar] [CrossRef] [PubMed]
- Chu, D.; Kim, L.; Young, P.; Zamiri, N.; Almenawer, S.; Jaeschke, R.; Szczeklik, W.; Schünemann, H.; Neary, J.; Alhazzani, W. Mortality and morbidity in acutely ill adults treated with liberal versus conservative oxygen therapy (IOTA): A systematic review and meta-analysis. Lancet 2018, 391, 1693–1705. [Google Scholar] [CrossRef] [PubMed]
- Girardis, M.; de Man, A.M.E.; Singer, M. Trials on Oxygen Targets in the Critically Ill Patients: Do They Change Our Knowledge and Practice? Intensive Care Med. 2023, 49, 559–562. [Google Scholar] [CrossRef]
- Singer, M.; Young, P.J.; Laffey, J.G.; Asfar, P.; Taccone, F.S.; Skrifvars, M.B.; Meyhoff, C.S.; Radermacher, P. Dangers of Hyperoxia. Crit. Care 2021, 25, 440. [Google Scholar] [CrossRef]
- Wetterslev, J.; Meyhoff, C.S.; Jørgensen, L.N.; Gluud, C.; Lindschou, J.; Rasmussen, L.S. The effects of high perioperative inspiratory oxygen fraction for adult surgical patients. Cochrane Database Syst. Rev. 2015, 6, CD008884. [Google Scholar] [CrossRef]
- Lass Klitgaard, T.; Schjørring, O.; Nielsen, F.; Meyhoff, C.; Perner, A.; Wetterslev, J.; Rasmussen, B.; Barbateskovic, M. Higher versus lower fractions of inspired oxygen or targets of arterial oxygenation for adults admitted to the intensive care unit. Cochrane Database Syst. Rev. 2023, 9, CD012631. [Google Scholar]
- UK-ROX. Intensive Care Unit Randomised Trial Comparing Two Approaches to OXygen Therapy. Available online: https://www.icnarc.org/Our-Research/Studies/Uk-Rox/About (accessed on 5 December 2023).
- Mega-ROX. In: ANZICS [Internet]. Available online: https://www.anzics.com.au/current-active-endorsed-research/mega-rox/ (accessed on 5 December 2023).
- Johnson, M. Beta2-adrenoceptors: Mechanisms of action of beta2-agonists. Paediatr. Respir. Rev. 2001, 2, 57–62. [Google Scholar] [CrossRef]
- Sears, M.R. Adverse Effects of β-Agonists. J. Allergy Clin. Immunol. 2002, 110, S322–S328. [Google Scholar] [CrossRef]
- Medical Research, C. Controlled trial of effects of cortisone acetate in status asthmaticus. Lancet 1956, 2, 803–806. [Google Scholar]
- Rowe, B.H.; Spooner, C.; Ducharme, F.M.; Bretzlaff, J.A.; Bota, G.W. Early emergency department treatment of acute asthma with systemic corticosteroids. Cochrane Database Syst. Rev. 2001, 1, CD002178. [Google Scholar] [CrossRef] [PubMed]
- Rowe, B.H.; Edmonds, M.L.; Spooner, C.H.; Diner, B.; Camargo, C.A. Corticosteroid Therapy for Acute Asthma. Respir. Med. 2004, 98, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Cunnington, D.; Smith, N.; Steed, K.; Rosengarten, P.; Kelly, A.M.; Teichtahl, H. Oral versus intravenous corticosteroids in adults hospitalised with acute asthma. Pulm. Pharmacol. Ther. 2005, 18, 207–212. [Google Scholar] [CrossRef]
- Harrison, B.; Hart, G.; Ali, N.; Stokes, T.; Vaughan, D.; Robinson, A. Need for intravenous hydrocortisone in addition to oral prednisolone in patients admitted to hospital with severe asthma without ventilatory failure. Lancet 1986, 1, 181–184. [Google Scholar] [CrossRef]
- Ratto, D.; Alfaro, C.; Sipsey, J.; Glovsky, M.M.; Sharma, O.P. Are intravenous corticosteroids required in status asthmaticus? JAMA 1988, 260, 527–529. [Google Scholar] [CrossRef]
- Becker, J.M.; Arora, A.; Scarfone, R.J.; Spector, N.D.; Fontana-Penn, M.E.; Gracely, E.; Joffe, M.D.; Goldsmith, D.P.; Malatack, J.J. Oral versus intravenous corticosteroids in children hospitalized with asthma. J. Allergy Clin. Immunol. 1999, 103, 586–590. [Google Scholar] [CrossRef] [PubMed]
- Young, A.; Marsh, S. Steroid Use in Critical Care. BJA Educ. 2018, 18, 129–134. [Google Scholar] [CrossRef]
- Rower, J.E.; Liu, X.; Yu, T.; Mundorff, M.; Sherwin, C.M.T.; Johnson, M.D. Clinical pharmacokinetics of magnesium sulfate in the treatment of children with severe acute asthma. Eur. J. Clin. Pharmacol. 2017, 73, 325–331. [Google Scholar] [CrossRef]
- Cairns, C.B.; Krafi, M. Magnesium Attenuates the Neutrophil Respiratory Burst in Adult Asthmatic Patients. Acad. Emerg. Med. 1996, 3, 1093–1097. [Google Scholar] [CrossRef]
- Panahi, Y.; Mojtahedzadeh, M.; Najafi, A.; Ghaini, M.; Abdollahi, M.; Sharifzadeh, M.; Ahmadi, A.; Rajaee, S.; Sahebkar, A. The role of magnesium sulfate in the intensive care unit. EXCLI J. 2017, 16, 464–482. [Google Scholar]
- del Castillo, J.; Engbaek, L. The nature of the neuromuscular block produced by magnesium. J. Physiol. 1954, 124, 370–384. [Google Scholar] [CrossRef] [PubMed]
- Goodacre, S.; Cohen, J.; Bradburn, M.; Gray, A.; Benger, J.; Coats, T. Intravenous or nebulised magnesium sulphate versus standard therapy for severe acute asthma (3Mg trial): A double-blind, randomised controlled trial. Lancet Respir. Med. 2013, 1, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Kew, K.M.; Kirtchuk, L.; Michell, C.I. Intravenous magnesium sulfate for treating adults with acute asthma in the emergency department. Cochrane Database Syst. Rev. 2014, 5, CD010909. [Google Scholar]
- Nair, P.; Milan, S.J.; Rowe, B.H. Addition of intravenous aminophylline to inhaled beta2-agonists in adults with acute asthma. Cochrane Database Syst. Rev. 2012, 12, CD002742. [Google Scholar] [CrossRef] [PubMed]
- Dent, G.; Giembycz, M.A.; Rabe, K.F.; Wolf, B.; Barnes, P.J.; Magnussen, H. Theophylline suppresses human alveolar macrophage respiratory burst through phosphodiesterase inhibition. Am. J. Respir. Cell Mol. Biol. 1994, 10, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Meissner, G. Structure-Activity Relationship of Xanthines and Skeletal Muscle Ryanodine Receptor/Ca2+ Release Channel. Pharmacology 2008, 54, 135–143. [Google Scholar] [CrossRef]
- Chen, J.-F.; Chern, Y.; Fredholm, B. Impacts of Methylxanthines and Adenosine Receptors on Neurodegeneration: Human and Experimental Studies. Handb. Exp Pharmacol. 2011, 200, 267–310. [Google Scholar]
- Kelly, A.M.; Powell, C.; Kerr, D. Snapshot of acute asthma: Treatment and outcome of patients with acute asthma treated in Australian emergency departments. Intern. Med. J. 2003, 33, 406–413. [Google Scholar] [CrossRef]
- Dalabih, A.; Harris, Z.L.; Bondi, S.A.; Arnold, D.H. Contemporary aminophylline use for status asthmaticus in pediatric ICUs. Chest 2012, 141, 1122–1123. [Google Scholar] [CrossRef]
- Secombe, P.; Stewart, P.; Singh, S.; Campbell, L.; Stephens, D.; Tran, K.; White, H.; Sheehy, R.; Gibson, J.; Cooke, R.; et al. Clinical management practices of life-threatening asthma: An audit of practices in intensive care. Crit. Care Resusc. 2019, 21, 53–62. [Google Scholar] [CrossRef]
- Mitra, A.A.D.; Bassler, D.; Watts, K.; Lasserson, T.J.; Ducharme, F.M. Intravenous aminophylline for acute severe asthma in children over two years receiving inhaled bronchodilators. Cochrane Database Syst. Rev. 2005, 2, CD001276. [Google Scholar] [CrossRef]
- Travers, A.H.; Milan, S.J.; Jones, A.P.; Camargo, C.A., Jr.; Rowe, B.H. Addition of intravenous beta2-agonists to inhaled beta2-agonists for acute asthma. Cochrane Database Syst. Rev. 2012, 12, CD010179. [Google Scholar]
- Travers, A.A.; Jones, A.P.; Kelly, K.D.; Camargo, C.A.J.; Barker, S.J.; Rowe, B.H. Intravenous beta2-agonists for acute asthma in the emergency department. Cochrane Database Syst. Rev. 2001, 2, CD002988. [Google Scholar] [CrossRef]
- Browne, G.J.; Penna, A.S.; Phung, X.; Soo, M. Randomised trial of intravenous salbutamol in early management of acute severe asthma in children. Lancet 1997, 349, 301–305. [Google Scholar] [CrossRef]
- Nowak, R. Reduced Hospital Admission and Improved Pulmonary Function Following Intravenous MN-221 (Bedoradrine), a Novel, Highly Selective Beta2-Adrenergic Receptor Agonist, Adjunctive to Standard of Care in Severe Acute Exacerbation of Asthma. Chest J. 2010, 138, 166A. [Google Scholar] [CrossRef]
- Bogie, A.L.; Towne, D.; Luckett, P.M.; Abramo, T.J.; Wiebe, R.A. Comparison of Intravenous Terbutaline Versus Normal Saline in Pediatric Patients on Continuous High-Dose Nebulized Albuterol for Status Asthmaticus. Pediatr. Emerg. Care 2007, 23, 355–361. [Google Scholar] [CrossRef]
- Ruangsomboon, O.; Limsuwat, C.; Praphruetkit, N.; Monsomboon, A.; Chakorn, T. Nasal High-flow Oxygen Versus Conventional Oxygen Therapy for Acute Severe Asthma Patients: A Pilot Randomized Controlled Trial. Acad. Emerg. Med. 2021, 28, 530–541. [Google Scholar] [CrossRef]
- Magdy, D.; Metwally, A. High-flow nasal cannula therapy versus standard pressure support non-invasive ventilation in treating adult patients with severe asthma exacerbation complicated with respiratory failure. Eur. Respir. J. 2021, 58 (Suppl. 65), OA1627. [Google Scholar]
- Deng, H.; He, Y.; Fu, X.; Mei, Z.; Li, Y. The efficacy of high-flow oxygen versus conventional oxygen for asthma control: A meta-analysis of randomized controlled studies. Adv. Dermatol. Allergol./Postępy Dermatol. Alergol. 2022, 39, 1077–1082. [Google Scholar] [CrossRef]
- Kallet, R.H. Noninvasive ventilation in acute care: Controversies and emerging concepts. Respir. Care 2009, 54, 259–263. [Google Scholar]
- Soroksky, A.; Klinowski, E.; Ilgyev, E.; Mizrachi, A.; Miller, A.; Ben Yehuda, T.M.; Shpirer, I.; Leonov, Y. Noninvasive positive pressure ventilation in acute asthmatic attack. Eur. Respir. Rev. 2010, 19, 39–45. [Google Scholar] [CrossRef]
- Althoff, M.D.; Holguin, F.; Yang, F.; Grunwald, G.K.; Moss, M.; Vandivier, R.W.; Ho, P.M.; Kiser, T.H.; Burnham, E.L. Noninvasive Ventilation Use in Critically Ill Patients with Acute Asthma Exacerbations. Am. J. Respir. Crit. Care Med. 2020, 202, 1520–1530. [Google Scholar] [CrossRef]
- Smith, A.; Franca, U.L.; McManus, M.L. Trends in the Use of Noninvasive and Invasive Ventilation for Severe Asthma. Pediatrics 2020, 146, e20200534. [Google Scholar] [CrossRef]
- Bond, K.R.; Horsley, C.A.; Williams, A.B. Non-invasive ventilation use in status asthmaticus: 16 years of experience in a tertiary intensive care. Emerg. Med. Australas 2018, 30, 187–192. [Google Scholar] [CrossRef]
- Stefan, M.S.; Nathanson, B.H.; Lagu, T.; Priya, A.; Pekow, P.S.; Steingrub, J.S.; Hill, N.S.; Goldberg, R.J.; Kent, D.M.; Lindenauer, P.K. Outcomes of Noninvasive and Invasive Ventilation in Patients Hospitalized with Asthma Exacerbation. Ann. Am. Thorac. Soc. 2016, 13, 1096–1104. [Google Scholar] [CrossRef]
- Lim, W.J.; Mohammed Akram, R.; Carson, K.V.; Mysore, S.; Labiszewski, N.A.; Wedzicha, J.A.; Rowe, B.H.; Smith, B.J. Non-invasive positive pressure ventilation for treatment of respiratory failure due to severe acute exacerbations of asthma. Cochrane Database Syst. Rev. 2012, 12, CD004360. [Google Scholar] [CrossRef]
- Dai, J.; Wang, L.; Wang, F.; Wang, L.; Wen, Q. Noninvasive positive-pressure ventilation for children with acute asthma: A meta-analysis of randomized controlled trials. Front. Pediatr. 2023, 11, 1167506. [Google Scholar] [CrossRef]
- Thapamagar, S.B.; Doshi, V.; Shenoy, S.; Ganesh, A.; Lankala, S. Outcomes of Noninvasive Ventilation in Obese Patients with Acute Asthma Exacerbations. Am. J. Ther. 2018, 25, e635–e641. [Google Scholar] [CrossRef]
- ICNARC Reports 2012. Report 11. Available online: https://www.icnarc.org/Our-Audit/Audits/Cmp/Our-National-Analyses/Reason-For-Admission (accessed on 5 December 2023).
- Brenner, B.; Corbridge, T.; Kazzi, A. Intubation and Mechanical Ventilation of the Asthmatic Patient in Respiratory Failure. Proc. Am. Thorac. Soc. 2009, 6, 371–379. [Google Scholar] [CrossRef]
- Chakraborty, R.K.; Basnet, S. Status Asthmaticus. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Kohn, M.S. Intubation of the asthma patient. Clin. Allergy Immunol. 1999, 13, 419–428. [Google Scholar]
- Farrow, S.; Farrow, C.; Soni, N. Size matters: Choosing the right tracheal tube. Anaesthesia 2012, 67, 815–819. [Google Scholar] [CrossRef] [PubMed]
- De Jong, A.; Molinari, N.; Terzi, N.; Mongardon, N.; Arnal, J.-M.; Guitton, C.; Allaouchiche, B.; Paugam-Burtz, C.; Constantin, J.-M.; Lefrant, J.-Y.; et al. Early Identification of Patients at Risk for Difficult Intubation in the Intensive Care Unit. Am. J. Respir. Crit. Care Med. 2013, 187, 832–839. [Google Scholar] [CrossRef]
- Bellomo, R.; McLaughlin, P.; Tai, E.; Parkin, G. Asthma Requiring Mechanical Ventilation. Chest 1994, 105, 891–896. [Google Scholar] [CrossRef]
- Demoule, A.; Brochard, L.; Dres, M.; Heunks, L.; Jubran, A.; Laghi, F.; Mekontso-Dessap, A.; Nava, S.; Ouanes-Besbes, L.; Penuelas, O.; et al. How to ventilate obstructive and asthmatic patients. Intensive Care Med. 2020, 46, 2436–2449. [Google Scholar] [CrossRef]
- Tuxen, D.V.; Lane, S. The effects of ventilatory pattern on hyperinflation, airway pressures, and circulation in mechanical ventilation of patients with severe air-flow obstruction. Am. Rev. Respir. Dis. 1987, 136, 872–879. [Google Scholar] [CrossRef] [PubMed]
- Tuxen, D.V. Detrimental effects of positive end-expiratory pressure during controlled mechanical ventilation of patients with severe airflow obstruction. Am. Rev. Respir. Dis. 1989, 140, 5–9. [Google Scholar] [CrossRef]
- Blanch, L.; Bernabé, F.; Lucangelo, U. Measurement of air trapping, intrinsic positive end-expiratory pressure, and dynamic hyperinflation in mechanically ventilated patients. Respir. Care 2005, 50, 110–124. [Google Scholar]
- Briel, M.; Meade, M.; Mercat, A.; Brower, R.G.; Talmor, D.; Walter, S.D.; Slutsky, A.S.; Pullenayegum, E.; Zhou, Q.; Cook, D.; et al. Higher vs. Lower Positive End-Expiratory Pressure in Patients with Acute Lung Injury and Acute Respiratory Distress Syndrome. JAMA 2010, 303, 865. [Google Scholar] [CrossRef]
- Brower, R.G.; Lanken, P.N.; MacIntyre, N.; Matthay, M.A.; Morris, A.; Ancukiewicz, M.; Schoenfeld, D.; Thompson, B.T. Higher versus Lower Positive End-Expiratory Pressures in Patients with the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2004, 351, 327–336. [Google Scholar]
- Oddo, M.; Feihl, F.; Schaller, M.D.; Perret, C. Management of mechanical ventilation in acute severe asthma: Practical aspects. Intensive Care Med. 2006, 32, 501–510. [Google Scholar] [CrossRef]
- Garner, O.; Ramey, J.S.; Hanania, N.A. Management of Life-Threatening Asthma: Severe Asthma Series. Chest 2022, 162, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Leatherman, J. Mechanical ventilation for severe asthma. Chest 2015, 147, 1671–1680. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, C. Ketamine: A review. Update Anaesth. 2005, 20, 25–29. [Google Scholar]
- Betts, E.K.B.E.K.; Parkin, C.E. Use of Ketamine in an Asthmatic Child: A Case Report. Anesth. Analg. 1971, 50, 420–421. [Google Scholar] [CrossRef]
- Kohtala, S. Ketamine—50 years in use: From anesthesia to rapid antidepressant effects and neurobiological mechanisms. Pharmacol. Rep. 2021, 73, 323–345. [Google Scholar] [CrossRef] [PubMed]
- La Via, L.; Sanfilippo, F.; Cuttone, G.; Dezio, V.; Falcone, M.; Brancati, S.; Crimi, C.; Astuto, M. Use of ketamine in patients with refractory severe asthma exacerbations: Systematic review of prospective studies. Eur. J. Clin. Pharmacol. 2022, 78, 1613–1622. [Google Scholar] [CrossRef]
- Sato, T.; Hirota, K.; Matsuki, A.; Zsigmond, E.K.; Rabito, S.F. The Role of the N-Methyl-D-Aspartic Acid Receptor in the Relaxant Effect of Ketamine on Tracheal Smooth Muscle. Anesth. Analg. 1998, 87, 1383–1388. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Chen, T.-L.; Sheu, J.-R.; Chen, R.-M. Suppressive effects of ketamine on macrophage functions. Toxicol. Appl. Pharmacol. 2005, 204, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Heshmati, F.; Zeinali, M.; Noroozinia, H.; Abbacivash, R.; Mahoori, A. Use of Ketamine in Severe Status Asthmaticus in Intensive Care Unit. Iran. J. Allergy Asthma Immunol. 2004, 2, 175–180. [Google Scholar]
- Esmailian, M.; Koushkian Esfahani, M.; Heydari, F. The Effect of Low-Dose Ketamine in Treating Acute Asthma Attack: A Randomized Clinical Trial. Emergency 2018, 6, e21. [Google Scholar]
- Howton, J.C.; Rose, J.; Duffy, S.; Zoltanski, T.; Levitt, M.A. Randomized, Double-Blind, Placebo-Controlled Trial of Intravenous Ketamine in Acute Asthma. Ann. Emerg. Med. 1996, 27, 170–175. [Google Scholar] [CrossRef]
- Sharif, S.; Munshi, L.; Burry, L.; Mehta, S.; Gray, S.; Chaudhuri, D.; Duffett, M.; Siemieniuk, R.A.; Rochwerg, B. Ketamine sedation in the intensive care unit: A survey of Canadian intensivists. Can. J. Anaesth. 2023. Advance online publication. [Google Scholar] [CrossRef]
- Goyal, S.; Agrawal, A. Ketamine in status asthmaticus: A review. Indian J. Crit. Care Med. 2013, 17, 154–161. [Google Scholar] [PubMed]
- Hudson, A.E.; Hemmings, H.C. Pharmacokinetics of Inhaled Anesthetics. In Pharmacology and Physiology for Anesthesia, 2nd ed.; Hemmings, H.C., Egan, T.D., Eds.; Elsevier Inc.: Philadelphia, PA, USA, 2019; pp. 44–69. [Google Scholar]
- Pabelick, C.M.; Ay, B.; Prakash, Y.S.; Sieck, G.C. Effects of Volatile Anesthetics on Store-operated Ca2+Influx in Airway Smooth Muscle. Anesthesiology 2004, 101, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Goff, M.J.; Arain, S.R.; Ficke, D.J.; Uhrich, T.D.; Ebert, T.J. Absence of Bronchodilation during Desflurane Anesthesia: A Comparison to Sevoflurane and Thiopental. Anesthesiology 2000, 93, 404–408. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, S.H. Treatment of Status Asthmaticus with Halothane. JAMA 1984, 251, 2688–2689. [Google Scholar] [CrossRef] [PubMed]
- Johnston, R.G.; Noseworthy, T.W.; Friesen, E.G.; Yule, H.A.; Shustack, A. Isoflurane Therapy for Status Asthmaticus in Children and Adults. Chest 1990, 97, 698–701. [Google Scholar] [CrossRef]
- Shankar, V.; Churchwell, K.B.; Deshpande, J.K. Isoflurane therapy for severe refractory status asthmaticus in children. Intensive Care Med. 2006, 32, 927–933. [Google Scholar] [CrossRef]
- Schutte, D.; Zwitserloot, A.M.; Houmes, R.; de Hoog, M.; Draaisma, J.M.; Lemson, J. Sevoflurane therapy for life-threatening asthma in children. BJA Br. J. Anaesth. 2013, 111, 967–970. [Google Scholar] [CrossRef]
- Baigel, G. Volatile Agents to Avoid Ventilating Asthmatics. Anaesth. Intensive Care 2003, 31, 208–210. [Google Scholar] [CrossRef]
- Nadaud, J.; Landy, C.; Steiner, T.; Pernod, G.; Favier, J.-C. Helium-sevoflurane association: A rescue treatment in case of acute severe asthma. Ann. Fr. Anesth. Rèanim. 2009, 28, 82–85. [Google Scholar] [CrossRef] [PubMed]
- Maltais, F.; Sovilj, M.; Goldberg, P.; Gottfried, S.B. Respiratory Mechanics in Status Asthmaticus: Effects of Inhalational Anesthesia. Chest 1994, 106, 1401–1406. [Google Scholar] [CrossRef] [PubMed]
- Blondonnet, R.; Quinson, A.; Lambert, C.; Audard, J.; Godet, T.; Zhai, R.; Pereira, B.; Futier, E.; Bazin, J.E.; Constantin, J.M.; et al. Use of volatile agents for sedation in the intensive care unit: A national survey in France. PLoS ONE 2021, 16, e0249889. [Google Scholar] [CrossRef] [PubMed]
- Baker, A.; Richardson, D.; Craig, G. Extracorporeal Carbon Dioxide Removal (ECCO2 R) in Respiratory Failure: An Overview, and where Next? J. Intensive Care Soc. 2012, 13, 232–237. [Google Scholar] [CrossRef]
- Barrett, N.A.; Camporota, L. The evolving role and practical application of extracorporeal carbon dioxide removal in critical care. Crit. Care Resusc. J. Australas. Acad. Crit. Care Med. 2017, 19 (Suppl. 1), 62–67. [Google Scholar]
- Abrams, D.; Brodie, D. Extracorporeal Membrane Oxygenation for Adult Respiratory Failure. Chest 2017, 152, 639–649. [Google Scholar] [CrossRef]
- Conrad, S.A.; Broman, L.M.; Taccone, F.S.; Lorusso, R.; Malfertheiner, M.V.; Pappalardo, F.; Di Nardo, M.; Belliato, M.; Grazioli, L.; Barbaro, R.P.; et al. The Extracorporeal Life Support Organization Maastricht Treaty for Nomenclature in Extracorporeal Life Support. A Position Paper of the Extracorporeal Life Support Organization. Am. J. Respir. Crit. Care Med. 2018, 198, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Brenner, K.; Abrams, D.C.; Agerstrand, C.L.; Brodie, D. Extracorporeal carbon dioxide removal for refractory status asthmaticus: Experience in distinct exacerbation phenotypes. Perfusion 2014, 29, 26–28. [Google Scholar] [CrossRef]
- De Rosa, S.; Golino, G.; Ronco, C. Extracorporeal carbon dioxide removal in heart-beating donor with acute severe asthma: A case report. Respir. Med. Case Rep. 2020, 29, 101010. [Google Scholar] [CrossRef]
- Elliot, S.C.; Paramasivam, K.; Oram, J.; Bodenham, A.R.; Howell, S.J.; Mallick, A. Pumpless extracorporeal carbon dioxide removal for life-threatening asthma. Crit. Care Med. 2007, 35, 945–948. [Google Scholar] [CrossRef]
- Bromberger, B.J.; Agerstrand, C.; Abrams, D.; Serra, A.; Apsel, D.; Tipograf, Y.; Ginsburg, M.E.; Ebright, M.I.; Stanifer, B.P.; Oommen, R.; et al. Extracorporeal Carbon Dioxide Removal in the Treatment of Status Asthmaticus. Crit. Care Med. 2020, 48, E1226–E1231. [Google Scholar] [CrossRef] [PubMed]
- McNamee, J.J.; Gillies, M.A.; Barrett, N.A.; Perkins, G.D.; Tunnicliffe, W.; Young, D.; Bentley, A.; Harrison, D.A.; Brodie, D.; Boyle, A.J.; et al. Effect of Lower Tidal Volume Ventilation Facilitated by Extracorporeal Carbon Dioxide Removal vs. Standard Care Ventilation on 90-Day Mortality in Patients with Acute Hypoxemic Respiratory Failure. JAMA 2021, 326, 1013–1023. [Google Scholar] [CrossRef]
- NICE Procedures Guidence [IPG564]. Available online: https://www.nice.org.uk/guidance/ipg564 (accessed on 5 December 2023).
- Makdisi, G.; Wang, I.W. Extra Corporeal Membrane Oxygenation (ECMO) review of a lifesaving technology. J. Thorac. Dis. 2015, 7, E166–E176. [Google Scholar] [PubMed]
- Camporota, L.; Meadows, C.; Ledot, S.; Scott, I.; Harvey, C.; Garcia, M.; Vuylsteke, A. Consensus on the referral and admission of patients with severe respiratory failure to the NHS ECMO service. Lancet Respir. Med. 2021, 9, e16–e17. [Google Scholar] [CrossRef]
- Skinner, S.C.; Hirschl, R.B.; Bartlett, R.H. Extracorporeal life support. Semin. Pediatr. Surg. 2006, 15, 242–250. [Google Scholar] [CrossRef] [PubMed]
- López Sanchez, M. Mechanical ventilation in patients subjected to extracorporeal membrane oxygenation (ECMO). Med. Intensiv. 2017, 41, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Thanthitaweewat, V.; Sriprasart, T. Therapeutic Bronchoscopy under Extracorporeal Membrane Oxygenation (ECMO) Support: Case Series; Interventional Pulmonology, European Respiratory Society International Congress: Madrid, Spain, 2019; p. PA3404. [Google Scholar]
- Peek, G.J.; Mugford, M.; Tiruvoipati, R.; Wilson, A.; Allen, E.; Thalanany, M.M.; Hibbert, C.L.; Truesdale, A.; Clemens, F.; Cooper, N.; et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): A multicentre randomised controlled trial. Lancet 2009, 374, 1351–1363. [Google Scholar] [CrossRef] [PubMed]
- Brazzi, L.; Lissoni, A.; Panigada, M.; Bottino, N.; Patroniti, N.; Pappalardo, F.; Gattinoni, L. Simulation-Based Training of Extracorporeal Membrane Oxygenation During H1N1 Influenza Pandemic. Simul. Healthc. J. Soc. Simul. Healthc. 2012, 7, 32–34. [Google Scholar] [CrossRef]
- Chan, S.-Y.; Figueroa, M.; Spentzas, T.; Powell, A.; Holloway, R.; Shah, S. Prospective Assessment of Novice Learners in a Simulation-Based Extracorporeal Membrane Oxygenation (ECMO) Education Program. Pediatr. Cardiol. 2013, 34, 543–552. [Google Scholar] [CrossRef]
- Yeo, H.J.; Kim, D.; Jeon, D.; Kim, Y.S.; Rycus, P.; Cho, W.H. Extracorporeal membrane oxygenation for life-threatening asthma refractory to mechanical ventilation: Analysis of the Extracorporeal Life Support Organization registry. Crit. Care 2017, 21, 297. [Google Scholar] [CrossRef]
- Warren, A.; Chiu, Y.-D.; Villar, S.S.; Fowles, J.-A.; Symes, N.; Barker, J.; Camporota, L.; Harvey, C.; Ledot, S.; Scott, I.; et al. Outcomes of the NHS England National Extracorporeal Membrane Oxygenation Service for adults with respiratory failure: A multicentre observational cohort study. Br. J. Anaesth. 2020, 125, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Sy, E.; Sklar, M.C.; Lequier, L.; Fan, E.; Kanji, H.D. Anticoagulation practices and the prevalence of major bleeding, thromboembolic events, and mortality in venoarterial extracorporeal membrane oxygenation: A systematic review and meta-analysis. J. Crit. Care 2017, 39, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Alzeer, A.H.; Al Otair, H.A.; Khurshid, S.M.; El Badrawy, S.; Bakir, B.M. A case of near fatal asthma: The role of ECMO as rescue therapy. Ann. Thorac. Med. 2015, 10, 143–145. [Google Scholar] [CrossRef]
- Di Lascio, G.; Prifti, E.; Messai, E.; Peris, A.; Harmelin, G.; Xhaxho, R.; Fico, A.; Sani, G.; Bonacchi, M. Extracorporeal membrane oxygenation support for life-threatening acute severe status asthmaticus. Perfusion 2017, 32, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Kowalewski, C.; Schnürer, P.; Kopp, S.; Windschmitt, J.; Oezkur, M.; Kriege, M.; Münzel, T.; Kaes, J.; Sagoschen, I.; Wild, J. VV-ECMO as bridge and safety net for successful therapeutic polypragmasy in a case of influenza-triggered near-fatal asthma. Clin. Case Rep. 2023, 11, e7709. [Google Scholar] [CrossRef] [PubMed]
- Maqsood, U.; Patel, N. Extracorporeal membrane oxygenation (ECMO) for near-fatal asthma refractory to conventional ventilation. BMJ Case Rep. 2018, 2018, bcr-2017-223276. [Google Scholar] [CrossRef] [PubMed]
- Bendstrup, E.; Jensen, J. Inhaled heparin is effective in exacerbations of asthma. Respir. Med. 2000, 94, 174–175. [Google Scholar] [CrossRef]
- Ashmawy, R.; Zaki, A.; Baess, A.; El Sayed, I. Efficacy and safety of inhaled heparin in asthmatic and chronic obstructive pulmonary disease patients: A systematic review and a meta-analysis. Sci. Rep. 2023, 13, 13326. [Google Scholar] [CrossRef]
- Niven, A.S.; Argyros, G. Alternate Treatments in Asthma. Chest 2003, 123, 1254–1265. [Google Scholar] [CrossRef]
- Martineau, P.; Vaughan, L.M. Heparin Inhalation for Asthma. Ann. Pharmacother. 1995, 29, 71–73. [Google Scholar] [CrossRef]
- Shak, S.; Capon, D.J.; Hellmiss, R.; Marsters, S.A.; Baker, C.L. Recombinant human DNase I reduces the viscosity of cystic fibrosis sputum. Proc. Natl. Acad. Sci. USA 1990, 87, 9188–9192. [Google Scholar] [CrossRef] [PubMed]
- Picot, R.; Das, I.; Reid, L. Pus, deoxyribonucleic acid, and sputum viscosity. Thorax 1978, 33, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Silverman, R.A.; Foley, F.; Dalipi, R.; Kline, M.; Lesser, M. The use of rhDNAse in severely ill, non-intubated adult asthmatics refractory to bronchodilators: A pilot study. Respir. Med. 2012, 106, 1096–1102. [Google Scholar] [CrossRef] [PubMed]
- Greally, P. Human recombinant DNase for mucus plugging in status asthmaticus. Lancet 1995, 346, 1423–1424. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Harrison, E.; Durward, A.; Murdoch, I.A. Intratracheal recombinant human deoxyribonuclease in acute life-threatening asthma refractory to conventional treatment. Br. J. Anaesth. 2000, 84, 505–507. [Google Scholar] [CrossRef] [PubMed]
- Hull, J.H.; Castle, N.; Knight, R.K.; Ho, T.B. Nebulised DNase in the treatment of life threatening asthma. Resuscitation 2007, 74, 175–177. [Google Scholar] [CrossRef]
- Gluck, E.H.; Onorato, D.J.; Castriotta, R. Helium-Oxygen Mixtures in Intubated Patients with Status Asthmaticus and Respiratory Acidosis. Chest 1990, 98, 693–698. [Google Scholar] [CrossRef]
- Diehl, J.L.; Peigne, V.; Guérot, E.; Faisy, C.; Lecourt, L.; Mercat, A. Helium in the adult critical care setting. Ann. Intensive Care 2011, 1, 24. [Google Scholar] [CrossRef]
- Chevrolet, J.-C. Helium oxygen mixtures in the intensive care unit. Crit. Care 2001, 5, 179–181. [Google Scholar] [CrossRef]
- Rodrigo, G.J.; Pollack, C.V.; Rodrigo, C.; Rowe, B.H. Heliox for non-intubated acute asthma patients. Cochrane Database Syst. Rev. 2006, 4, CD002884. [Google Scholar] [CrossRef]
- Rodrigo, G.J.; Castro-Rodriguez, J.A. Heliox-Driven Β2-Agonists Nebulization for Children and Adults with Acute Asthma: A Systematic Review with Meta-Analysis. Ann. Allergy Asthma Immunol. 2014, 112, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Hashemian, S.M.; Fallahian, F. The use of heliox in critical care. Int. J. Crit. Illn. Inj. Sci. 2014, 4, 138–142. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Relative Indications | Immediate Indications |
|---|---|
| Progressive exhaustion | Cardiac arrest |
| Increasing use of accessory muscles or change in rate/depth of respiration | PaO2 < 8.0 kPa and/or PaCO2 > 6.5 kPa |
| Change in posture or speech | Severe obtundation or coma |
| Failure to reverse severe respiratory acidosis despite intensive therapy | Impending respiratory failure with gasping or inability to speak |
| Altered sensorium | Respiratory arrest |
| Severe hypoxemia with maximal oxygen delivery | |
| Silent chest |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Talbot, T.; Roe, T.; Dushianthan, A. Management of Acute Life-Threatening Asthma Exacerbations in the Intensive Care Unit. Appl. Sci. 2024, 14, 693. https://doi.org/10.3390/app14020693
Talbot T, Roe T, Dushianthan A. Management of Acute Life-Threatening Asthma Exacerbations in the Intensive Care Unit. Applied Sciences. 2024; 14(2):693. https://doi.org/10.3390/app14020693
Chicago/Turabian StyleTalbot, Thomas, Thomas Roe, and Ahilanandan Dushianthan. 2024. "Management of Acute Life-Threatening Asthma Exacerbations in the Intensive Care Unit" Applied Sciences 14, no. 2: 693. https://doi.org/10.3390/app14020693