In this section, the results related to each research question are presented. The first subsection provides the existing definitions of sustainability of e-health solutions. The second and third subsection discusses the sustainability dimensions and elements, and assessment methods.
4.2.2. Sustainability Dimensions
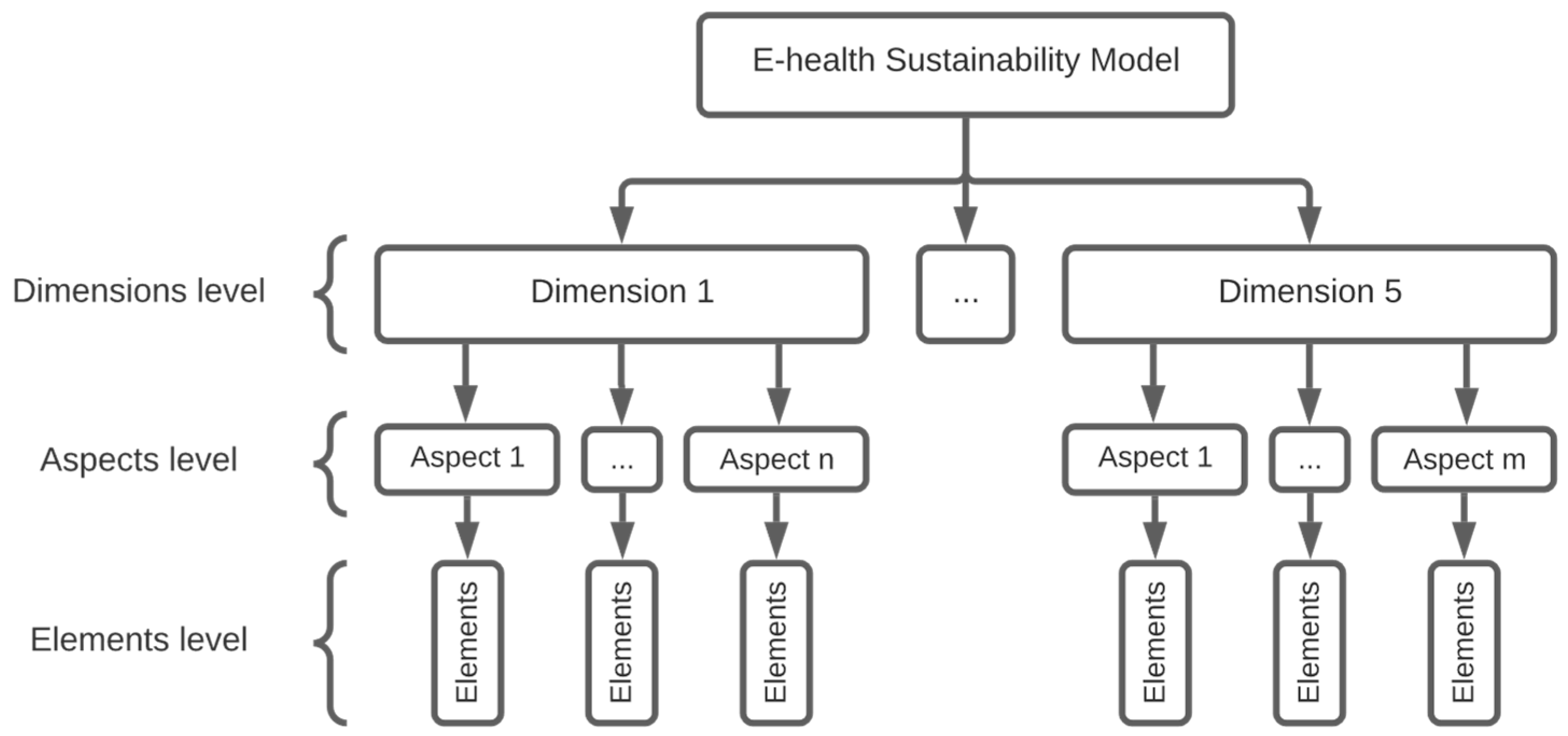
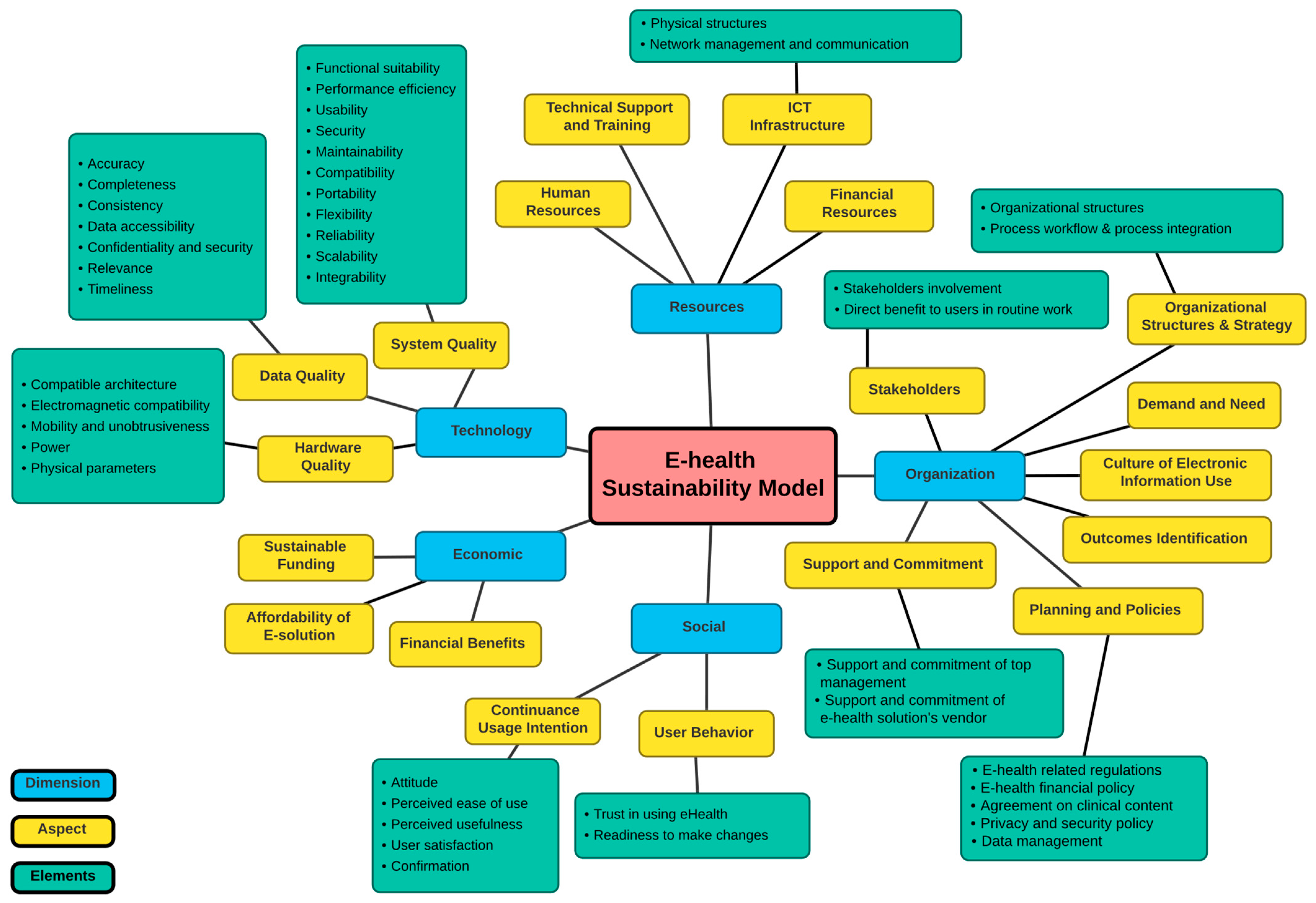
The studies discussed the sustainability of e-health solutions by presenting some of its dimensions or aspects. In the data extraction, the constructs of the sustainability mentioned in the studies were categorized into dimensions and aspects. The dimensions are the essential pillars of sustainability, which are high-level categories that involve a set of aspects, which influence the sustainability of e-health solutions. The aspects are a fine-grained level of detail of the dimensions that include elements and items through which data can be collected and sustainability evaluation is enabled.
Table 8 presents the dimensions mentioned in the studies, which are technology, economic, social/human, organization/management/environment, political/legal, and resourcing.
Table 9 contains all aspects mentioned in the studies.
Two studies [
8,
35] discussed the issue of sustaining the implementation of e-health solutions and identified similar sustainability dimensions, which are social, environmental, economic, technological, and individual dimensions. It is worth noting that the focus of the environment dimension in both studies was different. In the study of Ouhbi et al. [
8], the focus was on the sustainability from an ecological perspective, by raising environmental issues such as energy consumption and emissions of carbon dioxide. The study underlined how the e-health solution should consider this aspect in order for it to be sustainable. The same conception of the environment dimension was found in study [
32]. On the other hand, study [
35] focused on the work and organizational environment, such as organizational culture, values, leadership, and resources.
Joshua et al. [
26] concluded that some issues impact the sustainability of health information exchange (HIE). These are financial, political, and organizational issues. In their study, they discussed the strengths and weaknesses of organizational models used for HIE in New York State, such as regional health information organization (RHIO). In addition, they provided suggestions to ensure the sustainability and effectiveness of exchange efforts. Financial issues were perceived as upfront costs, decreased profits, and funding, while political and organizational issues were summarized as the difficulty of cooperation and collaboration among healthcare organizations (e.g., other competitive hospitals). The authors suggested that existing public/government funding and codifying health laws that enforce and facilitate the HIE would help in solving these issues. Another study [
30] investigated the sustainability of a pilot project for smart connected health services that used Internet of Things (IoT) technology and were provided for both patients and health professionals. The results showed that in order to sustain smart connected hospital services, it is necessary to consider the technical feasibility, economic feasibility, and organizational commitment and support.
Iandolo et al. [
38] argued that the focus of healthcare technology assessment should be shifted from efficiency and effectiveness to sustainability. By proposing a reference framework, they stated that the sustainability of the technology can be achieved by assessing three aspects, along with considering the relations and interactions between them [
25]. These aspects are economic, social, and political. Garde et al. [
9] analyzed the inhibitors and enablers that influence the sustainability of health information systems (HIS). They proposed a high-level sustainability framework based on four pillars, which are clinical, technical, socio-technical, and political/business. Wade et al. [
7] investigated 54 telehealth services in Australia to understand the reasons behind the continuing and ceased services, and to assess their sustainability. The results revealed that insufficient demand, issues with technology, funding, loss of senior management support, and loss of the interest of clinicians are the failure reasons among the ceased telehealth services. On the other hand, the success factors of sustainable healthcare services are sufficient demand, available funding, and developing organizational structures that help to integrate telehealth into their regular operations. Furthermore, they demonstrated the importance of routinization and integration of the telehealth service, especially when it is executed within an existing clinical unit. Moreover, they stated that in the public sector, the funding is not a major issue; as long as the need and the support could be demonstrated, then the funds would follow. Additionally, the sustainability of a telehealth application called TeleRehab was discussed by Scheideman-Miller et al. [
28] and concluded that six factors impact the sustainability of TeleRehab. These factors are organizational strategy, establishment of need, organizational stakeholders, organizational commitment, human factors, revenue/cost savings, and outcomes. Organizational strategy addresses the customer, clinical operations, financial, and clinical development for health care providers and the organization. The human factors involve acceptance, long-term commitment of healthcare providers, specialized training, and user satisfaction. In addition, the outcomes of the e-solution vary whether they are clinical, financial, technical, or social outcomes. Therefore, they should be defined by the organization itself and need to be evaluated regularly. It was stated that a partnership of collaborators within an organization, including clinical, technical, and administrative professionals, will help in ensuring the success and sustainability of a telemedicine program.
Similar dimensions were mentioned in other studies that presented frameworks and methods to assess e-health sustainability. Fanta et al. [
35] evaluated the contribution of four frameworks for the implementation of e-health systems in a resource-constrained environment. The evaluation was carried out in terms of four sustainability dimensions. These are social, environmental, economic, and technological. They underlined that it is essential to consider the alignment of social, economic, and environmental factors with the technology factor to ensure the sustainability of e-health. In a following study [
33], Fanta et al. presented the topic of sustaining the e-health implementation and emphasized the importance of the technological, social, organizational, and economic dimensions in this regard. The study proposed a conceptual framework for the sustainability of e-health implementation that focused on both organizational and technological dimensions. The organizational dimension comprises some aspects such as resources (i.e., human, physical, and financial resources), workflow process, and management support, while the technological dimension encompasses system quality, information quality, and service quality. Furthermore, they underlined the techno-organizational processes that are essential for the success of e-health implementation. These processes are user training, data management, stakeholder engagement, project management, and organizational communications. Remondino [
32] proposed a framework that includes five dimensions, which are management, organization, technology, environment, and social. The framework helps in the long-term assessment of the sustainability of IT applications and projects in healthcare and their implications on the healthcare organization, with respect to the five mentioned dimensions.
With regard to engineering requirements, Ouhbi et al. [
8] have demonstrated the need for defining sustainability software requirements that are not focused only on the energy consumption of the software. Instead, they developed a design catalog called SCH-CAT for sustainable connected health applications. The catalog contains five dimensions: economic, individual, social, environment, and technical; all of these have their own sustainability requirements except for the economic dimension, whose requirements were not covered because they are not considered inherent requirements. The catalog was used in the study to evaluate the sustainability of a connected health app for blood donation. Dyk et al. [
36] discussed two models that aim to assist in the successful implementation and sustainability of e-health solutions. The technology, users, work processes, finances, and policy categories were included in both models, as they contribute to the sustainability of e-health solutions. Along with that, Chowdhury et al. [
10] proposed an optimization integrated fuzzy QFD methodology to determine the optimal strategies that can be used to mitigate a service’s barriers and achieve an organization’s sustainability goals. They emphasized three dimensions that must be considered and balanced for sustainable service design. These dimensions are social, environmental, and economic. The proposed methodology was applied to an m-health services setting in Bangladesh, by which lists of barriers and strategies to mitigate them were identified regarding m-health service sustainability. The results of the study emphasized the importance of training the service providers and collecting customers’ feedback to improve the service quality. Furthermore, they stated that mitigating a service’s barriers has a substantial impact on the sustainable health service.
Moreover, some studies argued that user acceptance is significant to sustain e-health solutions. Wade et al. [
37] developed an explanatory model for the telehealth services’ sustainability. In their work, they argued that the acceptance of clinicians is the key factor that influences the sustainability of telehealth services. The model shows how other components, such as workforce availability, clinician demand, adequate technology, and resourcing are related to clinician acceptance. The two factors, clinician demand for the service and adequate technology, impact the clinician acceptance of the service, which in turn influences the clinician workforce availability and leads to the telehealth service being sustained. To achieve clinician acceptance, the study suggested two strategies, legitimation and relationship building. Legitimation consists of promoting positive beliefs about telehealth among clinicians, while relationship building is concerning with maintaining good relationships with those who provide the care, both of which are shown in the model as parts of champions promoting telehealth. The continuous usage intention of electronic medical records (EMRs) among healthcare professionals was evaluated using technology continuance theory (TCT) in [
29]. With continuance of usage being one factor of sustainability, the study focused on the six acceptance constructs that influence continuance usage. The six constructs are confirmation, satisfaction, perceived usefulness (PU), perceived ease of use (PEU), attitude, and continuance intention. Spies [
34] identified the concerns of m-health implementation when sustainable use is the intended goal for the system. The concerns were discussed in terms of the patient’s and health practitioner’s perspectives (e.g., acceptance, usefulness, wearability, and quality of service), as well as the considerations of hardware and software design (e.g., compatibility, data management, functionality, and interoperability).
Technical, political, and management dimensions were the focus of other studies. Petersen [
27] addressed the role of technical support for hardware, software, and people-ware in sustaining the hospital information system (IS) and information technology (IT) infrastructure. Lenz [
31] stated that two goals must be considered equally for the sustainability of healthcare information systems, which are process integration and systems integration. Chen and Wu [
25] proposed a judgment-decomposition analytic hierarchy process (JD-AHP) approach to help decision-makers in assessing the sustainability of smart e-health applications, such as the smart body analyzer. The main factors that critically influence the sustainability of a smart technology application are unobtrusiveness, supporting online social networking, relaxation of the related medical laws, future e-health market size, correct identification of need and situation. Shabo [
23,
24] discussed the sustainability of electronic health records (EHRs). The first study discussed sustainability issues of three different models of EHR from management (i.e., conflicts of interests and access restriction for some special cases), legal (i.e., patients’ bill of rights), and technological (i.e., semantic interoperability standards) aspects. Furthermore, the study proposed the Independent Health Record Banks (IHRBs) model that would help in sustaining the her, while the following paper [
24] discussed sustainability considerations of IHRBs, which are legal and ethical (e.g., authentication, access control, privacy, data integrity), business (i.e., revenue and reducing the cost of data archiving), and technological (i.e., information exchange standards). These considerations act as guidelines for the new legislation needed for IHRBs to be established and operate successfully.
4.2.3. Evaluation/Assessment Methods
Eight of the primary studies [
8,
25,
29,
32,
33,
34,
35,
36] discussed a method, a framework, a model, or a theory to evaluate the sustainability of e-health solutions. These are the JD-AHP approach [
25], the technology continuance theory (TCT) model [
29], the HCC-MOTES framework [
32], a conceptual framework to sustain e-health implementation [
33], a model to evaluate m-health systems [
34], the SCH-CAT catalog [
8], a conceptual framework for e-health systems in a resource-constrained environment [
35], and a model for sustaining telemedicine projects [
36]. The e-health solutions mentioned in the studies are smart e-health applications, EMRs, information technology in healthcare, the Electronic Health Management Information System (eHMIS), m-health systems, and telehealth.
Table 10 presents a summary of the proposed evaluation/assessment methods.
Chen and Wu [
25] identified several factors that are critical to the sustainability of technology applications in healthcare. By using the JD-AHP method proposed in their study, the priority of critical sustainability factors in two or more technologies are compared by a decision-maker to determine which technology is more likely to be sustained. Using 10 smart technologies in e-health, the proposed method was compared against existing methods, which are AHP, OWA, and MACBETH. However, as stated in the study, this method works for one decision-maker, if more were involved, then the sustainability problem becomes considerably complicated.
Gilani et al. [
29] used the TCT model to evaluate the continuance usage intention of an EMR system among users (i.e., healthcare professionals) in the post-adoption phase. In their study, the hypotheses discussed the positive effect of satisfaction, attitude, perceived usefulness, and perceived ease of use for healthcare professionals on their continuance intention to use the EMR system. In order to test the hypotheses, a survey was carried out on 195 respondents consisting of various healthcare professionals from five hospitals. Results showed that all hypotheses in the TCT model were supported, which indicates the significant power of TCT to explain EMR system continuance usage intention of both short- and long-term users. As indicated in their study, TCT will help policymakers and managers in the healthcare sector to understand the factors that result in the ongoing use of an EMR system after the adoption phase.
Remondino [
32] developed a framework, named HHC-MOTES, that contains a novel set of key performance indicators (KPIs) to evaluate the sustainability of healthcare IT projects in terms of five dimensions (management, organization, technology, environment, and social). The framework aimed to provide a qualitative measurement of various aspects related to the sustainability of IT applications in healthcare. It is stated in the study that the HHC-MOTES framework can be used by healthcare decision-makers for strategic decisions regarding introducing or updating IT systems or examining current systems and identify limitations and shortcomings. However, it worth noting that the mentioned KPIs of all dimensions, other than the technology dimension, were focused on assessing the positive impact of IT systems on the efficiency of the healthcare system. For example, in the environment dimension, the indicators evaluated the reduction in paper use and energy consumption as a result of using the IT system. However, the technological KPIs discussed the aspects that should be considered to ensure the sustainability of IT systems in healthcare. Examples of these indicators are modifiability, reusability, portability, and supportability of the IT system.
Fanta et al. [
33] developed a conceptual framework that describes how organizational and technical factors influence the sustainability of eHealth implementation. The framework has four sections. These sections are (1) inputs, which contains organizational and technological factors, (2) processes, which deals with activities executed to achieve the desired outputs, (3) outputs, which consists of intention to use, actual use, and user satisfaction, and (4) outcomes, which represents the organizational benefits (i.e., improving the decision-making process and internal communications in the organization). By using a causal loop diagram (CLD), the study presented the dynamic interactions between organizational factors and the technological dimensions. Additionally, the study drew insights from the literature about measuring the technological aspects. For system quality, it could be measured by ease of use, functionality, reliability, flexibility, portability, integration, and importance of the system [
42,
43,
44]. The measures of information quality consist of accuracy, timeliness, completeness, relevance, and consistency of information produced by the IT system [
42,
43,
44,
45]. Moreover, the service quality measures include up-to-date hardware and software, reliability, responsiveness, assurance, and empathy of technical support [
43,
44].
The model proposed by Spies [
34] aimed to be used as an evaluation method for developed and under-developed m-health systems to assess the sustained use of them. The model focuses on evaluating aspects related to the user (i.e., patients and physicians) and system design (i.e., hardware and software), each of which are intended to be measured by endorsed standards. The standards are included in
Table 10.
As requirements engineering plays a vital role in software sustainability, Ouhbi et al. [
8] designed the SCH-CAT catalog for software quality requirements that are critical to the sustainability of connected health (CH) applications. Although the SCH-CAT catalog targets the design phase of CH applications, a checklist can be generated from it, which includes a set of requirements to be used to evaluate the sustainability of CH applications in the implementation phase. The catalog was applied to assess the sustainability of a running CH application called Blood Donor+. A questionnaire containing requirements as checklist questions was used to evaluate the CH app, in which the answer is one of the three options: yes (+1), no (+0), and partially (+0.5). The overall score was calculated and the threshold score that determines the app’s sustainability was set to be 50%.
Based on a literature survey, Fanta et al. [
35] constructed a conceptual framework that can support the efforts of developers, researchers, managers, and policy makers to ensure the implementation of sustainable e-health systems in resource-constrained settings. In the study, the framework was used to assesses the contribution of four e-health frameworks. The framework consists of four sustainability aspects, namely, social, environmental, economic, and technological, all of which contain indicators that can be used to evaluate the sustainability of e-health systems.
Dyk et al. [
36] discussed two models, the TeleMedicine Maturity Model (TMMM) and the CeHRes roadmap, that were demonstrated to be effective in facilitating, implementing, and sustaining telemedicine projects. The CeHRes roadmap serves as a guide to the establishment of a telemedicine service, whilst the TMMM is concerned with maturation of the existing telemedicine service. In the study, the authors proposed a new model by combining these two models. In the proposed model, it was suggested that each maturity level of TMMM serves as a stage gate for each of the phases of the CeHRes roadmap. Maturity levels are initial, managed, defined, quantitatively managed, and optimized. The maturity levels are used to evaluate the maturity categories, which are technology, users, work processes, finances, and policies. By applying the proposed model to an e-health solution, the resulting maturity level of each category determines its sustainability.
Iandolo et al. [
38] argued that the focus of healthcare technology assessment should be shifted from efficiency and effectiveness to sustainability. They proposed a reference framework containing efficiency and effectiveness dimensions to achieve the sustainability dimension of healthcare technology. They defined efficiency as the plans (i.e., things are done in the right way), effectiveness to be the goals (i.e., the right things get done.), and sustainability as when the right relationships exist with other service systems. As they indicated, efficiency can be measured with reference to the structure, whilst the effectiveness of a system is measured with reference to its specific context and in relation to the general environment; sustainability therefore can be achieved.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}