

The New Role of the Dental Assistant and Nurse in the Age of Advanced Artificial Intelligence in Telehealth Orthodontic Care with Dental Monitoring: Preliminary Report

 ,
,  ,
,  ,
,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials, Methods, and Concept
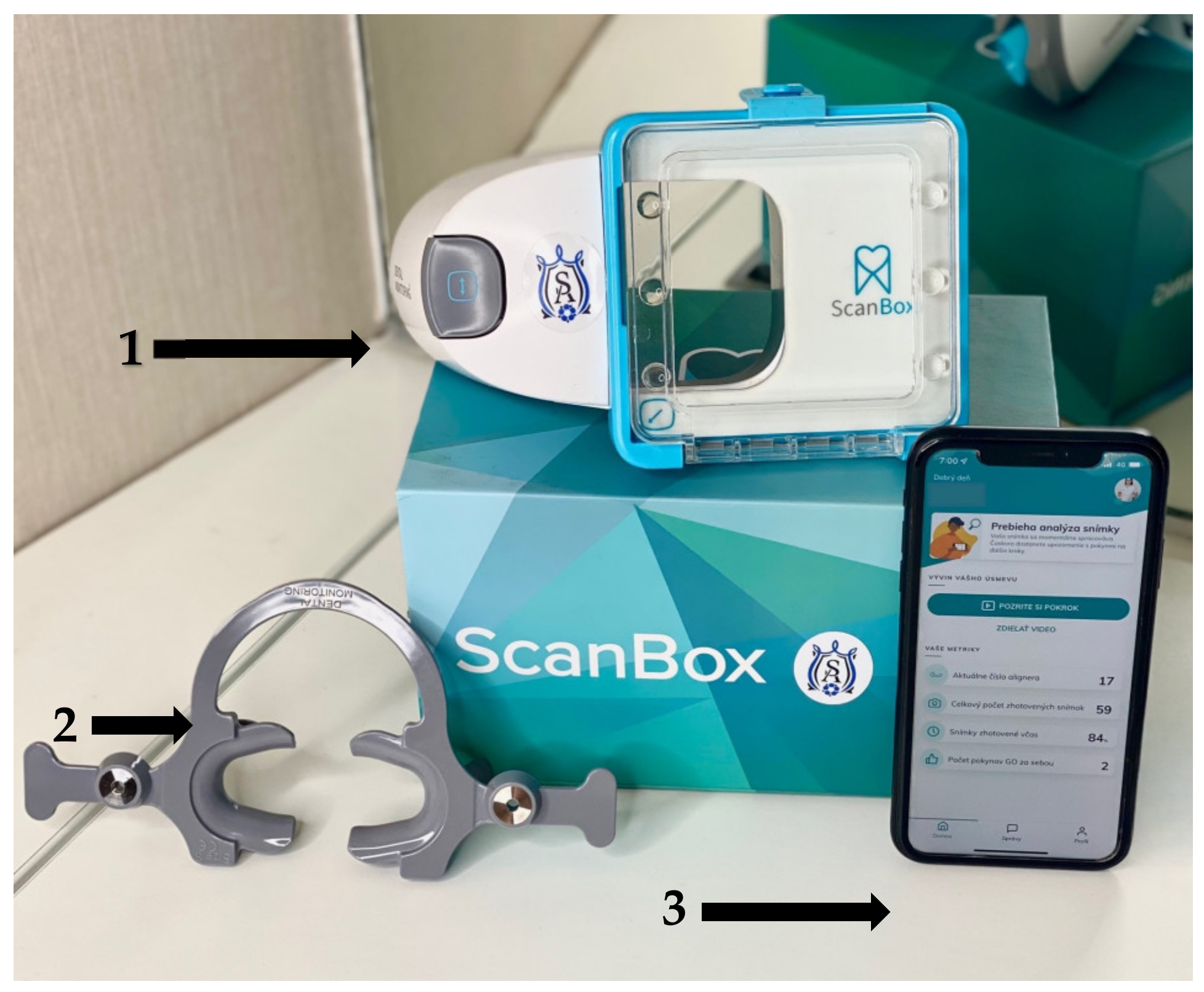
2.1. Materials
- The dental monitoring scan box;
- Retractor;
- The patient’s smartphone.
2.2. Methods
2.2.1. Method of Evaluation
- A comparison of average treatment refinements per patient from a 3 year average before implementation of DM and after. Implementation of DM into a treatment workflow has been compulsory since 2019;
- A reduction in the number of in-person appointments required for patients who received dental monitoring and in the period without DM;
- An online patient satisfaction feedback provided after every appointment; an improvement in patient satisfaction and comfort level with the use of Dental Monitoring® (DM) (Dental Monitoring Co., Paris, France);
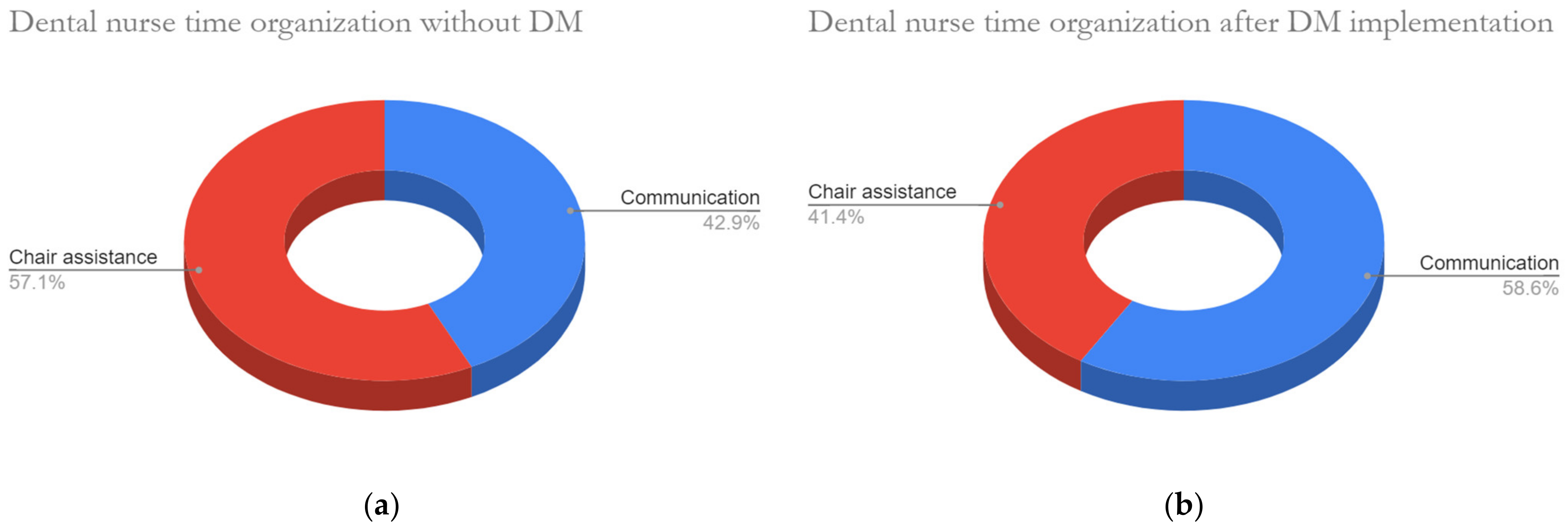
- Evaluation of the nurse’s/assistant’s daily activities in relation to the organization of time.
2.2.2. Practical Aspects of Dental Monitoring® (DM) (Dental Monitoring Co., Paris, France)
- Semi-automatic AI communication with the patient (e.g., non-ideal dental hygiene with automatic recommendations for improvement);
- Digital or face-to-face problem management with the dental assistant (e.g., inadequate dental hygiene or the need to improve the wearing of aligners);
- Need for direct decision-making by the dentist, revision of treatment, or direct doctor-patient communication, depending on the severity and nature of the problem detected by the DM app. Or when a clinical alert, setup by the doctor, has been achieved.
- A scan of bitten teeth without aligners;
- A scan of the teeth apart, without aligners;
- A scan where the patient has his mouth open and the inside of the teeth is scanned, without aligners;
- A scan of teeth apart with aligners.
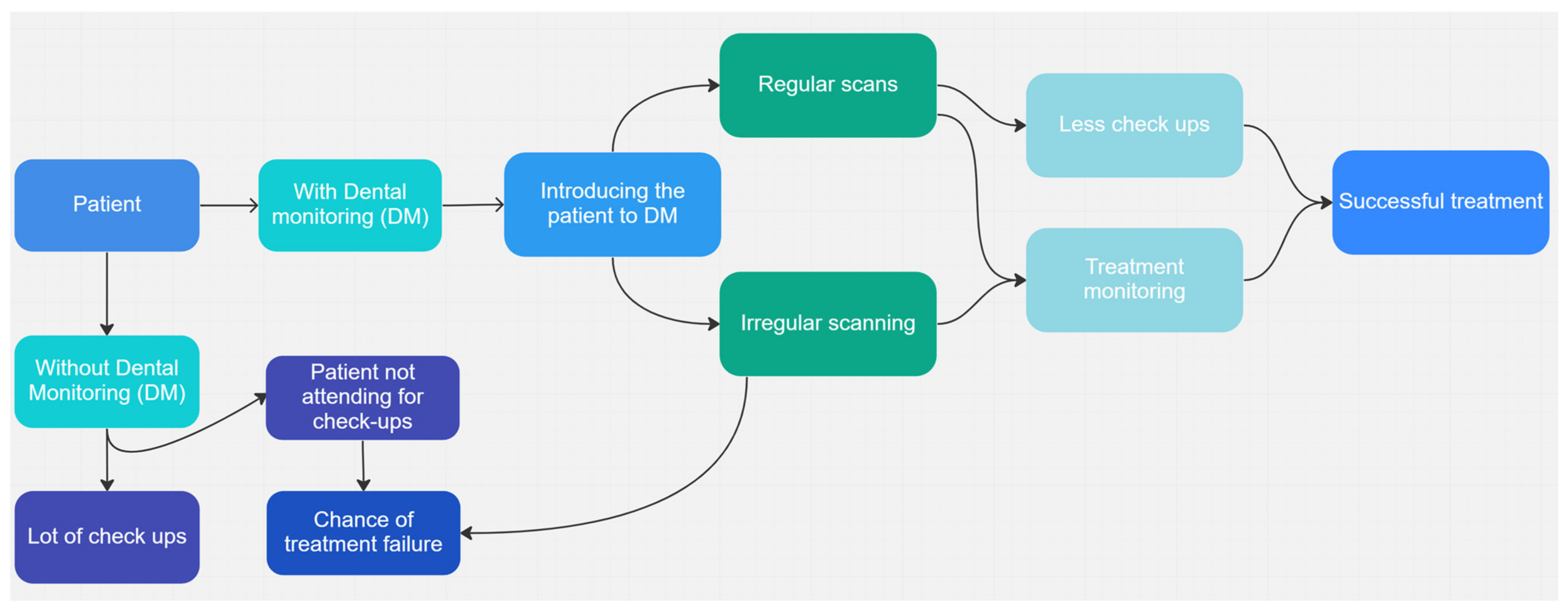
2.3. Concept
3. Results
4. Discussion
- Automation of tasks: AI can automate tasks that dental nurses currently perform, such as scheduling appointments, taking patient histories, and providing patient education. This can free up time for dental nurses to focus on more complex tasks or to interact with patients in a more meaningful way;
- Improved accuracy: AI can be used not only to analyze patient data or create more accurate diagnoses and treatment plans. It can also predict complications, keep an eye on allergies, or provide a nonstop monitor and alert system in harmony with telehealth solutions. This can lead to improved patient outcomes and increased efficiency in the clinic;
- Personalized treatment plans and communication: AI can be used to create personalized treatment plans based on a patient’s individual needs and perform more personalized communication depending on patient individuality and shown communication preferences. This can lead to better patient outcomes and increased patient satisfaction;
- Improved patient experience: AI-powered chatbots that will be learning from nurses’ answers to patient questions will provide personalized advice;
- The combination of telemedicine and AI provides software solutions for orthodontic treatment that allow some parts of orthodontic treatment to be performed in locations other than the dental office. This can lead to further disruption of established clinical care workflows.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsolakis, I.A.; Christopoulou, I.; Siotou, K.; Alexiou, A.; Psarras, V.; Papadopoulou, E.; Tsolakis, A.I. Frequency and Management of Accidental Incidents in Orthodontics. Children 2022, 9, 1801. [Google Scholar] [CrossRef]
- Thurzo, A.; Javorka, V.; Stanko, P.; Lysy, J.; Suchancova, B.; Lehotska, V.; Valkovic, L.; Makovnik, M. Digital and Manual Cephalometric Analysis. Bratisl. Lek. Listy 2010, 111, 97–100. [Google Scholar] [PubMed]
- Tsolakis, I.A.; Tsolakis, A.I.; Elshebiny, T.; Matthaios, S.; Palomo, J.M. Comparing a Fully Automated Cephalometric Tracing Method to a Manual Tracing Method for Orthodontic Diagnosis. J. Clin. Med. 2022, 11, 6854. [Google Scholar] [CrossRef] [PubMed]
- Tsolakis, I.A.; Kolokitha, O.-E.; Papadopoulou, E.; Tsolakis, A.I.; Kilipiris, E.G.; Palomo, J.M. Artificial Intelligence as an Aid in CBCT Airway Analysis: A Systematic Review. Life 2022, 12, 1894. [Google Scholar] [CrossRef]
- Lachinov, D.; Getmanskaya, A.; Turlapov, V. Cephalometric Landmark Regression with Convolutional Neural Networks on 3D Computed Tomography Data. Pattern Recognit. Image Anal. 2020, 30, 512–522. [Google Scholar] [CrossRef]
- Lee, S.M.; Kim, H.P.; Jeon, K.; Lee, S.-H.; Seo, J.K. Automatic 3D Cephalometric Annotation System Using Shadowed 2D Image-Based Machine Learning. Phys. Med. Biol. 2019, 64, 55002. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.; Li, X.; Xu, J. Promoting Healthcare Workers’ Adoption Intention of Artificial-Intelligence-Assisted Diagnosis and Treatment: The Chain Mediation of Social Influence and Human–Computer Trust. Int. J. Env. Res. Public Health 2022, 19, 13311. [Google Scholar] [CrossRef]
- Yoshioka-Maeda, K.; Honda, C.; Sumikawa, Y.; Okamoto, Y.; Shimada, M.; Fujii, H.; Iwasaki-Motegi, R.; Miura, T.; Otsuki, M. Developing a Virtual Reality Simulation Program for Improving Nursing Students’ Clinical Reasoning Skills in Home Settings: A Protocol Paper. Nurs. Rep. 2022, 12, 968–979. [Google Scholar] [CrossRef]
- Kosan, E.; Krois, J.; Wingenfeld, K.; Deuter, C.E.; Gaudin, R.; Schwendicke, F. Patients’ Perspectives on Artificial Intelligence in Dentistry: A Controlled Study. J. Clin. Med. 2022, 11, 2143. [Google Scholar] [CrossRef]
- Thurzo, A.; Kurilová, V.; Varga, I. Artificial Intelligence in Orthodontic Smart Application for Treatment Coaching and Its Impact on Clinical Performance of Patients Monitored with AI-TeleHealth System. Healthcare 2021, 9, 1695. [Google Scholar] [CrossRef]
- Thurzo, A.; Urbanová, W.; Novák, B.; Czako, L.; Siebert, T.; Stano, P.; Mareková, S.; Fountoulaki, G.; Kosnáčová, H.; Varga, I. Where Is the Artificial Intelligence Applied in Dentistry? Systematic Review and Literature Analysis. Healthcare 2022, 10, 1269. [Google Scholar] [CrossRef] [PubMed]
- Thurzo, A.; Strunga, M.; Havlínová, R.; Reháková, K.; Urban, R.; Surovková, J.; Kurilová, V. Smartphone-Based Facial Scanning as a Viable Tool for Facially Driven Orthodontics? Sensors 2022, 22, 7752. [Google Scholar] [CrossRef] [PubMed]
- lo Giudice, A.; Ronsivalle, V.; Venezia, P.; Ragusa, R.; Palazzo, G.; Leonardi, R.; Lazzara, A. Teleorthodontics: Where Are We Going? From Skepticism to the Clinical Applications of a New Medical Communication and Management System. Int. J. Dent. 2022, 2022, 7301576. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Russo, D.; Herford, A.S.; Gorassini, F.; Meto, A.; D’Amico, C.; Cervino, G.; Cicciù, M.; Fiorillo, L. Teledentistry in the Management of Patients with Dental and Temporomandibular Disorders. Biomed. Res. Int. 2022, 2022, 7091153. [Google Scholar] [CrossRef] [PubMed]
- Vaid, N.R.; Hansa, I.; Bichu, Y. Smartphone Applications Used in Orthodontics: A Scoping Review of Scholarly Literature. J. World Fed. Orthod. 2020, 9, S67–S73. [Google Scholar] [CrossRef]
- Hansa, I.; Katyal, V.; Semaan, S.J.; Coyne, R.; Vaid, N.R. Artificial Intelligence Driven Remote Monitoring of Orthodontic Patients: Clinical Applicability and Rationale. Semin. Orthod. 2021, 27, 138–156. [Google Scholar] [CrossRef]
- Nasir, M.; Ramadhany, Y.F. Tele-Orthodontic as a Recent Solution in Malocclusion Treatment. Makassar Dent. J. 2020, 9, 78–81. [Google Scholar] [CrossRef]
- Hannequin, R.; Ouadi, E.; Racy, E.; Moreau, N. Clinical Follow-up of Corticotomy-Accelerated Invisalign Orthodontic Treatment with Dental Monitoring. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 878–888. [Google Scholar] [CrossRef]
- Roisin, L.-C.; Brézulier, D.; Sorel, O. Remotely-Controlled Orthodontics: Fundamentals and Description of the Dental Monitoring System. J. Dentofac. Anom. Orthod. 2016, 19, 408. [Google Scholar] [CrossRef]
- Hansa, I.; Katyal, V.; Ferguson, D.J.; Vaid, N. Outcomes of Clear Aligner Treatment with and without Dental Monitoring: A Retrospective Cohort Study. Am. J. Orthod. Dentofac. Orthop. 2021, 159, 453–459. [Google Scholar] [CrossRef]
- Tandon, D.; Rajawat, J. Present and Future of Artificial Intelligence in Dentistry. J. Oral Biol. Craniofac. Res. 2020, 10, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Rogowski, L.; Kim, J.H.; al Shami, S.; Howell, S.E.I. Teledentistry Platforms for Orthodontics. J. Clin. Pediatr. Dent. 2021, 45, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Thurzo, A.; Urbanová, W.; Waczulíková, I.; Kurilová, V.; Mriňáková, B.; Kosnáčová, H.; Gális, B.; Varga, I.; Matajs, M.; Novák, B. Dental Care and Education Facing Highly Transmissible SARS-CoV-2 Variants: Prospective Biosafety Setting: Prospective, Single-Arm, Single-Center Study. Int. J. Env. Res. Public Health 2022, 19, 7693. [Google Scholar] [CrossRef] [PubMed]
- Thurzo, A.; Stanko, P.; Urbanova, W.; Lysy, J.; Suchancova, B.; Makovnik, M.; Javorka, V. The WEB 2.0 Induced Paradigm Shift in the e-Learning and the Role of Crowdsourcing in Dental Education. Bratisl. Lek. Listy 2010, 111, 168–175. [Google Scholar] [PubMed]
- Dwyer, M.; Prior, S.J.; Jan, P.; Dam, V.; O’brien, L.; Griffin, P. Development and Evaluation of a Massive Open Online Course on Healthcare Redesign: A Novel Method for Engaging Healthcare Workers in Quality Improvement. Nurs. Rep. 2022, 12, 850–860. [Google Scholar] [CrossRef]
- Ye, J.; Wang, S.; Wang, Z.; Liu, Y.; Sun, Y.; Ye, H.; Zhou, Y. Comparison of the Dimensional and Morphological Accuracy of Three-Dimensional Digital Dental Casts Digitized Using Different Methods. Odontology 2023, 111, 165–171. [Google Scholar] [CrossRef]
- Impellizzeri, A.; Horodynski, M.; De Stefano, A.; Palaia, G.; Polimeni, A.; Romeo, U.; Guercio-Monaco, E.; Galluccio, G. CBCT and Intra-Oral Scanner: The Advantages of 3D Technologies in Orthodontic Treatment. Int. J. Environ. Res. Public Health 2020, 17, 9428. [Google Scholar] [CrossRef]
- Impellizzeri, A.; Horodinsky, M.; Barbato, E.; Polimeni, A.; Salah, P.; Galluccio, G. Dental Monitoring Application: It Is a Valid Innovation in the Orthodontics Practice? Clin. Ter. 2020, 171, E260–E267. [Google Scholar] [CrossRef]
- Islam, M.R.R.; Islam, R.; Ferdous, S.; Watanabe, C.; Yamauti, M.; Alam, M.K.; Sano, H. Teledentistry as an Effective Tool for the Communication Improvement between Dentists and Patients: An Overview. Healthcare 2022, 10, 1586. [Google Scholar] [CrossRef]
- Bruno, G.; Gracco, A.; Barone, M.; Mutinelli, S.; de Stefani, A. Invisalign® vs. SparkTM Template: Which Is the Most Effective in the Attachment Bonding Procedure? A Randomized Controlled Trial. Appl. Sci. 2021, 11, 6716. [Google Scholar] [CrossRef]
- Farshidfar, N.; Jafarpour, D.; Hamedani, S.; Dziedzic, A.; Tanasiewicz, M. Proposal for Tier-Based Resumption of Dental Practice Determined by COVID-19 Rate, Testing and COVID-19 Vaccination: A Narrative Perspective. J. Clin. Med. 2021, 10, 2116. [Google Scholar] [CrossRef] [PubMed]
- Lengert, E.V.; Savkina, A.A.; Ermakov, A.V.; Saveleva, M.S.; Lagutina, D.D.; Stepanova, T.V.; Ivanov, A.N. Influence of the New Formulation Based on Silver Alginate Microcapsules Loaded with Tannic Acid on the Microcirculation of the Experimental Periodontitis in Rats. Mater. Sci. Eng. C 2021, 126, 112144. [Google Scholar] [CrossRef] [PubMed]
- Lin, E.; Julien, K.; Kesterke, M.; Buschang, P.H. Differences in Finished Case Quality between Invisalign and Traditional Fixed Appliances. Angle Orthod. 2022, 92, 173–179. [Google Scholar] [CrossRef]
- Vaidya, S.; Limbu, S.; Malla, M. Virtual Dental Care–Pediatric Teledentistry. J. Nepal. Assoc. Pediatr. Dent. 2021, 2, 45–48. [Google Scholar] [CrossRef]
- Holland, C. Will a Robot Take My Job? BDJ Team 2022, 9, 26–28. [Google Scholar] [CrossRef]
- Ma, J.; Schneider, L.; Lapuschkin, S.; Achtibat, R.; Duchrau, M.; Krois, J.; Schwendicke, F.; Samek, W. Towards Trustworthy AI in Dentistry. J. Dent. Res. 2022, 101, 1263–1268. [Google Scholar] [CrossRef] [PubMed]
- Pilipenko, N.D.; Maksyukov, S.Y. Accuracy of Predicting the Upper Arch Expansion Using the ClinCheck Software. Russ. J. Dent. 2021, 25, 159–166. [Google Scholar] [CrossRef]
- Tien, R.; Patel, V.; Chen, T.; Lavrin, I.; Naoum, S.; Lee, R.J.H.; Goonewardene, M.S. The Predictability of Expansion with Invisalign: A Retrospective Cohort Study. Am. J. Orthod. Dentofac. Orthop. 2022, 163, 47–53. [Google Scholar] [CrossRef]
- Bates, M.T.; Shroff, B.; Carrico, C.K.; Kheirandish, N.; Lindauer, S.J. Perceived Efficacy of Extrusion of Maxillary Lateral Incisors with Aligners. Am. J. Orthod. Dentofac. Orthop. 2022, 163, 252–259. [Google Scholar] [CrossRef]
- Pojda, D.; Tomaka, A.A.; Luchowski, L.; Tarnawski, M. Integration and Application of Multimodal Measurement Techniques: Relevance of Photogrammetry to Orthodontics. Sensors 2021, 21, 8026. [Google Scholar] [CrossRef]
- D’Antò, V.; Valletta, R.; Ferretti, R.; Bucci, R.; Kirlis, R.; Rongo, R. Predictability of Maxillary Molar Distalization and Derotation with Clear Aligners: A Prospective Study. Int. J. Environ. Res. Public Health 2023, 20, 2941. [Google Scholar] [CrossRef] [PubMed]
- Dalessandri, D.; Sangalli, L.; Tonni, I.; Laffranchi, L.; Bonetti, S.; Visconti, L.; Signoroni, A.; Paganelli, C. Attitude towards Telemonitoring in Orthodontists and Orthodontic Patients. Dent. J. 2021, 9, 47. [Google Scholar] [CrossRef]
- Daniel, S.J.; Kumar, S. Teledentistry: A Key Component in Access to Care. J. Evid. Based Dent. Pract. 2014, 14, 201–208. [Google Scholar] [CrossRef]
- Thurzo, A.; Šufliarsky, B.; Urbanová, W.; Čverha, M.; Strunga, M.; Varga, I. Pierre Robin Sequence and 3D Printed Personalized Composite Appliances in Interdisciplinary Approach. Polymers 2022, 14, 3858. [Google Scholar] [CrossRef] [PubMed]
- Thurzo, A.; Kosnáčová, H.S.; Kurilová, V.; Kosmeľ, S.; Beňuš, R.; Moravanský, N.; Kováč, P.; Kuracinová, K.M.; Palkovič, M.; Varga, I. Use of Advanced Artificial Intelligence in Forensic Medicine, Forensic Anthropology and Clinical Anatomy. Healthcare 2021, 9, 1545. [Google Scholar] [CrossRef] [PubMed]
- Thurzo, A.; Urbanová, W.; Neuschlová, I.; Paouris, D.; Čverha, M. Use of Optical Scanning and 3D Printing to Fabricate Customized Appliances for Patients with Craniofacial Disorders. Semin. Orthod. 2022, 28, 92–99. [Google Scholar] [CrossRef]
- Švábová nee Uhrová, P.; Beňuš, R.; Chovancová nee Kondeková, M.; Vojtušová, A.; Novotný, M.; Thurzo, A. Use of Third Molar Eruption Based on Gambier’s Criteria in Assessing Dental Age. Int. J. Leg. Med. 2023, 137, 691–699. [Google Scholar] [CrossRef]
- Thurzo, A.; Jančovičová, V.; Hain, M.; Thurzo, M.; Novák, B.; Kosnáčová, H.; Lehotská, V.; Moravanský, N.; Varga, I. Human Remains Identification Using Micro-CT, Spectroscopic and A.I. Methods in Forensic Experimental Reconstruction of Dental Patterns After Concentrated Acid Significant Impact. Molecules 2022, 27, 4035. [Google Scholar] [CrossRef]
- Kim, I.-H.; Cho, H.; Song, J.S.; Park, W.; Shin, Y.; Lee, K.E. Assessment of Real-Time Active Noise Control Devices in Dental Treatment Conditions. Int. J. Env. Res. Public Health 2022, 19, 9417. [Google Scholar] [CrossRef]
- Vitale, M.C.; Gallo, S.; Pascadopoli, M.; Alcozer, R.; Ciuffreda, C.; Scribante, A. Local Anesthesia with SleeperOne S4 Computerized Device vs. Traditional Syringe and Perceived Pain in Pediatric Patients: A Randomized Clinical Trial. J. Clin. Pediatr. Dent. 2023, 47, 82–90. [Google Scholar] [CrossRef]
- Poggio, C.; Colombo, M.; Arciola, C.R.; Greggi, T.; Scribante, A.; Dagna, A. Copper-Alloy Surfaces and Cleaning Regimens against the Spread of SARS-CoV-2 in Dentistry and Orthopedics. From Fomites to Anti-Infective Nanocoatings. Materials 2020, 13, 3244. [Google Scholar] [CrossRef] [PubMed]
- Strunga, M.; Urban, R.; Surovková, J.; Thurzo, A. Artificial Intelligence Systems Assisting in the Assessment of the Course and Retention of Orthodontic Treatment. Healthcare 2023, 11, 683. [Google Scholar] [CrossRef] [PubMed]
- Thurzo, A.; Strunga, M.; Urban, R.; Surovková, J.; Afrashtehfar, K.I. Impact of Artificial Intelligence on Dental Education: A Review and Guide for Curriculum Update. Educ. Sci. 2023, 13, 150. [Google Scholar] [CrossRef]
- Urban, R.; Haluzová, S.; Strunga, M.; Surovková, J.; Lifková, M.; Tomášik, J.; Thurzo, A. AI-Assisted CBCT Data Management in Modern Dental Practice: Benefits, Limitations and Innovations. Electronics 2023, 12, 1710. [Google Scholar] [CrossRef]
- Ferlito, T.; Hsiou, D.; Hargett, K.; Herzog, C.; Bachour, P.; Katebi, N.; Tokede, O.; Larson, B.; Masoud, M.I. Assessment of Artificial Intelligence-Based Remote Monitoring of Clear Aligner Therapy: A Prospective Study. Am. J. Orthod. Dentofac. Orthop. 2023. [Google Scholar] [CrossRef]
- Ryu, J.; Kim, Y.H.; Kim, T.W.; Jung, S.K. Evaluation of Artificial Intelligence Model for Crowding Categorization and Extraction Diagnosis Using Intraoral Photographs. Sci. Rep. 2023, 13, 5177. [Google Scholar] [CrossRef]
- Bao, H.; Zhang, K.; Yu, C.; Li, H.; Cao, D.; Shu, H.; Liu, L.; Yan, B. Evaluating the Accuracy of Automated Cephalometric Analysis Based on Artificial Intelligence. BMC Oral Health 2023, 23, 191. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Surovková, J.; Haluzová, S.; Strunga, M.; Urban, R.; Lifková, M.; Thurzo, A. The New Role of the Dental Assistant and Nurse in the Age of Advanced Artificial Intelligence in Telehealth Orthodontic Care with Dental Monitoring: Preliminary Report. Appl. Sci. 2023, 13, 5212. https://doi.org/10.3390/app13085212
Surovková J, Haluzová S, Strunga M, Urban R, Lifková M, Thurzo A. The New Role of the Dental Assistant and Nurse in the Age of Advanced Artificial Intelligence in Telehealth Orthodontic Care with Dental Monitoring: Preliminary Report. Applied Sciences. 2023; 13(8):5212. https://doi.org/10.3390/app13085212
Chicago/Turabian StyleSurovková, Jana, Sára Haluzová, Martin Strunga, Renáta Urban, Michaela Lifková, and Andrej Thurzo. 2023. "The New Role of the Dental Assistant and Nurse in the Age of Advanced Artificial Intelligence in Telehealth Orthodontic Care with Dental Monitoring: Preliminary Report" Applied Sciences 13, no. 8: 5212. https://doi.org/10.3390/app13085212