
Validation of the Implant Stability Test for Implant Provisional Crowns: An In Vitro Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Fabrication of Provisional Crown
2.2. Measurement of the IST Value
2.3. Statistical Analysis
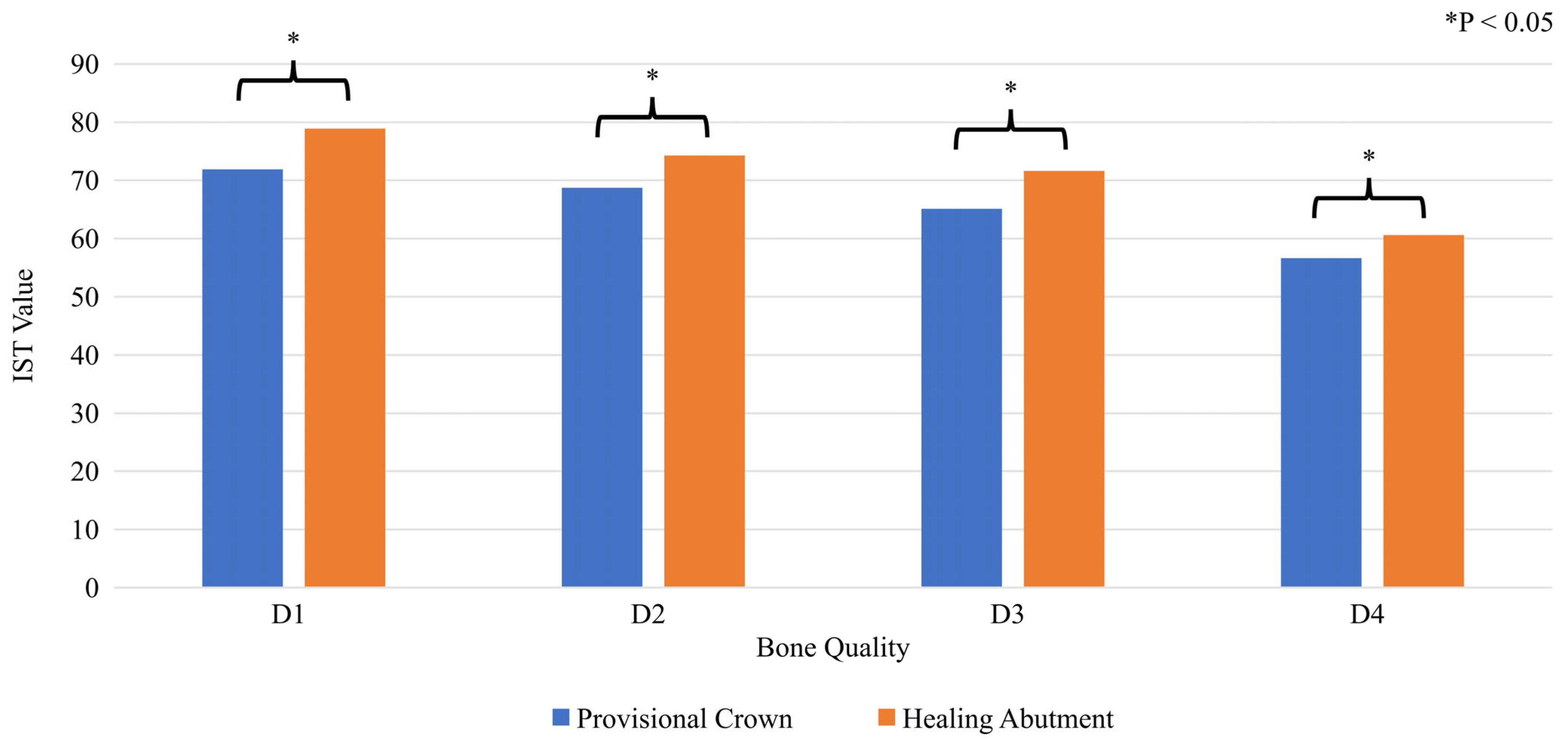
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smeets, R.; Stadlinger, B.; Schwarz, F.; Beck-Broichsitter, B.; Jung, O.; Precht, C.; Kloss, F.; Gröbe, A.; Heiland, M.; Ebker, T. Impact of dental implant surface modifications on osseointegration. BioMed Res. Int. 2016, 2016, 6285620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makowiecki, A.; Hadzik, J.; Błaszczyszyn, A.; Gedrange, T.; Dominiak, M. An evaluation of superhydrophilic surfaces of dental implants—A systematic review and meta-analysis. BMC Oral Health 2019, 19, 79. [Google Scholar] [CrossRef] [PubMed]
- Papaspyridakos, P.; De Souza, A.; Vazouras, K.; Gholami, H.; Pagni, S.; Weber, H.P. Survival rates of short dental implants (≤6 mm) compared with implants longer than 6 mm in posterior jaw areas: A meta-analysis. Clin. Oral Implant. Res. 2018, 29 (Suppl. S16), 8–20. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Salvi, G.E.; Huynh-Ba, G.; Ivanovski, S.; Donos, N.; Bosshardt, D.D. Early osseointegration to hydrophilic and hydrophobic implant surfaces in humans. Clin. Oral Implant. Res. 2011, 22, 349–356. [Google Scholar] [CrossRef]
- Chambrone, L.; Shibli, J.A.; Mercúrio, C.E.; Cardoso, B.; Preshaw, P.M. Efficacy of standard (SLA) and modified sandblasted and acid-etched (SLActive) dental implants in promoting immediate and/or early occlusal loading protocols: A systematic review of prospective studies. Clin. Oral Implant. Res. 2015, 26, 359–370. [Google Scholar] [CrossRef]
- Moretto, D.; Gargari, M.; Nordsjö, E.; Gloria, F.; Ottria, L. Immediate loading: A new implant technique with immediate loading and aesthetics: Nobel Active™. Oral Implantol. Rome 2008, 1, 50–55. [Google Scholar]
- Atsumi, M.; Park, S.H.; Wang, H.L. Methods used to assess implant stability: Current status. Int. J. Oral Maxillofac. Implant. 2007, 22, 743–754. [Google Scholar]
- Park, Y.H.; Leesungbok, R.; Lee, S.W.; Peak, J.; Lee, J.Y. Differences in percussion-type measurements of implant stability according to height of healing abutments and measurement angle. J. Korean Acad. Prosthodont. 2018, 56, 278. [Google Scholar] [CrossRef] [Green Version]
- Okuhama, Y.; Nagata, K.; Kim, H.; Tsuruoka, H.; Atsumi, M.; Kawana, H. Validation of an implant stability measurement device using the percussion response: A clinical research study. BMC Oral Health 2022, 22, 286. [Google Scholar] [CrossRef]
- Staedt, H.; Kämmerer, P.W.; Goetze, E.; Thiem, D.G.E.; Al-Nawas, B.; Heimes, D. Implant primary stability depending on protocol and insertion mode—An ex vivo study. Int. J. Implant. Dent. 2020, 6, 49. [Google Scholar] [CrossRef]
- Koutouzis, T.; Koutouzis, G.; Gadalla, H.; Neiva, R. The effect of healing abutment reconnection and disconnection on soft and hard peri-implant tissues: A short-term randomized controlled clinical trial. Int. J. Oral Maxillofac. Implant. 2013, 28, 807–814. [Google Scholar] [CrossRef] [Green Version]
- Misch, C.E. Density of bone: Effect on treatment plans, surgical approach, healing, and progressive bone loading. Int. J. Oral Implantol. 1990, 6, 23–31. [Google Scholar]
- Hill, E.E.; Phillips, S.M.; Breeding, L.C. Implant abutment screw torque generated by general dentists using a hand driver in a limited access space simulating the mouth. J. Oral Implantol. 2007, 33, 277–279. [Google Scholar] [CrossRef]
- Atieh, M.A.; Ibrahim, H.M.; Atieh, A.H. Platform switching for marginal bone preservation around dental implants: A systematic review and meta-analysis. J. Periodontol. 2010, 81, 1350–1366. [Google Scholar] [CrossRef]
- Makary, C.; Menhall, A.; Zammarie, C.; Lombardi, T.; Lee, S.Y.; Stacchi, C.; Park, K.B. Primary stability optimization by using fixtures with different thread depth according to bone density: A clinical prospective study on early loaded implants. Materials 2019, 12, 2398. [Google Scholar] [CrossRef] [Green Version]
- Falco, A.; Berardini, M.; Trisi, P. Correlation between implant geometry, implant surface, insertion torque, and primary stability: In vitro biomechanical analysis. Int. J. Oral Maxillofac. Implant. 2018, 33, 824–830. [Google Scholar] [CrossRef]
- van Eekeren, P.; Said, C.; Tahmaseb, A.; Wismeijer, D. Resonance frequency analysis of thermal acid-etched, hydrophilic implants during first 3 months of healing and osseointegration in an early-loading protocol. Int. J. Oral Maxillofac. Implant. 2015, 30, 843–850. [Google Scholar] [CrossRef] [Green Version]
- Benic, G.I.; Mir-Mari, J.; Hämmerle, C.H. Loading protocols for single-implant crowns: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Implant. 2014, 29, 222–238. [Google Scholar] [CrossRef] [Green Version]
- Mijiritsky, E.; Barone, A.; Cinar, I.C.; Nagy, K.; Shacham, M. 3D Considerations and outcomes of immediate single implant insertion and provisionalization at the maxillary esthetic one: A long-term retrospective follow-up study of up to 18 years. J. Clin. Med. 2021, 10, 4138. [Google Scholar] [CrossRef]
- Douglas de Oliveira, D.W.; Lages, F.S.; Lanza, L.A.; Gomes, A.M.; Queiroz, T.P.; Costa Fde, O. Dental implants with immediate loading using insertion torque of 30 Ncm: A systematic review. Implant. Dent. 2016, 25, 675–683. [Google Scholar] [CrossRef]
- Maló, P.; Lopes, A.; de Araújo Nobre, M.; Ferro, A. Immediate function dental implants inserted with less than 30N·cm of torque in full-arch maxillary rehabilitations using the All-on-4 concept: Retrospective study. Int. J. Oral Maxillofac. Surg. 2018, 47, 1079–1085. [Google Scholar] [CrossRef] [PubMed]
- Darriba, I.; Seidel, A.; Moreno, F.; Botelho, J.; Machado, V.; Mendes, J.J.; Leira, Y.; Blanco, J. Influence of low insertion torque values on survival rate of immediately loaded dental implants: A systematic review and meta-analysis. J. Clin. Periodontol. 2023, 50, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Santing, H.J.; Meijer, H.J.; Raghoebar, G.M.; Özcan, M. Fracture strength and failure mode of maxillary implant-supported provisional single crowns: A comparison of composite resin crowns fabricated directly over PEEK abutments and solid titanium abutments. Clin. Implant. Dent. Relat. Res. 2012, 14, 882–889. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Fan, Y.; Lin, Z.; Song, Z.; Shu, R.; Xie, Y. Survival rate and potential risk indicators of implant loss in non-smokers and systemically healthy periodontitis patients: An up to 9-year retrospective study. J. Periodontal Res. 2021, 56, 547–557. [Google Scholar] [CrossRef] [PubMed]
- Cannizzaro, G.; Leone, M.; Ferri, V.; Viola, P.; Gelpi, F.; Esposito, M. Immediate loading of single implants inserted flapless with medium or high insertion torque: A 6-month follow-up of a split-mouth randomised controlled trial. Eur. J. Oral Implantol. 2012, 5, 333–342. [Google Scholar]
- Alfadda, S.A.; Chvartszaid, D.; Tulbah, H.I.; Finer, Y. Immediate versus conventional loading of mandibular implant-supported fixed prostheses in edentulous patients: 10-year report of a randomised controlled trial. Int. J. Oral Implantol. Berl. 2019, 12, 431–446. [Google Scholar]
- Mitsias, M.; Siormpas, K.; Pistilli, V.; Trullenque-Eriksson, A.; Esposito, M. Immediate, early (6 weeks) and delayed loading (3 months) of single, partial and full fixed implant supported prostheses: 1-year post-loading data from a multicentre randomised controlled trial. Eur. J. Oral Implantol. 2018, 11, 63–75. [Google Scholar]
- Lopes, A.; Maló, P.; de Araújo Nobre, M.; Sanchez-Fernández, E. The NobelGuide® All-on-4® treatment concept for rehabilitation of edentulous jaws: A prospective report on medium- and long-term outcomes. Clin. Implant. Dent. Relat. Res. 2015, 17 (Suppl. S2), e406–e416. [Google Scholar] [CrossRef]
- Toljanic, J.A.; Ekstrand, K.; Baer, R.A.; Thor, A. Immediate loading of implants in the edentulous maxilla with a fixed provisional restoration without bone augmentation: A report on 5-year outcomes data obtained from a prospective clinical trial. Int. J. Oral Maxillofac. Implant. 2016, 31, 1164–1170. [Google Scholar] [CrossRef]
- Al-Jamal, M.F.J.; Al-Jumaily, H.A. Can the bone density estimated by CBCT predict the primary stability of dental implants? A new measurement protocol. J. Craniofac. Surg. 2021, 32, e171–e174. [Google Scholar] [CrossRef]
- Lim, H.K.; Lee, S.J.; Jeong, Y.; Lee, J.S.; Ryu, J.J.; Shim, J.S.; Song, I.S. Clinical Validation of Dental Implant Stability by Newly Designed Damping Capacity Assessment Device during the Healing Period. Medicina 2022, 58, 1570. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healing Abutment Height | IST Value |
|---|---|
| 7 mm | +6 |
| 6 mm | +4 |
| 5 mm | +2 |
| 4 mm | ±0 |
| 3 mm | −2 |
| 2 mm | −4 |
| 1 mm | −6 |
| Provisional Crown | D1 | D2 | D3 | D4 | Healing Abutment | D1 | D2 | D3 | D4 |
|---|---|---|---|---|---|---|---|---|---|
| Mean | 71.9 | 68.7 | 65.1 | 56.6 | Mean | 78.9 | 74.3 | 71.6 | 60.6 |
| SD | 1.62 | 1.58 | 0.93 | 1.24 | SD | 1.54 | 2.96 | 0.89 | 1.33 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okuhama, Y.; Nagata, K.; Nakashizu, T.; Wakamori, K.; Okubo, M.; Tsuruoka, H.; Kawana, H. Validation of the Implant Stability Test for Implant Provisional Crowns: An In Vitro Study. Appl. Sci. 2023, 13, 3947. https://doi.org/10.3390/app13063947
Okuhama Y, Nagata K, Nakashizu T, Wakamori K, Okubo M, Tsuruoka H, Kawana H. Validation of the Implant Stability Test for Implant Provisional Crowns: An In Vitro Study. Applied Sciences. 2023; 13(6):3947. https://doi.org/10.3390/app13063947
Chicago/Turabian StyleOkuhama, Yurie, Koudai Nagata, Toshifumi Nakashizu, Kana Wakamori, Manabu Okubo, Hayato Tsuruoka, and Hiromasa Kawana. 2023. "Validation of the Implant Stability Test for Implant Provisional Crowns: An In Vitro Study" Applied Sciences 13, no. 6: 3947. https://doi.org/10.3390/app13063947